
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dev Bhoomi Uttarakhand University, School of Pharmacy and Research
Herbal medicines are very much in demand due to their wide range of therapeutic and biological properties, safety and lower cost. The aim of this review is to compose and focus on the recent findings about Lepidium sativum and its therapeutic uses. Worldwide, millions of people suffer from osteoarthritis, the most common arthritis. The main reason it takes place is due to the gradual deterioration of the cartilage that cushions the ends of the bones. Although osteoarthritis can affect any joint, it mostly affects hands, knees, hips and spine. Its symptoms are mainly manageable even if joint degeneration cannot be undone. Keeping up with an active lifestyle, following proper diet to maintain weight and taking therapies helps to reduce joint related pain and further reduces the progression of Disease. Adding to it, Lepidium sativum also has medical potential to reduce the progression and to manage arthritis especially in case of osteoarthritis. It contains bioactive substances like kaempferol, glucuronide, gallic acid, protocatechuic acid, coumaric acid, caffeic acid, terpenes, and glucosinolates, it also has high amounts of proteins, fatty acids, minerals, and vitamins. Garden cress shows its ability for treating osteoarthritis even though further research is required to improve its bioavailability and further Research is needed to improve its formulations, dosage pattern, routes of administration.
Osteoarthritis (OA) is the most prevalent chronic health condition that affects not only physical function and pain but also a wide range of other outcomes, such as mental health, sleep, work participation, and even mortality [1]. Collectively, it can be understood as a diverse group of conditions that cause joint symptoms and signs associated with the loss of integrity of the articular cartilage, along with changes in the underlying bone and joint margins [2]. Some estimates say that 3.8% of the world's population, or about 277 million people, have symptomatic knee OA. [3]. OA symptoms usually start out mild, but they get worse over time and make it harder for people to do their daily tasks and work well [4]. The precise etiology of OA is yet to be elucidated; it is a multifaceted condition affected by various factors, including body mass, age, sex, genetics, and occupational exposures [5,6]. India is the second most populous country in the world, and its population is growing faster than China's. [7]. There are big differences in socioeconomic status, culture, ethnicity, genetics, and health systems between states. Some states even have populations that are bigger than those of some other countries [8]. India's life expectancy has gone up by 10 years or more, and over the past 30 years, health-related epidemiological and demographic indicators have gotten a lot better [9].
The percentage of people who have crossed 65 years of age has significantly increased from 3.8% in 1990 to 6.4% in 2019, and the prevalence of overweight and obesity is rising faster than the global average [10]. These trends highlight the burden of age and lifestyle-related diseases, underscoring the importance of understanding their impact on public health. OA is one such condition with a substantial global burden. In 2019, an estimated 528 million people worldwide were affected by OA, a number expected to rise due to aging populations and increasing obesity rates.[11] .By 2021, there were about 607 million cases of OA around the world. The number of cases and the number of people who have it have been steadily rising since 1990. In 2023, OA was responsible for 2.5% of Australia's overall disease burden (DALYs) and almost 20% of the burden of musculoskeletal diseases. In India, OA poses a considerable public health challenge [12,13]. Acharya et al. (2025) report that the prevalence of knee osteoarthritis (OA) among elderly adults is 47% (95% confidence interval: 38.4%-55.8%), signifying that nearly half of the elderly population is affected by knee OA, which imposes a significant burden on the healthcare system [14]. It is essential to comprehend national and state-level estimates of OA burden in India for the formulation of effective healthcare interventions and the allocation of resources.
2. Osteoarthritis (OA):
2.1 Etiology of osteoarthritis
It is still unknown exactly what causes osteoarthritis. This disorder is the result of the interaction of several factors, including obesity, trauma, and heredity. Osteoarthritis can result from any event that alters the chondrocyte's environment; some risk factors are summarized in Table 1 [15]. Furthermore, focus is currently increasing on intrinsic factors such as proprioception, laxity, alignment, and strength [16]. A classification of OA risk factors that considers ethnicity, sports participation, and muscle weakness has been proposed by Michael et al. Although severe joint damage alone may be enough to induce OA, the disease is frequently the result of a combination of local and systemic factors or biomechanical insult, like a knee injury [17]. Figure 1 shows the conditions of a healthy and an osteoarthritic knee joint.
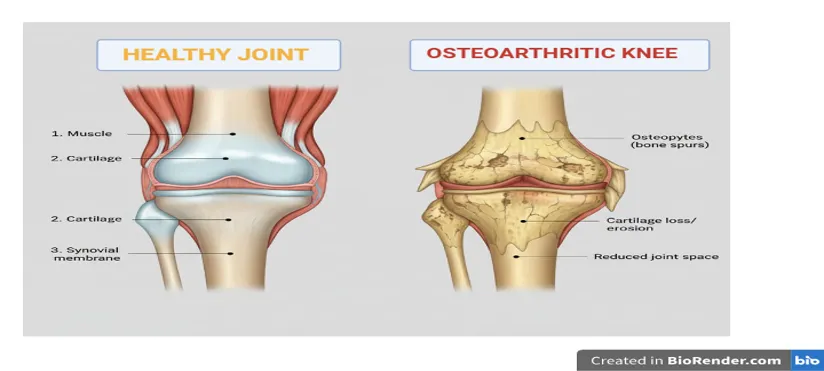
Figure 1: Osteoarthritis conditions in healthy and diseased condition
Table1: Risk factors and symptoms[17,18]
|
Sr.no. |
Risk factor |
Symptoms |
|
1. |
High bone mineral density |
Joint pain |
|
2. |
History of immobilization |
Joint stiffness |
|
3. |
Injury to the joint |
Joint instability |
|
4. |
Joint hypermobility or instability |
Creptius |
|
5. |
Obesity (weight-bearing joints) |
Restricted joint motion |
|
6. |
Peripheral neuropathy |
Joint tenderness |
|
7. |
Prolonged occupational or sports stress |
Muscle atropy |
|
8. |
Genetics |
Bony changes |
|
9. |
Metabolic diseases |
Inflammation |
|
10. |
Age |
Joint deformity |
2.2 Pathophysiology of osteoarthritis:
OA has long been associated mainly with the degeneration of articular cartilage, which is frequently caused by trauma, obesity, metabolic diseases, and genetic predispositions. Recent research indicates that subchondral bone lesions are crucial in the early stages of the disease, helping to develop osteophytes and ectopic bone [19]. Age, obesity, trauma, and congenital joint abnormalities that lead to articular cartilage degeneration are the main causes of OA [20]. OA primarily affects middle-aged and older people, particularly in weight-bearing joints (e.g., the hip and knee) and the cervical and lumbar vertebrae 21]. Changes in gene expression patterns and the inheritance of cartilage and subchondral bone are examples of genetic factors[22]. According to epidemiological studies, OA is primarily a mechanically induced disease, and its severity is further influenced by various factors [23].
2.2.1 Changes in Osteochondral Units in Osteoarthritis:
The distal end of calcified cartilage, also known as subchondral bone (SB), is made up of two parts: the subchondral bone plate (SBP) and the subchondral bone trabecula7[24]. The SBP is made up of a layer of porous cortical plate that sits beneath the calcified cartilage. Overlying the trabecular bone is a layer of highly vascularized cortical bone called the SBP [25]. Subchondral bone experiences distinctive alterations in OA. According to Coaccioli et al., even in the early stages of the disease, "subchondral bone marrow lesions (SBMLs), reported by abnormal MRI signals below the calcified cartilage," are common [26]. A high in situ turnover rate, pain, and proinflammatory pathway activation are all present at SBML sites, which ultimately lead to increased subchondral sclerosis and bone mineral density. Studies have shown a strong correlation between SBML size and the loss of overlying cartilage as the lesions enlarge [26,27]. As a result, "subchondral bone remodeling is now considered a key element of OA," which can cause "increased crosstalk between cartilage and subchondral bone" and disturb the osteochondral unit[28,29]. Such remodeling, which often leads to the formation of ectopic bone and osteophytes, may precede and accelerate cartilage degeneration. It includes sclerosis of the bone plate and altered trabeculae [30].
2.2.2 Inflammation of the synovium (synovitis)
It is now understood that OA is primarily caused by low-grade synovial Inflammation. One of the main characteristics of the pathophysiology of OA, according to Coaccioli et al., is "low-grade chronic Inflammation of the synovial membrane (synovitis)"[31,32]. Accordingly, they observe that "the majority of OA patients exhibit low-grade inflammation, which has thus been crucial in OA development and progression" [33]. Numerous studies "have shown the presence of synovitis in OA patients and demonstrated a direct association between joint inflammation and disease progression," according to Mobasheri and Batt [34–36]. A catabolic environment is fueled by proinflammatory mediators (IL-1β, TNF-α, chemokines, ROS, etc.) released by activated synovial cells (macrophages, fibroblasts, mast cells, etc.). They "degrade the extracellular matrix and mediate cartilage loss" in OA, for instance [37]. Therefore, chronic synovitis contributes to progressive joint damage and maintains the inflammatory milieu.
2.2.3Adaptive and Innate Immune System Participation
Both innate and adaptive immunity are responsible for the sterile inflammation characteristics seen in OA. Innate pattern-recognition receptors are activated by damage-associated molecular patterns resulting from matrix breakdown. TLR-2 and TLR-4 are upregulated in the synovial tissue of patients with OA, which results in the upregulation of prostaglandin E2, nitric oxide, and matrix metalloproteases, as Coaccioli et al. observed [38]. When these Toll-like receptors are activated, a self-reinforcing inflammatory loop is fueled, and chondrocyte apoptosis is triggered, which is "a dominant feature in OA" [33]. Concurrently, cytokines and cartilage fragments in the joint fluid "activate synovial macrophages," which in turn "further stimulate the release of proinflammatory cytokines, such as IL-1β and TNF-α involved in OA pathology"[39]. Coaccioli et al. note that "CD4+ T cells and macrophages are abundantly present in OA synovium and can activate each other", suggesting that adaptive immunity is also involved [40]. Specifically, Th1-type CD4+ T cells trigger B cells to produce autoantibodies against cartilage components and "activate both innate and adaptive immune responses, propagate synovial inflammation, and increase cartilage deterioration" [41]. Therefore, OA entails a coordinated innate/adaptive immune response that intensifies tissue destruction and synovitis.
2.2.4 Oxidative Stress
Oxidative stress is a key driver of OA pathology. According to Coaccioli et al., "oxidative stress and ROS production were found elevated in patients with OA, and the concept of chronic or prolonged ROS production is considered central to the progression of inflammatory disease"[42]. This indicates that ROS production is chronically elevated in OA. Antioxidant enzyme levels (SOD, catalase, glutathione peroxidase) are decreased in OA cartilage and synovium, while indicators of oxidative damage (lipid peroxidation products, nitrotyrosine, etc.) are accumulated [43]. These results "indicate that oxidative stress plays a part in the pathophysiology of OA".
2.2.5 Chondrosenescence
One factor contributing to OA is age-related chondrocyte senescence. To characterize this process, Mobasheri and Batt coined the term "chondrosenescence." According to them, the age-dependent decline in chondrocyte function that causes cartilage dysfunction in OA is known as "chondrosenescence"[30]. OA chondrocytes release proinflammatory and matrix-degrading substances and display classic senescence markers, including telomere erosion and DNA damage indicators. The authors suggest that a small number of "senescent chondrocytes" may take advantage of the inflammatory environment and "further [contribute] to the age-related degradation of articular cartilage, subchondral bone, synovium, and other tissues"[30] It is significant to note that even a small fraction of these "senescent" cells can have significant effects. Thus, chondrosenescence connects the long-term, progressive joint damage of OA with cellular aging.
2.2.6 Central Sensitization and Neuroinflammation
In OA, pain reflects central sensitization and neuroimmune interactions. In chronic OA pain, Coaccioli et al. report "bidirectional interactions between the immune and nervous systems" [44], which include crosstalk in the spinal cord, dorsal root ganglia, and synovium. They "are more sensitive to experimental noxious stimuli at body sites distant from their affected joint, suggesting the presence of central sensitization," which is consistent with the widespread hyperalgesia seen in OA patients. NGF, histamine, and other mediators released by mast cell degranulation, for instance, "enhance and support electrophysiological alterations of nerve fibers, leading to their sensitization"[45,46]. This is one example of how peripheral immune cells enhance nociception. Eventually, this ongoing peripheral sensitization "leads to the hyperexcitability of second-order neurons and activation of microglia," which in turn causes central alterations [27]. In conclusion, both local neuroinflammation and supraspinal sensitization mechanisms contribute to OA pain.
2.2.7 Neoangiogenesis
Another characteristic of OA is abnormal blood vessel growth. According to Coaccioli et al., "increased subchondral bone angiogenesis and the blood vessel invasion into the avascular cartilage" are early indicators of OA 47]. Because new vessels allow inflammatory cells to enter the cartilage and introduce nociceptive fibers, angiogenesis is "a key factor in the pathogenesis of OA". In OA, vascular growth takes over, and articular cartilage "loses its resistance to vascularization" [48]. Consequently, sensory nerves travel along vascular channels that develop from the subchondral bone into the cartilage. Interestingly, "sensory nerves invade noncalcified articular cartilage, osteophytes, and the inner regions of menisci, where they normally do not occur, and grow along new blood vessels in OA joints" [26].In OA, pain and tissue damage are directly caused by this pathological neovascularization and the ensuing nerve ingrowth [26].
2.2.8. Formation of Osteophytes
One characteristic of OA joint remodeling is the formation of osteophytes. "Osteocartilaginous outgrowths that typically form at the joint margins" is how they are defined [49]. It is generally accepted that osteophytes form as a mechanical stabilizing response. They are "considered an endogenous repair response to excessive mechanical load" in degenerative joints, redistributing forces to help preserve cartilage [50–52]. In fact, abnormal loading (such as meniscal malalignment) and joint instability are frequently associated with osteophytes [53,54]. Interestingly, osteophyte biology is also influenced by immunological processes. For instance, one study discovered mast cells in OA osteophytes whose maturation was synchronized with disease progression in synovial fluid [55]
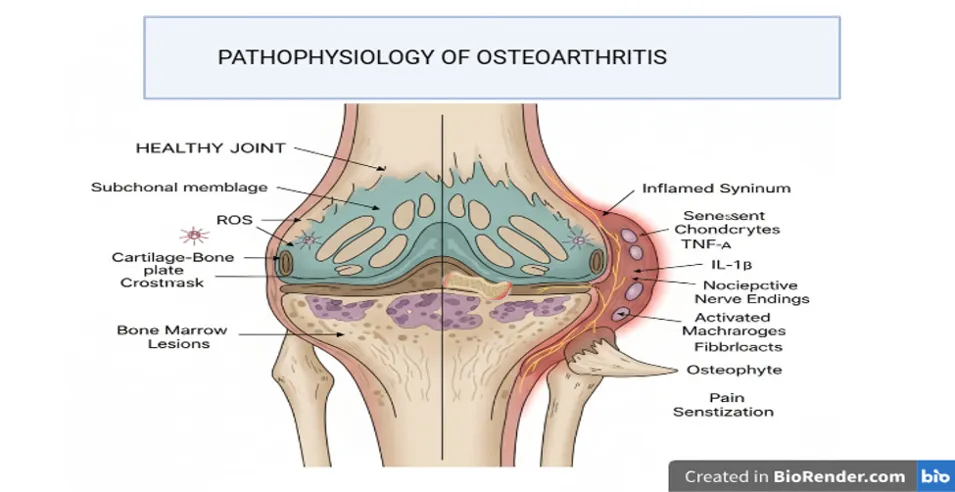
Fig. 2: Pathophysiology of osteoarthritis
2.3 Therapeutic Strategies employed for OA:
Some ways to treat OA are physical therapy, medicine, and surgery. Pharmacological interventions for pain management and enhancement of joint function typically comprise chondroprotective agents and nonsteroidal anti-inflammatory drugs [56]. Physical treatments that increase blood flow and reduce Inflammation include extracorporeal shockwave therapy and intermediate-frequency pulse electrotherapy [56,57]. Joint replacement surgery might be necessary in cases of severe OA. Traditional Chinese Medicine (TCM) is increasingly being used to treat OA. To relieve symptoms, TCM treatment focuses on reestablishing homeostasis using massage, acupuncture, and herbal remedies [58,59]. Recent advances have significantly influenced the creation of treatment plans and our understanding of the pathological mechanisms underlying OA [60]. Novel approaches to treating OA have been made possible by studies that concentrate on the Wnt signaling pathway, the interaction between autophagy and apoptosis, and synovial inflammation [61]. For example, cartilage homeostasis depends on Wnt signaling activation.
On the other hand, OA causes matrix degradation and chondrocyte apoptosis due to its abnormal activation [62]. Clinical trials have demonstrated that Wnt signaling inhibition improves OA [59]. Furthermore, the development of cutting-edge technologies such as gene engineering and cell-based therapies offers new methods for treating OA [63]. Despite the complexity of OA's etiology, a cure has not yet been found. As a result, the main goals of current treatments are to reduce symptoms, slow the course of the disease, and enhance quality of life [63,64]
Table 2: Clinical candidates used in the treatment of osteoarthritis
|
Drug Category |
Examples |
Moa |
Side Effects |
|
Analgesics |
Paracetamol |
Inhibit prostaglandin synthesis in CNS |
Liver toxicity (high dose), nausea |
|
NSAIDS |
Diclofenac, Ibuprofen, naproxen |
Inhibit cox leading to decrease in prostaglandins |
Gastric irritation, ulcers, Kidney issues |
|
Cox-2 inhibitors |
Celecoxib, etoricoxib |
Selectively inhibit cox-2 Reducing Inflammation |
CVS risk, mild GI Upset |
|
Intra-articular drugs |
Corticosteroids, hyaluronic acid |
Reduce Inflammation and improve joint lubrication |
Joint pain may increase |
3.0 Lepidium sativum Linn
3.1 Lepidium sativum Linn., also called garden cress, is an upright, glabrous annual that grows to a height of 15 to 45 cm and is grown as a salad plant in India, Europe, and the United States. It is a member of the Cruciferae family. The cauline leaves are typically whole and sessile. It has long racemes of tiny white flowers. The pods are winged, elliptic, rotundate, emarginated, obovate, or broadly obovate, and have an apical notch. Although it does well in moist loam, the plant can grow in any good light soil. Although it can be grown year-round at all elevations, the winter months yield the best crop (Wealth of India, 1962) [65]. This cool-season herb, which originated in Southwest Asia and Egypt, is now widely grown in hot, temperate climates worldwide for a range of culinary and medicinal uses [66]. The leaves of the plant are eaten raw in salads, cooked in vegetable curries, and used for garnishing. The plant is used to make feed for horses and camels. It also has therapeutic qualities and is used to treat asthma, cough, and bleeding piles. Leaves can help with liver issues and scorbutic diseases, and they are also mild stimulants and diuretics. The root is used to treat secondary syphilis and tenesmus. The plant's seeds are aphrodisiac, diuretic, laxative, tonic, galactogogue, emmenagogue, and rubefacient [65]
Garden cress is a fast-growing, short-lived herb with distinct morphological features across its roots, stems, leaves, and seeds. The roots are thin, shallow, and not very branched, which helps them grow quickly, take in nutrients, and stay in place [67,68]. The stem is green, soft, herbaceous, and upright. Some types may have a faint purple tint or start to bolt early. It helps leaves and flowers stay in place, and the young stems are safe to eat [67]. The leaves make a base rosette and are soft, curly, or lobed. They are bright green and sometimes have colour. They are the main food source and are high in antioxidants and vitamin C [69]. The seeds are small, oval, smooth, reddish-brown, and 3 to 4 mm long and 1 to 2 mm wide. They have a pointed triangular end and furrows on both sides that go down two-thirds of the way.When the seeds are soaked in water, the edges swell and form a colourless, mucilaginous coating with a distinct taste. Seeds are commonly utilised in traditional medicine, encompassing oil extraction and diverse therapeutic applications [72]. The seed has a testa, a single-layered tegmen, a dense polygonal embryo, and thick-walled polygonal endosperm cells that surround the embryo and serve as food for the embryo. Powdered seeds show fragments of testa, embryo cells, and oil droplets, highlighting their structural and bioactive composition [73]
Table 3: Botanical description of and taxonomical classification (USFDA) of Lepidium Sativum [72]
|
Botanical Description |
|
Taxonomical Classification |
||
|
Parameter |
characteristics |
|
Kingdom |
Plantae |
|
Height |
47-50cm |
|
Subkingdom |
Tracheobionta |
|
Flower |
Small, white to pinkish in colour |
|
Super division |
Spermatophyta |
|
Leaves |
Lobed shaped with linear segment |
|
Division |
Magnoliophyte |
|
Pods |
Obavate,5mm length |
|
Class |
Magnoliopsida |
|
Harvesting time |
90 days |
|
Subclass |
Dilleniidae |
|
Taste |
Peppery, pungent taste with hot mouth feel |
|
Order |
Capparales |
|
Colour of seeds |
Reddish-brown |
|
Family |
Brassicaeae |
|
Shape of seed |
Oval |
|
Genus |
Lepidium |
Table:4 Vernacular names of garden cress plant in India [68]
|
Languages |
Word |
|
Hindi |
Chandrasur, Halam, Chansur, Halim |
|
Sanskrit |
Raktabija,Chandrika,Pashu,Chandsura |
|
Himachali |
Haloyen |
|
Marathi |
Haliv, Ahaliva |
|
Assamese |
Chandrakiri, Halim shak |
|
Manipuri |
Chantruk |
|
Nepali |
Chausur, chamsur , chansur |
|
Telegu |
Adiyalu, Adeli |
|
Urdu |
Halim |
|
Punjabi |
Halium, Holan,Tezak |
|
Bengali |
Halim shak , Alaverie |
|
Oriya |
Hidamba saag |
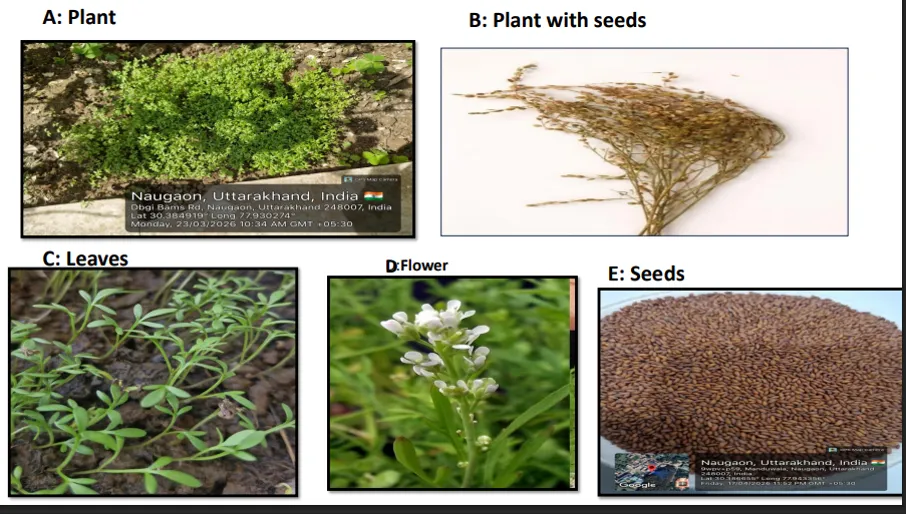
Figure 2. Morphological description of plant
3.2 Chemical composition
Garden cress's extremely nutrient-dense profile makes it a superfood. It contains 21–25% protein, which is necessary for tissue repair and muscle growth. The seeds are a good source of energy for people who are undernourished because they contain fat (23–25%) and carbohydrates (30–34%). Garden cress seeds contained the following nutrients: protein (24.2), fat (23.2), carbohydrate (30.7), fiber (11.9), ash (7.1), and moisture (2.9) [74] This seed contains adequate levels of thiamine (0.59 mg), riboflavin (0.61 mg), and niacin (14.3 mg) [71]. In addition to being a good source of calcium, magnesium, and iron, garden cress has a higher potassium content than dates (696 mg/100 g), white beans (561 mg/100 g), spinach (558 mg/100 g), avocado (485 mg/100 g), and banana (358 mg/100 g).Garden cress contains calcium (377 mg/100 g) and magnesium (430 mg/100 g), which help muscles contract correctly for healthy heart and limb movements [74]. High amounts of linolenic (26–34%), linoleic (7.5–11.8%), and arachidic (2–3.5%) fatty acids, which are also beneficial for the brain and memory, are characteristics of the fatty acid profile of garden cress seeds. The seeds also contain oleic, stearic, and palmitic acids. Alpha-tocopherol and beta-sitosterol are present in the contraction of unsaponifiable materials [75]Garden cress seed protein is of excellent quality and includes essential amino acids like phenylalanine (5.65 g) and lysine (6.26 g). One of the limiting amino acids in the seeds is methionine (0.97 g) [76]. Furthermore, glutamic acid and aspartic acid, two primary, non-essential amino acids, are abundant in garden cress seeds. According to the oilseed analysis, the most prevalent amino acids in garden cress seeds were glutamic acid (19.33 ± 0.19%) and aspartic acid (9.76 ± 0.03%) [77].
Table5: Chemical constituents of Lepidium sativum [71]
|
Carbohydrate Profile |
% in Gc seeds |
|
Starch |
10.3±0.69 |
|
Pentosans |
11.0±0.38 |
|
Free reducing sugars |
0.76±0.03 |
|
Crude fiber |
16.5±1.05 |
|
Acid detergent fibe |
27.3±0.43 |
|
Neutral detergent fiber |
35.7±0.82 |
|
Hemi cellulose |
8.4±0.39 |
|
Cellulose |
9.4±0.03 |
|
Acid insoluble lignin |
17.9±0.40 |
Table 6: Carbohydrate profile of garden cress seeds [78]
|
Nutrient |
Whole Meal |
Bran |
|
Moisture Content |
4.14±0.05 |
4.27±0.01 |
|
Protein |
22.47±0.78 |
12.58±0.21 |
|
Fat |
27.48±0.14 |
6.34±0.19 |
|
Carbohydrates** |
34.24±0.92 |
50.31±0.08 |
|
Crude Fiber |
7.01±0.08 |
14.29±0.06 |
|
Ash |
4.65±0.09 |
6.19±0.01 |
|
Energy (Kcal) |
474±1.06 |
363±0.87 |
|
Insoluble Dietary Fiber |
28.49±0.38 |
74.07±1.48 |
|
Soluble Dietary Fiber |
1.51±0.09 |
0.93±0.01 |
|
Total Dietary Fiber |
30±0.47 |
75±1.49 |
Table7: Amino Acid profile of Garden cress seed [71]
|
Non-essential amino acid |
g/100g protein |
Essential amino acid |
g/100g protein |
|
Aspartic Acid |
9.76±0.03 |
Histidine |
2.66±0.09 |
|
Glutamic Acid |
19.33±0.19 |
Threonin |
4.51±0.03 |
|
Serine |
4.96±0.09 |
Arginine |
8.04±0.03 |
|
Glycine |
- |
Valine |
5.67±0.02 |
|
Alanine |
- |
Metheonine |
0.97±0.02 |
|
Tyrosine |
- |
Phenyl Alanine |
5.65±0.03 |
|
Proline |
- |
Isoleucine |
5.11±0.03 |
|
|
|
Leucine |
8.21±0.01 |
|
|
|
Lysine |
6.26±0.39 |
|
|
|
Total (%) |
47.08 |
3.3 Ethnopharmacognosy of Lepidium sativum
Garden cress, or Lepidium sativum L., is a member of the Brassicaceae family and has been used in folk medicine and traditional medical systems such as Ayurveda to treat bone and joint disorders, especially osteoarthritis and fractures. Known locally as Sandhivata or Sandhishula, the seeds are traditionally used to treat joint pain, swelling, and stiffness. People often eat them as powders, pastes, or decoctions, and sometimes they are mixed with ghee or other herbal preparations [79].Ayurvedic clinical studies have shown that L. sativum can help with joint problems, showing a big improvement in osteoarthritis symptoms like pain, swelling, and limited movement [80]. Its analgesic and anti-inflammatory properties have been pharmacologically validated in various experimental models, where seed extracts significantly reduced pain and oedema, corroborating traditional claims in the treatment of arthritis [80]. Flavonoids, alkaloids, glucosinolates, phenolic acids, and fatty acids are examples of active phytoconstituents that help lower oxidative stress and inflammatory pathways linked to osteoarthritis these compounds have anti-inflammatory and antioxidant properties [81].The seeds are also full of important minerals like iron, calcium, and phosphorus, which help bones grow and strong [82].Preclinical studies and ethnopharmacological reports indicate that L. sativum seeds expedite fracture healing; administration of seed powder or extracts resulted in elevated osteocalcin levels, enhanced histological bone architecture, and augmented callus formation in rabbit and rat models [83].It is believed that this effect is due to the upregulation of bone regeneration markers, the stimulation of osteoblastic activity, and the promotion of bone matrix formation [84]. Furthermore, L. sativum supplementation demonstrated efficacy in enhancing bone mineral density and inhibiting bone loss in experimental osteoporotic models, suggesting its potential application in osteoporosis management [85] The plant has a lot of pharmacological benefits in addition to its musculoskeletal ones. These include hepatoprotective, galactagogue, antidiabetic, antioxidant, and gastroprotective properties, which show how flexible it is in ethnomedicine [86]. To ensure safety in long-term use, studies of herb drug interactions, toxicity assessment, and therapeutic dose standardization are still necessary, even though L. sativum seeds are generally accepted to be safe when consumed as food [87]. Hence, garden cress seeds have promising joint-healing and bone-strengthening potential, especially in the treatment of osteoarthritis and fractures, according to both traditional and experimental evidence. However, more clinical research and extract standardization are necessary to convert these traditional claims into scientifically validated therapies [88]. The leaves are used to treat vitamin C deficiency, cough, and asthma. They are also traditionally used as a diuretic, expectorant, and anti-scorbutic. [89] As a galactagogue, laxative, anti-inflammatory, and nutritional tonic, seeds are frequently used in traditional medicine, particularly to treat anemia and aid in digestion [90]. In traditional medicine, roots are used to treat digestive issues and as a mild stimulant and carminative [91]. Because of its calming and antimicrobial qualities, stem juice or paste is used ethnomedically to treat minor wounds and skin irritations. [92]
4.0 Lepidium sativum in osteoarthritis:
Because it reduces joint pain and Inflammation, garden cress (Lepidium sativum L.) has long been used in Ayurveda to treat Sandhivata (osteoarthritis) and other musculoskeletal conditions. Raval ND et al. conducted a thorough investigation of the plant's seeds to support this claim. A total of 98 patients were split up into two groups for this study. Chandrashura churna was administered to the trial drug group, while patients in the placebo group received starch-containing capsules for a month. The patients' cardinal signs and symptoms of Sandhivata were evaluated using scores based on their intensity, frequency, and duration both before and after treatment. According to the results, Chandrashura offers excellent relief from the following cardinal signs and symptoms: Aakunchan prasaranjanya vedana (difficulty in movement), Sparshashyata (tenderness), Sandhishula (joint pain), Sandhishotha (swelling), Sandhigraha (stiffness), and Sandhisphutana (crepitus). Thirty percent of the patients in this study experienced total remission, thirty-seven percent experienced marked improvement, twenty-five percent experienced moderate improvement, and seven percent did not experience any improvement [93]. Bioactive phytoconstituents, including flavonoids, alkaloids, glucosinolates, sterols, tannins, and phenolic acids, are abundant in the seeds and have been shown to have strong analgesic, antioxidant, and anti-inflammatory properties that are pertinent to the pathophysiology of osteoarthritis [94]. The reduction of synovial Inflammation and stiffness, which are frequently seen in osteoarthritic joints, is mainly ascribed to the down-regulation of inflammatory mediators such as prostaglandins, TNF-α, and IL-1β [95].Rich in flavonoids and phenolic compounds, seed extracts have strong antioxidant properties that are essential for scavenging reactive oxygen species and avoiding oxidative damage to extracellular matrix proteins and chondrocytes, two major processes in cartilage degeneration [96]. The effectiveness of Lepidium sativum seeds in the treatment of osteoarthritis was examined. There were two patient groups in the study. For 30 days, the drug group was given Lepidium sativum powder divided into two daily doses of 6 gm each, while the control group was given starch as a placebo. To find out if there were any improvements, assessments of osteoarthritis symptoms were carried out both before and after treatment.With 30% achieving full remission, 37.5% demonstrating substantial progress, and 25.5% reporting moderate progress, the results demonstrated that over three-quarters of patients in the medication group saw a significant improvement in their symptoms [97]. It has been demonstrated that the seeds hasten glucocorticoid-induced osteoporosis in rats. On the other hand, they have been shown to accelerate the healing of artificial fractures in rabbits' left femur midshaft. However, ovariectomized rats have not been used to study the seeds' anti-osteoporotic effects or the underlying mechanisms [98,99]. The traditional use of Lepidium sativum for symptomatic relief in osteoarthritis has been supported by experimental animal studies that have confirmed its analgesic and anti-inflammatory properties.In models like formalin- and carrageenan-induced inflammation, seed extracts significantly decreased paw oedema and pain [93]. In rabbit and rat fracture models, seed supplementation expedited callus formation, enhanced histological architecture, and increased calcium and phosphate deposition in regenerating bone, demonstrating the seeds' osteogenic and bone-healing properties alongside symptom management [100]. This osteoprotective effect suggests that Lepidium sativum may strengthen peri-articular bone and inhibit subchondral bone degradation, thereby expediting the progression of osteoarthritis (101). The seed's high nutritional value also helps keep joints healthy. It provides alpha-linolenic acid, calcium, phosphorus, magnesium, and iron, which are all important for mineralizing bones, feeding synovial fluid, and keeping cartilage flexible [100]. Omega-3 fatty acids and sterols in the fixed oil fraction also help control the production of eicosanoids, which lowers chronic inflammation in joint tissues [93]. Also, its protein and amino acid makeup helps make collagen and proteoglycans, which makes cartilage stronger and helps it heal [93].. Because of its analgesic and anti-inflammatory qualities as well as its high Ca²⁺ ion concentration, Lepidium sativum has been proposed as a potential supplement to existing osteoarthritis treatment plans. Because all patients in both groups received the elimination of causative factors, only a small percentage of patients in the control group showed improvement [100]. Garden cress is a multipurpose substance that can treat osteoarthritis pain, Inflammation, oxidative stress, and bone weakness all at once thanks to these interconnected biochemical and nutritional processes [101]
CONCLUSION
Garden cress, or Lepidium sativum, is a promising herbal remedy that has several advantages for bone and joint health, especially in the treatment of osteoarthritis. Chronic Inflammation, oxidative stress, cartilage degradation, and subchondral bone remodeling are among the primary pathological mechanisms of osteoarthritis that are addressed by the special anti-inflammatory, antioxidant, analgesic, and osteogenic qualities of its seeds.
Chandrashura, or garden cress, has been identified in traditional Ayurvedic literature as an effective treatment for Sandhivata. This assertion is now substantiated by growing pharmacological and preclinical evidence that validates the plant's efficacy in alleviating pain and stiffness while facilitating bone repair. The seed's rich nutritional profile, which includes high levels of omega-3 fatty acids, calcium, phosphorus, and phenolic compounds, further supports its therapeutic function by supporting cartilage, improving joint lubrication, and strengthening peri-articular bone. Despite promising results in vitro and in vivo, there is still a lack of clinical validation through well-planned randomized controlled trials. Future research should focus on elucidating its specific molecular targets, enhancing dosage and formulation (such as oil-based preparations or standardized extracts), and evaluating its synergistic effects with other anti-arthritic medications or nutraceuticals. Moreover, advancements in phytopharmacology and nanotechnology may enable the formulation of novel delivery systems for its active constituents, thereby enhancing their bioavailability and specificity of action within joint tissues. In modern integrative medicine, Lepidium sativum seeds exhibit significant potential as a supplementary or adjunctive therapy for osteoarthritis and other degenerative bone and joint conditions, owing to their safety, cost-effectiveness, and robust ethnopharmacological foundation.
CONFLICT OF INTEREST
The authros declare no conflict of interest Associated with the present work
REFERENCES

Ishori Chhetry, Sourav Kumar, Mohd. Akhlad, Neha Sagar, Osteoarthritis: Epidemiology and the Role of Lepidium sativum in its Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2028-2046. https://doi.org/10.5281/zenodo.20595144
 10.5281/zenodo.20595144
10.5281/zenodo.20595144