
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Chemistry, Government Degree College, Tekkali 532201, Andhra Pradesh, India.
Phospholipids are fundamental components of biological membranes and play essential roles in cellular structure, signalling, and metabolism. Beyond their structural functions, phospholipids have emerged as promising therapeutic agents due to their biocompatibility, amphiphilic nature and ability to interact with biological membranes. Enzymes involved in phospholipid biosynthesis and remodelling, such as choline kinase ?, phospholipases, sphingosine kinases, and lyso-phosphatidylcholine acyltransferases, have emerged as promising targets for anticancer therapy. Inhibition of these enzymes disrupts membrane synthesis, oncogenic signalling pathways, and tumour cell survival, thereby providing novel opportunities for targeted intervention. This article summarises the most common cancer therapeutic uses of dietary phospholipids and provides an overview of their approved and proposed benefits. Furthermore, the roles of different phospholipid molecules in regulating health span and life span, as well as their potential mechanisms of action, were discussed.
Phospholipids (PL) are a class of lipids that are major components of cell membranes. In biological systems, phospholipids play significant roles in maintaining cellular integrity, cell signalling, membrane fluidity, and transporting molecules across membranes [1]. The brain contains the highest content of PLs in comparison to other organs. Classification of PLs was represented in Figure (1). Phosphatidylcholine (PC), phosphatidyl ethanolamine (PE) and phosphatidylserine (PS) are critical components of biological membranes, forming a fluid lipid bilayer that serves to maintain the structural integrity and selective permeability of cells. Phospholipids have numerous functions in cell division, autophagy, and apoptosis and serve as second messengers, protein chaperones, and receptors for the recruitment of membrane-bound proteins [2]

Figure 1: Classification of Phospholipids
1.1 Phospholipids in Cellular Physiology:
PLs are amphiphilic molecules comprising of a hydrophilic head region formed of a negatively charged phosphate group, two hydrophobic tails formed of long-chain fatty acids and a glycerol or alcohol group that links the head and tail areas [3]. This structure allows Phospholipids to form bilayers in cell membranes, providing structural integrity and regulating the passage of substances in and out of cells. These unique properties make phospholipids most appropriate to be employed as important pharmaceutical excipients, and they have a very wide range of applications in drug delivery systems [4]. Owing to their amphiphilic nature, phospholipids are multipurpose excipients that can be used in oral formulations as emulsifiers, wetting agents, solubilisers, and a liposome former. Besides, they can be used as a matrix material for solid dispersions and slow-release tablet formulations [5].
1.2 Phospholipids as a Diagnostic and Therapeutic Target :
Many phospholipid-based liposomal formulations have reached the market, including Doxil®, Myocet®, Daunoxome®, etc. [6]. Phospholipids are categorised as Generally Regarded As Safe (GRAS) by the United States Food and Drug Administration. They have very low toxicity and can therefore be suitable for all the routes of administration. Phospholipids were useful to overcome several challenges that hampered the therapeutic potential of conventional drug delivery systems. The majority of the studies indicate that dietary PLs have a positive impact on several diseases, apparently without severe side effects. Furthermore, they were shown to reduce the side effects of some drugs [7]. Phospholipids have been extensively studied for their potential in the prevention and management of chronic diseases, including cancer, cardiovascular disease, diabetes, and neurodegenerative disorders. In cancer treatment and management, Plant-based phospholipid (PPs) liposomes enable targeted drug delivery as they enhance the permeability and retention (EPR) effect in the cancer cells [8].
Phospholipids can be obtained from naturally occurring materials such as eggs, bovine brain, soybean, sunflower, rapeseed, cottonseed, etc. [9]. PPs are a diverse lipid group that have suitable structures for applications in various fields, including drug delivery, food processing and cosmetics [10]. Altered phosphatidylcholine and phosphatidylethanolamine membrane content, phospholipid metabolite levels, and fatty acid profiles are frequently identified as hallmarks of cancer development and progression. Phosphatidylcholine and phosphatidylethanolamine are two phospholipids that comprise the majority of cell membranes. De novo biosynthesis of phosphatidylcholine and phosphatidylethanolamine occurs via the Kennedy pathway, and perturbations in the regulation of this pathway are linked to a variety of human diseases, including cancer [11]. Abnormal choline metabolism drives cancer cell growth, survival, proliferation, and resistance to therapies. Controlling lipid metabolism represents a promising strategy toward cancer control and treatment by interference with PC metabolism [12].
2. PHOSPHOLIPID-BASED DRUG DELIVERY SYSTEMS
2.1 Overview of Cancer :
Cancer is characterised by the uncontrolled proliferation of cells resulting from the accumulation of genetic mutations and dysregulation of signalling pathways that govern cellular growth, survival, and proliferation. The complexity of cancer cells at both the genetic and phenotypic levels underlies their clinical heterogeneity and resistance to therapy. Chemotherapy is the most commonly used treatment among a variety of approaches currently being used for the treatment of cancer. The conventional treatment of cancer, such as chemotherapy, is highly prone to non-specific toxicity, in addition to limited drug targeting and rapid drug clearance. These challenges not only intensified side effects but also hindered the therapeutic effectiveness of the treatment. Personalised targeting strategies further improved therapeutic precision and minimised off-target effects [13].
2.2 Plant-based phospholipid (PP) liposomes in Cancer Management :
Liposomes are adaptable drug-delivery vehicles that can also be chemically engineered to improve targeting specificity and therapeutic efficacy for cancer. Moreover, these liposomes can evade rapid clearance by the immune system, extending their circulation time and enhancing accumulation in tumour tissues through the EPR effect. This targeted delivery strategy reduces the need for higher drug doses, thereby limiting systemic toxicity and side effects, improving treatment tolerance [14]. The usage of Plant-based phospholipid (PP) liposomes can address various conventional challenges, including drug resistance, toxicity, overdose, and off-target effects. Phospholipids are synthesised naturally in both animals and plants; however, PPs are evident as a sustainable and eco-friendly alternative to animal-derived phospholipids [15].
Plant-based phospholipid liposomes (PPL) are sustainable and biocompatible carriers with advantages over synthetic and animal-derived lipids, including lower immunogenic risk and available from sources such as soy, sunflower, and canola. The structural resemblance of phospholipid bilayers to native cellular membranes facilitates efficient interaction with cancer cells, enabling targeted delivery and enhanced accumulation of therapeutic agents within the tumour microenvironment [16,17]. PPLs offer an innovative and environmentally sustainable approach to cancer treatment, with demonstrated preclinical benefits in both efficacy and safety. Different Types of Liposomal Drug Delivery Systems and Compositions were presented in Table 1.
Table 1: Liposomal Drug Delivery Systems and Composition.
|
Liposomal Drug |
Active Drug |
Lipid Composition* |
Liposome Type |
Major Indication |
|
Doxil / Caelyx |
Doxorubicin |
HSPC, Cholesterol, MPEG-DSPE |
PEGylated liposome |
Ovarian cancer, Kaposi's sarcoma, multiple myeloma |
|
DaunoXome |
Daunorubicin |
DSPC, Cholesterol |
Conventional liposome |
Kaposi's sarcoma |
|
Myocet |
Doxorubicin |
EPC, Cholesterol |
Non-PEGylated liposome |
Metastatic breast cancer |
|
Marqibo |
Vincristine |
Sphingomyelin, Cholesterol |
Conventional liposome |
Acute lymphoblastic leukemia |
|
Vyxeos |
Daunorubicin + Cytarabine |
DSPC, DSPG, Cholesterol |
Dual-drug liposome |
Acute myeloid leukemia |
|
Onivyde |
Irinotecan |
DSPC, Cholesterol, MPEG-DSPE |
PEGylated liposome |
Metastatic pancreatic cancer |
|
Mepact |
Mifamurtide |
POPC, OOPS |
Multilamellar liposome |
Osteosarcoma |
|
Lipusu |
Paclitaxel |
Lecithin, Cholesterol |
Conventional liposome |
Lung, ovarian, breast cancers |
2.3 Mechanism of Drug Delivery:
Phospholipid-based systems, particularly liposomes, offer a solution by improving drug encapsulation, protecting the drug from degradation, and enabling targeted delivery directly to cancerous cells [18]. PP liposomes co-loaded with chemotherapeutics exhibited synergistic anticancer effects, increased tumour accumulation, and reduced systemic toxicity. Phospholipids possess amphiphilic properties, comprising hydrophilic head groups and hydrophobic fatty acid tails, which drive their spontaneous self-assembly into bilayers and facilitate liposome formation in aqueous environments. Liposomes serve as versatile drug delivery systems owing to their membrane-like structure, which is typically composed of biocompatible phospholipids, sphingolipids, cholesterol, and hydrophilic polymers [19]. These characteristics are essential for encapsulating and delivering active ingredients to specific targets. In drug delivery systems, phospholipids enhance the pharmacokinetic properties of drugs by improving their stability and bioavailability while promoting controlled release and increased therapeutic efficacy [20].
The bilayer can encapsulate hydrophilic drugs in the aqueous core and hydrophobic drugs within the lipid membrane [21]. The composition of liposomes can be tailored to enhance their stability, release profiles, and targeting abilities [22]. PPs’ composition contains mainly phosphatidylcholine (PC), phosphatidylethanolamine (PE), and other minor components such as phosphatidylserine (PS) to provide a chemical handle (e.g., a primary amine or carboxylic acid) that can be used to perform covalent crosslinking (e.g., amide linkages). The size of liposomes typically ranges from 50 nanometers to several micrometres, affecting their biodistribution and cellular uptake [23]. The most common phospholipid component of liposomes is 2-distearoyl-sn-glycerophosphocholine (DSPC). The chemical structure of DSPC is presented in Figure 2.
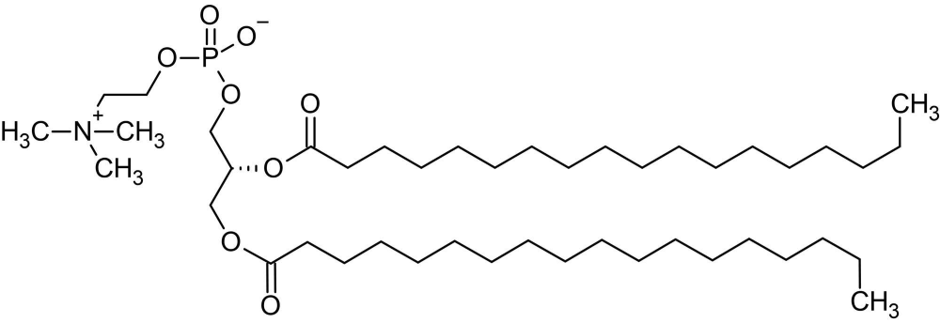
Figure. 2: Chemical structure of DSPC (2-distearoyl-sn-glycerophosphocholine)
One additional benefit of liposomal delivery systems in cancer therapy is their potential to penetrate the blood–brain barrier (BBB), a protective layer that often restricts drug access to the brain, thus hindering treatment for brain tumours and metastases. Phospholipids employed in liposomal formulations are capable of encapsulating both hydrophobic and hydrophilic anticancer drugs, improving their stability during systemic circulation and promoting targeted delivery to cancerous tissues [24]. Particularly in Breast Cancer treatment, liposomal encapsulation of chemotherapeutic agents such as doxorubicin (Figure 3) has been shown to increase drug accumulation within tumour tissues while minimising exposure to normal or healthy cells [25].
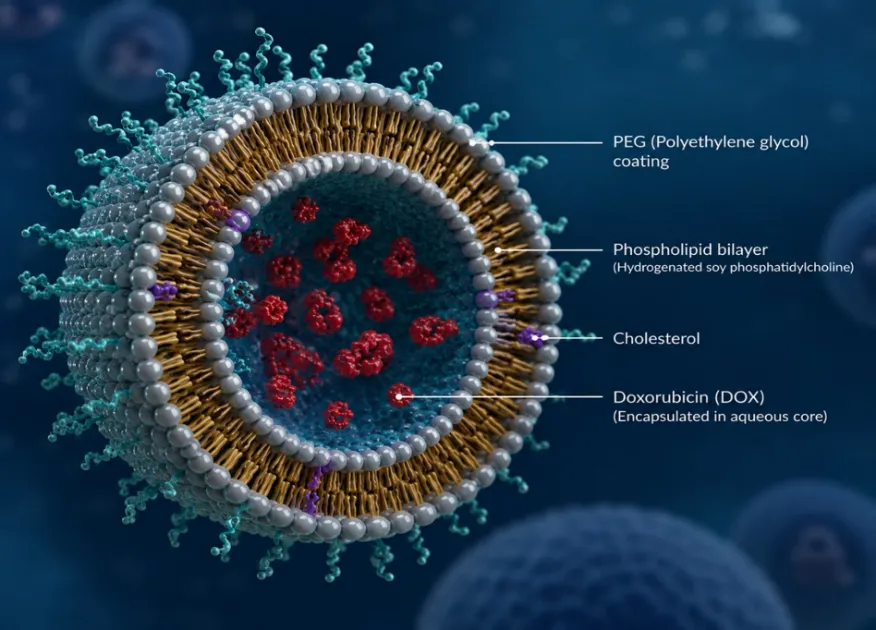
Figure. 3: Liposomal encapsulation of chemotherapeutic agent Doxorubicin
At the molecular level, PPs improve drug encapsulation, stability, and targeted intracellular delivery, increasing uptake by cancer cells and greater endosomal escape, leading to enhanced DNA intercalation and apoptosis [26, 27, 28]. Liposomal drug delivery systems have gained significant attention as an effective approach for enhancing the targeted delivery of anticancer agents [29]. By leveraging the distinctive expression patterns of cell surface receptors, these delivery systems facilitate targeted drug uptake by tumour cells, thereby improving drug accumulation, overcoming therapeutic resistance, and enhancing treatment efficacy [30]. One of the most notable examples is Doxil, a pegylated liposomal formulation of doxorubicin, which has been successfully utilised in the treatment of breast cancer [31-36]. Studies have demonstrated that Liposomal Doxil significantly reduces the cardiotoxicity associated with free doxorubicin while maintaining efficacy in tumour reduction.
3. PHOSPHOLIPIDS AS BIOMARKERS IN CANCER DIAGNOSIS
The potential for phospholipids to serve as biomarkers for diagnostics or as anticancer therapy targets was discussed. According to the National Cancer Institute, a biomarker is defined as "a biological molecule found in blood, other bodily fluids, or tissues that is indicative of a normal or abnormal process, or of a condition or disease”. Lipid profile may be considered a crucial prognostic factor in cancer patients. Quantitative changes in lipids are observed in all neoplastic cells as compared to non-malignant cells. Therefore, some lipids (e.g. phosphatidylcholine) may be considered as tumour markers in certain malignancies. Changes in membrane lipid production are frequently linked to the dysregulation of cellular signalling pathways, resulting in metabolic reprogramming that supports tumour progression. Variations in membrane lipid profiles between healthy and malignant cells offer a promising basis for the design of targeted therapies that enhance the efficacy of chemotherapeutic agents and counteract multidrug resistance. Concentrations of the two major phospholipid components, phosphatidylcholine (PC) and phosphatidylethanolamine (PE), increased with increasing breast cancer tumour grade [(37], indicating that the phospholipid synthesis rate increases with oncogenesis and tumour progression as compared to normal tissue.
3.1 Choline Kinase α (CKα) :
Choline Kinase Alpha(CKα) is well established as an oncogene that promotes tumour initiation and progression [38, 39, 40]. Its overexpression and elevated enzyme activity are one of the most established factors that contribute to increased PC in various tumour tissues, including breast, ovarian, colorectal, prostate, lung and pancreatic cancers [41]. Phospholipid abnormalities are detectable during the initial stages of disease progression, and alterations in the expression of critical genes regulating phospholipid synthesis may serve as prognostic indicators of patient survival [42,43]. Increased expression and activity of CKα are associated with increased proliferation and malignancy and are an indicator of patient survival in Non-Small Cell Lung Cancer (NSCLC) [44]. In early-stage NSCLC, patients with higher CKα had a greater risk of death compared to patients with lower CKα, who demonstrated improved survival [45].
3.2 De novo biosynthesis via the Kennedy pathway:
De novo biosynthesis of phosphatidylcholine and phosphatidylethanolamine occurs via the Kennedy pathway ( Figure.4), and perturbations in the regulation of this pathway are linked to a variety of human diseases, including cancer. Altered phosphatidylcholine and phosphatidylethanolamine membrane content, phospholipid metabolite levels, and fatty acid profiles are frequently identified as hallmarks of cancer development and progression. Choline and ethanolamine are nutrients obtained through diet. The main fate of these nutrients is to enter the phospholipid Kennedy pathway, which is responsible for the de novo synthesis of PC and PE. The phosphatidylcholine (PC) and phosphatidylethanolamine (PE) branches of the Kennedy pathway are referred to as the Cytidine Diphosphate Choline (CDP-choline) and Cytidine Diphosphate Ethanolamine (CDP-ethanolamine) pathways, respectively. In these pathways, choline and ethanolamine are converted into PC and PE through a series of analogous enzymatic reactions involving phosphorylation, cytidylyltransferase-mediated activation, and phosphotransferase-catalysed lipid synthesis [46-49].
3.3 Prognostic Significance of Phospholipid Biomarkers :
PC Metabolism and CKα are elevated in Cancers. Elevated PC metabolism is an important hallmark of cancer [50,51]. Activated choline metabolism is associated with breast cancer malignancy and tumour progression, and differences in PC metabolite levels could be detected in early carcinogenesis [52]. Glycerophosphocholine (GPC) is the predominant choline-containing metabolite in normal cells; however, a metabolic shift toward phosphocholine (PCho) as the dominant metabolite is observed in both immortalised and oncogene-transformed cells. Elevated phosphocholine levels are a hallmark of malignant transformation and reflect increased choline metabolism. In colorectal cancer, phosphatidylcholine (PC) levels are generally increased, with the species PC(16:0/16:1) showing a particularly marked elevation in advanced stages of the disease. Cancer prognostic summary of the phospholipid enzymes was presented in Table 2.
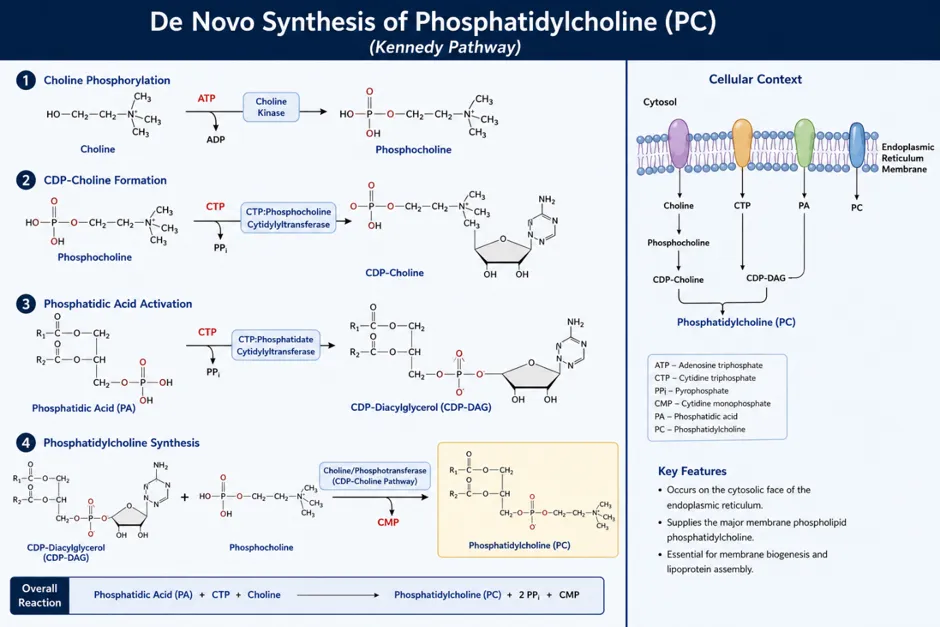
Figure 4: De novo biosynthesis of Phosphatidylcholine
Table 2: Cancer prognostic summary of the Phospholipid Enzymes
|
Enzyme |
Phospholipid Target/Function |
Cancer Types Associated |
Prognostic Significance |
Clinical Outcome |
|
Choline Kinase α (CHKA) |
Converts choline to phosphocholine in phosphatidylcholine synthesis |
Breast, lung, colorectal, prostate, ovarian cancers |
Frequently overexpressed |
Associated with poor prognosis, increased proliferation, invasion, and metastasis |
|
Phospholipase D1 (PLD1) |
Hydrolyzes phosphatidylcholine to phosphatidic acid |
Breast, gastric, renal, colorectal cancers |
Elevated expression correlates with aggressive disease |
Reduced overall survival and increased metastatic potential |
|
Phospholipase D2 (PLD2) |
Generates phosphatidic acid from phosphatidylcholine |
Breast, melanoma, colorectal cancer |
High expression linked to tumor progression |
Poor prognosis and enhanced cell migration |
|
Phospholipase Cγ1 (PLCγ1) |
Hydrolyzes PIP2 into DAG and IP3 |
Breast, colorectal, gastric cancers |
Overexpression associated with invasion and metastasis |
Shortened disease-free survival |
|
Cytosolic Phospholipase A2 (cPLA2α) |
Releases arachidonic acid from membrane phospholipids |
Lung, breast, colorectal, pancreatic cancers |
Elevated activity promotes inflammation and tumor growth |
Associated with unfavorable prognosis |
|
Lipoprotein-associated Phospholipase A2 (Lp-PLA2) |
Hydrolyzes oxidized phospholipids |
Prostate and breast cancers |
Increased expression linked to tumor aggressiveness |
Correlates with disease progression |
|
Sphingosine Kinase 1 (SPHK1) |
Produces sphingosine-1-phosphate (S1P) |
Breast, lung, gastric, colorectal cancers |
Strong overexpression in advanced tumors |
Poor overall survival and treatment resistance |
|
Sphingosine Kinase 2 (SPHK2) |
Generates S1P in nucleus and mitochondria |
Leukemia, breast, liver cancers |
Variable role depending on tumor type |
Often associated with poor survival |
|
Acid Sphingomyelinase (ASM) |
Converts sphingomyelin to ceramide |
Glioblastoma, leukemia, melanoma |
Reduced expression frequently observed |
Low levels associated with therapy resistance |
|
Neutral Sphingomyelinase 2 (nSMase2) |
Produces ceramide from sphingomyelin |
Breast cancer, leukemia |
Generally acts as tumor suppressor |
Higher expression often predicts better outcome |
|
Phosphatidylserine Synthase 1 (PSS1) |
Catalyzes phosphatidylserine synthesis |
Various solid tumors |
Altered expression affects membrane remodeling |
Potential marker of tumor progression |
|
Lysophosphatidylcholine Acyltransferase 1 (LPCAT1) |
Remodels phosphatidylcholine via Lands cycle |
Prostate, lung, gastric, liver cancers |
Frequently overexpressed |
Poor prognosis and enhanced tumor growth |
|
Autotaxin (ENPP2) |
Converts lysophosphatidylcholine to lysophosphatidic acid |
Breast, ovarian, thyroid, glioblastoma |
Elevated expression predicts aggressive disease |
Reduced survival and increased metastasis |
|
Lipid Phosphate Phosphatase 3 (LPP3/PPAP2B) |
Degrades lysophosphatidic acid |
Breast, colon cancers |
Often downregulated |
Loss associated with tumor progression and poor prognosis |
Phosphocholine, which is a substrate for PC synthesis and a product of PC metabolism by various phospholipases, is increased in advanced tumours and may serve as an indicator of tumour grade. CKα, which produces phosphocholine from choline, is overexpressed in most cancers, and increased CKα levels lead to increased phosphocholine and cancer progression [53]. Overexpression of CKα causes a more aggressive cancer phenotype, increased invasion, and drug resistance in breast cancer cells [54]. Analysis of PEMT in lung cancer tissues relative to adjacent non-cancer lung tissues revealed that greater PEMT expression ratios were associated with shorter patient survival. The deceased patients were also found to have a 32% higher PEMT expression ratio compared to surviving patients [55].
3.4 Targeting of Phospholipid Metabolism- Enzyme inhibitors :
CKα has been extensively studied as a target for cancer therapies, and several CKα inhibitors with antitumor activity have been identified. For example, the novel small molecule, 1,1′-(1,12-Dodecanediyl)bis[4-(dimethylamino) pyridinium] dibromide (ICL-CCIC-0019) inhibits growth and reduces cell survival in several cancer cell lines, and suppresses tumour xenograft growth in mice . siRNA-mediated suppression of CKα expression promotes apoptotic cell death in diverse cancer cells while reducing the proliferative capacity of breast cancer cells. In addition, in MDA-MB-231 tumour-bearing mice, the use of direct (H89) and indirect CKα inhibitors (sorafenib) decreased choline content, demonstrating the effectiveness of these treatments in vivo [56,57].
PCYT2 has also been proposed as a target for novel cancer therapies. Meclizine, a direct inhibitor of PCYT2, is a potential anticancer drug when used in conjunction with the phosphofructokinase (PFKFB3) inhibitor PFK158. This renders cells more susceptible to meclizine-induced cytotoxicity, as inhibition of PCYT2 leads to an accumulation of phosphoethanolamine, which in turn disrupts the mitochondrial electron transport chain and thus inhibits mitochondrial oxidative phosphorylation [103]. In a human hepatocarcinoma cell xenotransplantation model, the combination of PFK158 and meclizine reduced liver tumours [58]. Cancer drugs and their phospholipid enzyme targets were presented in Table 3.
Table 3: Cancer Drug Inhibitors Targeting Phospholipid Enzymes
|
Target Enzyme |
Drug/ Inhibitor |
Mechanism of Action |
Cancer Types Studied |
Therapeutic Effect |
|
Choline Kinase α (CHKA) |
TCD-717, MN58b |
Blocks phosphorylation of choline → reduces phosphatidylcholine synthesis |
Breast, lung, colon cancer |
Induces apoptosis, reduces membrane synthesis, anti-proliferative |
|
Phospholipase D1/2 (PLD1/PLD2) |
FIPI |
Inhibits PLD-mediated phosphatidic acid production |
Breast, prostate, melanoma |
Reduces mTOR signaling, inhibits invasion & metastasis |
|
Phospholipase C (PLCγ1) |
U73122 |
Inhibits PLC-mediated PIP2 hydrolysis |
Breast, gastric cancer |
Blocks Ca²⁺ signaling and tumor cell migration |
|
Cytosolic Phospholipase A2 (cPLA2α) |
AACOCF3, Pyrrophenone |
Prevents arachidonic acid release → reduces eicosanoid signaling |
Lung, colorectal, breast cancer |
Anti-inflammatory, anti-tumor growth |
|
Sphingosine Kinase 1 (SPHK1) |
PF-543 |
Blocks formation of sphingosine-1-phosphate (S1P) |
Breast, colon, lung cancer |
Promotes apoptosis, reduces angiogenesis |
|
Sphingosine Kinase 2 (SPHK2) |
ABC294640 (Opaganib) |
Inhibits S1P production in nucleus/mitochondria |
Liver cancer, leukemia, prostate cancer |
Induces autophagy & apoptosis |
|
Autotaxin (ENPP2) |
GLPG1690 (Ziritaxestat) |
Blocks LPA production from LPC |
Breast, ovarian, glioblastoma |
Reduces metastasis, tumor migration |
|
Lysophosphatidylcholine Acyltransferase (LPCAT1) |
Experimental inhibitors (no FDA-approved drug) |
Disrupts phosphatidylcholine remodeling (Lands cycle) |
Prostate, lung cancer |
Reduces proliferation & lipid membrane remodeling |
|
Acid Sphingomyelinase (ASM) |
Functional inhibitors (FIASMAs: fluoxetine, imipramine) |
Inhibits ceramide generation pathway |
Glioblastoma, leukemia |
Alters apoptosis signaling |
|
Neutral Sphingomyelinase (nSMase) |
GW4869 |
Blocks ceramide production |
Breast cancer, leukemia |
Modulates exosome formation, reduces tumor growth |
|
Phosphatidylserine externalization pathway |
Bavituximab |
Targets tumor cell membrane PS exposure |
Solid tumors |
Immune-mediated tumor killing |
|
Lysophosphatidic acid receptor (LPAR) |
Ki16425, AM095 |
Blocks LPA receptor signaling |
Breast, ovarian cancer |
Reduces migration and invasion |
3.5 Phosphoethanolamine derivatives :
The PE precursors, ethanolamine and phosphoethanolamine, have been gaining interest for their antitumor activity [59]. Studies have shown that synthetic phosphoethanolamine (Pho-s) is effective against multiple cancer cell types, including Ehrlich ascites tumour, renal carcinoma, and breast cancer cells, highlighting its potential as an anticancer agent [60]. While the mechanism of action of Pho-s remains unclear, this agent has been found to have anti-proliferative activity, anti-metastatic activity, and does not exhibit cytotoxic effects on normal cells. Pho-s inhibits tumour growth and prolongs survival in Ehrlich ascites tumour-bearing mice [61] and melanoma-bearing mice [62]. The development of a non-toxic ethanolamine derivative yielded promising antitumor effects, as evidenced by significant tumour size reduction in prostate xenograft mice after four weeks of treatment and in colon xenograft mice after two weeks of treatment.
Novel CKα inhibitors, including EB-3D and EB-3P, have demonstrated significant anticancer activity in preclinical studies [63]. These compounds effectively suppressed cancer cell proliferation and exhibited promising therapeutic potential [64,65]. Among the CKα inhibitors evaluated, RSM932A showed the most pronounced in vivo antitumor activity, significantly inhibiting tumour growth in mouse xenograft models without causing detectable toxicity [66].
3.6 Phosphatidylserine-targeting therapies :
Phosphatidylserine (PS) on the outer membrane of tumour cells can be used as an effective target for cancer therapy. Targeting phosphatidylserine with agents such as bavituximab and the peptide–peptoid hybrid PPS1D1 has been shown to induce significant cytotoxicity in cancer cells, highlighting the therapeutic potential of PS-directed strategies [67]. For example, a cationic liposomal carrier, phosphatidylcholine-stearylamine (PC-SA), strongly binds and kills cancer cells through direct interaction with negatively charged surface-exposed PS. The anticancer properties of drugs like camptothecin and doxorubicin entrapped in PC-SA liposomes were demonstrated on cancer cell lines, both in vitro and in different mouse models [68]. (Figure.5)
Duramycin is a small tetracyclic peptide produced by the bacterium Streptoverticillium cinnamoneus and is closely related to cinnamycin produced by Streptomyces sp.. Both duramycin and cinnamycin are capable of binding to PE specifically in areas of membrane with high curvature, inducing trans-bilayer phospholipid movements that lead to cell death [69]. Another group of interesting molecules are cyclotides, cyclic peptides that exert their biological activities by acting on the cell membrane, binding to phospholipids containing PE headgroups. This binding is followed by membrane disruption and cell death. The increased levels of exposed PE on the outer membrane of cancer cells allow those membrane-active peptides to exert their cytotoxic effects without harming healthy cells [70].
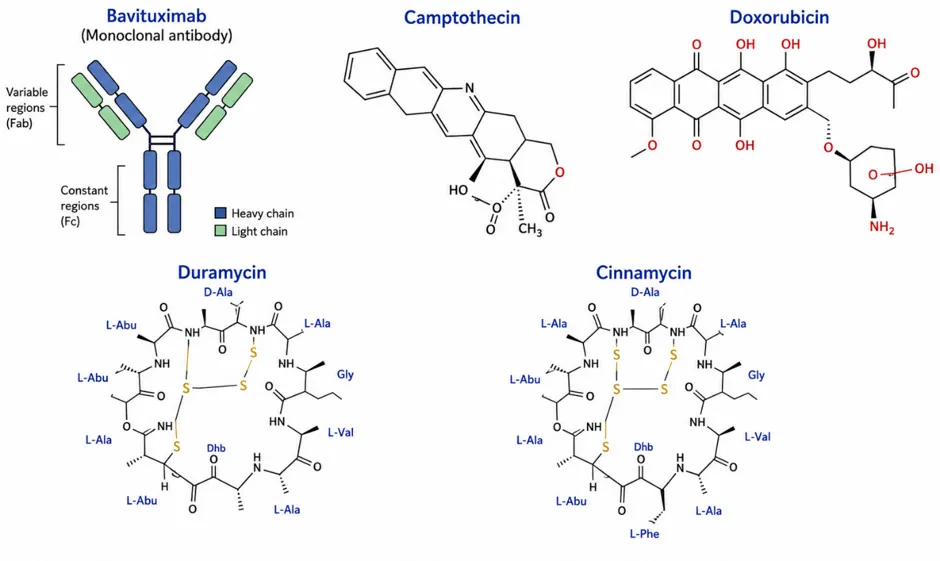
Figure. 5: Chemotherapeutic Agents for Cancer Treatment
CONCLUSION:
The unique biochemical properties of phospholipids have enabled their application as both therapeutic targets and drug delivery platforms in cancer management. Phospholipids are essential structural and functional components of cellular membranes that play critical roles in membrane integrity, signal transduction, energy metabolism, and cell survival. Growing evidence indicates that alterations in phospholipid metabolism are closely associated with cancer initiation, progression, metastasis, and therapeutic resistance. In addition to their therapeutic significance, phospholipids and their metabolites serve as valuable diagnostic and prognostic biomarkers. Dysregulated pathways involving phosphatidylcholine, phosphatidylethanolamine, phosphatidylserine, sphingomyelin, and their metabolising enzymes contribute to the metabolic reprogramming that characterises malignant cells.
Biomarkers derived from phospholipid metabolic pathways offer a non-invasive approach for improving diagnostic accuracy and personalised treatment strategies. Clinically approved liposomal formulations such as liposomal doxorubicin and irinotecan have demonstrated the successful translation of phospholipid-based technologies into cancer therapy. In conclusion, phospholipids represent a versatile and rapidly evolving area in oncology, serving as both diagnostic indicators and therapeutic tools. Their multifaceted roles in cancer biology, coupled with ongoing innovations in phospholipid-targeted therapies and delivery systems, position them as key contributors to the development of more effective, selective, and patient-centered approaches for cancer management.
REFERENCES


Periyala. V. N. Acharyulu, B. Satish Kumar, V. Luke Paul, Phospholipids as Therapeutic and Diagnostic Tools in Cancer Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 5828-5843. https://doi.org/10.5281/zenodo.20806454
 10.5281/zenodo.20806454
10.5281/zenodo.20806454