Psoriasis is a chronic, immune-mediated inflammatory skin disorder characterized by abnormal keratinocyte proliferation and dysregulated immune responses involving cytokines such as tumor necrosis factor-alpha (TNF-?), interleukin (IL)-17, and IL-23. Conventional therapies, including topical corticosteroids, systemic agents, biologics, and phototherapy, are effective in disease management but are often associated with adverse effects during long-term use. Consequently, increasing attention has been directed toward plant-based therapies as safer and complementary treatment options. This systematic review aims to evaluate the efficacy and safety of medicinal plants used in the management of psoriasis. Relevant literature was collected from published scientific articles, review papers, and clinical studies focusing on herbal interventions for psoriasis. Various medicinal plants including Mahonia aquifolium (Oregon grape), Aloe barbadensis (Aloe vera), Curcuma longa (Turmeric), Azadirachta indica (Neem), Allium sativum (Garlic), Nigella sativa (Black cumin), and Glycyrrhiza glabra (Liquorice) demonstrated anti-inflammatory, antioxidant, immunomodulatory, and antiproliferative activities that may contribute to the reduction of erythema, scaling, itching, and plaque formation. Several studies reported improvements in Psoriasis Area and Severity Index (PASI) scores and symptom control with herbal formulations. The findings suggest that plant-derived therapies possess significant potential as adjunctive or alternative approaches for psoriasis management. However, further well-designed clinical trials are required to establish their long-term efficacy, safety, and therapeutic standardization.
Psoriasis is a chronic, immune-mediated, inflammatory skin disorder characterized by excessive proliferation and abnormal differentiation of keratinocytes, resulting in the formation of erythematous, scaly plaques on the skin. It affects approximately 2-4% of the global population and significantly impacts the quality of life of affected individuals. The disease is multifactorial in nature and develops through a complex interaction of genetic susceptibility, immune dysregulation, and environmental triggers. Although psoriasis is primarily recognized as a dermatological condition, it is now considered a systemic inflammatory disease associated with several comorbidities, including psoriatic arthritis, cardiovascular diseases, metabolic syndrome, obesity, inflammatory bowel disease, and psychological disorders such as anxiety and depression.
The pathogenesis of psoriasis involves activation of dendritic cells and T-lymphocytes, leading to the release of pro-inflammatory cytokines including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-17, IL-23, and IL-22. These cytokines stimulate keratinocyte hyperproliferation and chronic inflammation, resulting in the characteristic psoriatic lesions. The disease follows a relapsing-remitting course, with periods of exacerbation and remission influenced by factors such as infections, stress, smoking, alcohol consumption, obesity, trauma, and certain medications. Clinically, psoriasis manifests in several forms including plaque psoriasis, guttate psoriasis, inverse psoriasis, pustular psoriasis, erythrodermic psoriasis, and nail psoriasis. Among these, plaque psoriasis is the most common subtype, accounting for nearly 80-90% of all cases. The severity of psoriasis is commonly assessed using the Psoriasis Area and Severity Index (PASI), Body Surface Area (BSA), and Dermatology Life Quality Index (DLQI).
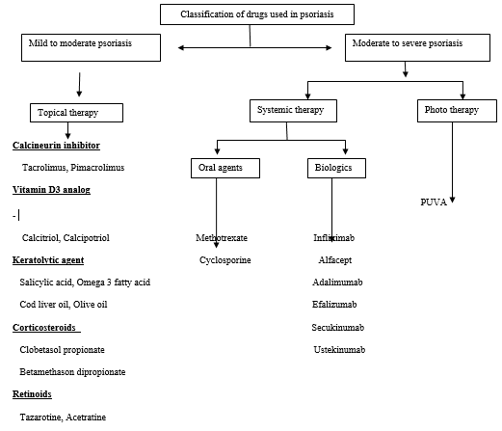
Current treatment strategies include topical therapies, phototherapy, systemic agents, and biologic drugs. Commonly used medications include corticosteroids, vitamin D analogues, methotrexate, cyclosporine, retinoids, and biologics targeting TNF-α, IL-17, and IL-23 pathways. Although these therapies are effective in controlling symptoms, long-term treatment is often associated with adverse effects, high costs, treatment resistance, and disease recurrence.
Consequently, there has been growing interest in plant-based therapeutic approaches for psoriasis management. Medicinal plants have been utilized for centuries in traditional systems of medicine due to their anti-inflammatory, antioxidant, immunomodulatory, and wound-healing properties. Numerous phytoconstituents such as curcumin, berberine, aloin, glycyrrhizin, allicin, and thymoquinone have demonstrated promising anti-psoriatic activities through modulation of inflammatory pathways and inhibition of keratinocyte proliferation.
The present systematic review aims to evaluate the efficacy and safety of medicinal plants and their bioactive constituents in the management of psoriasis. Furthermore, this review highlights the pharmacological mechanisms, therapeutic potential, and clinical evidence supporting the use of herbal therapies as complementary or alternative treatment options for psoriasis.
Types of psoriasis
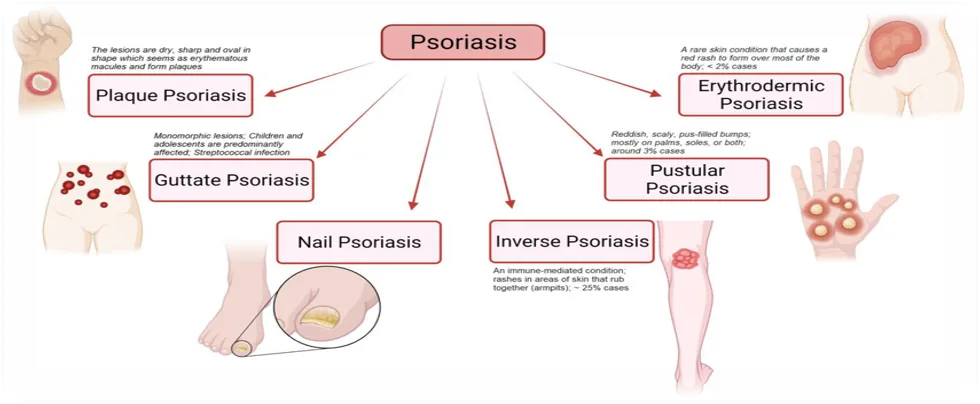
Fig. 1: Types of Psoriasis
There are various types of psoriasis like plaque psoriasis, guttate psoriasis, nail psoriasis, inverse psoriasis, pustular psoriasis, erythrodermic psorosis.
1. Plaque Psoriasis (Psoriasis Vulgaris)
The most common form of psoriasis, accounting for approximately 80-90% of cases. It is characterized by well-demarcated erythematous plaques covered with silvery-white scales, commonly affecting the elbows, knees, scalp, and lower back.
2. Guttate Psoriasis
Characterized by multiple small, drop-shaped erythematous lesions distributed over the trunk and extremities. It commonly occurs in children and young adults following streptococcal infections.
3. Inverse Psoriasis
Presents as smooth, shiny, erythematous lesions occurring in skin folds such as the axillae, groin, inframammary regions, and intergluteal cleft.
4. Pustular Psoriasis
A severe inflammatory variant characterized by sterile pustules on erythematous skin. It may be localized or generalized and can be associated with systemic symptoms such as fever and malaise.
5. Erythrodermic Psoriasis
A rare but potentially life-threatening form involving widespread erythema, scaling, and exfoliation affecting more than 75% of the body surface area.
6. Nail Psoriasis
Affects fingernails and toenails, leading to pitting, discoloration, subungual hyperkeratosis, onycholysis, and nail plate deformities.
Symptoms
Psoriasis is a long-term, non-communicable autoimmune condition that results in thick, scaly, inflammatory areas due to the quick formation of dead skin cells. It is typified by cycles of remission and flare-ups, with symptoms sometimes getting worse for weeks or months before getting better. Itching, burning, and discomfort are common symptoms, however they vary greatly depending on the kind, severity, and skin tone of psoriasis.
Common Symptoms of Psoriasis
Plaques (Raised Patches): The most common sign, especially in plaque psoriasis (which accounts for 80-90% of cases), is the presence of thick, inflamed patches of skin.
Coloration: These patches vary by skin tone—appearing pink or red with silvery-white scale on lighter skin, and purple, dark brown, or grayish on darker skin tones.
Scaling: The surface of these patches is often covered in a buildup of dead skin cells (scales) that may flake off.
Itching and Burning: Affected areas are often intensely itchy, sore, or feel like they are burning.
Dry, Cracked Skin: The skin may become extremely dry and crack, sometimes leading to bleeding.
Joint Pain: Up to 30% of people with psoriasis also experience joint pain, stiffness, and swelling (psoriatic arthritis).
Nail Changes: Psoriasis frequently affects fingernails and toenails, causing pitting (tiny dents), discoloration (yellow/brown spots), thickening, or the nail separating from the bed (onycholysis).
Diagnosis
Clinical evaluation (primary technique) : A dermatologist studies the skin, scalp, nails, and joints for the characteristic picture: well-defined, erythematous plaques with silvery-white scales, frequently on the head, knees, and elbows, and changes to the nails (pitting, onycholysis). The diagnosis is typically made based on morphology and distribution without the need for additional testing. Inquiries about itching, burning, recent stress, illnesses, drugs, and family history are also made by the doctor.
Health and family background: The diagnosis is supported by information on the onset, triggers (drugs, stress, trauma, and streptococcal throat infection), symptom pattern, and whether family members have psoriasis.
Physical symptoms and dermatoscopyAuspitz sign: pinpoint blood occurs when scales are scraped off. Thick scales rise like wax in the candle-wax symbol. These bedside indicators can be demonstrated by the grattage test (glass slide)
Scoring instruments (not for diagnosis, but to measure severity) : After a diagnosis is made, the Dermatology Life Quality Index (DLQI), Body-Surface Area (BSA), and Psoriasis Area and Severity Index (PASI) are recorded.
Skin biopsy (in cases of concern) : A little punch biopsy is performed if the rash may be caused by lichen planus, dermatophyte infection, eczema, etc. Histological observations that confirm psoriasis and rule out imitators include epidermal hyperplasia, parakeratosis, neutrophils (Munro microabscesses), and elongation of rete ridges.
Tests for differential diagnosis : For scaly plaques, use KOH wet mount to rule out fungal infection. Blood tests (CBC, ESR/CRP, rheumatoid factor, HLA-B27) may be conducted to assess for metabolic comorbidities or associated psoriatic arthritis, although they are not diagnostic for psoriasis itsel
Causes & Risk factors
Psoriasis is an immune-mediated, chronic, non-contagious condition that results in thick, scaly, and itchy patches due to the fast growth of skin cells. Although the precise etiology is still unknown, it is understood to be a complicated interplay between environmental factors and a person's DNA. About 2-4% of people have this chronic illness, which has symptoms and cures throughout life.
Causes
The fundamental cause of psoriasis is an overactive immune system, specifically involving T-cells (white blood cells) and cytokines.
Immune System Dysfunction: The growth and shedding of skin cells take around 30 days in a healthy organism. T-cells in psoriasis incorrectly target healthy skin cells, promoting this cycle to only three to four days. The characteristic plaques are caused by the old skin cells developing up because they cannot shed quickly enough.
Genetic Predisposition: Research indicates that psoriasis is 60-90% heritable, and it frequently runs in families. It is caused by more than 60 susceptibility loci, including HLA-Cw6, which is associated with severe, early-onset disease.
Parental Risk: A child has a roughly 10% chance of getting psoriasis if one parent has it. The risk rises to more than 50% if both parents have it.
Environmental Triggers: A person frequently has to be exposed to particular surroundings in order to start the disease, even if they have a genetic weakness.
Risk factors
Triggers are things that cause a flare-up in a person who already has psoriasis, whereas risk factors are things that raise the chance of getting the condition.
1. Lifestyle Factors
Obesity: Being overweight creates a serious risk. Adipose (fat) tissue is thought to emit inflammatory chemicals that can cause or enhance psoriasis, especially in skin folds (inverse psoriasis).
Smoking: Smoking is a significant risk factor for psoriasis and frequently makes the condition worse. The risk increases by two times for smokers compared to non-smokers, and it is closely associated with pustular psoriasis, a form that is challenging to treat.
Alcohol Use: Excessive alcohol use is linked to increased risk, worsened symptoms, and less successful treatment outcomes.
Stress: Prolonged physical or mental stress is a powerful inducer of the disease's onset and aggravation.
2. Infections
Infections, especially strep throat (a streptococcal infection), are frequent causes of guttate psoriasis in children and young adults.
HIV: Although HIV does not directly cause psoriasis, it can cause it to manifest initially or significantly exacerbate pre-existing symptoms.
Other diseases: respiratory diseases, bronchitis, and ear infections can all serve as triggers.
3. Medications
Certain, often commonly prescribed, medications can cause psoriasis to appear or flare up:
Lithium: Used for bipolar disorder and psychiatric illnesses.
Beta-blockers: Used for high blood pressure and heart problems.
Antimalarial Drugs: Including chloroquine and hydroxychloroquine.
NSAIDs: Nonsteroidal anti-inflammatory drugs like indomethacin.
Withdrawal of Corticosteroids: Rapidly stopping systemic or strong topical steroids can cause a severe flare
4. Skin Injuries (Koebner Phenomenon)
Psoriasis often develops at the site of skin trauma, a phenomenon known as the Koebner response. Examples include:
Cuts, scrapes, or scratches.
Severe sunburn.
Vaccinations.
Tattoos or piercings
Complications
Approximately 3 percent of people worldwide suffer from psoriasis, a chronic inflammatory condition that is immune-mediated. Psoriasis, which is typified by scaly, erythematous skin plaques, is becoming more widely acknowledged as a systemic illness rather than merely a skin disorder. Many severe, frequently fatal consequences are caused by the chronic systemic inflammation linked to psoriasis, especially in patients with moderate-to-severe illness. Given that these conditions may manifest 1-2 years following the onset of the initial cutaneous complaints, prompt identification and continuous, thorough monitoring are essential.
The complications of psoriasis span physical health, mental wellbeing, and long-term functional impairment, sometimes even increasing mortality risk.
Arthritis Psoriatica (PsA): Up to 30% of patients with psoriasis will develop psoriatic arthritis, the most prevalent consequence. It is an inflammatory, persistent, and possibly fatal type of arthritis that can cause irreversible joint destruction and, in severe cases (10% of patients), limiting disability.
Cardiovascular Complications: Psoriasis increases the risk of cardiovascular diseases due to chronic systemic inflammation.
Patients with moderate to severe psoriasis have a higher risk of:
Hypertension
Atherosclerosis
Myocardial infarction
Stroke
Blood artery plaque and endothelial dysfunction are caused by inflammatory mediators such TNF-α, IL-17, and IL-23. Atherosclerosis is accelerated by the ongoing inflammatory
3. Impact on Mental Health and Psychology
Studies reveal that up to 98% of people with psoriasis express negative psychological effects, indicating that the condition frequently causes severe mental stress.
Anxiety and Depression: About 30% of patients have anxiety, and about 18% may develop depression.
Social Stigmatization: Lesion-related disfigurement frequently results in sexual dysfunction, low self-esteem, shame, and social disengagement.
7-17% of patients report having suicidal thoughts, especially those with severe, noticeable skin involvement.
4. Dermatological Issues:
Severe, acute consequences may arise in the skin itself, especially if the condition is not well treated or is brought on by outside influences.
Extreme pain, severe scaling, and systemic symptoms, such as fever, are caused by extensive inflammation in the rare but potentially fatal variant of erythrodermic psoriasis. High-output heart failure, electrolyte abnormalities, and significant protein/fluid loss are possible outcomes.
Blisters packed with pus are the hallmark of pustular psoriasis, which needs to be treated right away since it can lead to fever, infection, and, in extreme cases, sepsis.
Secondary Infections: Bacterial or fungal skin infections can result from psoriasis-related open, fissured skin.
Psoriatic nail disease, which results in pitted, discolored, or disintegrating nails, can be extremely painful and impede one's ability to work.
5. Other Co-occurring Conditions
Inflammatory Bowel Disease IBD: Because psoriasis and Crohn's disease overlap inflammatory pathways, patients with psoriasis are approximately twice as likely to develop Crohn's disease and ulcerative colitis.
Eye Problems: Eye issues include blepharitis (inflammation of the eyelids), conjunctivitis (pink eye), and uveitis (inflammation of the eye).
Chronic Kidney Disease (CKD): There is a strong correlation, especially in severe cases, which could be brought on by treatment-related toxicities or long-term vascular damage.
Cancer: Systemic inflammation and therapies like phototherapy (PUVA) may be connected to an increased risk of non-melanoma skin malignancies (squamous and basal cell carcinomas) and cancer in general, especially lymphoma.
Liver Disease: NAFLD, or nonalcoholic fatty liver disease, is a common condition linked to metabolic syndrome.
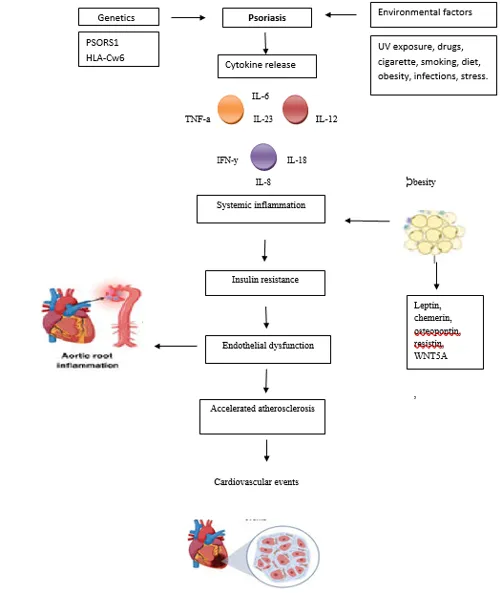
Pathophysiology of the Disease
Complex pathogenesis including genetic autoimmune and environmental factors:
T cell (Th1) activation and release of cytokines (TNFα, IFγ, IL12, etc.)
Dendritic cells produce IL23, which activates Th17 cells, which then play a key role in the development of psoriasis; IL23 also induces macrophages to secrete TNFα
Th17 cells produce IL17, which promotes the production of other proinflammatory molecules (IL22, produced by Th17 and Th22 cells, plays a role in stimulating the proliferation of keratinocytes and causing the development of psoriatic plaques
Overexpression of antimicrobial peptides (β-defensins, cathelicidin and S100) stimulate inflammation
NFκB induces expression of keratins 6 and 16, leading to acanthosis and increased turnover of keratinocytes.
Allopathic remedies
Ayurvedic plants used in psoriasis
Several herbal drugs are used as complementary or adjunctive therapies for psoriasis, with the most evidence supporting the use of Mahonia aquifolium (Oregon grape), Indigo naturalis (Qing dai), and Aloe vera (Aloe barbadensis), Turmeric (Curcuma longa), Berberry (Berberis vulgaris), Neem (Azadiratchta indica), Garlic (Allium sativum) Onion (Allium cepa), Black cumin (Nigella sativa), Liqurorice (Glicyrrhiza glabra), Sandalwood (Santalum album).
BARBERRY (Berberis vulgaris),
(Fig.1.2)
Barberry plant extracts, specifically those from species like Mahonia aquifolium (Oregon grape, a type of barberry), are used topically for mild to moderate psoriasis and have shown promising results in clinical studies. The primary active ingredient responsible for its effects is the alkaloid berberine.[12]
Barberry (Berberis vulgaris) is known for its potential anti-inflammatory and antioxidant properties, which may benefit skin conditions like psoriasis.
Anti-inflammatory Effects: Berberine, which is found in barberries, has been demonstrated to lessen inflammation, possibly easing some Psoriasis symptoms
Antioxidant Properties: People with psoriasis frequently have higher levels of oxidative stress, which the antioxidants in barberry can help fight.
Herbal Teas or Infusions: Some people utilize barberry's possible health benefits, such as its anti-inflammatory qualities, by incorporating it into herbal teas.
Topical Treatments: Barberry extracts are used in ointments and lotions to reduce scaling and soothe inflamed skin. These goods might aid with symptom relief.
Traditional Remedies: In tradition l medicine, it has been used for various skin conditions, including psoriasis, due to its purported ability to support skin healing.
Turmeric (Curcuma longa)
(Fig.1.3)
Turmeric is obtained from curcuma longa and belongs to the family of zingiberaceae Curcumin gel may help relieve psoriasis when combined with:
Topical steroids
Antibiotics and avoidance of allergens
.Immunological Modulation: Curcumin can assist in regulating the immunological response, an autoimmune disease in which the immune system targets healthy skin cells.
Anti-inflammatory Effects: It reduces inflammation, redness, and scaling by blocking pro-inflammatory cytokines like TNF-α and interleukins (IL-6, IL-17, and IL-22), which are overactive in psoriasis patients.
Antioxidant Activity: The oxidative stress linked to psoriatic lesions is lessened by curcumin's antioxidant qualities.
Use of turmeric of psoriasis:
Dietary Incorporation: Include turmeric in soups, curries, and other foods. This has anti-inflammatory properties that can have systemic advantages.
Turmeric Baths: Putting turmeric powder in a warm bath will help with soreness and irritation.
Topical Uses: Turmeric Paste: To make a paste, combine this powdered turmeric with water or coconut oil. To relieve discomfort and lower inflammation, apply to the afflicted regions. Creams or Ointments with Turmeric
Garlic (Allium sativum):
(Fig.1.4)
Garlic (Allium sativum) is being researched for its potential anti-inflammatory and Immunomodulatory properties in managing psoriasis, primarily due to the compound allicin. While traditional use and some studies suggest benefits, clinical effectiveness is still being thoroughly explored, and direct application can cause skin irritation.
Effects on Inflammation: Psoriasis is an inflammatory disease. By blocking particular signaling pathways (such as the nuclear transcription factor kappaβ and IL-17 signaling cascades) that are connected to the proliferation of skin cells and inflammation in psoriasis, allicin has demonstrated strong anti-inflammatory effects.
Antioxidant Properties: Containing with antioxidants, garlic helps regulate the activity of free radicals, which lead to inflammation and cell damage.
Immunomodulation: Garlic may help modulate the immune system response, which is overactive in people with psoriasis.
Use of garlic for psoriasis:
Home Remedies: Some individuals combine crushed garlic with a carrier oil (such as coconut or olive oil) to treat problems like scalp psoriasis.
Topical Garlic Extract/Gel: Research indicates that using garlic extract topically may help treat psoriasis. Garlic gel greatly increased the effectiveness of betamethasone valerate, a common topical steroid, in treating alopecia areata, according to a randomized controlled experiment. This suggests that garlic gel could be used as an adjuvant treatment for other inflammatory skin disorders, such as psoriasis.
Allicin-Based Nanogels: New delivery methods, such as allicin-loaded transethosomal gels, are being investigated as a potential topical therapy strategy because of allicin's instability and low skin penetration. These specialty nanogels have shown potential in treating mild-to-moderate plaque psoriasis in clinical tests
Aloe vera (Aloe barbadensis):
(Fig.1.5)
Aloe vera is a common plant used in first aid products for thermal injuries and beauty maintenance.
Patients treated their psoriatic plaques with self-administered topical Aloe vera extract cream or a vehicle control three times a day without occlusion for four weeks. In practically every patient, the aloe group had significantly greater rates of psoriatic plaque removal.[8]
The primary active ingredients in aloe vera, anthraquinone and acemannan, have antibacterial properties against Streptococcus and Staphylococcus species, which may explain why they are effective treatments for psoriasis
Promotes healing: Its wound-healing properties can help repair damaged skin and accelerate the growth of healthy skin cells.
Reduces Psoriasis Area and Severity Index (PASI) scores: According to some research, aloe vera lotion can help patients with mild to moderate psoriasis by considerably removing plaque and reducing severity scores
Use of aloe vera for psoriasis:
Reduces Redness and Inflammation: Aloe Vera’s active ingredients may help lessen the redness and inflammation brought on by psoriatic plaques.
Moisturizes Skin: Its high water content and mucopolysaccharides aid in maintaining skin integrity and moisture retention, preventing dry, cracked skin.
Calms Itching and Scaling: The gel's calming properties can help soften thick, scaly areas (plaques) and offer momentary relief from itching.
Promotes Wound Healing: If psoriasis plaques break or bleed, it may hasten the healing process.
Liqurorice (Glicyrrhiza glabra)
(Fig.1.6)
Liquorice (Glycyrrhiza glabra), also known as licorice, is used for psoriasis primarily in topical applications due to its significant anti-inflammatory and antioxidant properties. Its main active ingredients, glycyrrhizin (or glycyrrhizic acid) and glabridin, help reduce the redness, scaling, and inflammation associated with psoriasis
Topical Application: Applying licorice topically is the most popular and advised method of treating psoriasis. It comes in a number of forms:
Gels and Emulgels: In order to improve the delivery of the active ingredients deep into the skin lesions, research has concentrated on creating non-greasy, readily spreadable emulgels based on licorice oil.
Creams & Lotions: To relieve irritated skin and treat inflammatory diseases, licorice extracts are frequently added to prescription or over-the-counter creams and lotions.
DIY Masks/Pastes: According to some conventional or anecdotal usage, licorice powder can be combined with a liquid (such as milk, water, or aloe vera gel) to make a paste that can be applied directly to afflicted regions.
Mouth Rinses: Licorice-containing rinses can be used to lessen discomfort and hasten the healing of ulcers when psoriasis affects the mouth, however this is less common.
Black cumin (Nigella sativa)
(Fig.1.7)
Black cumin (Nigella sativa), also known as black seed, is traditionally used for skin conditions including psoriasis due to its potent anti-inflammatory, antioxidant, and Immunomodulatory properties. Its primary active ingredient, thymoquinone, is responsible for these therapeutic effects.
Topical Oil/Ointment: You can apply black cumin seed oil straight to the skin's afflicted spots. Research on palm plantar psoriasis, or psoriasis of the palms and soles, using a particular black cumin oil ointment revealed a notable decrease in skin thickness and fissuring.
Improved Formulations: In contrast to the raw oil, which naturally contains lower amounts of thymoquinone, patented gels and particular formulations with standardized, therapeutically effective doses of thymoquinone have been created and tested to improve penetration and efficacy.
Uses of Black cumin for psoriasis:
Anti-inflammatory Effects: Thymoquinone, the main active ingredient, has strong anti-inflammatory qualities that lessen the redness, swelling, and inflammation brought on by psoriatic lesions.
Regulation of Skin Cells: Research using animal models suggests that black cumin extracts may aid in preventing keratinocytes (skin cells), a major feature of psoriasis, from proliferating and differentiating abnormally.
Antioxidant Activity: Oxidative stress is associated with psoriasis. The potent antioxidants in black cumin shield skin cells from harm and may help control symptoms.
Protection and Moisturizing: Packed with important fatty acids, black cumin seed oil can provide the skin with deep moisture, reducing irritation, scaling, and dryness.
Neem (Azadiratchta indica):
(Fig.1.8)
Neem has anti-inflammatory and antibacterial qualities are the main reasons it is used as a supplemental treatment for psoriasis symptoms like dryness, itching, and inflammation.[13]
There are several types of Neem that can be applied topically. To prevent skin irritation, it is essential to conduct a patch test first and dilute strong forms, such as the oil.
Soothes Itching and Irritation: Its cooling nature and soothing effect help to lessen the urge to scratch, which prevents further skin damage and potential infection.
Protects Against Infection: The natural antifungal and antimicrobial properties of Neem help protect cracked or wounded skin from secondary infections.
Reduces Itching and Irritation: Its cooling properties and calming impact reduce the need to scratch, preventing additional skin damage and possible infection.
Reduces Inflammation: It contains compounds like nimbidin that can be help to calm irritated skin, reducing redness of skin and swelling associated with psoriasis flares.
Use of Neem for psoriasis:
Anti-inflammatory: Neem's compounds help lessen the swelling and redness brought on by flare-ups of psoriasis.
Antimicrobial: The inherent antifungal and antibacterial qualities can aid in preventing infections that may arise from scratching dry, damaged skin.
Neem helps retain moisture, which lessens the dryness and scaling that are typical with psoriasis.
Oral Supplements: Neem extracts, which are utilized in traditional medicine for systemic effects like blood purification and immunological modulation, are available orally as capsules or powder. Only after speaking with a healthcare professional should these be taken.
Mohniya Aquifoliun (Oregon grape)
(Fig.1.9)
Mahonia aquifolium (Oregon grape) is a safe, effective topical treatment for mild-to-moderate psoriasis, typically used as a 10% extract cream or ointment. According to studies, by preventing keratinocyte hyperproliferation and lowering inflammation, it dramatically lowers plaque thickness, scaling, and redness in just two to four weeks. It has little adverse effects and is well tolerated.[12]
Uses of Mohnia aquifolium for psoriasis:
Skin Conditions: Research indicates that M. aquifolium reduces skin cell proliferation and soothes irritation to effectively treat plaque psoriasis. Additionally, it is used to treat general skin inflammation, acne, and eczema.
Berberine, which is found in the root and bark, has antimicrobial and anti-inflammatory properties.
Digestive Support: It has historically been used to promote liver and gallbladder function and aid in digestion.
Topical Application: To address sensitive skin conditions like redness, irritation, and itching, it is incorporated into creams and serums.
CONCLUSION
Herbal medicine extends a promising and supportive approach for the treatment of psoriasis a chronic inflammatory skin disease. Conventional therapy such as phototherapy, topical steroids & systemic medicine are effective for many patients but long time uses of that medicine may cause side effect because psoriasis is a lifelong condition with periods of flare-ups and remission. Many patients look for safer and more natural options to control their symptoms. The medicines which are obtained from plant & natural sources have been traditionally used in different system of medicine & are now gaining scientific attention. Various herbs such as a Neem, Indigo turmeric, Aloe-Vera, Liquorice, Barberry, Garlic, Black cumin have shown anti-inflammatory, anti-oxidant & Immunomodulator properties that may reduce redness, scaling, itching and thickness of psoriatic plaques. Some clinical studies suggest that these herbal remedies can improves skin lesions and enhance quality of life in addition herbal formulation are often more affordable and culturally acceptable in many communities.
REFERENCES
Farber EM, Nall LM. The natural history of psoriasis in 5600 patients. Dermatologica1974;(148): 1-18.
Martin BA, Chalmers RJ, Telfer NR. How great is the risk of further psoriasis following a single episode of acute guttate psoriasis? Arch Dermatol. 1996; (132):717-18.
Choonhakarn C, Busaracome P, Sripanidkulchai B, Sarakarn P. A prospective, randomized clinical trial comparing topical Aloe Vera with 0.1% triamcinolone acetonide in mild to moderate plaque psoriasis. J Eur Acad Dermatol Venereol., 2010; (24):168-72.
Richardson SK, Gelfand JM. Update on the natural history and systemic treatment of psoriasis. Adv Dermatol 2008;( 24):171-96.
Langley RG. Effective and sustainable biologic treatment of psoriasis: What can we learn from new clinical data? J Eur Acad Dermatol Venereol 2012; (26):S21-9.
Bhardwaj S, Gaur PK, Tiwari A. Development of topical nanoemulgel using combined therapy for treating psoriasis. Assay Drug Dev Technol 2022; (20): 42-54. doi: 10.1089/adt.2021.112
Thaçi D, Strober B, Gordon KB, Foley P, Gooderham M, Morita A, et al. Deucravacitinib in moderate to severe psoriasis: clinical and quality-of-life outcomes in a phase 2 trial. Dermatol Ther (Heidelb) 2022; (12): 495-510. doi: 10.1007/s13555-021-00649-y.
Khan A, Qadir A, Ali F, Aqil M. Phytoconstituents based Nano medicines for the management of psoriasis. J Drug Deliv Sci Technol 2021; 64: 102663. doi: 10.1016/j.jddst.2021.102663.
Syed TA, Ahmad SA, Holt AH, Ahmad SA, Ahmad SH, Afzal M. Management of psoriasis with aloe Vera extract in a hydrophilic cream: A placebo-controlled, double-blind study. Trop Med Int Health., 1996; 1: 505-509.
Bäumer W, Hoppmann J, Rundfeldt C, Kietzmann M. Highly selective phosphodiesterase 4 inhibitors for the treatment of allergic skin diseases and psoriasis. Inflamm Allergy -Drug Targets. 2006;6(1):17-26.
Gulliver WP, Donsky HJ. A report on three recent clinical trials using Mahonia aquifolium 10% topical cream and a review of the worldwide clinical experience with Mahonia aquifolium for the treatment of plaque psoriasis. Am J Ther. 2005; 12(5):398- 406.
Antiga E Oral Curcumin is effective as an adjuvant treatment & is able to reduce IL-22 Serum level in patient with psoriasis vulgaris. Biomed Res Int 2015:2015:283634.
Rakam Gopi Krishna, Kuchi Manjeera, Repudi Lalitha, Nadumula Sunitha. Preliminary phytochemical screening and in vitro antibacterial activity of Bridelia retusa plant extract. World Journal of Pharmaceutical Research. 2013; 2(6): 3337-3347.
Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol 1995 ;(32):982-6.
Kang NW, Kim MH, Sohn SY, Kim KT, Park JH, Lee SY, et al. Curcumin-loaded lipid-hybridized cellulose nanofiber film ameliorates imiquimod-induced psoriasis-like dermatitis in mice. Biomaterials 2018; 182: 245-58. doi: 10.1016/j. biomaterials.2018.08.030
Raval AM, Maneklal RJ, Dilipbhai MU. Development and Evaluation of PolyherbalTopical Cream for Wound Healing Applications Using Alum, Turmeric, and Aloe Vera. Asian Journal of Pharmaceutical Research and Development. 2026 Apr 15;14(2):234-40.
Panthaki J, Bhai YL, Kumar VS, Raval AM. Formulation and Evaluation of Body Scrub Using Walnut Shell Powder. Asian Journal of Pharmaceutical Research and Development. 2026 Apr 15;14(2):241-7.
Raval AM, Rana T, Joshi SY, Buch S, Arora B, Patel VS. Artificial intelligence in pharmacy and healthcare: applications in drug discovery, precision medicine, clinical practice, and future perspectives. Asian Journal of Pharmaceutical Research and Development. 2026 Apr 15;14(2):62-9.
Thakor AD, Dharajiya RM, Shaikh MZ, Raval AM. A review on neuropharmacology: mechanisms, drug classes, and clinical applications. Asian Journal of Pharmaceutical Research and Development. 2026 Feb 15;14(01):114-21.
Reference
Farber EM, Nall LM. The natural history of psoriasis in 5600 patients. Dermatologica1974;(148): 1-18.
Martin BA, Chalmers RJ, Telfer NR. How great is the risk of further psoriasis following a single episode of acute guttate psoriasis? Arch Dermatol. 1996; (132):717-18.
Choonhakarn C, Busaracome P, Sripanidkulchai B, Sarakarn P. A prospective, randomized clinical trial comparing topical Aloe Vera with 0.1% triamcinolone acetonide in mild to moderate plaque psoriasis. J Eur Acad Dermatol Venereol., 2010; (24):168-72.
Richardson SK, Gelfand JM. Update on the natural history and systemic treatment of psoriasis. Adv Dermatol 2008;( 24):171-96.
Langley RG. Effective and sustainable biologic treatment of psoriasis: What can we learn from new clinical data? J Eur Acad Dermatol Venereol 2012; (26):S21-9.
Bhardwaj S, Gaur PK, Tiwari A. Development of topical nanoemulgel using combined therapy for treating psoriasis. Assay Drug Dev Technol 2022; (20): 42-54. doi: 10.1089/adt.2021.112
Thaçi D, Strober B, Gordon KB, Foley P, Gooderham M, Morita A, et al. Deucravacitinib in moderate to severe psoriasis: clinical and quality-of-life outcomes in a phase 2 trial. Dermatol Ther (Heidelb) 2022; (12): 495-510. doi: 10.1007/s13555-021-00649-y.
Khan A, Qadir A, Ali F, Aqil M. Phytoconstituents based Nano medicines for the management of psoriasis. J Drug Deliv Sci Technol 2021; 64: 102663. doi: 10.1016/j.jddst.2021.102663.
Syed TA, Ahmad SA, Holt AH, Ahmad SA, Ahmad SH, Afzal M. Management of psoriasis with aloe Vera extract in a hydrophilic cream: A placebo-controlled, double-blind study. Trop Med Int Health., 1996; 1: 505-509.
Bäumer W, Hoppmann J, Rundfeldt C, Kietzmann M. Highly selective phosphodiesterase 4 inhibitors for the treatment of allergic skin diseases and psoriasis. Inflamm Allergy -Drug Targets. 2006;6(1):17-26.
Gulliver WP, Donsky HJ. A report on three recent clinical trials using Mahonia aquifolium 10% topical cream and a review of the worldwide clinical experience with Mahonia aquifolium for the treatment of plaque psoriasis. Am J Ther. 2005; 12(5):398- 406.
Antiga E Oral Curcumin is effective as an adjuvant treatment & is able to reduce IL-22 Serum level in patient with psoriasis vulgaris. Biomed Res Int 2015:2015:283634.
Rakam Gopi Krishna, Kuchi Manjeera, Repudi Lalitha, Nadumula Sunitha. Preliminary phytochemical screening and in vitro antibacterial activity of Bridelia retusa plant extract. World Journal of Pharmaceutical Research. 2013; 2(6): 3337-3347.
Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol 1995 ;(32):982-6.
Kang NW, Kim MH, Sohn SY, Kim KT, Park JH, Lee SY, et al. Curcumin-loaded lipid-hybridized cellulose nanofiber film ameliorates imiquimod-induced psoriasis-like dermatitis in mice. Biomaterials 2018; 182: 245-58. doi: 10.1016/j. biomaterials.2018.08.030
Raval AM, Maneklal RJ, Dilipbhai MU. Development and Evaluation of PolyherbalTopical Cream for Wound Healing Applications Using Alum, Turmeric, and Aloe Vera. Asian Journal of Pharmaceutical Research and Development. 2026 Apr 15;14(2):234-40.
Panthaki J, Bhai YL, Kumar VS, Raval AM. Formulation and Evaluation of Body Scrub Using Walnut Shell Powder. Asian Journal of Pharmaceutical Research and Development. 2026 Apr 15;14(2):241-7.
Raval AM, Rana T, Joshi SY, Buch S, Arora B, Patel VS. Artificial intelligence in pharmacy and healthcare: applications in drug discovery, precision medicine, clinical practice, and future perspectives. Asian Journal of Pharmaceutical Research and Development. 2026 Apr 15;14(2):62-9.
Thakor AD, Dharajiya RM, Shaikh MZ, Raval AM. A review on neuropharmacology: mechanisms, drug classes, and clinical applications. Asian Journal of Pharmaceutical Research and Development. 2026 Feb 15;14(01):114-21.
Nikita Thakar
Corresponding author
Assistant Professor, Vidhyadeep Institute of Pharmacy, Anita, Kim, Surat, Gujarat, India
Gautam Sonara
Co-author
Principal and Professor, Vidhyadeep Institute of Pharmacy, Anita, Kim, Surat, Gujarat, India
Mahek Mojidra
Co-author
Vidhyadeep Institute of Pharmacy, Anita, Kim, Surat, Gujarat, India
Mahek Nayak
Co-author
Vidhyadeep Institute of Pharmacy, Anita, Kim, Surat, Gujarat, India
Purvi Marche
Co-author
Vidhyadeep Institute of Pharmacy, Anita, Kim, Surat, Gujarat, India
Nidhi Chumbhatiya
Co-author
Vidhyadeep Institute of Pharmacy, Anita, Kim, Surat, Gujarat, India
Nikita Thakar, Gautam Sonara, Mahek Mojidra, Mahek Nayak, Purvi Marche, Nidhi Chumbhatiya, Plant-Based Approaches to Psoriasis: A Systematic Review of Efficacy and Safety, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 374-389. https://doi.org/10.5281/zenodo.21140234










 10.5281/zenodo.21140234
10.5281/zenodo.21140234