
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1, 3,4,5General Physician, Corporación Universitaria Rafael Núñez, Cartagena, Colombia
2General Physician, Universidad del Sinu, Cartagena, Colombia.
Background: Polycystic ovary syndrome (PCOS) is the most common endocrine disorder affecting adolescent females and represents a major cause of menstrual irregularities, hyperandrogenism, and metabolic dysfunction. The diagnosis of PCOS during adolescence remains challenging due to the physiological overlap between normal pubertal development and pathological manifestations, contributing to substantial variability in reported prevalence rates across different populations and healthcare settings.Objective: To review and synthesize current evidence regarding the prevalence and clinical characteristics of PCOS in adolescents, emphasizing findings from multicenter studies and international cohorts.Methods: A narrative review was conducted focusing on multicenter observational studies, epidemiological investigations, and consensus guidelines addressing adolescent PCOS. Relevant literature evaluating prevalence estimates, diagnostic criteria, clinical manifestations, metabolic abnormalities, and associated comorbidities was examined to provide a comprehensive overview of the condition in this age group.Results: The reported prevalence of adolescent PCOS varies considerably depending on the diagnostic criteria employed, ranging from approximately 3% to over 20% in population-based studies. Menstrual irregularities and clinical or biochemical hyperandrogenism constitute the most frequently reported manifestations. Common clinical features include oligomenorrhea, acne, hirsutism, obesity, insulin resistance, and acanthosis nigricans. Metabolic abnormalities, including dyslipidemia, impaired glucose metabolism, and increased cardiometabolic risk, are observed in a significant proportion of affected adolescents. Recent multicenter investigations highlight substantial geographic and ethnic differences in disease presentation, suggesting that genetic, environmental, and lifestyle factors contribute to phenotypic variability. Furthermore, growing evidence indicates that psychological comorbidities, including anxiety, depression, and reduced quality of life, are common among adolescents diagnosed with PCOS.Conclusions: PCOS is a prevalent and heterogeneous disorder among adolescents, characterized by reproductive, metabolic, and psychological manifestations that may persist into adulthood. Variability in diagnostic approaches continues to influence prevalence estimates and complicates comparisons across studies. Early recognition, standardized diagnostic criteria, and multidisciplinary management strategies are essential to improve long-term reproductive and metabolic outcomes in this population
Polycystic ovary syndrome (PCOS) is one of the most prevalent endocrine and metabolic disorders affecting females of reproductive age and represents the leading cause of hyperandrogenism and ovulatory dysfunction worldwide. The syndrome is characterized by a heterogeneous clinical presentation that includes menstrual irregularities, clinical or biochemical hyperandrogenism, metabolic abnormalities, and reproductive dysfunction. Although traditionally considered a disorder of adult women, increasing evidence suggests that its manifestations frequently begin during adolescence, making this developmental period critical for early recognition and intervention [1,2].
The epidemiology of adolescent PCOS remains controversial due to the substantial overlap between normal pubertal physiological changes and the pathological features that define the syndrome. During adolescence, menstrual irregularities, acne, transient hyperandrogenism, and multifollicular ovarian morphology may occur as part of normal maturation of the hypothalamic–pituitary–ovarian axis. Consequently, distinguishing physiological pubertal development from true PCOS represents a significant diagnostic challenge for clinicians and researchers alike [3, 4]. This diagnostic complexity has contributed to considerable variability in prevalence estimates reported across studies, populations, and geographical regions.
Current evidence indicates that the prevalence of PCOS among adolescents varies widely depending on the diagnostic criteria employed. Studies have reported prevalence rates ranging from approximately 3% to more than 20%, reflecting differences in population characteristics, ethnic composition, study design, and diagnostic definitions [1,4]. Historically, the Rotterdam criteria, the National Institutes of Health (NIH) criteria, and the Androgen Excess and PCOS Society criteria have been used to establish the diagnosis; however, concerns regarding overdiagnosis in adolescents have led to the development of age-specific recommendations. Recent international evidence-based guidelines recommend that the diagnosis of adolescent PCOS should be based on the presence of persistent menstrual irregularities and hyperandrogenism after exclusion of alternative etiologies, while ovarian ultrasound and anti-Müllerian hormone measurements are not recommended for diagnosis during the early postmenarcheal years [5, 6].
Beyond its reproductive manifestations, PCOS has emerged as a multisystem disorder associated with significant metabolic and psychological consequences. Insulin resistance, compensatory hyperinsulinemia, obesity, dyslipidemia, impaired glucose tolerance, and increased risk of type 2 diabetes mellitus have been consistently documented among affected adolescents [7]. These metabolic alterations may appear early in the disease course and contribute to the development of long-term cardiometabolic complications extending into adulthood. Furthermore, evidence suggests that adolescents with PCOS experience a higher prevalence of anxiety, depressive symptoms, body image disturbances, eating disorders, and reduced health-related quality of life when compared with their healthy peers [8].
The clinical phenotype of PCOS is influenced by complex interactions among genetic susceptibility, epigenetic mechanisms, environmental exposures, lifestyle factors, and ethnicity. Recent multicenter and multinational studies have demonstrated significant regional variations in both prevalence and clinical presentation, suggesting that ethnic background and socioeconomic determinants may substantially influence disease expression [9]. Such heterogeneity has important implications for diagnosis, screening strategies, and individualized therapeutic approaches.
Given the growing global burden of PCOS and the potential lifelong consequences associated with delayed diagnosis and treatment, a comprehensive understanding of its epidemiological profile and clinical manifestations during adolescence is essential. Early identification of affected individuals may facilitate timely interventions aimed at improving reproductive, metabolic, and psychological outcomes while reducing future morbidity. Therefore, this narrative review aims to synthesize current evidence regarding the prevalence and clinical characteristics of polycystic ovary syndrome in adolescents, with particular emphasis on findings derived from multicenter investigations and international studies. By integrating contemporary evidence, this review seeks to provide clinicians and researchers with an updated perspective on the diagnosis, presentation, and clinical significance of adolescent PCOS.
Methodology
Study Design
This study was conducted as a narrative review aimed at synthesizing current evidence regarding the prevalence and clinical characteristics of polycystic ovary syndrome (PCOS) in adolescents. A narrative review approach was selected because it allows the integration of epidemiological, clinical, metabolic, and psychological findings derived from diverse study designs, including multicenter observational studies, cohort studies, cross-sectional investigations, clinical practice guidelines, and systematic reviews. This methodology facilitates a comprehensive understanding of the heterogeneity of adolescent PCOS and the evolving diagnostic criteria applied across different healthcare settings.
Literature Search Strategy
A comprehensive literature search was performed in the electronic databases PubMed/MEDLINE, Scopus, Web of Science, Embase, and Google Scholar. The search focused on studies published in English between January 2015 and May 2026 to ensure inclusion of the most recent evidence and international recommendations regarding adolescent PCOS.
The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords using Boolean operators. The primary search terms included: "polycystic ovary syndrome", "PCOS", "adolescents", "teenagers", "prevalence", "epidemiology", "hyperandrogenism", "menstrual irregularities", "insulin resistance", "clinical characteristics", and "multicenter study". Various combinations of these terms were employed to maximize sensitivity and identify relevant publications.
Additionally, the reference lists of selected articles, systematic reviews, consensus statements, and international guidelines were manually screened to identify potentially relevant studies not captured during the initial database search.
Eligibility Criteria
Studies were considered eligible if they met the following inclusion criteria:
1. Investigated adolescents aged 10–19 years, according to the World Health Organization definition of adolescence.
2. Reported data on the prevalence, epidemiology, clinical manifestations, metabolic characteristics, or psychological features of PCOS.
3. Included multicenter, population-based, cohort, cross-sectional, or observational study designs.
4. Employed recognized diagnostic criteria for PCOS, including the National Institutes of Health (NIH), Rotterdam, Androgen Excess and PCOS Society, or International Evidence-Based Guideline criteria.
5. Were published in peer-reviewed journals and available in English.
The exclusion criteria were:
1. Studies exclusively involving adult women without separate adolescent analyses.
2. Case reports, conference abstracts, editorials, letters to the editor, and expert opinions lacking original data.
3. Studies with insufficient methodological information or unavailable full-text articles.
4. Publications focused exclusively on therapeutic interventions without reporting epidemiological or clinical outcomes relevant to the objectives of this review.
Study Selection and Data Extraction
The study selection process was performed through sequential screening of titles, abstracts, and full-text articles. Publications identified through database searches were assessed for relevance based on the predefined eligibility criteria. Data extraction focused on study characteristics, geographic location, sample size, diagnostic criteria utilized, prevalence estimates, reproductive manifestations, metabolic abnormalities, psychological outcomes, and major conclusions.
Special attention was given to multicenter investigations and international collaborative studies because these provide broader population representation and improve the generalizability of findings across different ethnic and socioeconomic groups.
Data Synthesis
The extracted evidence was analyzed qualitatively and organized into thematic categories. Findings were synthesized according to four principal domains: prevalence of PCOS in adolescents, reproductive and clinical manifestations, metabolic characteristics, and psychological outcomes. Particular emphasis was placed on identifying similarities and differences among studies conducted in distinct geographic regions and healthcare systems.
Given the heterogeneity of diagnostic criteria, study populations, and outcome definitions, a quantitative meta-analysis was not performed. Instead, a descriptive narrative synthesis was employed to summarize current evidence and highlight areas of consensus and ongoing controversy within the literature.
Ethical Considerations
As this study is based exclusively on previously published literature and does not involve human participants, patient data, or biological samples, institutional ethical approval and informed consent were not required. The review was conducted in accordance with internationally accepted principles of scientific integrity, transparency, and responsible reporting of research findings.
Development
Clinical Characteristics and Phenotypic Presentation of Polycystic Ovary Syndrome in Adolescents
Polycystic ovary syndrome (PCOS) is currently recognized as a complex and heterogeneous endocrine-metabolic disorder characterized by significant variability in clinical presentation, disease severity, and long-term health consequences. During adolescence, the syndrome presents unique diagnostic and clinical challenges because several manifestations overlap with physiological pubertal development. Consequently, the identification of pathological features requires careful clinical evaluation and longitudinal follow-up to distinguish transient pubertal changes from persistent endocrine dysfunction [10,14].
The clinical spectrum of adolescent PCOS extends beyond reproductive abnormalities and includes dermatological, metabolic, psychological, and cardiometabolic manifestations. This heterogeneity has led researchers to conceptualize PCOS not as a single disease entity but rather as a spectrum of interrelated phenotypes influenced by genetic predisposition, environmental exposures, lifestyle factors, and ethnic background [14,15].
Reproductive Manifestations
Menstrual dysfunction remains one of the earliest and most common clinical manifestations of adolescent PCOS. The maturation of the hypothalamic-pituitary-ovarian axis during puberty frequently results in transient menstrual irregularities; however, persistent abnormalities extending beyond the expected postmenarcheal period warrant further evaluation [10].
The most frequently reported menstrual abnormalities include:
- Oligomenorrhea
- Secondary amenorrhea
- Prolonged menstrual cycles
- Irregular uterine bleeding
- Chronic anovulation
Studies consistently demonstrate that menstrual dysfunction is present in more than 70% of adolescents eventually diagnosed with PCOS [10,14].
Table 1. Common Reproductive Manifestations in Adolescent PCOS
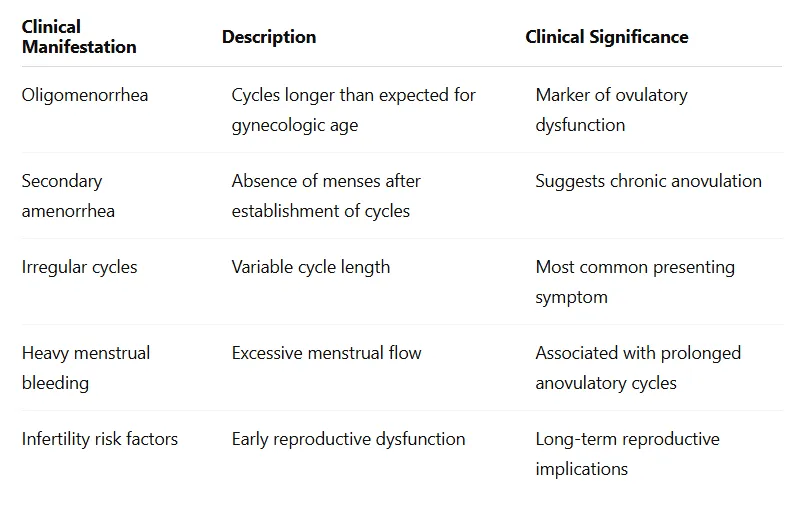
Persistent ovulatory dysfunction contributes to prolonged exposure to unopposed estrogen, potentially increasing future risks of endometrial hyperplasia and reproductive complications [15].
Hyperandrogenism: The Hallmark of Adolescent PCOS
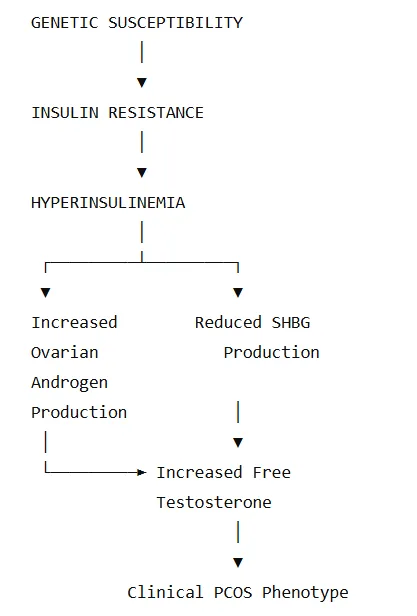
Hyperandrogenism constitutes one of the central pathophysiological and diagnostic components of PCOS. Excess androgen production arises primarily from ovarian theca cells and is frequently amplified by insulin resistance and hyperinsulinemia [16].
Hyperandrogenism may be expressed clinically or biochemically.
Clinical Hyperandrogenism
The most common manifestations include:
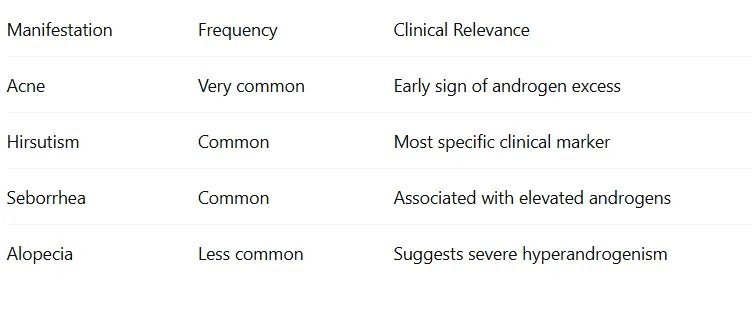
Acne
Acne vulgaris is highly prevalent during adolescence; however, severe, persistent, treatment-resistant acne may suggest underlying androgen excess. Several studies have identified moderate-to-severe inflammatory acne as one of the earliest dermatological manifestations associated with adolescent PCOS [16].
Hirsutism
Hirsutism is defined as excessive terminal hair growth in androgen-dependent areas and represents one of the most specific clinical markers of hyperandrogenism.
Common affected regions include:
- Upper lip
- Chin
- Neck
- Chest
- Abdomen
- Lower back
- Thighs
The Ferriman-Gallwey score remains the most widely used clinical assessment tool, although ethnic variations substantially influence its interpretation [17].
Alopecia
Although less frequent during adolescence than adulthood, androgenic alopecia may occur and is often associated with more severe androgen excess.
Table 2. Clinical Manifestations of Hyperandrogenism
Metabolic Characteristics
Increasing evidence supports the concept that PCOS is fundamentally a metabolic disorder rather than solely a reproductive condition [11].
Insulin resistance represents the central metabolic abnormality identified in adolescents with PCOS and may occur independently of obesity.
Pathophysiological Model
Obesity
Obesity affects a substantial proportion of adolescents with PCOS and amplifies reproductive and metabolic dysfunction [11].
Several studies have demonstrated:
- Increased visceral adiposity
- Elevated waist circumference
- Increased inflammatory markers
- Greater insulin resistance
Notably, lean adolescents may also develop PCOS, indicating that obesity is neither necessary nor sufficient for diagnosis [15].
Dyslipidemia
The most common lipid abnormalities include:
- Elevated triglycerides
- Reduced HDL cholesterol
- Elevated LDL cholesterol
- Increased non-HDL cholesterol
These alterations contribute to increased long-term cardiovascular risk [18].
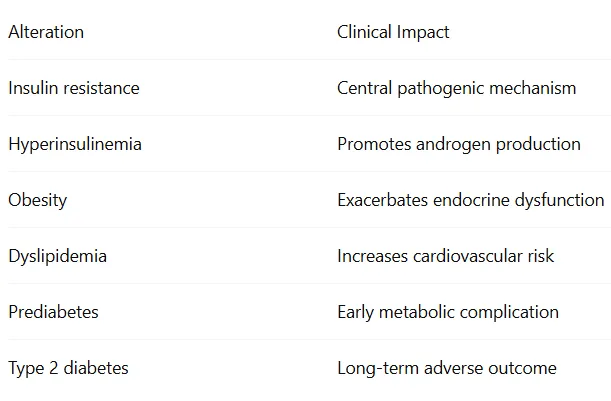
Glucose Metabolism Abnormalities
Adolescents with PCOS demonstrate higher prevalence of:
- Impaired fasting glucose
- Impaired glucose tolerance
- Hyperinsulinemia
- Type 2 diabetes mellitus
International guidelines recommend metabolic screening at diagnosis due to the elevated cardiometabolic burden associated with the syndrome [11].
Table 3. Major Metabolic Alterations in Adolescent PCOS
Psychological and Psychosocial Manifestations
One of the most underrecognized aspects of adolescent PCOS involves its psychological burden.
Recent international recommendations emphasize routine screening for mental health disorders because adolescents with PCOS demonstrate increased rates of anxiety, depression, body dissatisfaction, reduced self-esteem, and impaired quality of life [11].
Several factors contribute to psychological distress:
- Hirsutism
- Acne
- Obesity
- Menstrual irregularities
- Concerns regarding fertility
- Social stigma
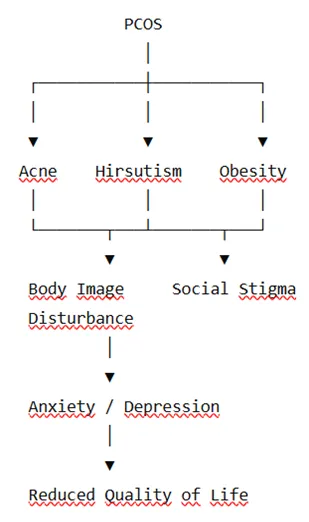
Figure 1. Psychological Consequences of Adolescent PCOS
Growing evidence suggests that psychological manifestations may emerge early and persist into adulthood if not adequately addressed [11,19].
Phenotypic Variability
The expression of PCOS differs substantially among adolescents.
Researchers generally recognize four major phenotypic patterns:
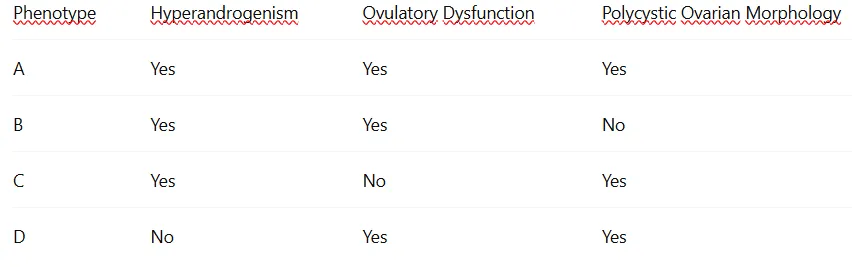
However, current adolescent guidelines caution against using ovarian morphology as a primary diagnostic criterion because multifollicular ovaries are common during normal pubertal maturation [10,11].
Consequently, adolescent diagnosis should prioritize persistent menstrual dysfunction and hyperandrogenism while excluding alternative causes of androgen excess.
The marked phenotypic heterogeneity observed worldwide underscores the need for individualized diagnostic and management approaches. Future multicenter studies incorporating genetic, metabolic, and environmental data may help refine phenotypic classification systems and improve risk stratification in adolescents with PCOS.
DISCUSSION
Polycystic ovary syndrome (PCOS) is increasingly recognized as one of the most prevalent endocrine disorders affecting adolescent females worldwide. The evidence analyzed in this review highlights the complexity of the syndrome, which extends beyond reproductive dysfunction and encompasses metabolic, dermatological, and psychological manifestations. The heterogeneity observed across studies reinforces the concept that PCOS should be regarded as a multifactorial and multisystem condition rather than a purely gynecological disorder [10,11].One of the principal findings emerging from the reviewed literature is the substantial variability in reported prevalence rates. Current estimates range from approximately 3% to 11%, depending largely on the diagnostic criteria applied [12]. This variation reflects one of the most significant challenges in adolescent PCOS research: the overlap between physiological pubertal changes and pathological manifestations of the syndrome. Azziz et al. emphasized that inconsistencies in diagnostic definitions have historically limited epidemiological comparisons and contributed to discrepancies in prevalence estimates across populations [20]. Similarly, recent international recommendations highlight that adult diagnostic criteria may not be entirely appropriate for adolescents because menstrual irregularities and multifollicular ovarian morphology frequently occur during normal pubertal maturation [11,27].The findings of this review further support the central role of hyperandrogenism in the pathogenesis and clinical expression of adolescent PCOS. Clinical manifestations such as hirsutism, persistent acne, and seborrhea remain among the most common reasons for medical consultation and often represent the earliest recognizable signs of disease [16,17]. Escobar-Morreale proposed that androgen excess functions as a pivotal biological mechanism linking reproductive dysfunction to broader metabolic disturbances [21]. Consequently, the identification and management of hyperandrogenism remain fundamental components of clinical care.Another important observation concerns the role of insulin resistance as a major pathogenic factor. Current evidence suggests that insulin resistance may be present even among adolescents with normal body mass index, indicating that metabolic dysfunction is not exclusively related to obesity [14,15]. Rosenfield and Ehrmann described how hyperinsulinemia stimulates ovarian androgen synthesis while simultaneously suppressing hepatic production of sex hormone-binding globulin, thereby increasing circulating free androgen concentrations and exacerbating clinical manifestations [22]. This pathophysiological model provides a coherent explanation for the close association between reproductive abnormalities and metabolic disturbances observed in affected adolescents.The relationship between obesity and PCOS remains particularly relevant given the global increase in pediatric and adolescent obesity. Although obesity is not considered a diagnostic criterion, it significantly amplifies insulin resistance, hyperandrogenism, chronic inflammation, and cardiometabolic risk [23]. Meta-analytic evidence has demonstrated that individuals with PCOS exhibit higher rates of central adiposity, metabolic syndrome, and cardiovascular risk factors compared with healthy controls [23]. Nevertheless, the existence of lean phenotypes highlights the complexity of disease pathogenesis and suggests that genetic and environmental factors play substantial roles independent of body weight.The metabolic implications of adolescent PCOS deserve particular attention because they may influence long-term health outcomes. Numerous investigations have reported increased prevalence of impaired glucose tolerance, dyslipidemia, metabolic syndrome, and type 2 diabetes mellitus among affected individuals [18,25]. Joham et al. emphasized that PCOS should be considered a lifelong condition associated with increased cardiometabolic risk extending well beyond the reproductive years [25]. Early identification of metabolic abnormalities may therefore provide opportunities for preventive interventions capable of reducing future morbidity and mortality.Psychological manifestations constitute another major component of the disease burden. The present review identified consistent evidence linking PCOS with elevated rates of anxiety, depression, body image dissatisfaction, reduced self-esteem, and impaired quality of life [19]. Dokras reported that psychological morbidity is substantially more common among individuals with PCOS than in the general population and may significantly influence treatment adherence and long-term outcomes [24]. These findings are particularly important during adolescence, a developmental stage characterized by heightened sensitivity to body image and peer perception. Consequently, comprehensive management strategies should include routine assessment of mental health and psychosocial well-being.The marked phenotypic heterogeneity observed among adolescents represents an additional challenge. Some individuals present predominantly reproductive manifestations, whereas others exhibit severe metabolic dysfunction despite relatively mild gynecological symptoms [14,15]. This variability likely reflects complex interactions among genetic susceptibility, intrauterine programming, lifestyle factors, ethnicity, and environmental exposures. Ibáñez et al. proposed that PCOS should be viewed as a developmental disorder influenced by early-life metabolic and endocrine disturbances that manifest clinically during adolescence and adulthood [31]. Such perspectives may help explain the broad spectrum of disease presentations observed across populations.Ethnic and geographic differences also contribute significantly to disease variability. Multicenter investigations have demonstrated important differences in prevalence, clinical presentation, and metabolic risk among populations from different regions of the world [13]. Adolescents of South Asian, Hispanic, and Middle Eastern ancestry frequently demonstrate greater insulin resistance and cardiometabolic risk than their European counterparts, whereas manifestations of hyperandrogenism may differ substantially among ethnic groups [25]. These findings underscore the necessity of considering population-specific characteristics when interpreting epidemiological data and implementing clinical guidelines.Despite substantial progress in understanding adolescent PCOS, several important knowledge gaps remain. First, the majority of available studies are cross-sectional, limiting the ability to establish causal relationships and evaluate disease progression over time [26]. Second, universally accepted biochemical thresholds for adolescent hyperandrogenism have not yet been established, contributing to diagnostic uncertainty. Third, the clinical utility of emerging biomarkers such as anti-Müllerian hormone, inflammatory mediators, metabolomic profiles, and genetic markers remains incompletely defined [27]. Future research should prioritize large-scale prospective multicenter studies capable of clarifying the natural history of the syndrome and identifying reliable predictors of long-term outcomes.Another area requiring further investigation involves the optimization of therapeutic strategies. Although lifestyle modification remains the cornerstone of management, evidence suggests that treatment responses vary considerably among patients [32]. Individualized approaches that consider phenotype, metabolic profile, psychological status, and reproductive goals may ultimately prove more effective than standardized interventions. The growing interest in precision medicine may therefore provide new opportunities for improving outcomes in adolescents with PCOS.he clinical implications of these findings are substantial. Early recognition of adolescents at risk for PCOS may facilitate timely interventions aimed at improving metabolic health, reducing psychological distress, and preventing future reproductive complications. Given the chronic nature of the syndrome and its association with long-term cardiometabolic morbidity, multidisciplinary care involving pediatricians, endocrinologists, gynecologists, nutritionists, psychologists, and primary care providers appears essential for optimal management.In conclusion, the evidence synthesized in this review supports the recognition of adolescent PCOS as a complex multisystem disorder with significant reproductive, metabolic, and psychological consequences. While recent international guidelines have improved diagnostic consistency, challenges related to disease heterogeneity, diagnostic uncertainty, and long-term management remain. Continued research focusing on adolescent-specific diagnostic tools, emerging biomarkers, and personalized therapeutic strategies will be crucial for improving clinical outcomes and reducing the global burden of PCOS.
CONCLUSION
Polycystic ovary syndrome (PCOS) represents one of the most prevalent endocrine disorders affecting adolescent females and constitutes a major clinical and public health challenge worldwide. The evidence reviewed in this study demonstrates that PCOS is a complex, multifactorial, and heterogeneous condition characterized by reproductive, metabolic, dermatological, and psychological manifestations that frequently emerge during adolescence and may persist throughout adulthood.The findings of this review indicate that the reported prevalence of adolescent PCOS varies considerably according to the diagnostic criteria employed, highlighting the importance of standardized diagnostic approaches specifically adapted to the adolescent population. Recent international recommendations have contributed significantly to improving diagnostic accuracy by emphasizing persistent menstrual irregularities and hyperandrogenism while minimizing the risk of overdiagnosis associated with physiological pubertal changes.Beyond its reproductive manifestations, PCOS should be recognized as a multisystem disorder with important metabolic implications. Insulin resistance, obesity, dyslipidemia, impaired glucose metabolism, and increased cardiometabolic risk are frequently observed among affected adolescents and may contribute to the development of long-term complications, including type 2 diabetes mellitus and cardiovascular disease. Furthermore, growing evidence underscores the substantial psychological burden associated with the syndrome, including increased rates of anxiety, depression, body image dissatisfaction, and reduced quality of life.The marked phenotypic variability observed across populations reflects the complex interaction between genetic susceptibility, endocrine dysfunction, metabolic disturbances, environmental exposures, and lifestyle factors. This heterogeneity reinforces the need for individualized diagnostic and therapeutic approaches capable of addressing the diverse clinical presentations encountered in daily practice.Despite important advances in understanding the pathophysiology and clinical characteristics of adolescent PCOS, several challenges remain. Diagnostic uncertainty during puberty, limited longitudinal data, and the absence of universally accepted biomarkers continue to hinder early identification and optimal management. Future multicenter prospective studies are needed to clarify the natural history of the syndrome, validate emerging diagnostic markers, and establish evidence-based personalized treatment strategies.In summary, adolescent PCOS should be considered a chronic multisystem disorder with significant reproductive, metabolic, and psychosocial consequences. Early recognition, comprehensive evaluation, and multidisciplinary management are essential to reduce disease burden, improve quality of life, and prevent long-term complications. Continued research and international collaboration will be fundamental to advancing knowledge, refining diagnostic criteria, and optimizing clinical outcomes for adolescents affected by this condition.
REFERENCES

Hellen Beatriz Guzmán Vergara, Diana Milena Alzate López, Efraín Martínez Moreno, Orlando Vargas Payares, Alder Gomez Angulo, Prevalence And Clinical Characteristics of Polycystic Ovary Syndrome In Adolescents: A Multicenter Narrative Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6687-6700, https://doi.org/10.5281/zenodo.20927170
 10.5281/zenodo.20927170
10.5281/zenodo.20927170