
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3UG Scholar, Dr. Rajendra Gode College of Pharmacy, Amravati, Maharashtra, India.
4Assistant Professor, Dr. Rajendra Gode College of Pharmacy, Amravati, Maharashtra, India.
5Principal, Dr. Rajendra Gode College of Pharmacy, Amravati, Maharashtra, India
Transdermal drug delivery is an attractive alternative to oral and parenteral administration due to its non-invasive nature, improved patient compliance, and avoidance of first-pass metabolism. However, the stratum corneum presents a major barrier to the transdermal transport of hydrophilic and macromolecular drugs. Microneedle (MN) technology has emerged as a promising approach to overcome this limitation by creating transient microchannels in the skin with minimal pain and tissue damage. Microneedles are micron-scale needle arrays capable of delivering a wide range of therapeutic agents, including small molecules, peptides, proteins, vaccines, and nucleic acids. This article reviews the principles of transdermal drug delivery using microneedles, with emphasis on types of microneedles (solid, coated, dissolving, hollow, hydrogel-forming, and porous), materials used, fabrication techniques, and mechanisms of drug transport. Recent advances in microneedle fabrication methods such as microelectromechanical systems (MEMS), micromolding, laser micromachining, and additive manufacturing are discussed. The clinical and therapeutic applications of microneedles in diabetes management, vaccination, cancer therapy, and delivery of biopharmaceuticals are highlighted. Despite challenges related to drug loading capacity, mechanical strength, manufacturing scalability, and regulatory approval, microneedle-based systems represent a versatile and promising platform for next-generation transdermal drug delivery.
Transdermal drug delivery has emerged as an attractive alternative to oral and parenteral routes, owing to its potential for painless administration, avoidance of first-pass metabolism, improved patient compliance, and the ability to maintain sustained plasma levels. However, the effectiveness of conventional transdermal systems is fundamentally constrained by the skin’s outermost barrier, the stratum corneum, which limits permeation, especially of hydrophilic and large-molecule therapeutics.¹-³
In this context, microneedle (MN) technologies have been increasingly explored as a minimally invasive hybrid between hypodermic needles and transdermal patches. These micron-scale arrays are designed to penetrate the stratum corneum and viable epidermis, thereby creating transient microchannels for enhanced drug transport with minimal pain and tissue trauma.⁴-⁶
The past decade has witnessed extensive developments in microneedle design, including various geometries (solid, coated, hollow, dissolving, and hydrogel-forming), materials (metals, silicon, and biodegradable polymers), and fabrication methods (micromoulding, photolithography, and 3D printing).⁷ These advances have enabled the delivery of small molecules, peptides, proteins, nucleic acids, vaccines, and other biopharmaceuticals that were traditionally challenging for transdermal administration.⁸
Moreover, microneedle-based systems are frequently combined with other enhancement strategies—such as iontophoresis, sonophoresis, and nanoparticle-assisted delivery—to further enhance drug permeation, control release kinetics, and broaden therapeutic applications.⁹
Despite these promising developments, translation into widespread clinical use remains limited due to challenges such as restricted drug loading capacity, scalability of manufacturing, sterilization requirements, regulatory hurdles, and concerns regarding long-term safety and biocompatibility.¹⁰-¹¹
For over 150 years, syringes and regular needles have been used to give medicines to people. The hollow needle was invented in 1844, and it completely changed how doctors treated patients. Even today, needles remain one of the most common ways to deliver drugs because many medicines can’t be taken by mouth—they may not absorb well in the stomach or may be broken down by enzymes before they can work.In the early days, syringes and needles were made entirely of metal and used a leather plunger to push the medicine out. These old devices were reused many times and were hard to clean properly. Modern syringes are much safer and easier to use—they are disposable and usually made from plastic, while the needles are made from stainless steel. The thinnest needles available, mostly used for insulin injections, are extremely small: about 254–305 micrometers wide (that’s about one-third of a millimeter).
Microneedles are much smaller versions of regular needles—tiny enough to painlessly pass through the outer layer of the skin. They’re being developed for delivering vaccines and drugs directly through the skin. The idea of using very small needles came up in the 1970s, but it wasn’t possible to make them until newer manufacturing techniques became available in the 1990s.
Today, scientists use methods from the microelectronics industry to make microneedles. Early versions were made from silicon because it was easy to shape precisely. Now, microneedles are often made from metals or polymers (special types of plastics).
There are two main types of microneedles: solid and hollow.
Solid microneedles can make tiny holes in the skin to help medicines pass through more easily, or they can be coated with dry medicine that dissolves after insertion.
Polymer microneedles can have the drug built inside them, which then dissolves or releases the medicine slowly after being inserted.
Hollow microneedles have a tiny channel inside, allowing liquid medicine to be injected directly into the skin.
Common materials for making microneedles include metals like stainless steel, titanium, and nickel-iron, as well as biodegradable or water-soluble polymers such as polycarbonate, PLGA, and carboxymethylcellulose.
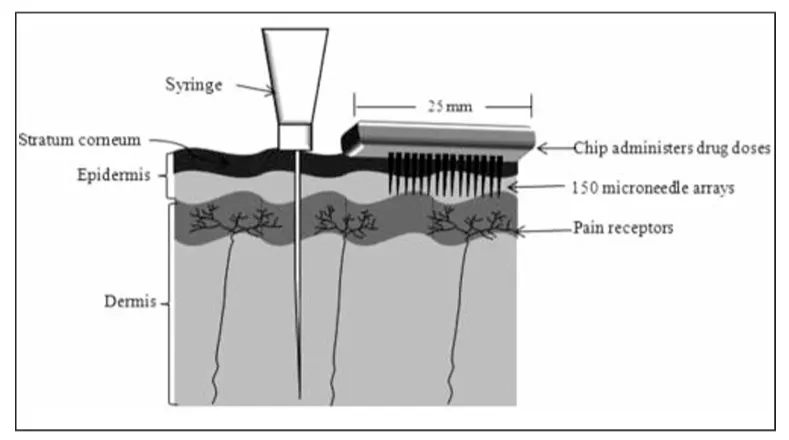
Figure: 1 Process of percutaneous absorption and transdermal delivery (I: Intercellular route, II: Transcellular route and III: Follicular route).12
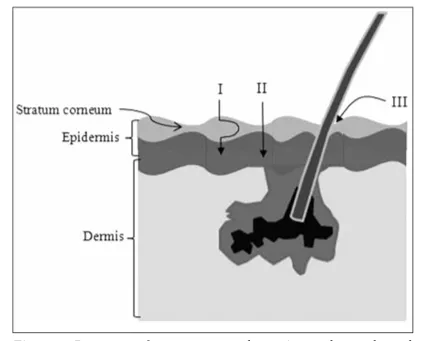
Figure 2: Comparison of a hypodermic syringe and microneedle arrays.12
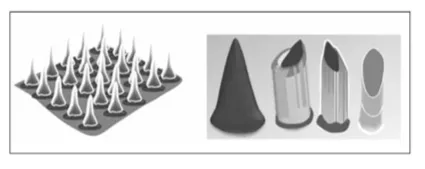
Figure 3: Examples of solid and hollow microneedle designs.12
Microneedles are tiny needle-like structures that can be made using a technology called microelectromechanical systems (MEMS). Their fabrication usually involves three main steps — deposition, patterning, and etching.
Deposition means forming very thin layers of material (from a few nanometers up to about 100 micrometers thick) on a surface.
Patterning is the process of creating specific shapes or designs on that layer. This is often done using lithography, where light or other types of radiation are used to transfer a pattern onto a light-sensitive material. There are different lithography methods like photolithography, electron-beam lithography, ion-beam lithography, X-ray lithography, and even diamond patterning.
Etching involves using chemicals or plasma to remove selected parts of the material, leaving behind the desired pattern. It can be done through wet etching (using liquids) or dry etching (using gases or plasma). The specific technique used depends on the microneedle material and its design.
Researchers have developed several methods to make microneedles from biodegradable polymers (materials that can safely break down in the body). For example, Park et al. made polymer microneedles using a micro-molding method. They first created molds with different tip shapes (like beveled, chisel, or cone-shaped) from materials such as SU-8 or polyurethane. Then, melted biodegradable polymer was poured into these molds under vacuum and heat. Once the polymer filled the mold, it was cooled and separated to form the final microneedles.
Aoyagi et al. explored laser-based microneedle fabrication and found that making microneedles under normal air conditions caused unwanted chemical reactions in polylactic acid (PLA). However, when the process was done in a vacuum, these reactions didn’t occur, resulting in better-quality needles.
Donnelly et al. used laser micromachining to create silicon molds for microneedles and then filled these molds with polymer blends to form the needles. Other techniques for making polymer microneedles include casting, injection molding, and hot embossing.
Finally, Chen et al. developed a gas-jet coating method to evenly coat microneedles with biological materials such as vaccines, DNA, and proteins, making them useful for delivering therapeutic agents.
Overview of fabrication approaches
Fabrication of microneedles (MNs) spans microfabrication (MEMS/lithography/etching), micromolding/replica casting, subtractive machining and laser ablation, and additive manufacturing (3D printing). Choice of method depends on needle geometry, material (silicon, metals, ceramics, polymers, sugars, hydrogels), intended dose/release mechanism (solid/coated, hollow, dissolving, hydrogel), mechanical strength requirements, and throughput. Recent reviews stress that combining methods (e.g., 3D-printed masters + micromolding) often gives the best balance between geometric control and scalable production.
MEMS, photolithography and silicon-based microfabrication
Early and high-precision MNs were made using MEMS techniques on silicon wafers — photolithography, deep reactive ion etching (DRIE), wet anisotropic etching, and electrochemical etching are common. These methods give excellent dimensional control and sharp tips suitable for hollow and solid MNs, but silicon is brittle, requires cleanroom facilities, and can be expensive for mass production; hence, silicon processes are often used to create masters or molds rather than final, disposable devices.
Micromolding and replica casting (polymers, sugars, dissolving MNs)
Micromolding (replica molding) is the dominant route for polymeric and dissolving MNs. A hard master (silicon, metal, or 3D-printed mold) is used to produce an elastomeric negative (e.g., PDMS), which becomes the reusable mold for casting polymer, sugar or gel formulations. For dissolving MNs, aqueous polymer/drug formulations (e.g., PVA, PVP, carboxymethylcellulose) are cast into molds, centrifuged or vacuum-filled, dried, and demolded — sometimes in multi-step layering to localize drug to needle tips. Micromolding is relatively low-cost, scalable (roll-to-roll or multi-cavity molds), and compatible with many drug-loaded matrices.
3D printing / additive manufacturing
Additive manufacturing (stereolithography, two-photon polymerization, digital light processing, fused deposition modeling) has rapidly advanced MN fabrication by enabling rapid prototyping and complex geometries (tapered, hollow, porous, interlocking shapes). Two-photon polymerization gives sub-micron resolution for research masters; DLP/SLA offer a balance of resolution and speed for production of master molds or direct printing of polymer MNs. 3D printing simplifies iteration and personalized geometries but materials (biocompatibility, mechanical strength) and throughput remain considerations for clinical translation.
Laser micromachining, milling and subtractive approaches
Laser ablation and micro-milling are used to shape metallic or polymer blanks into MNs or to create master molds. Laser cutting is useful for flat or in-plane MNs from metal sheets; precision milling provides good mechanical strength for metal/hollow MNs. These methods are flexible for small-batch and custom designs but can be slower or more costly for very high-volume manufacture than molding approaches.
Coating and drug-loading techniques
For coated MNs, solution coating (dip-coating, spray coating, inkjet deposition, and electrostatic deposition) is used to load drug on needle surfaces; controlling coating thickness and uniformity is essential for dose consistency. For dissolving MNs, drug is mixed into the polymer matrix or localized to the needle tips via layer casting or tip-filling methods. Hollow MNs are filled via microfluidic or syringe loading and can deliver bolus or infusion doses. Each approach requires optimization to prevent loss of bioactivity (stability), to ensure accurate dose, and to maintain mechanical integrity.
Hydrogel-forming and swellable MN fabrication
Hydrogel-forming MNs (crosslinked polymers that swell upon insertion) are typically fabricated by casting prepolymer solutions into molds followed by controlled crosslinking (thermal, UV or chemical). Crosslink density, swelling kinetics, and pore structure are tuned to control uptake and diffusion from an attached reservoir. Hydrogel MNs avoid leaving residue in skin (no needle remnants) and can enable sustained release, but their mechanical performance during insertion and swelling must be validated.
Quality control, characterization and scale-up considerations
Key QC tests include mechanical strength/fracture testing (axial and transverse forces), insertion/penetration assessment (optical coherence tomography, histology), dose uniformity (for coated/dissolving MNs), residual material analysis, sterility, and dissolution/release profiling. For industrial scale-up, mold durability, batch-to-batch reproducibility, GMP-compliant drying/packaging, and sterilization compatibility (e.g., terminal sterilization vs aseptic processing) are critical. Hybrid manufacturing (3D-printed masters + high-throughput molding) and roll-to-roll molding are promising routes to reconcile precision with volume.
Challenges and emerging directions in fabrication
Remaining fabrication challenges include (1) achieving higher drug loading for systemic delivery while maintaining mechanical strength, (2) manufacturing cost reduction for single-use patches, (3) maintaining labile biologic stability in polymer matrices, (4) ensuring uniform insertion across skin types, and (5) integrating sensing or microfluidics (closed-loop or combined diagnostic/therapeutic MNs). Ongoing work focuses on advanced polymers, stimuli-responsive formulations, automated coating/printing for precise dosing, and regulatory-driven process validation.14-23
The main idea behind microneedles is to deliver medicines into the skin in a minimally invasive way—that is, without causing pain or damage like regular needles do. To achieve this, researchers have explored several different methods for using microneedles in drug delivery.
One common method involves using solid microneedles made of materials like silicon or metal to create tiny holes in the skin. After making these holes, a drug patch is placed on the skin’s surface so that the medicine can move through the openings. This movement can happen naturally through diffusion, or it can be sped up by applying a small electric current, a process called iontophoresis.
Another approach, called “coat and poke,” involves coating the microneedles with the drug before inserting them into the skin. In this case, the medicine is carried entirely on the needle itself—there’s no patch or extra reservoir on the skin. A similar technique, known as “dip and scrape,” dips the needles into a drug solution and then gently scrapes the skin so that the medicine gets deposited in the small scratches made by the needles.
Researchers have also experimented with hollow microneedles, which work more like miniature versions of hypodermic needles. These allow liquids to flow directly through the hollow center of the needle into the skin. Although they are more complex to design and use, they can deliver drugs much faster and in controlled amounts over time.
The following sections summarize published research on using microneedles to deliver various substances—such as drugs, proteins, DNA, and vaccines—through the skin. The focus is on studies that actually test how well microneedles deliver medicine, rather than on engineering papers that only describe new needle designs. Likewise, it does not include unpublished or confidential company research that has not yet been made publicly available.26
Overview — functional and material classifications
Microneedles (MNs) are commonly classified both by their function/release mechanism (solid, coated, hollow, dissolving, hydrogel-forming, porous, swellable/detachable) and by material/geometry (metallic, silicon, ceramic, polymeric, sugar; in-plane vs out-of-plane designs). Each class offers different payload capacity, release kinetics, mechanical strength and manufacturing requirements — therefore type selection depends on the therapeutic goal (bolus vs sustained release, vaccine vs biologic vs small molecule) and regulatory/manufacturing considerations.27-28
Solid (poke-and-patch) microneedles
Solid MNs are solid projections used to pre-treat (poke) the skin to create microconduits through the stratum corneum; after removal a drug patch or topical formulation is applied to the treated site for passive diffusion. Solid MN arrays are mechanically robust and simple to produce (metal or silicon), but they do not directly carry drug in the needle matrix and thus require a two-step application.29-30
Coated microneedles
Coated MNs are solid needles whose surfaces are coated with drug formulations (solutions, suspensions, or dried films). Upon insertion the coating dissolves rapidly, delivering a defined, usually low, dose of drug to the epidermis/dermis. Coating techniques include dip-coating, spray-coating, inkjet and electrostatic deposition; controlling coating thickness and uniformity is critical for dose accuracy. Coated MNs are attractive for vaccine dose-sparing and quick release but have limited payload capacity relative to dissolving designs.31-32
Dissolving / biodegradable microneedles
Dissolving MNs are fabricated from water-soluble or biodegradable polymers/sugars (PVP, PVA, CMC, trehalose, etc.) that encapsulate drug within the needle matrix and fully dissolve in the skin after insertion, leaving no sharps waste. They support secure single-use delivery, potential for higher tip-loaded doses (via tip-filling), and improved stability for some vaccines/biologics when formulated appropriately, though formulation stability and moisture sensitivity are key challenges.33-35
Hollow microneedles (microinjection / sampling)
Hollow MNs contain an internal bore and act as miniature hypodermic needles to inject liquid formulations or withdraw interstitial fluid. They permit controlled bolus or infusion dosing and integration with microfluidic pumps and sensors. Fabrication (DRIE, laser drilling, two-photon 3D printing, micro-milling) and mechanical robustness (avoiding tip collapse) are central engineering challenges. Hollow MNs are used where higher liquid doses or sampling (diagnostics) are required.36-38
Unlike solid microneedles, hollow microneedles have a tiny channel inside them that allows medicines or other substances to flow through. These hollow needles can deliver drugs into the skin either slowly by diffusion or quickly by applying pressure. Although many types of hollow microneedles have been created, only a few studies have looked at how well they work for delivering drugs into the skin.
In one study, McAllister and colleagues tested a single glass microneedle to inject insulin into the skin of diabetic hairless rats. The insulin was delivered over 30 minutes, and the rats’ blood sugar levels dropped by up to 70% within five hours after treatment. The needles were made with very fine tips (around 60 micrometers wide) and were inserted about 500–800 micrometers deep into the skin. This experiment proved that hollow microneedles can successfully inject drugs through the skin.
Other researchers have explored similar uses. Stoeber and Liepmann injected liquids into chicken tissue using microneedle arrays, while Chen and Wise used microneedles to deliver chemical substances into brain tissue. Smart and Subramanian used single microneedles to draw very small amounts of blood from the skin for glucose testing.39
Hydrogel-forming and swellable microneedles
Hydrogel-forming MNs are crosslinked polymer networks that swell upon insertion and act as conduits/reservoirs for drug diffusion from an attached reservoir (or for interstitial fluid extraction). HFMs do not dissolve or leave residue in skin and enable sustained release or biosensing; their properties depend on polymer chemistry, crosslink density and swelling kinetics. They are appealing for sustained delivery and sampling applications but require careful control of insertion mechanics and swelling behavior.40-42
Porous and matrix-type microneedles
Porous MNs (ceramic or polymeric) contain micro-/nano-porosity that allows fluid uptake and diffusion, enabling sustained release or fluid sampling. Matrix-type MNs (similar to dissolving) embed drug within a porous scaffold that gradually releases payload by diffusion or erosion. Porous architectures increase surface area and can be engineered for controlled release profiles but may compromise mechanical strength if porosity is too high.43,44
Swellable, separable (detachable) and arrowhead microneedles
Some MNs are designed to detach from their backing after insertion (separable or “arrowhead” designs) so that drug-loaded tips remain embedded as depot implants while the base is removed. Swellable or semi-dissolving hybrid MNs combine fast tip dissolution with a robust base to tune delivery. These approaches expand dosing capacity and enable prolonged local release or depot formation for sustained therapy.45,46
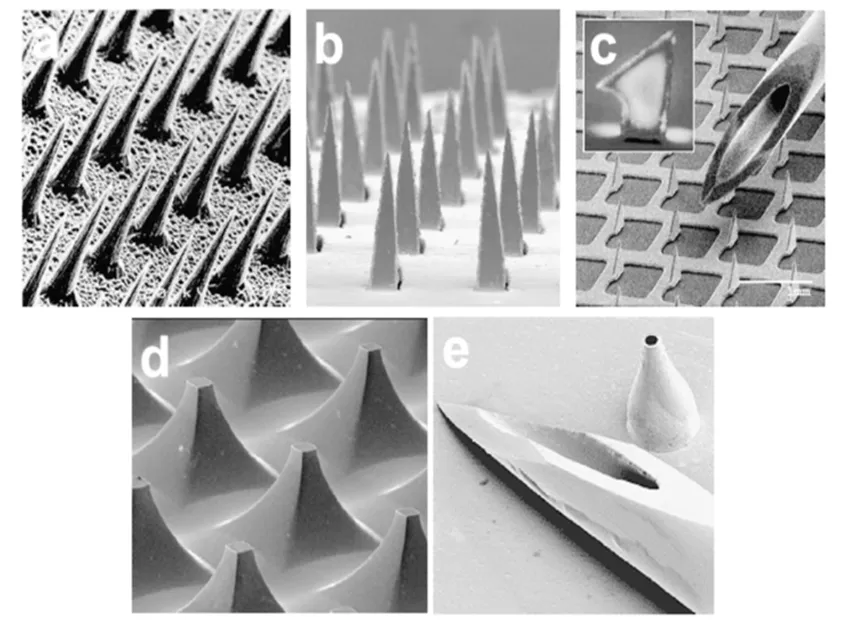
Figure 4: Images of microneedles used for transdermal drug delivery. (a) Solid microneedles (150 Am tall) etched from a silicon wafer were used in the first study to demonstrate microneedles for transdermal delivery. (b) Solid microneedles (1000 Am tall) laser-cut from a stainless steel sheet were used to deliver insulin to diabetic rats. (c) Solid microneedles (‘‘microprojection array’’, 330 Am tall) acid-etched from a titanium sheet were coated with protein antigen for vaccine delivery in vivo; similar needles were used to deliver oligonucleotides in vivo. (d) Solid microneedles (‘‘microenhancer array’’, 200 Am tall) chemically etched from a silicon wafer were dipped in plasmid DNA solution for vaccine delivery in vivo. (e) Hollow microneedles (500 Am tall) formed by electrodeposition of metal onto a polymer mold were used for needle insertion and fracture force measurements47
While most research on microneedles has focused on how they’re made and how well they deliver drugs, the actual process of how these tiny needles enter the skin hasn’t been studied as much — even though it’s a key part of making them work effectively. For microneedles to successfully pierce the skin, their shape and physical strength have to be just right. Some designs can be pushed into the skin by hand, but others need to be inserted quickly or with extra force. If too much force is required, the needles can bend or break before they manage to go in.
A study by Davis and colleagues looked closely at these mechanical aspects. They measured how much force was needed for a microneedle to break, how much force was needed to insert it into the skin, and compared the two values. This comparison was called the margin of safety — meaning how much stronger the needle is than the force required to insert it.
In their tests, they used tiny hollow metal needles that were about 500 micrometers long (roughly the width of a few human hairs). The tips ranged from 30 to 80 micrometers in radius, and the walls varied from very thin (5 micrometers) to solid.
When testing on human skin, they measured how much force it took for the needles to actually break through the surface. The required force ranged from about 0.1 to 3 newtons (roughly 10 to 300 grams of pressure), and it increased in proportion to the size of the needle tip. Interestingly, how thick the needle walls were didn’t affect how easily the needle went in — meaning that the skin didn’t bend inward to fill the hollow part of the needle.
They also tested how strong the needles were by pressing them against a hard surface until they snapped. The breaking force ranged between 0.5 and 6 newtons. Needles with thicker walls were much stronger, and those with wider angles at the tip were slightly stronger. However, the sharpness (tip radius) didn’t really change the breaking force.
Finally, when comparing breaking force to insertion force, they found that most microneedles were strong enough to safely enter the skin without breaking — in fact, many had a margin of safety greater than one, and some were over ten times stronger than needed. The best designs had sharp, narrow tips (to make insertion easier) and thick walls (to make them stronger).47
1. Skin barrier and overall principle
Transdermal uptake is normally restricted by the stratum corneum — a 10–20 µm, highly lipophilic barrier of corneocytes and lipid lamellae — which blocks hydrophilic and large molecules. Microneedles (MNs) mechanically breach the stratum corneum to form micron-scale conduits that permit direct transport into the viable epidermis and upper dermis, thereby enabling local delivery or entry into dermal capillaries for systemic absorption while avoiding the pain and invasiveness of hypodermic needles.
2. Solid (poke-and-patch) and coated MN mechanism
Solid MNs operate by creating microchannels in the skin (poke-and-patch): after removal of the array, a drug formulation applied over the treated area diffuses through these channels into the viable skin. Coated MNs carry drug on the needle surface; upon insertion the coating rapidly dissolves in interstitial fluid and releases a defined, usually low, dose into the epidermis/dermis. Both approaches rely principally on passive diffusion through MN-created microconduits, with coated MNs offering single-step delivery and faster onset.
3. Dissolving/biodegradable MN mechanism
Dissolving MNs are composed of water-soluble or biodegradable matrices that encapsulate the therapeutic. Once inserted, the matrix absorbs skin fluid and dissolves (or degrades), releasing the payload directly into the tissue; dissolution kinetics (and thus release profile) are controlled by polymer chemistry, needle geometry and formulation additives. Because the needle matrix dissolves, these systems avoid sharps waste and can be engineered to concentrate drug at the needle tip (tip-loading) for efficient delivery.
4. Hollow MNs — microinjection and infusion
Hollow MNs contain an internal lumen and enable direct fluid flow into the dermis (microinjection) or sampling of interstitial fluid. Delivery is driven by applied pressure or a pump and can be controlled as a bolus or infusion; the mechanism is therefore similar to miniature hypodermic injection but with much smaller insertion depth and typically lower volumes/rates. Hollow designs permit larger liquid doses and integration with microfluidic systems but require robust wall strength to avoid tip collapse.
5. Hydrogel-forming MNs — swelling-mediated transport
Hydrogel-forming MNs (HFMs) are crosslinked polymeric needles that do not dissolve but rapidly swell on uptake of interstitial fluid, creating a continuous, hydrated hydrogel conduit between an external reservoir (or drug-loaded backing) and the dermis. Drug diffuses through the hydrated network into skin; HFMs can enable sustained, controlled release or sampling while leaving no solid residues in skin. Swelling kinetics, crosslink density and mesh size set the transport rates.
6. Porous, matrix and separable-depot MNs
Porous MNs use a micro-porous architecture (ceramic or polymeric) to permit capillary-driven fluid uptake and diffusion, supporting sustained release or sampling. Separable (or arrowhead) MNs and separable-tip designs intentionally leave a drug-loaded fragment (tip) embedded as a micro-depot that then releases drug by diffusion or erosion over time—this is a hybrid between implant and transdermal approaches designed to increase dose capacity and prolong local therapy.
7. Biological and immunological mechanisms (vaccines & adjuvant effects)
When MNs are used for vaccine delivery, antigen delivery to abundant antigen-presenting cells (Langerhans cells in the epidermis and dermal dendritic cells) often produces potent immune responses with dose-sparing potential. The localized, intradermal deposition of antigen and adjuvants—plus the transient, local inflammatory signals from tissue disruption—facilitate antigen uptake, migration to lymph nodes and adaptive immune activation, explaining the favorable immunogenicity shown in many preclinical and clinical studies.
8. Transport kinetics: diffusion, dissolution, convection & capillary uptake
Transport through MN-created conduits combines multiple physical processes: (i) rapid dissolution of coatings or matrices releases payload into interstitial fluid; (ii) molecular diffusion through hydrated tissue or hydrogel networks controls local spread; (iii) convection/pressure-driven flow (in hollow MNs) governs infusion; and (iv) capillary action in porous structures assists uptake/sampling. The relative contribution of each depends on MN type, geometry, drug physicochemistry, and applied mechanical/pressure conditions.
9. Factors that govern successful penetration and transport
Key mechanical and design factors determine effective breach and subsequent delivery: needle length, tip sharpness and bevel, array density, base support (backing stiffness), insertion velocity/force, and skin site/thickness. Skin biomechanics (age, hydration, anatomical site) and application method (manual vs applicator) influence whether needles fully penetrate without buckling or fracture; incomplete insertion reduces delivered dose and reproducibility.
10. Barrier recovery, healing and safety mechanisms
After MN removal (or after matrix dissolution/swelling), the microchannels typically reseal within hours to days depending on initial depth and skin condition; re-epithelialization and lipid matrix restoration restore the barrier. Infection risks are low with proper handling because channels are transient and shallow, but sterility, formulation microbial limits, and handling protocols remain critical for clinical use. Mechanical failure (needle fracture and retained fragments) is a safety concern that drives material choice and mechanical testing standards.
11. Modeling, in vitro–in vivo correlation and translational considerations
Mechanistic models combining insertion mechanics, dissolution/swelling kinetics and diffusion/convection equations are used to predict dose delivered and PK profiles; however, inter-subject variability in skin properties complicates IVIVC. For clinical translation, robust characterization (mechanical testing, OCT imaging of penetration, dissolution assays, PK studies) and reproducible manufacturing are required to ensure consistent mechanistic performance across populations.48
In the early stages of microneedle research, solid microneedle arrays made from silicon were used to pierce the skin and bypass the tough outer layer called the stratum corneum. After creating these tiny holes, a medicated patch was placed on the treated area to deliver the drug — this method is called the “poke and patch” technique. The same method was also tested for drawing out interstitial fluid to check glucose levels without using needles.
Later, scientists developed “coat and poke” microneedles. In this approach, the needles were coated with a thin layer of drug using a dip-coating process. Once inserted into the skin, the coating dissolved and released the medicine. However, only a small amount of drug (around 1 mg) could be applied this way, and getting a uniform coating required careful optimization.
Further advancements led to the “poke and release” method. Here, microneedles were made from biodegradable materials like polymers or sugars that slowly dissolved in the skin after insertion, gradually releasing the drug. The main benefit of this technique was that the release rate could be controlled by adjusting the material, but it still couldn’t deliver large doses of medicine.
To solve this limitation, researchers created hollow microneedles — the “poke and flow” technique. These tiny needles had channels through which liquid drugs could flow from a reservoir patch into the skin after insertion. For example, Wang and colleagues designed a hollow microneedle system with a built-in drug reservoir that released the medicine when gentle pressure was applied. The holes in these needles were usually placed on the side rather than at the tip to make insertion easier and reduce clogging.
The overall design of microneedles is very important — they must be strong enough not to break but also gentle enough not to cause pain or irritation. Depending on the type, microneedles can be used for delivering drugs throughout the body or targeting a specific area.49
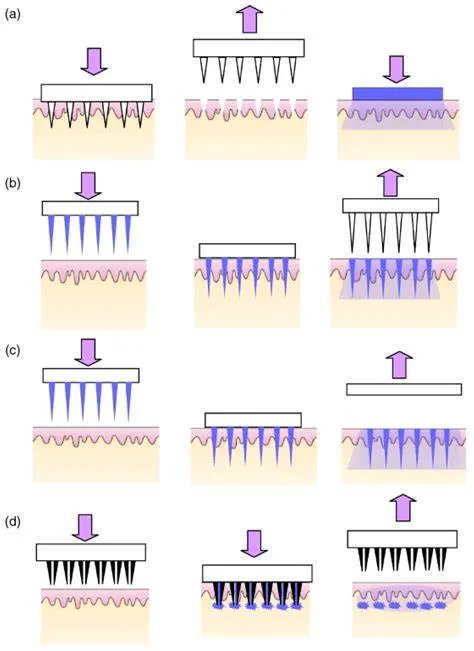
Figure:4 Approaches for drug delivery by different designs of microneedles: (a) ‘poke and patch’ using solid microneedles, (b) ‘coat and poke’ using coated solid microneedles, (c) ‘poke and release’ using polymeric microneedles, (d) ‘poke and flow’ using hollow microneedles.49
Microneedle-based and transdermal drug delivery systems are modern methods that help medicines pass through the skin into the body. They combine the benefits of traditional skin patches with new microneedle technology, giving several clear advantages over regular injections or tablets.
1. Less Painful and Gentle on Skin:
Microneedles are tiny and only go into the upper layer of the skin. They don’t reach the nerves or blood vessels, so the process is almost painless and much more comfortable than injections.
2.Avoids Liver Breakdown:
When drugs enter the body through the skin, they bypass the liver at first. This means more of the medicine stays active and reaches the bloodstream, instead of being partly broken down before it can work.
3. Helps More Medicine Get Through the Skin:
The small holes made by microneedles allow larger or water-loving drug molecules to enter the body more easily, which is difficult with normal patches.50
4. Can Release Medicine Slowly:
Microneedle patches can be designed to release medicine slowly over time. This helps maintain steady drug levels and reduces how often doses are needed.
5. Safer and Cleaner:
Because microneedles don’t go deep into the skin, they reduce the risk of bleeding, infection, or accidental injuries that can happen with regular needles.
6. Easy to Use by Patients:
People can easily apply microneedle patches on their own without help from medical staff, making treatment more convenient and accessible.
7. Can Deliver Many Types of Medicines:
Microneedles can carry different kinds of drugs—such as vaccines, proteins, peptides, and small-molecule medicines—making them useful for a wide range of treatments.51
1. Limited Drug Load:
Microneedles can only deliver small amounts of drug at a time, making them less suitable for medications that require high doses.
2. Skin Irritation and Sensitivity:
Some individuals may experience redness, itching, or irritation at the site of application. Repeated use could worsen skin reactions in sensitive patients.
3. Mechanical Weakness and Breakage Risk:
Microneedles must be strong enough to penetrate the skin but can sometimes break or bend, which may reduce effectiveness or pose safety concerns.
4. Cost of Fabrication:
Manufacturing microneedle patches requires specialized equipment and materials, making them more expensive than conventional transdermal patches or oral medications.
5. Limited Drug Types:
Not all drugs are suitable for microneedle delivery. Large or highly hydrophobic molecules may have difficulty passing through microchannels.
6. Storage and Stability Issues:
Some microneedle formulations, especially those containing proteins or vaccines, may require strict storage conditions to remain effective.52
1. Insulin (Diabetes) Delivery
Microneedle patches have been widely studied to deliver insulin transdermally. Because microneedles can bypass the stratum corneum barrier and deliver macromolecules like insulin painlessly and in a controlled manner, they offer a promising alternative to daily subcutaneous injections, improving patient compliance and reducing the risk of injection-related complications.
2. Vaccine / Immunization
Microneedle arrays are being leveraged for cutaneous (intradermal) vaccination. The skin is rich in immune cells (like dendritic cells and Langerhans cells), so delivering vaccines via microneedles can generate strong immune responses, often with lower doses than traditional intramuscular injections. Furthermore, some microneedles can carry vaccine antigens in a dry, stable form, improving thermal stability and ease of transport/storage.
3. Cancer Therapy:
Microneedles are being explored for localized delivery of anticancer agents (e.g., chemotherapeutic drugs, cancer vaccines, gene therapy) through the skin. This approach reduces systemic toxicity, allows targeted delivery, and may improve patient comfort compared to systemic chemotherapy or frequent injections.
4. Delivery of Biopharmaceuticals / Large Molecules
Many therapeutic biomolecules—proteins, peptides, antibodies, oligonucleotides—are difficult to deliver via classical transdermal patches because of their size and hydrophilicity. Microneedles (solid, dissolving, hollow, swelling, etc.) can increase delivery efficiency of such macromolecules, preserving their stability (e.g., by encapsulation), reducing degradation, and enabling controlled release.
5. Antihypertensive Drug Delivery
Specific small-molecule drugs (such as antihypertensives) with poor aqueous solubility or low bioavailability have been formulated in microneedle systems. The microneedle route can help to bypass first-pass metabolism, improve pharmacokinetics, and increase patient adherence (painless application, less frequent dosing).53
CONCLUSION
Microneedle-based transdermal drug delivery systems represent a significant advancement in overcoming the limitations of conventional transdermal and injectable therapies. By creating transient microchannels across the stratum corneum, microneedles enable efficient, minimally invasive, and largely pain-free delivery of a wide range of therapeutic agents, including small molecules, peptides, proteins, vaccines, and nucleic acids. The versatility of microneedle technology is evident from the diverse types developed—solid, coated, dissolving, hollow, hydrogel-forming, and porous—each offering distinct advantages in terms of drug loading, release kinetics, safety, and patient acceptability.
Substantial progress in materials science and fabrication technologies, such as MEMS-based microfabrication, micromolding, laser micromachining, and additive manufacturing, has facilitated precise control over microneedle geometry, mechanical strength, and functionality. These advances have expanded clinical and therapeutic applications ranging from vaccination and diabetes management to cancer therapy and delivery of biopharmaceuticals. Moreover, integration with enhancement techniques and smart systems (e.g., microfluidics and biosensing) further broadens the potential of microneedle platforms.
Despite these promising developments, challenges related to limited drug loading capacity, large-scale manufacturing, long-term stability of biologics, sterilization, and regulatory approval continue to hinder widespread commercialization. Addressing these issues through optimized formulations, hybrid manufacturing strategies, and robust quality control will be critical for successful clinical translation. Overall, microneedle technology holds strong promise as a next-generation transdermal drug delivery platform, with the potential to transform patient-friendly, controlled, and effective therapeutic administration in the future.
REFERENCES

Apurva Khandare *, Sakshi Dindokar, Vaishnavi Deshmukh, N. Wakchaware, H. Sawarkar., Recent Advances in Microneedle Technology for Transdermal Drug Delivery: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3579-3595. https://doi.org/ 10.5281/zenodo.20701287
 10.5281/zenodo.20701287
10.5281/zenodo.20701287