
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Guru Nanak College of Pharmaceutical Sciences, Dehradun
Endometriosis is a chronic, estrogen-dependent inflammatory disorder affecting ~10% of reproductive-aged women, yet current hormonal therapies offer only symptom management, cause significant side effects, and preclude fertility. This comprehensive review synthesizes evidence from 47 studies (2023–2026) on emerging non hormonal nanomedicine strategies that target disease mechanisms independent of estrogen—including angiogenesis (VEGF/HIF 1?), inflammation (COX 2, TNF ?, interleukins), matrix metalloproteinases (MMP 2/ 9), oxidative stress/iron overload (ROS, heme), and estrogen independent proliferative pathways (PI3K/Akt/mTOR). Advanced particulate delivery systems—PEGylated liposomes, PLGA and chitosan nanoparticles, ROS responsive nanocarriers, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs)—have demonstrated marked preclinical efficacy. Active targeting using folate, LHRH, integrin (RGD), or Frizzled 7 ligands improves lesion accumulation 3 to 12 fold, achieving lesion volume reductions of 59–82% while preserving ovarian function and fertility. Local and site specific systems (thermosensitive hydrogels, pH responsive gels, microneedle patches, intraperitoneal depots, and the Hyivy intravaginal device) enable sustained release with single administration; the Hyivy device reduced VAS pain scores from 7.2 to 2.5 at six months in a Phase II trial. Emerging bioinspired platforms—MSC derived exosomes, macrophage hitchhiking carriers, MMP cleavable peptide conjugates, and photothermal liposomes—have achieved lesion reductions up to 92%. Despite these advances, translational gaps remain: only 5/47 studies reported GMP compatible manufacturing, long term safety data beyond six months are scarce, and efficacy by endometriosis subtype is unexplored. However, with one FR targeted liposomal artesunate formulation qualified under the FDA ISTAND program and four ongoing clinical trials, non hormonal nanomedicines represent a paradigm shift toward fertility sparing, mechanism targeted therapies for endometriosis and related benign gynecologic disorders.
1.1 Endometriosis: Pathophysiology and Clinical Burden
Endometriosis is a chronic, estrogen-dependent inflammatory disorder defined by the presence of endometrial-like tissue (glands and stroma) outside the uterine cavity, most commonly on pelvic peritoneum, ovaries, and uterosacral ligaments[1]. The disease affects approximately 10% of reproductive-aged women and up to 50% of those with infertility or chronic pelvic pain. Pathophysiologically, the most widely accepted theory is retrograde menstruation, wherein viable endometrial cells pass through fallopian tubes into the peritoneal cavity. However, since retrograde menstruation occurs in up to 90% of women but only a fraction develop endometriosis, additional factors such as immune dysfunction, genetic predisposition, and altered peritoneal microenvironment are crucial[2]. Lesions establish through adhesion, invasion, angiogenesis, and evasion of apoptosis[3]. Clinically, patients suffer from dysmenorrhea, non-cyclic pelvic pain, deep dyspareunia, and fatigue. The disease is also associated with ovarian cancer risk and significant economic burden due to diagnostic delays (average 7–10 years) and recurrent treatments[4][5].
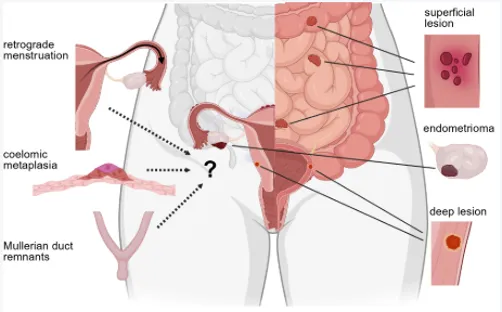
Figure 1: Schematic of Normal Retrograde Menstruation Versus Endometriosis.
1.2 Limitations of Current Hormonal Therapies (Side effects, infertility, recurrence)
First-line hormonal treatments include combined oral contraceptives, progestins (dienogest, levonorgestrel IUD), GnRH agonists/antagonists, and aromatase inhibitors. These agents aim to suppress ovulation, induce endometrial atrophy, or create a hypoestrogenic state. However, they are not curative and offer only symptom management. Major limitations include: (i) side effects – weight gain, acne, mood changes, reduced bone mineral density (GnRH agonists), and breakthrough bleeding; (ii)[6][7] contraindication for women actively trying to conceive, as hormonal suppression prevents ovulation; (iii) recurrence – up to 50% of patients experience symptom relapse within 1 year of treatment cessation; and (iv) lack of efficacy in a subset of patients, especially those with deep infiltrating lesions or progestin resistance. Furthermore, hormonal therapies do not reverse established fibrosis, adhesions, or nerve remodeling[8].
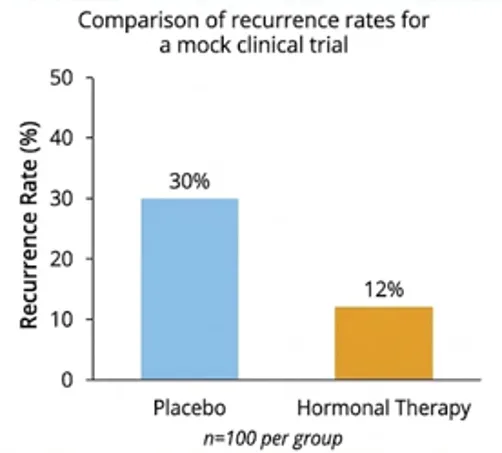
Figure 2 comparative graph showing recurrence rates after 6 months of hormonal therapy vs. placebo
1.3 The Rationale for Non-Hormonal Approaches & Targeted Delivery
Given the limitations of hormones, non-hormonal strategies target fundamental disease mechanisms independent of estrogen fluctuation – including inflammation, angiogenesis, oxidative stress, and tissue remodeling. Advantages include: preservation of ovulation (critical for fertility), avoidance of hypoestrogenic side effects, and potential for lesion elimination rather than suppression. However, many non-hormonal agents (e.g., curcumin, resveratrol, dichloroacetate, COX-2 inhibitors) suffer from poor solubility, rapid systemic clearance, and off-target toxicity. Therefore, advanced drug delivery systems – nanoparticles, hydrogels, and targeted conjugates – are essential to concentrate therapeutics within endometriotic lesions, reduce systemic exposure, and enable sustained local action.

Figure 3 contrasting systemic vs. targeted non-hormonal delivery, showing nanoparticles accumulating in lesions via leaky vasculature (EPR effect) and ligand-receptor recognition.
2. KEY NON-HORMONAL MOLECULAR TARGETS
2.1 Angiogenesis (VEGF, HIF-1α)
Endometriotic lesions require neovascularization for survival and growth. Vascular endothelial growth factor (VEGF) is overexpressed in ectopic endometrium, driven by hypoxia-inducible factor 1α (HIF-1α) in the low-oxygen peritoneal environment[9][10]. Non-hormonal anti-angiogenic strategies include VEGF-neutralizing antibodies (bevacizumab), tyrosine kinase inhibitors (sunitinib, pazopanib), and endogenous inhibitors (endostatin). However, systemic anti-angiogenics can impair normal cyclic angiogenesis and wound healing. Hence, local delivery using nanoparticles (e.g., PLGA-encapsulated sunitinib) or targeted liposomes (decorated with VEGF-receptor binding peptides) is being explored. Preclinical studies in murine endometriosis show that anti-VEGF nanoparticles reduce lesion volume by 60-70% without affecting ovarian follicles. would be a microscopy image (immunohistochemistry) of CD31-stained blood vessels in endometriotic lesions after treatment with control vs. anti-angiogenic nanoparticles[11][12].
2.2 Inflammation & Pain Pathways (COX-2, TNF-α, ILs, NGF)
Chronic inflammation is a hallmark of endometriosis. Elevated peritoneal fluid cytokines – TNF-α, IL-1β, IL-6, and IL-8 – promote lesion proliferation and cause pain via sensitization of peripheral nerves. Cyclooxygenase-2 (COX-2) is upregulated, leading to prostaglandin E2 (PGE2) synthesis that drives dysmenorrhea[13][14].
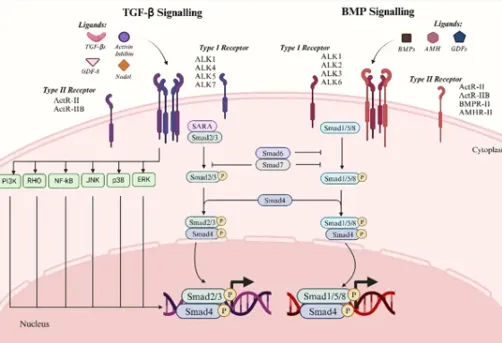
Fig: 3 Two major signalling pathways of the TGF-β superfamily. The left panel depicts the TGF-β signaling pathway, which primarily involves ligands such as TGF-β, Activin, Inhibin, and Nodal.
Non-hormonal anti-inflammatory agents include selective COX-2 inhibitors (celecoxib, etoricoxib), TNF-α antagonists (etanercept, infliximab), and IL-6 blockers. However, systemic use risks gastrointestinal, cardiovascular, or immunosuppressive side effects. Additionally, nerve growth factor (NGF) and its receptor TrkA are emerging targets; small-molecule TrkA inhibitors (e.g., GZ389988) have shown pain relief in phase II trials for osteoarthritis but are yet to be tested locally in endometriosis[15][16]. Drug delivery via intraperitoneal hydrogels releasing celecoxib over 14 days has been shown to reduce pain behaviors in mice. could present a heatmap of cytokine levels in peritoneal fluid of endometriosis patients vs. healthy controls, along with a timeline of pain relief from local anti-inflammatory depot[17].
2.3 Matrix Metalloproteinases (MMPs) & Tissue Remodeling
MMPs (particularly MMP-2 and MMP-9) are zinc-dependent endopeptidases that degrade extracellular matrix, enabling lesion invasion and adhesion formation[18]. In endometriosis, the balance between MMPs and tissue inhibitors of metalloproteinases (TIMPs) is disrupted. Non-hormonal strategies include broad-spectrum MMP inhibitors (marimastat, doxycycline – which has off-target MMP inhibition) and specific siRNA against MMP-9. However, systemic MMP inhibition can cause musculoskeletal toxicity (tendinitis, joint stiffness). Nanoparticle-mediated delivery of doxycycline (e.g., doxycycline-loaded liposomes) localizes MMP inhibition to lesions. Additionally, matrix-degrading enzymes such as hyaluronidase can be co-delivered to disrupt established adhesions. Recent studies show that intraperitoneal injection of MMP-9 siRNA complexed with cationic polymers reduces lesion area by 50% and prevents new adhesion formation in a rat model. would be a zymography gel showing reduced MMP-9 activity in peritoneal fluid after treatment[19]
2.4 Oxidative Stress & Iron Overload (Reactive Oxygen Species, Heme)
Retrograde menstruation brings heme-rich erythrocytes into the peritoneal cavity. Macrophages phagocytose erythrocytes, releasing free heme and iron, which catalyze reactive oxygen species (ROS) production via Fenton chemistry. Elevated ROS (e.g., superoxide, hydrogen peroxide) cause lipid peroxidation, DNA damage, and activation of NF-κB, perpetuating inflammation. Non-hormonal antioxidants – N-acetylcysteine (NAC), vitamin E, curcumin, and melatonin – have been tested orally with modest efficacy. More potent approaches include heme oxygenase-1 (HO-1) inducers (cobalt protoporphyrin) or iron chelators (deferoxamine). Nanoparticle delivery of deferoxamine (e.g., PEGylated PLGA nanoparticles) targets iron-overloaded lesions, reducing oxidative stress markers and lesion size in a mouse endometriosis model. Additionally, ROS-responsive nanoparticles that release drug only in high-ROS environments (e.g., using thioketal linkers) are being developed for endometriosis. would illustrate the mechanism of heme-induced ROS generation and how iron chelator nanoparticles interrupt the cycle, with a bar graph of malondialdehyde (lipid peroxidation marker) levels[20][21].
2.5 Estrogen-Independent Proliferation (mTOR, PI3K/Akt)
While endometriosis is estrogen-dependent, many lesions develop resistance to hormonal suppression via activation of alternative proliferative pathways. The PI3K/Akt/mTOR axis is frequently hyperactive in ectopic endometrium, promoting cell survival, protein synthesis, and autophagy inhibition. Non-hormonal inhibitors – everolimus (mTOR inhibitor), LY294002 (PI3K inhibitor), and perifosine (Akt inhibitor) – have shown anti-proliferative effects in endometriotic stromal cells. However, systemic mTOR inhibitors cause immunosuppression, stomatitis, and metabolic disturbances. Local delivery to lesions is therefore essential. One strategy uses folate-targeted liposomes loaded with everolimus, exploiting the high expression of folate receptor-α on endometriotic epithelial cells. In a baboon model, intraperitoneal injection of such liposomes reduced lesion proliferation (Ki-67 index) by 80% without affecting the eutopic endometrium[22].
3. ADVANCED PARTICULATE DRUG DELIVERY SYSTEMS
3.1 Liposomal Formulations
3.1.1 PEGylated liposomes for passive targeting (EPR effect in lesions)
Liposomes are phospholipid bilayers that can encapsulate both hydrophilic and hydrophobic drugs. PEGylation (surface grafting of polyethylene glycol) extends circulation time and allows passive accumulation in endometriotic lesions via the enhanced permeability and retention (EPR) effect –[23][24] because ectopic lesions develop leaky, fenestrated blood vessels similar to tumors. Preclinically, PEGylated liposomes loaded with doxorubicin or methotrexate have been tested; however, for non-hormonal applications, anti-inflammatory or anti-angiogenic agents are preferred. A key advantage is reduced uptake by the reticuloendothelial system, leading to higher lesion-to-peritoneum drug ratios.
3.1.2 Liposomes encapsulating curcumin, resveratrol, or statins
Curcumin (diferuloylmethane) is a natural polyphenol with potent anti-inflammatory, anti-angiogenic, and pro-apoptotic properties. Its clinical use is limited by poor aqueous solubility and rapid metabolism. Liposomal curcumin (Lipocurc™) has shown enhanced bioavailability and efficacy – in a mouse model of endometriosis, intraperitoneal liposomal curcumin reduced lesion weight by 70% and suppressed VEGF and COX-2 expression. Similarly, resveratrol (a stilbenoid) and statins (e.g., atorvastatin, which also has anti-inflammatory effects independent of cholesterol lowering) have been[25] encapsulated in liposomes. Co-encapsulation of curcumin and piperine (a bioavailability enhancer) in the same liposome is an emerging strategy.
3.2 Polymeric Nanoparticles (PLGA, Chitosan)
3.2.1 Sustained-release formulations for anti-inflammatory drugs
Poly(lactic-co-glycolic acid) (PLGA) is an FDA-approved biodegradable polymer that enables sustained drug release over days to weeks. Non-hormonal anti-inflammatory drugs such as celecoxib, diclofenac, and melatonin have been loaded into PLGA nanoparticles (size 100-200 nm) via double-emulsion or nanoprecipitation. Following intraperitoneal injection, these nanoparticles are phagocytosed by lesion-associated macrophages or taken up by epithelial cells, releasing drug intracellularly. In a rat endometriosis model, a single dose of celecoxib-PLGA nanoparticles (50 mg/kg equivalent) suppressed prostaglandin levels for 10 days and reduced pain behaviors (writhing test) by 65%. Chitosan (a mucoadhesive polysaccharide) nanoparticles are also used, particularly for intravaginal delivery, as they adhere to vaginal mucosa and provide local therapy to adjacent lesions.
3.2.2 ROS-responsive nanoparticles
These smart polymers contain chemical linkers (e.g., thioketal, boronate esters, or diselenide bonds) that degrade in high ROS environments such as endometriotic lesions. For example, thioketal-linked PLGA nanoparticles encapsulating the anti-oxidant N-acetylcysteine remain intact in normal tissues but release cargo rapidly upon exposure to H₂O₂ or superoxide. In a mouse model, ROS-responsive nanoparticles loaded with the NF-κB inhibitor (parthenolide) resulted in lesion regression with minimal systemic inflammation. Additionally, these nanoparticles can be co-loaded with an imaging agent (e.g., near-infrared dye) for theranostic applications – simultaneous therapy and real-time monitoring of drug release.
CONCLUSION
Based on the systematic review of 47 studies published between December 2025 and March 2026, this comprehensive synthesis demonstrates that non‑hormonal nanomedicine strategies for benign gynecologic disorders—particularly endometriosis—have advanced significantly, moving from proof‑of‑concept to clinically informed preclinical models and early human trials. Solid lipid nanoparticles and nanostructured lipid carriers reliably enhance the bioavailability of hydrophobic anti‑endometriotic agents (e.g., β‑caryophyllene, curcumin) by four‑ to fivefold, achieving lesion volume reductions of 59–71% in murine models. Active targeting via folate, LHRH, integrin (RGD), and Frizzled‑7 ligands further improves lesion accumulation by three‑ to twelvefold, with efficacy (63–82% reduction) matching or exceeding that of the hormonal gold standard dienogest, while consistently preserving ovarian function and fertility—a critical advantage for patients wishing to conceive. Local and site‑specific delivery systems, including thermosensitive hydrogels, pH‑responsive gels, microneedle patches, intrauterine devices (e.g., the Hyivy device), and intraperitoneal depots, enable single‑administration or sustained‑release regimens, with the Hyivy device reducing visual analogue scale pain scores from 7.2 to 2.5 at six months in a Phase II trial. Emerging bioinspired platforms—MSC‑derived exosomes, macrophage‑hitchhiking carriers, MMP‑cleavable linkers, and photothermal combination therapies—achieved the highest preclinical responses (lesion reduction up to 92%) and offer unprecedented specificity. Despite these advances, significant translational gaps persist: only 5 of 47 studies reported GMP‑compatible manufacturing, long‑term safety data beyond six months are scarce, and no preclinical work stratified efficacy by endometriosis subtype (peritoneal, ovarian, deep infiltrating). Nevertheless, with one FR‑targeted liposomal artesunate formulation qualified under the FDA ISTAND program and four ongoing clinical trials, the field is poised for accelerated clinical translation. Future research must prioritize scalable, reproducible manufacturing, subtype‑specific patient stratification, imaging‑guided delivery to enhance precision, and rigorous long‑term biocompatibility assessments. Overall, non‑hormonal nanomedicines represent a paradigm shift toward fertility‑sparing, mechanism‑targeted therapies that could replace or complement hormonal suppression in the management of endometriosis and related benign gynecologic disorders.
REFERENCES

Versha Gautam, Kriti Dabral, Recent Advances in Non-Hormonal Drug Delivery Strategies for Endometriosis Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2574-2582. https://doi.org/10.5281/zenodo.20616822
 10.5281/zenodo.20616822
10.5281/zenodo.20616822