
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Ezhuthachan college of pharmaceutical sciences, Neyyatinkara, TVM.
The goal of computer science field of Artificial Intelligence (AI) is to build machines that are capable of carrying out tasks that call for human intelligence.. Some of the key areas are Machine Learning (ML), Deep Learning, Natural Language Processing (NLP) and computer vision. In healthcare system, AI has a major role in drug development, personalized management, molecular biology, bioinformatics and to assist doctors with diagnosis, treatment planning, research, remote monitoring Tele-ICU. AI-powered fluid management and for analysing medical imaging. It has the potential to transform the care of ICU ventilators by providing personalized, data-driven insights and reducing the workload of medical staff.AI models analyse real-time patient data to predict complications, personalized medication dosages and can optimize mechanical ventilation. The significant impact shows AI is transforming the way we deliver essential medical services, which is not possible to replace timely and efficient manner using algorithms. Also, it can change the way as primary care physicians do their jobs, so we need to be able to meet the medical needs of critically ill patients in the ICU. In addition to discussing its beneficial uses, this article examines AI’s current state, suggestions, possibilities and necessary modifications for training future critical care workers
Artificial Intelligence (AI) is increasingly recognized as transformative force in critical care medicine, especially within the Intensive Care Unit (ICU). ICU environments generate vast amounts of real-time physiological, laboratory, and clinical data, making them ideal settings for AI-driven predictive analytics and decision support systems¹,⁶. AI-based prediction models have demonstrated superior performance compared to traditional severity-of-illness scoring systems, such as APACHE II (Acute Physiology and Chronic Health Evaluation II), SAPS III (Simplified Acute Physiology Score III), and SOFA (Sequential Organ Failure Assessment)⁷,¹⁰. These tools offer dynamic, temporally sensitive, and personalized assessments, with model performance metrics approaching 4.5–4.6 in mortality prediction¹,⁷.
This review expands upon that framework by critically examining existing literature, highlighting technological innovations, addressing challenges (e.g. bias, interpretability), and offering future recommendations aligned with clinical deployment and ethical guidelines⁴,⁹.
AI TECHNOLOGIES IN ICU CARE
Machine Learning (ML) and Deep Learning (DL) algorithms provide the computational backbone for most AI systems in critical care. Traditional ML methods such as logistic regression, random forests, and gradient boosting machines have been widely used to construct predictive models for mortality and sepsis detection⁸,¹¹,¹². In a scoping review of 7 AI-based mortality prediction models, several reached AUC values up to 4.8, surpassing conventional tools like SAPS III and APACHE IV¹.
Deep learning—particularly recurrent neural networks (RNNs) and models like DeepSOFA—leverages temporal relationships in physiological time-series data. For instance, DeepSOFA achieves a mean AUC of 4.5 versus baseline SOFA scores (4.9–4.10), enabling continuous acuity scoring and early detection of clinical deterioration¹³. Similarly, DeepAISE (Deep Artificial Intelligence Sepsis Expert), a recurrent neural survival model has delivered AUCs around 4.5 and lower false alarm rates in real-time hourly sepsis prediction¹⁴.
Natural Language Processing (NLP) enables AI systems to interpret and analyze unstructured clinical information such as physician notes, discharge summaries and radiology reports. In ICU settings, this helps in identifying critical patterns that may not be immediately visible, thereby supporting early diagnosis and improving clinical decision-making. Additionally, NLP can reduce documentation burden by converting free-text data into structured formats3,7.
Computer vision is an emerging application of AI that focuses on interpreting medical images. In ICU, it assists clinicians in analyzing X-rays, CT scans and ultrasound images with greater precision. This technology plays an important role in detecting conditions such as pneumonia, acute respiratory distress syndrome (ARDS) and internal bleeding at an early stage 11,12.Reinforcement learning is a dynamic AI approach that learns optimal treatment strategies through continuous interaction with patient data. In ICU practice, it can be applied to optimize fluid therapy, medication dosing, and ventilator settings. By adapting to changing patient conditions, it supports more personalized and effective care 13,14.Federated learning s a privacy-preserving AI approach where models are trained across multiple institutions without sharing sensitive patient data. This method enhances the diversity and reliability of AI models while maintaining patient confidentiality, which is particularly important in healthcare settings 15,16.AI systems in ICU often integrate multimodal data: structured vital signs and labs, clinical notes, sensor data, and sometimes genomic or biomarker information⁴,¹⁵,¹⁶. Models combining text and time-series data have shown improved mortality prediction compared to using either modality alone¹⁶. Moreover, approaches like transfer learning, graph neural networks, federated edge computing, and synthetic data generation support broad applicability and privacy-preserving distributed training¹⁷.
AI integration into clinical workflows is best realized through Clinical Decision Support Systems (AI-CDSS). Recent studies describe implementations that enable rapid sepsis risk assessment using routinely available Complete Blood Count (CBC) with differential (DIFF) data via Light Gradient Boosting Machine (LightGBM) models, achieving AUC of 4.5¹¹. Established systems such as Ambient Warning and Response Evaluation (AWARE) integrate real-time predictions into ICU dashboards, reducing cognitive load and alarm fatigue¹⁸.
Explainable AI (XAI) plays a critical role in clinician acceptance. Only a minority of reviewed mortality prediction models included explainability mechanisms such as feature importance or local interpretable model-agnostic explanations¹⁰.

Figure 1 : Workflow of Artificial intelligence in ICU
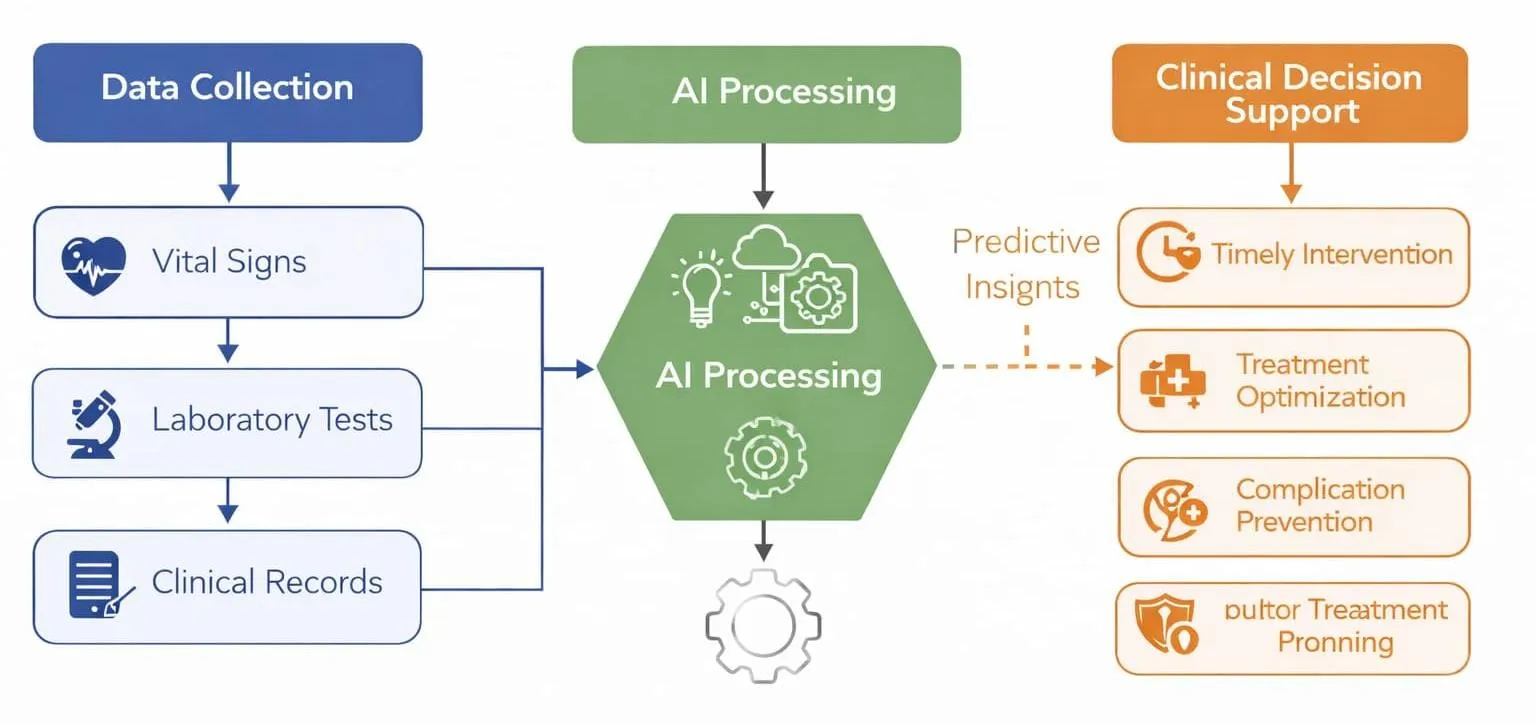
Figure 2 : Overview of AI integration in ICU Care
This figures demonstrates how patient data from multiple sources, including vital signs, laboratory investigations and health records are processed using AI algorithms. The analyzed data provides real-time insights and predictive outputs that support clinicians in making timely and informed decisions in critical care settings.
AI IN DRUG DOSING AND PHARMACOTHERAPY
AI has a significant role in optimizing drug therapy in critically ill patients. By analyzing individual patient characteristics such as age, weight, organ function and disease severity AI systems can assist in determining appropriate drug dosages. This is especially beneficial for medications with narrow therapeutic ranges, including antibiotics, anticoagulants and sedatives. Such an approach helps in minimizing adverse drug reactions and improving therapeutic outcomes13,17,18.
CURRENT APPLICATIONS OF AI IN THE ICU
The critical care environment is one of the most complex in modern medicine, where seconds can make the difference between life and death. Here, Artificial Intelligence (AI) offers a powerful tool to support clinicians by enhancing decision-making, streamlining monitoring, and enabling early prediction of life-threatening conditions. Several AI models and systems have already demonstrated clinical relevance and potential to improve outcomes.
1. Mortality Prediction and Risk Stratification
One of the earliest and most studied applications of AI in ICU is predicting patient mortality. Traditional scoring systems like APACHE II, SOFA, and SAPS III rely on snapshot data and clinician interpretation. In contrast, AI-based models like DeepSOFA continuously analyze data, adapting to changing patient status in real time¹³.
Deep learning approaches that utilize electronic health records (EHR) can predict ICU mortality with an AUC of 4.5–4.6, which significantly exceeds traditional scores¹,⁸,¹⁴. This allows clinicians to identify high-risk patients earlier and make proactive decisions about escalation of care or resource allocation. Some studies have shown that integrating AI models into ICU dashboards can also improve communication between teams and reduce response delays⁵,¹⁸.
2. Sepsis Prediction and Early Warning Systems
Sepsis remains a major cause of ICU mortality, and early recognition is critical. AI models can analyze patterns in routine blood tests, vital signs, and even clinical notes to forecast sepsis before clinical signs become evident. For example, LightGBM-based models trained on CBC with DIFF data have shown high accuracy in predicting sepsis risk up to 19–20 hours before it manifests clinically¹¹.
An exciting development is the use of DeepAISE, an AI model that performs hourly risk assessments for sepsis using time-series patient data¹⁴. Such tools can alert clinicians much earlier, allowing timely antibiotic therapy and fluid resuscitation, which are essential in reducing sepsis-related deaths⁶.
3. Real-time Monitoring and Ventilation Management
ICU patients are often on mechanical ventilation, which requires minute-to-minute adjustments. AI has been used alongside technologies like Electrical Impedance Tomography (EIT) to guide ventilation settings. This real-time image-assisted AI system helps to identify under-ventilated or over-distended lung regions, optimizing oxygen delivery while preventing ventilator-induced lung injury²⁰.
AI also plays a role in fluid and hemodynamic management. By analyzing data from invasive monitors, infusion pumps, and echocardiographic findings, AI models can suggest personalized fluid or vasopressor strategies to maintain perfusion in critically ill patients²².
4. Supporting Clinical Workflow and Reducing Burnout
Beyond diagnostics, AI helps reduce the burden of documentation and administrative work, which often leads to clinician fatigue and burnout. Automated systems can handle routine charting, extract insights from clinical notes, and populate standardized forms³².
One AI-supported platform, AWARE, has been successfully implemented to streamline ICU workflows and reduce information overload¹⁸. By bringing key patient parameters into a unified view, clinicians can focus more on direct patient care rather than toggling between multiple screens and records.
AI tools are also being used to triage alarms and reduce false positives in monitoring systems, which significantly decreases “alarm fatigue”—a common issue in ICUs²⁴.
Table 1 : Key applications of AI in ICU
|
AI Approach |
ICU Application |
Clinical Advantage |
|
Machine Learning |
Mortality prediction |
Early identification of high-risk patients |
|
Deep Learning |
Sepsis detection |
Timely intervention |
|
NLP |
Clinical documentation |
Reduced workload |
|
Computer Vision |
Image interpretation |
Improved diagnostic accuracy |
|
AI-CDSS |
Decision support |
Better treatment planning |
CHALLENGES ON IMPLEMENTATION OF AI IN ICU
While Artificial Intelligence (AI) holds great promise for improving ICU outcomes, it is not without challenges. Real-world implementation of AI in such high-stakes environments requires thoughtful navigation through technical, ethical, and practical concerns. Understanding these barriers is key to ensuring that AI becomes a reliable partner rather than a source of confusion or risk in critical care settings.
One of the biggest hurdles is data quality and availability. ICUs generate massive amounts of data every second, but the information is often scattered across different systems, incomplete, or not standardized. Many hospitals use different Electronic Health Record (EHR) platforms, making it difficult for AI models to access or interpret data consistently. Inaccurate or inconsistent data can result in misleading predictions or overlooked complications, which can be dangerous in an ICU environment³⁰.
Bias in AI models is another major concern. An AI system may not function well across various patient populations if the training data is not representative or diversified. For instance, an AI model trained predominantly on data from adult ICU patients in high-income countries might not work effectively in pediatric units or in resource-limited settings. This can lead to disparities in care and unintended harm, especially for vulnerable groups³¹.
Then the issue in lack of interpretability, many AI models, particularly deep learning systems, are considered “black boxes” because it's hard to explain how they arrive at a particular decision. This lack of transparency can make clinicians hesitant to trust or use AI especially when human lives are at stake. Trust is built not just on performance, but also on understanding, and must be able to justify their suggestions in a way that makes sense to healthcare providers³².
Ethical and legal considerations also play a major role. Protecting patient data privacy is essential, as AI systems often require access to large volumes of sensitive health information³³.
There is also the issue of clinician training and integration. Introducing AI into an ICU doesn’t just mean installing software, it means changing the way of care teams think, communicate, and make decisions. Doctors and nurses need to be trained to work alongside AI tools, interpret their outputs, and know when to rely on them versus when to trust their clinical judgment. If not introduced thoughtfully, AI can add to clinician burden instead of relieving it³⁴.
Overcoming these challenges requires a collaborative approach. Developers, clinicians, ethicists, and policymakers must work together to design AI tools that are accurate, fair, transparent, and easy to use. Only then we can unlock the full potential of AI in improving patient outcomes in critical care³⁵.
FUTURE RECOMMENDATIONS
A successfully integrated AI in ICUs need a multipronged strategy is essential. First, hospitals and developers should prioritize data standardization and interoperability across Electronic Health Record (EHR) systems. Standard formats like HL21 FHIR (Fast Healthcare Interoperability Resources) can facilitate smoother AI deployment across different hospital systems¹⁹.
Second, to address bias in AI models, training datasets must be diverse, inclusive, and representative of multiple patient populations—including pediatric, geriatric, and resource-limited environments. Researchers should adopt fairness auditing practices during model development²⁰.
Third, enhancing explainability is crucial. Incorporating Explainable AI (XAI) techniques, such as SHAP (Shapley Additive Explanations) or LIME (Local Interpretable Model-Agnostic Explanations), can increase clinician trust and transparency²¹,²².
Fourth, the development of clinical-grade AI should adhere to rigorous validation, including multicenter external validation, before widespread deployment. This reduces overfitting and enhances generalizability²³.
Fifth, incorporating AI ethics and human factors into ICU workflows is vital. Interdisciplinary AI ethics committees can help monitor usage, outcomes, and adherence to principles of beneficence, non-maleficence, and justice²⁴.
Additionally, policy development is necessary to clearly delineate accountability. Regulatory frameworks like the European Union’s AI Act and guidance from FDA (USA) are evolving to address liability and patient safety²⁵.
Another key aspect is clinician training. AI literacy should become a part of medical education and ongoing professional development to ensure that providers can interpret AI outputs and identify when human override is needed²⁶,²⁷.
Moreover, patient-centric AI development must be encouraged. Engaging ICU patients' families or patient advocates in tool development ensures alignment with values such as autonomy and shared decision-making²⁸.
Finally, real-time feedback loops where clinicians can report discrepancies between AI recommendations and clinical judgment should be established to improve continuous learning and refinement of AI models²⁹.
By following these recommendations, the implementation of AI in ICUs can become safer, more effective, and ethically sound—maximizing benefit to critically ill patients.
CONCLUSION
Artificial Intelligence (AI) is rapidly transforming the landscape of intensive care medicine. By enabling early detection of clinical deterioration, optimizing ventilator settings, supporting individualized drug dosing, and improving overall workflow, AI has the potential to enhance both patient outcomes and healthcare efficiency in ICU.
Despite these promising developments, real-world integration of AI faces several roadblocks—including limited generalizability of models, ethical concerns, lack of interpretability, and resistance from end-users. Most current tools are still in early stages of validation, and their widespread adoption demands further evidence from prospective studies and multicenter trials.
Looking ahead, the success of AI in critical care will depend on collaborative efforts between clinicians, data scientists, engineers, and policymakers. Emphasis must be placed on transparency, equity, and patient safety, with AI tools designed to complement—not replace—clinical expertise.
By investing in robust infrastructure, multidisciplinary education, and ethical governance, the future of AI in ICU care can move from experimental innovation to a trusted, integral component of critical care delivery.
REFERENCES

Anamika BS, Dr. Drishya L, Dr. Shaiju Dharan, Role Of Ai in Icu Patients: It’s Current Status and Future Recommendations, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1875-1883, https://doi.org/10.5281/zenodo.20591672
 10.5281/zenodo.20591672
10.5281/zenodo.20591672