
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,4 Shriram Shikshan Sanstha’s College of Pharmacy, Paniv, Maharashtra, India 413113
5,6 Chetana College of Pharmacy, Sardewadi, Indapur, Pune, Maharashtra, India 413106.
Drug-induced organ toxicity remains a major concern in clinical therapy because effective medicines may injure non-target tissues during metabolism, distribution or elimination. The liver, kidney, heart, nervous system, lung and gastrointestinal tract are frequently affected because these organs possess high metabolic activity, rich vascular exposure or specialized transport systems. A central mechanism connecting many toxic responses is oxidative stress, which arises when the formation of reactive oxygen species and reactive nitrogen species exceeds endogenous antioxidant capacity. Reactive metabolites, cytochrome P450-dependent bioactivation, mitochondrial electron leakage, glutathione depletion, lipid peroxidation, inflammatory cytokine release and apoptotic signalling combine to produce cellular and organ-level dysfunction. Natural antioxidants obtained from medicinal plants, fruits, vegetables, spices and marine sources have attracted attention as adjunctive protective agents. Curcumin, quercetin, resveratrol, silymarin, epigallocatechin gallate, lycopene, astaxanthin and antioxidant vitamins have shown protective effects in multiple experimental models through radical scavenging, metal chelation, up-regulation of endogenous antioxidant enzymes, activation of Nrf2-mediated cytoprotective pathways, suppression of NF-kB-related inflammation and stabilization of mitochondrial function. This review critically summarizes the mechanisms of drug-induced organ injury, classifies natural antioxidants according to source and mechanism, and organizes evidence by organ system. It also highlights limitations such as poor bioavailability, dose variability, lack of standardization, limited clinical trials and possible drug-herb interactions. Properly standardized antioxidant interventions may become valuable supportive strategies, but clinical translation requires rigorous pharmacokinetic, safety and efficacy evaluation. [1-4]
Modern pharmacotherapy has improved survival and quality of life in infectious diseases, cancer, cardiovascular disorders, metabolic diseases and inflammatory conditions. Nevertheless, many therapeutic agents cause adverse organ reactions, particularly when exposure is prolonged, dose is high, metabolism is altered or the patient has pre-existing disease. Drug-induced liver injury, nephrotoxicity, cardiotoxicity, neurotoxicity and pulmonary toxicity remain important reasons for treatment interruption and clinical monitoring. The problem is especially relevant in chronic therapy, polypharmacy and fragile patients, where the therapeutic window may be narrow and tissue reserve is limited. [1-6]
Drug-induced organ damage does not arise through a single pathway. Direct chemical injury, immune-mediated reactions, mitochondrial dysfunction, oxidative stress, altered calcium balance, endoplasmic reticulum stress, transporter inhibition and microvascular disturbance may contribute individually or together. The liver is vulnerable because it metabolizes xenobiotics through phase I and phase II pathways, the kidney because it concentrates drugs during filtration and secretion, and the heart because cardiomyocytes possess high mitochondrial density and limited regenerative capacity. Similarly, neurons and pulmonary cells are sensitive to redox imbalance and inflammatory injury because of high oxygen utilization and specialized membrane composition. [1-6]
Oxidative stress provides a mechanistic link across these organ toxicities. Under normal conditions, cells continuously generate reactive oxygen species such as superoxide anion, hydrogen peroxide and hydroxyl radicals during mitochondrial respiration and enzymatic reactions. These species are controlled by superoxide dismutase, catalase, glutathione peroxidase, thioredoxin systems, glutathione and dietary antioxidants. Toxic drug exposure may overwhelm these defences, producing lipid peroxidation, protein carbonylation, DNA strand breaks, mitochondrial permeability transition and cell death. This concept is central to redox biology and toxicology because the same reactive species may participate in signalling at physiological levels but become destructive when generated excessively or in the wrong cellular compartment. [1-6]
Natural antioxidants are biologically active compounds capable of attenuating oxidative and inflammatory damage. They include polyphenols, flavonoids, carotenoids, antioxidant vitamins, sulfur compounds, terpenoids and standardized plant extracts. Some agents act primarily as radical scavengers, whereas others enhance endogenous defences by inducing nuclear factor erythroid 2-related factor 2 (Nrf2), suppressing nuclear factor-kappa B (NF-kB), preserving mitochondrial function or improving glutathione metabolism. Their multi-target pharmacology makes them attractive for organ protection, but their use requires careful interpretation because preclinical efficacy does not automatically ensure clinical benefit. [1-6]
The present modified review paper reorganizes the original manuscript into a structured scientific format suitable for academic submission. The revised version provides a clear review methodology, mechanistic explanation, organ-wise discussion, standardized tables, original black-and-white flow diagrams and an expanded reference list. Emphasis is placed on meaningful scientific language, continuity of arguments and balanced evaluation of both promise and limitations. [1-6]
2. Review Methodology and Scope
This article was prepared as a narrative review with a structured search approach. Literature was identified from peer-reviewed journals, books and reputable biomedical databases. Search terms included drug-induced organ toxicity, oxidative stress, natural antioxidants, hepatotoxicity, nephrotoxicity, cardiotoxicity, neurotoxicity, phytochemicals, curcumin, quercetin, resveratrol, silymarin and epigallocatechin gallate. Priority was given to review articles, mechanistic toxicology papers, experimental organ-protection studies and clinical or translational discussions. [7-13]
Studies were considered relevant when they described biochemical mechanisms of drug-induced organ injury, reported antioxidant biomarkers, evaluated plant-derived antioxidant compounds or discussed formulation and clinical barriers. Articles unrelated to organ toxicity, papers without mechanistic interpretation and duplicate information were not emphasized. Because the topic includes broad preclinical and clinical evidence, findings are synthesized qualitatively rather than statistically pooled. [7-13]
The review scope includes organ injury caused by commonly used or clinically important drugs such as paracetamol, antitubercular drugs, methotrexate, valproic acid, cisplatin, gentamicin, non-steroidal anti-inflammatory drugs, doxorubicin, trastuzumab, cyclophosphamide, vincristine and selected neurotoxic agents. The focus is on oxidative stress-related mechanisms and the protective role of naturally derived antioxidants. [7-13]
Table 1. Structured review framework used for the modified paper.
|
Review component |
Description |
Purpose in paper |
|
Population/problem |
Drug-exposed cells, animals or patients with risk of organ injury |
Defines the clinical and toxicological context |
|
Mechanistic focus |
ROS/RNS formation, mitochondrial injury, inflammation and apoptosis |
Links toxicity across organs through common pathways |
|
Intervention concept |
Natural antioxidants and phytochemical-rich extracts |
Evaluates protective and supportive potential |
|
Outcome markers |
ALT/AST, creatinine, troponin, MDA, GSH, SOD, CAT, GPx and histology |
Provides measurable toxicity and protection endpoints |
|
Evidence synthesis |
Narrative comparison of mechanistic, preclinical and translational literature |
Builds a scientifically organized review rather than a simple list |
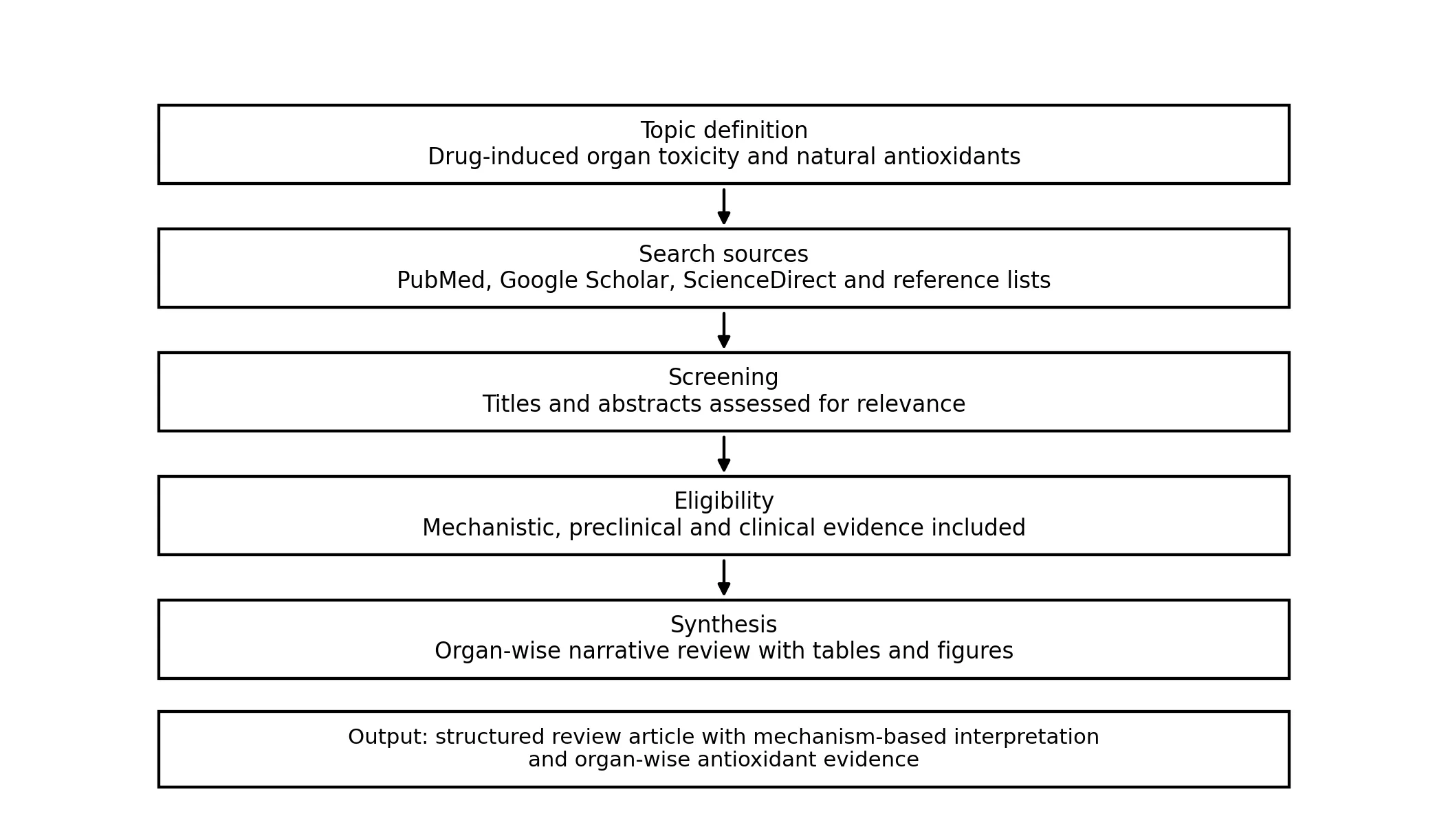
Figure 1. Literature-selection and review-development flow used to restructure the manuscript.
3. Biological Basis of Drug-Induced Organ Toxicity
Drug toxicity begins when the chemical structure of a medicine, its metabolite or its interaction with cellular systems disturbs normal homeostasis. Some drugs are intrinsically reactive, while others become toxic only after metabolic activation. Cytochrome P450 enzymes can convert relatively stable molecules into electrophilic metabolites capable of binding proteins, nucleic acids or lipids. When detoxification by glutathione conjugation, sulfation, glucuronidation or renal excretion is insufficient, reactive intermediates accumulate and initiate cellular stress. [6-10,14]
The mitochondrion is a key target and amplifier of toxicity. Mitochondrial injury reduces ATP production, increases electron leakage from the respiratory chain, promotes formation of superoxide and triggers opening of the mitochondrial permeability transition pore. Loss of mitochondrial membrane potential and release of cytochrome c can lead to caspase activation and apoptosis. In severe injury, ATP depletion favors necrosis, which releases danger-associated molecular patterns that intensify inflammation. [6-10,14]
Inflammation interacts closely with oxidative stress. Drug-induced injury may activate Kupffer cells, renal tubular inflammatory pathways, cardiac macrophages, microglia or pulmonary immune cells. Cytokines such as TNF-alpha, IL-1 beta and IL-6 increase oxidative enzyme activity and recruit leukocytes, thereby extending tissue damage beyond the initial chemical insult. The reciprocal relationship between oxidative stress and inflammation explains why antioxidants with anti-inflammatory properties may be more effective than compounds that only scavenge radicals. [6-10,14]
Apoptosis, necrosis, ferroptosis and autophagy imbalance represent cell-death or cell-survival responses in drug-induced organ toxicity. Lipid peroxidation can damage cellular membranes and may contribute to ferroptotic injury, especially when glutathione peroxidase activity is reduced. Autophagy may protect cells by removing damaged mitochondria, but excessive or defective autophagy can also impair tissue function. Thus, the protective action of natural antioxidants should be viewed as a network effect rather than a single chemical reaction. [6-10,14]
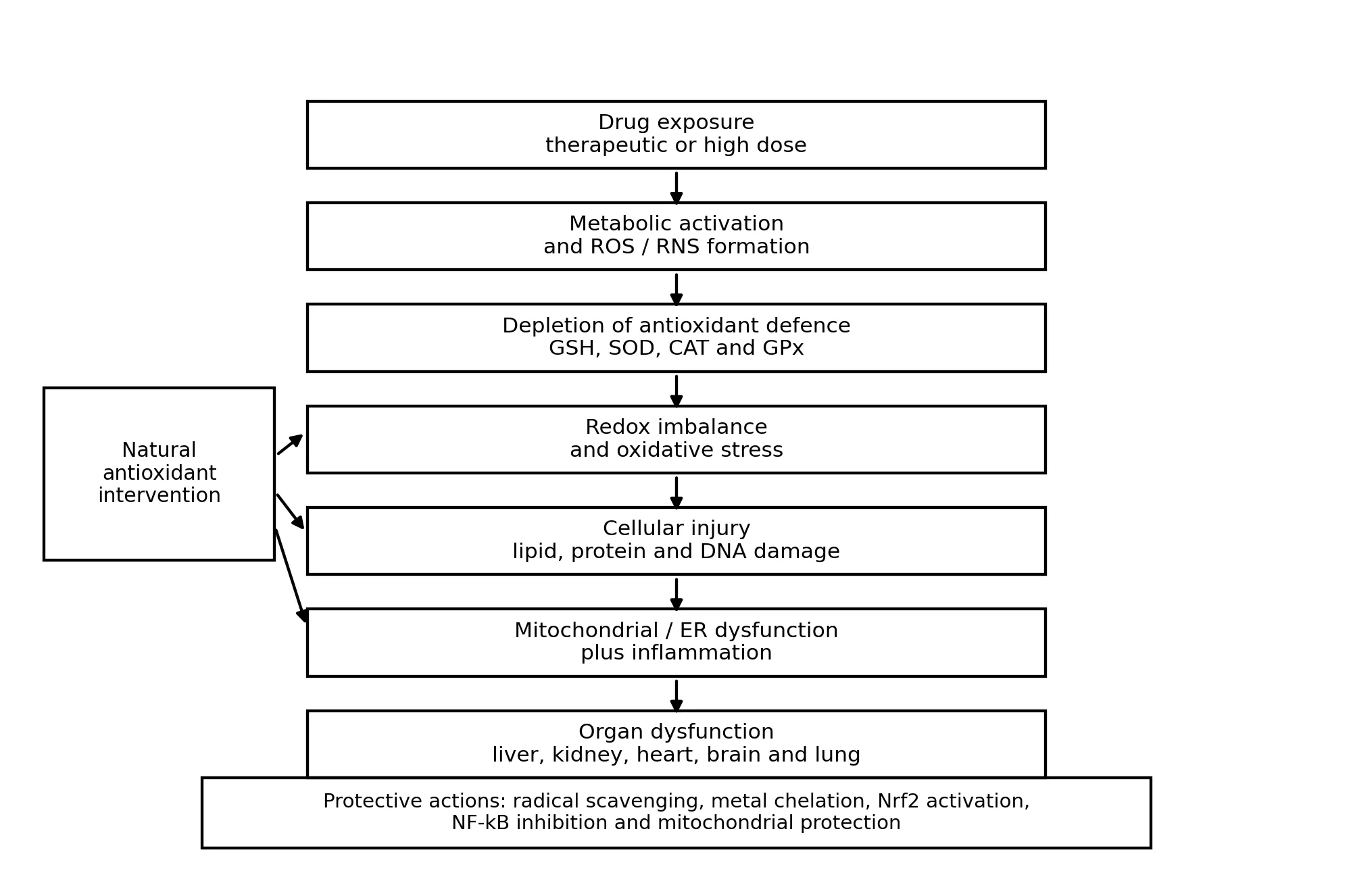
Figure 2. Mechanistic flow of drug-induced organ toxicity and major points of natural antioxidant intervention.
4. Organ-Specific Manifestations of Drug Toxicity
4.1 Hepatotoxicity
The liver is the principal organ for xenobiotic metabolism and is therefore highly exposed to reactive drug metabolites. Paracetamol overdose is the classical model of oxidative hepatotoxicity. Excess formation of N-acetyl-p-benzoquinone imine depletes glutathione and binds mitochondrial proteins, which leads to oxidant stress, mitochondrial dysfunction, necrosis and inflammatory amplification. Antitubercular drugs, methotrexate, valproic acid, halothane and some herbal products can also produce hepatocellular, cholestatic or mixed injury patterns. [7-10,16]
Hepatic injury is commonly monitored using serum alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, bilirubin and histopathological changes. At the mechanistic level, glutathione depletion, lipid peroxidation, altered mitochondrial respiration, bile-acid accumulation and immune-mediated reactions are important. Natural antioxidants such as silymarin, curcumin, quercetin and resveratrol have been studied for their ability to restore redox balance, preserve hepatocyte membranes and reduce inflammatory signalling. [7-10,16]
4.2 Nephrotoxicity
The kidney is susceptible to toxicity because it receives high blood flow, concentrates solutes in the tubular lumen and expresses transporters that actively accumulate drugs. Cisplatin, aminoglycosides, amphotericin B, cyclosporine, radiocontrast agents and non-steroidal anti-inflammatory drugs are common nephrotoxic agents. Tubular epithelial cells are particularly vulnerable due to high mitochondrial energy demand and exposure to concentrated chemicals. [11-13]
Cisplatin-induced nephrotoxicity is characterized by tubular injury, mitochondrial dysfunction, oxidative stress, inflammation and apoptosis. Biomarkers include serum creatinine, blood urea nitrogen, urinary kidney injury molecule-1, neutrophil gelatinase-associated lipocalin and histological evidence of tubular necrosis. Natural antioxidants may reduce renal injury by suppressing lipid peroxidation, maintaining glutathione, restoring SOD and catalase activity and inhibiting pro-inflammatory mediators. [11-13]
4.3 Cardiotoxicity
Drug-induced cardiotoxicity is clinically important because cardiac damage can be irreversible. Anthracyclines such as doxorubicin cause redox cycling, iron-mediated radical formation, mitochondrial injury, topoisomerase II beta-related DNA damage and cardiomyocyte apoptosis. Trastuzumab, cyclophosphamide and some tyrosine kinase inhibitors can also affect cardiac function through mitochondrial, inflammatory or signalling mechanisms. [14,15,23]
Cardiac protection requires preservation of mitochondrial respiration, contractile protein integrity, calcium homeostasis and endothelial function. Oxidative stress has a central role in doxorubicin cardiotoxicity, and several antioxidant compounds have been examined. Resveratrol has attracted attention because it can modulate oxidative stress, apoptosis, inflammation and mitochondrial signalling, although clinical application still requires stronger evidence regarding dose, timing and compatibility with anticancer efficacy. [14,15,23]
4.4 Neurotoxicity and Pulmonary Toxicity
The nervous system is vulnerable because neurons are highly dependent on mitochondrial ATP generation and contain lipid-rich membranes that are prone to peroxidation. Vincristine, cisplatin, methotrexate, isoniazid and some antiretroviral or chemotherapeutic agents may produce peripheral neuropathy, cognitive impairment or central nervous system toxicity. Mechanisms include axonal transport disruption, mitochondrial impairment, neuroinflammation, oxidative damage and altered neurotransmission. [24,28,29]
Pulmonary toxicity can occur with agents such as bleomycin, amiodarone, methotrexate and some anticancer drugs. Oxidative stress contributes to epithelial injury, inflammatory cell recruitment and fibrotic remodelling. Although natural antioxidants have shown promise in experimental pulmonary injury, clinical translation requires caution because excessive antioxidant supplementation may interfere with normal redox signalling and immune defence. [24,28,29]
Table 2. Common drug-induced organ toxicities, mechanisms and measurable indicators.
|
Organ/system |
Representative drugs |
Principal mechanisms |
Useful indicators |
|
Liver |
Paracetamol, isoniazid, rifampicin, methotrexate, valproic acid |
Reactive metabolites, GSH depletion, mitochondrial injury, cholestasis, inflammation |
ALT, AST, ALP, bilirubin, GSH, MDA, histology |
|
Kidney |
Cisplatin, gentamicin, amphotericin B, NSAIDs, cyclosporine |
Tubular accumulation, oxidative stress, vascular injury, apoptosis, inflammation |
Creatinine, urea, KIM-1, NGAL, renal MDA, SOD/CAT |
|
Heart |
Doxorubicin, trastuzumab, cyclophosphamide |
Redox cycling, mitochondrial damage, calcium imbalance, cardiomyocyte apoptosis |
Troponin, BNP, ECG, ejection fraction, cardiac MDA |
|
Brain/peripheral nerves |
Vincristine, cisplatin, methotrexate, isoniazid |
Mitochondrial injury, axonal damage, neuroinflammation, lipid peroxidation |
Behavioral tests, nerve conduction, oxidative markers |
|
Lung |
Bleomycin, amiodarone, methotrexate |
ROS generation, epithelial injury, cytokine activation, fibrosis |
Pulmonary function, collagen content, histology, inflammatory markers |
5. Oxidative Stress as a Common Pathogenic Pathway
Oxidative stress is best understood as a disturbance in redox signalling and control rather than simply the presence of oxidants. Physiological oxidants regulate cell proliferation, immune defence, vascular tone and adaptive signalling. Toxicity arises when oxidant formation is excessive, compartmentalized in vulnerable organelles or accompanied by depletion of reductive capacity. This distinction is important because total elimination of oxidants is neither possible nor desirable; the therapeutic objective is restoration of controlled redox balance. [1-3,34]
Major reactive species include superoxide anion, hydrogen peroxide, hydroxyl radical, nitric oxide, peroxynitrite and lipid peroxyl radicals. Superoxide may be converted to hydrogen peroxide by SOD; hydrogen peroxide is detoxified by catalase, glutathione peroxidase and peroxiredoxins; and hydroxyl radicals can attack almost any nearby biological molecule. Reactive nitrogen species formed from nitric oxide and superoxide further modify proteins through nitration and nitrosylation. [1-3,34]
Biochemical evidence of oxidative damage includes increased malondialdehyde, 4-hydroxynonenal, protein carbonyls, 8-hydroxy-2'-deoxyguanosine and decreased glutathione. The most informative assessment uses a panel of markers because a single marker may not accurately reflect the redox status of a whole organ. Experimental models also use histopathology and functional biomarkers to determine whether biochemical improvement translates into tissue protection. [1-3,34]
Table 3. Oxidative stress markers and interpretation in organ toxicity studies.
|
Marker |
Meaning |
Relevance for toxicity evaluation |
|
MDA and 4-HNE |
Products of lipid peroxidation |
Indicate membrane injury and oxidative degradation of polyunsaturated lipids |
|
GSH/GSSG ratio |
Balance between reduced and oxidized glutathione |
Reflects intracellular reducing capacity and detoxification reserve |
|
SOD, CAT and GPx |
Endogenous antioxidant enzymes |
Reduced activity suggests impaired enzymatic defence; restoration supports protection |
|
Protein carbonyls |
Oxidatively modified proteins |
Associated with enzyme dysfunction and structural damage |
|
8-OHdG |
Oxidative DNA damage marker |
Useful for evaluating genomic stress in chronic or severe injury |
|
ALT/AST, creatinine, troponin |
Organ function or injury markers |
Confirm whether redox changes are accompanied by clinically relevant organ injury |
6. Natural Antioxidants: Classes and Protective Mechanisms
Natural antioxidants are structurally diverse molecules obtained from plants, marine organisms, microbes and dietary sources. Phenolic hydroxyl groups, conjugated double bonds, sulfur-containing moieties and redox-active structures contribute to antioxidant potential. However, the biological effect of a compound depends not only on chemical radical-scavenging capacity but also on absorption, distribution, metabolism, tissue accumulation and interaction with cellular signalling pathways. [16-27,30-33]
Polyphenols such as curcumin, resveratrol and epigallocatechin gallate may modulate Nrf2, NF-kB, MAPK, SIRT1 and apoptotic pathways. Flavonoids such as quercetin, rutin and catechins can donate electrons, chelate metal ions and stabilize membranes. Carotenoids such as lycopene and astaxanthin quench singlet oxygen and protect lipid-rich membranes. Vitamins C and E act in aqueous and lipid compartments respectively, while plant extracts such as silymarin contain mixtures of bioactive molecules with hepatoprotective potential. [16-27,30-33]
Because many natural products act on several pathways, the term antioxidant should not be restricted to direct radical scavenging. A compound may have low direct radical-scavenging concentration at the target tissue but still produce strong cytoprotection by increasing endogenous antioxidant enzymes, inhibiting inflammatory transcription factors or maintaining mitochondrial function. This broader concept is more relevant for pharmacology and toxicology. [16-27,30-33]
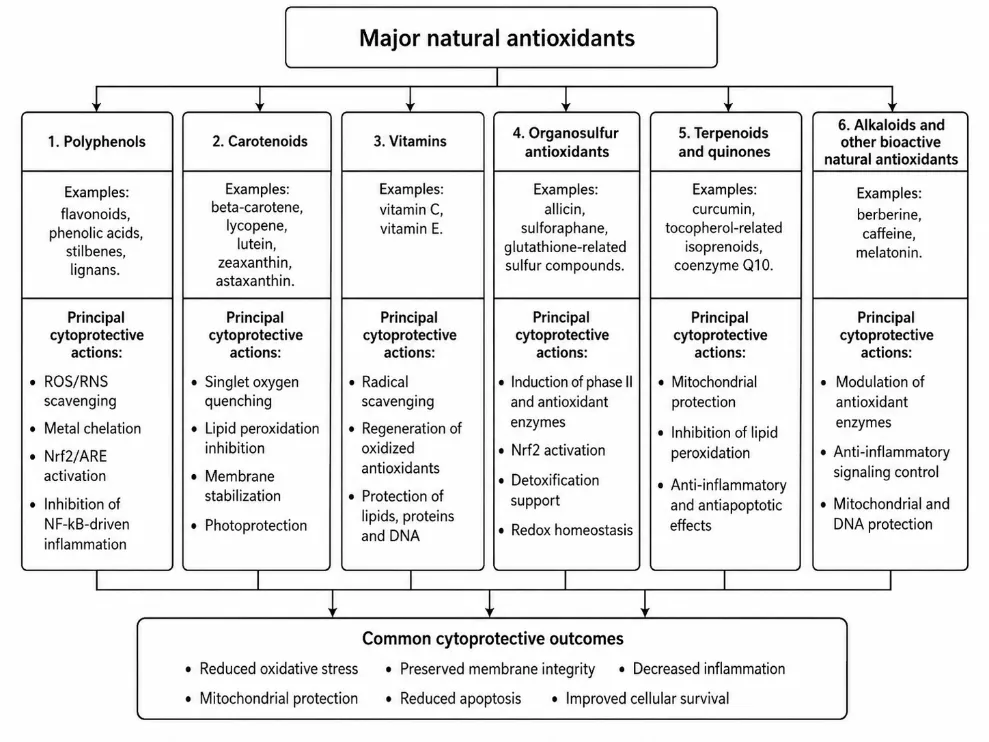
Figure 3. Classification of major natural antioxidants and their principal cytoprotective actions.
Table 4. Representative natural antioxidants and organ-protective relevance.
|
Antioxidant |
Major source |
Main organ relevance |
Mechanistic contribution |
|
Curcumin |
Curcuma longa rhizome |
Liver, brain, kidney |
Nrf2 activation, NF-kB suppression, GSH preservation and anti-apoptotic signalling |
|
Silymarin/silybin |
Silybum marianum seeds |
Liver |
Membrane stabilization, antioxidant enzyme support and hepatic regenerative signalling |
|
Quercetin |
Onion, apple, berries, tea |
Kidney, liver, cardiovascular system |
Metal chelation, radical scavenging and inflammatory pathway modulation |
|
Resveratrol |
Grapes, berries, peanuts |
Heart, liver, kidney |
SIRT1 and mitochondrial support, anti-inflammatory and anti-apoptotic activity |
|
EGCG |
Green tea |
Kidney, liver, nervous system |
ROS suppression, redox-sensitive signalling modulation and inflammatory control |
|
Lycopene |
Tomato and red fruits |
Heart, liver |
Singlet oxygen quenching and lipid membrane protection |
|
Astaxanthin |
Marine algae and seafood |
Heart, kidney, brain |
Lipid-phase antioxidant activity and mitochondrial protection |
|
Vitamin C and E |
Citrus fruits, nuts, seeds, oils |
Multiple organs |
Water- and lipid-phase antioxidant support; recycling of antioxidant networks |
7. Evidence for Organ Protection by Natural Antioxidants
7.1 Hepatoprotective effects
Curcumin is among the most extensively studied phytochemicals for liver protection. It can suppress lipid peroxidation, enhance antioxidant enzyme activity, modulate Nrf2 and reduce inflammatory signalling. In models of paracetamol, alcohol, carbon tetrachloride and other liver injuries, curcumin has been associated with lower transaminases, improved histology and reduced oxidative biomarkers. However, native curcumin has poor aqueous solubility and low oral bioavailability, which has encouraged development of nanoparticles, phospholipid complexes, piperine combinations and other delivery systems. [16-23,26,31,32]
Silymarin is a flavonolignan mixture obtained from milk thistle and is widely discussed as a hepatoprotective natural product. Its proposed benefits include hepatocyte membrane stabilization, inhibition of lipid peroxidation, stimulation of protein synthesis and anti-inflammatory action. Although it is not a substitute for evidence-based management of drug-induced liver injury, it remains a useful model compound for understanding how antioxidant, anti-inflammatory and regenerative mechanisms may combine in hepatic protection. [16-23,26,31,32]
Quercetin, resveratrol, lycopene and vitamin-based antioxidants have also shown liver-protective actions in experimental models. Their effectiveness depends on the injury model, dose, timing and route of administration. The most meaningful outcomes are those showing biochemical improvement together with functional and histological protection. Studies that report only antioxidant enzyme changes without organ outcome measures should be interpreted cautiously. [16-23,26,31,32]
7.2 Nephroprotective effects
Natural antioxidants have been widely evaluated in cisplatin and aminoglycoside nephrotoxicity. Cisplatin injury includes renal tubular uptake, DNA damage, oxidative stress, mitochondrial dysfunction, inflammatory cytokine production and apoptosis. Quercetin, curcumin, EGCG, resveratrol, gallic acid, astaxanthin and other phytochemicals may reduce renal lipid peroxidation, restore glutathione and antioxidant enzymes and attenuate histopathological tubular injury. [11-13,20,33]
The central translational challenge in nephroprotection is maintaining anticancer efficacy while reducing renal toxicity. Antioxidant co-administration should not interfere with the intended pro-oxidant or DNA-damaging action of anticancer drugs against tumor cells. Future studies should therefore include both toxicity and therapeutic-efficacy endpoints. Renal protective strategies should also consider hydration, dose adjustment and clinical monitoring alongside antioxidant support. [11-13,20,33]
7.3 Cardioprotective effects
Doxorubicin cardiotoxicity is a major model for studying antioxidant cardioprotection. Anthracycline redox cycling promotes ROS formation, damages mitochondrial membranes, disturbs calcium handling and activates apoptosis. Resveratrol has shown protective effects in experimental and systematic-review evidence by reducing oxidative stress, inflammation and cell-death signalling. Other natural antioxidants, including quercetin, curcumin, lycopene and coenzyme Q10, have also been studied in cardiac injury models. [14,15,23,26,31]
A key issue in cardioprotection is timing. Prophylactic antioxidant administration may differ from treatment after injury has begun. In cancer therapy, the antioxidant should ideally protect cardiomyocytes without reducing tumor response. Clinical translation therefore requires careful evaluation of pharmacodynamic interactions, cancer outcomes, cardiac biomarkers and long-term cardiac function. [14,15,23,26,31]
7.4 Neuroprotective and pulmonary protective effects
Neurotoxicity involves complex interactions among mitochondrial dysfunction, altered neurotransmission, inflammatory microglial activation and oxidative lipid injury. Natural antioxidants such as curcumin, resveratrol, quercetin, Ginkgo biloba extract, EGCG and astaxanthin have been evaluated for neuroprotective effects. Their actions include reduction of oxidative markers, suppression of neuroinflammation and support of mitochondrial function. Nevertheless, blood-brain barrier penetration and dose standardization remain important limitations. [24,27,28,30]
Pulmonary toxicity and gastrointestinal toxicity also involve redox and inflammatory mechanisms. Natural antioxidants may reduce epithelial injury, inflammatory cytokines and fibrosis-related signalling in experimental models. However, pulmonary redox biology is closely linked with host defence, and indiscriminate high-dose antioxidant supplementation may not be beneficial. The safest translational approach is evidence-guided adjunctive use with defined composition and monitoring. [24,27,28,30]
Table 5. Organ-wise summary of natural antioxidant evidence and research considerations.
|
Organ |
Promising antioxidants |
Main protective actions |
Important research consideration |
|
Liver |
Curcumin, silymarin, resveratrol, quercetin, lycopene |
GSH restoration, reduced MDA, membrane stabilization, lower cytokines |
Confirm clinical benefit and monitor herb-related hepatotoxicity risk |
|
Kidney |
Quercetin, EGCG, curcumin, resveratrol, astaxanthin |
Reduced tubular oxidative stress, preserved SOD/CAT/GPx, anti-apoptotic effects |
Ensure protection does not reduce anticancer drug efficacy |
|
Heart |
Resveratrol, quercetin, lycopene, coenzyme Q10, vitamin E |
Mitochondrial protection, anti-inflammatory signalling, improved contractile biomarkers |
Evaluate long-term ejection fraction and drug interactions |
|
Brain |
Curcumin, EGCG, Ginkgo biloba, astaxanthin, resveratrol |
Neuroinflammation reduction, mitochondrial support and lipid protection |
Improve brain delivery and use behavior plus biochemical endpoints |
|
Lung/GIT |
Vitamin C/E, polyphenols, carotenoids, plant extracts |
Epithelial protection, lower oxidative and inflammatory markers |
Avoid excessive antioxidant exposure that may disturb host defence |
8. Experimental Characterization and Evaluation Strategy
A scientifically acceptable organ-protection study should combine pharmacological, biochemical and histological evidence. Drug administration should be justified by clinically relevant dose or accepted experimental model. Antioxidant treatment should include dose rationale, route, duration and standardization of plant extract or pure compound. Control groups should include normal control, toxic control, antioxidant-only group where appropriate and treatment groups. Randomization, blinded histology and adequate sample size improve reliability. [1-3,29,30,34]
Biochemical evaluation should include organ-function markers and oxidative stress markers. For hepatic studies, ALT, AST, ALP, bilirubin, hepatic GSH, MDA, SOD, catalase and histology are useful. For renal studies, creatinine, urea, electrolyte balance, urine markers and renal histology are important. For cardiac studies, troponin, CK-MB, BNP, ECG, echocardiography and cardiac oxidative markers add value. For neurotoxicity, behavioral testing, neurotransmitter assays and histology should accompany antioxidant biomarkers. [1-3,29,30,34]
Characterization of natural antioxidants requires more than naming the plant source. Extracts should be standardized by total phenolic content, total flavonoid content, chromatographic fingerprinting or quantification of marker compounds. In vitro antioxidant assays such as DPPH, ABTS, FRAP and ORAC are useful screening tools but do not replace cellular or in vivo evidence. A compound with strong in vitro antioxidant activity may fail in vivo because of poor absorption, rapid metabolism or limited tissue distribution. [1-3,29,30,34]
Table 6. Recommended characterization and outcome parameters for future studies.
|
Study level |
Recommended parameters |
Reason for inclusion |
|
Phytochemical characterization |
Total phenolics, total flavonoids, HPLC/LC-MS marker profile, purity or extract standardization |
Ensures reproducibility and links activity to chemical composition |
|
In vitro antioxidant assay |
DPPH, ABTS, FRAP, ORAC and metal-chelation assays |
Provides preliminary antioxidant capacity but needs biological confirmation |
|
Cellular toxicity assay |
ROS probes, mitochondrial membrane potential, apoptosis markers, cytokines |
Identifies mechanism and cytoprotection in relevant cell types |
|
Animal organ toxicity model |
Organ function markers, oxidative enzymes, histology and dose-response analysis |
Determines whether biochemical changes translate into tissue protection |
|
Clinical evaluation |
Safety, pharmacokinetics, interaction testing, organ biomarkers and patient outcomes |
Required for evidence-based adjunctive use |
9. Formulation and Delivery Considerations
Many promising natural antioxidants suffer from poor water solubility, low permeability, chemical instability, rapid metabolism or extensive first-pass effect. Curcumin, resveratrol and quercetin are common examples where the pharmacological effect is limited by bioavailability. Formulation technologies such as nanoparticles, solid lipid carriers, phospholipid complexes, self-emulsifying systems, cyclodextrin inclusion complexes and phytosomes may improve solubility, stability and tissue exposure. [17-22,24,27,32]
Formulation improvement should not be treated as merely a technological addition. It can change pharmacokinetics, tissue distribution, safety and interaction potential. For example, increased bioavailability may enhance protective activity but may also increase adverse effects or drug interactions. Therefore, formulated antioxidants should undergo the same systematic evaluation as conventional pharmaceutical interventions, including stability, release, absorption, toxicity and dose optimization. [17-22,24,27,32]
Standardization is equally important for plant extracts. Variability in cultivation, harvesting, drying, extraction solvent and storage conditions can change bioactive composition. Without chemical standardization, different batches may show different potency and safety. A research-grade natural antioxidant product should clearly specify plant species, plant part, extraction method, marker compounds and quality-control limits. [17-22,24,27,32]
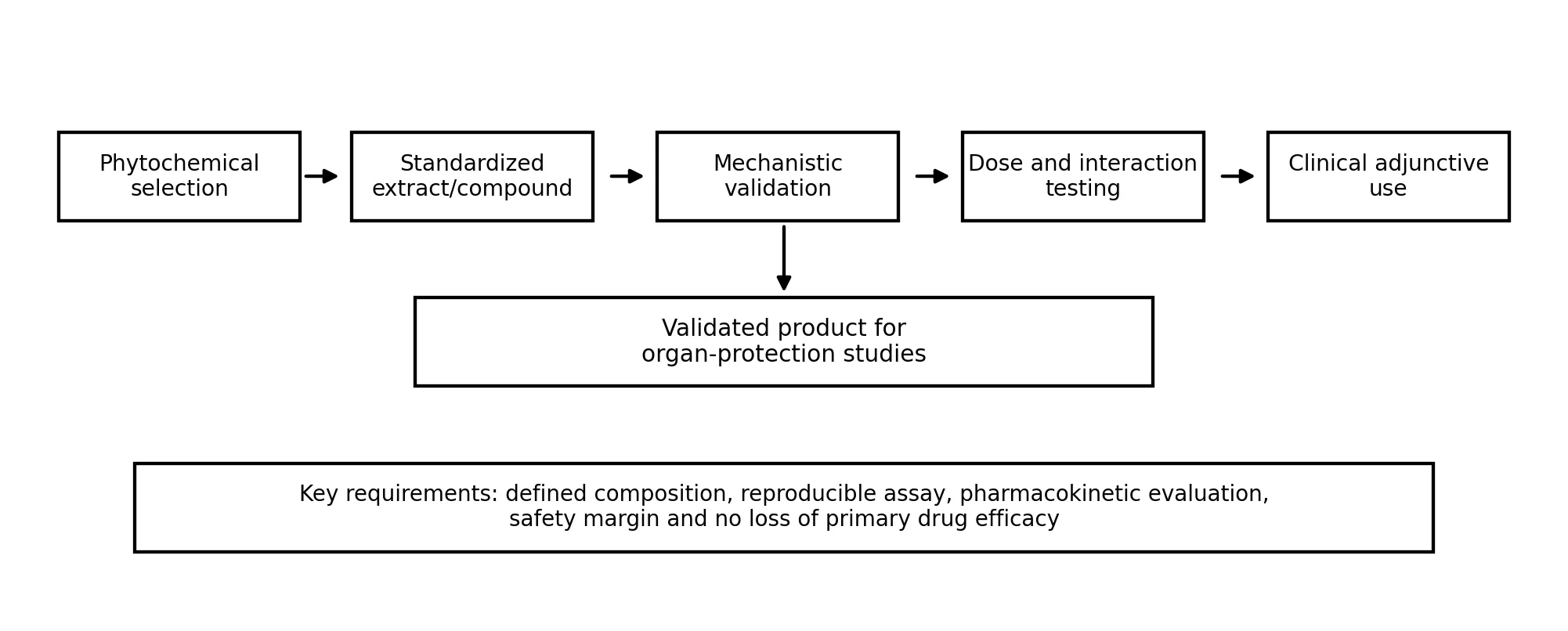
Figure 4. Translational workflow for developing natural antioxidant interventions against drug-induced organ toxicity.
10. Safety, Limitations and Drug-Herb Interaction Concerns
Natural origin does not automatically mean clinical safety. Several phytochemicals and herbal products can interact with drug-metabolizing enzymes, transporters, coagulation pathways or immune mechanisms. High-dose supplements may produce adverse effects or alter the pharmacokinetics of prescribed medicines. This is especially important in cancer chemotherapy, antitubercular therapy, anticoagulant therapy, antiepileptic therapy and transplant medicine. [23-25,29-35]
Another limitation is the difference between experimental models and clinical reality. Many preclinical studies use high antioxidant doses, short duration and controlled injury models. Human patients often have comorbidities, variable nutrition, genetic differences, polypharmacy and diverse degrees of organ reserve. Therefore, the conclusion that an antioxidant is protective in animals should be considered hypothesis-generating unless supported by controlled clinical trials. [23-25,29-35]
Bioavailability remains a major barrier. Polyphenols may undergo rapid glucuronidation, sulfation and microbial metabolism. The metabolites may differ from the parent compound in activity. Some antioxidant effects may arise from mild electrophilic or stress-adaptive signalling rather than from direct radical scavenging. Dose selection must therefore be based on pharmacokinetic and pharmacodynamic evidence, not only on traditional use or in vitro antioxidant values. [23-25,29-35]
A balanced approach is required. Natural antioxidants may be valuable supportive agents when standardized, appropriately dosed and evaluated for safety. They should not be promoted as replacements for established antidotes, dose adjustment, hydration, monitoring or withdrawal of the offending drug when clinically necessary. In drug-induced organ toxicity, supportive antioxidant use should remain integrated with conventional clinical decision-making. [23-25,29-35]
Table 7. Key challenges and practical solutions for translation of natural antioxidants.
|
Challenge |
Scientific concern |
Recommended solution |
|
Poor bioavailability |
Low tissue exposure may limit activity despite strong in vitro antioxidant effect |
Use validated delivery systems and pharmacokinetic studies |
|
Dose variability |
Traditional doses and experimental doses may not be comparable |
Define dose range, exposure and safety margin |
|
Extract variability |
Different batches may contain different active content |
Apply marker-based standardization and quality control |
|
Drug interaction risk |
Effects on CYP enzymes, transporters or therapeutic drug action |
Conduct interaction screening and avoid unsupervised use in high-risk therapy |
|
Limited clinical trials |
Preclinical findings may not predict patient outcomes |
Design randomized studies with organ-specific biomarkers and clinical endpoints |
|
Overgeneralization |
One antioxidant may not protect all organs or all drugs |
Use mechanism-matched antioxidant selection |
FUTURE PERSPECTIVES
Future research should move from descriptive antioxidant studies toward mechanism-guided organ protection. Selection of the natural antioxidant should match the dominant injury pathway of the toxic drug. For example, glutathione-supporting and mitochondrial-protective agents may be prioritized in acetaminophen-like toxicity, while anti-inflammatory and tubular-protective agents may be emphasized in cisplatin nephrotoxicity. This approach can avoid nonspecific screening and improve translational value. [8,12,15,30,34,35]
Multi-omics methods, network pharmacology, molecular docking, metabolomics and systems toxicology may help identify pathway-level effects of antioxidants. These tools can reveal whether a compound affects Nrf2 signalling, mitochondrial biogenesis, inflammatory pathways, ferroptosis, apoptosis or drug-metabolizing enzymes. However, computational predictions should be validated experimentally and should not replace biochemical and functional evidence. [8,12,15,30,34,35]
Combination antioxidant therapy may be useful because drug-induced toxicity is multi-factorial. A rational combination could include a radical scavenger, an Nrf2 activator and a mitochondrial stabilizer. Nevertheless, combinations increase complexity and interaction risk. Therefore, future studies should first establish safety, dose and mechanism of each component before evaluating combinations. [8,12,15,30,34,35]
Clinical translation requires well-designed trials. Important outcomes include reduction in organ injury biomarkers, preservation of function, decreased treatment interruption and absence of negative effects on the therapeutic action of the primary drug. Trials should also include pharmacovigilance for adverse effects and herb-drug interactions. Ultimately, the goal is to develop standardized, evidence-based supportive interventions rather than unregulated supplementation. [8,12,15,30,34,35]
CONCLUSION
Drug-induced organ toxicity remains a clinically significant problem and is strongly associated with oxidative stress, mitochondrial dysfunction, inflammation and cell-death pathways. The liver, kidney, heart, brain and lung are affected by different drug classes, but many share common redox-sensitive mechanisms. Natural antioxidants provide a scientifically plausible approach for mitigation of drug-induced injury because they can restore endogenous antioxidant defences, reduce lipid peroxidation, modulate inflammatory signalling and protect mitochondrial function. [1-35]
Curcumin, silymarin, quercetin, resveratrol, EGCG, lycopene, astaxanthin and antioxidant vitamins represent important examples of natural compounds with organ-protective potential. Their benefits have been supported mainly by experimental evidence and selected translational observations. However, poor bioavailability, lack of standardization, dose uncertainty and possible drug interactions limit immediate clinical application. The most appropriate future direction is mechanism-based, standardized and clinically validated antioxidant intervention. A scientifically developed natural antioxidant strategy may complement conventional therapy and reduce organ injury without compromising the primary therapeutic effect. [1-35]
REFERENCES


Pooja Thavare, Jayshri Hake, Abhijeet Pawar, Ghogare Ashvini, Prajakta Zagade, Prajakta Gaikwad, Role of Natural Antioxidants in Mitigating Drug-Induced Organ Damage: Mechanistic Basis, Organ-Specific Evidence and Translational Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7672-7687, https://doi.org/10.5281/zenodo.21066384
 10.5281/zenodo.21066384
10.5281/zenodo.21066384