
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Clinicogenomics Lab, Sir Surendranath Banerjea Advanced Research Centre, Department of Physiology, Surendranath College, University of Calcutta, India
2Department of Physiology, Vidyasagar Metropolitan College, University of Calcutta, India.
Female infertility is increasingly emerging as a multifactorial metabolic–endocrine systems disorder driven by the intricate interplay among endocrine imbalance, metabolic dysfunction, micronutrient deficiency, chronic inflammation, genetic susceptibility, and adverse lifestyle behaviour. Among the major infertility-associated conditions, polycystic ovary syndrome (PCOS) represents a complex metabolic–reproductive disorder characterized by hyperandrogenism, insulin resistance, oxidative stress, mitochondrial dysfunction, and impaired folliculogenesis. Accumulating evidence further indicates that sedentary lifestyle, unhealthy dietary practices, and vitamin D deficiency (VDD) collectively exacerbate reproductive dysfunction through interconnected molecular and endocrine pathways.This review critically integrates current evidences regarding the role of vitamin D signaling, lifestyle-associated metabolic disturbances, and PCOS biology in female infertility. Particular emphasis has been placed on the molecular mechanisms through which VDD and vitamin D receptor (VDR) polymorphisms modulate ovarian steroidogenesis, insulin signaling, inflammatory activation, oxidative stress, mitochondrial homeostasis, and hypothalamic–pituitary–ovarian axis regulation. Sedentary behaviour and excessive consumption of ultra-processed, calorie-dense diets further aggravate endocrine and metabolic dysregulation by altering AMPK, PI3K/Akt, mTOR, FOXO, and inflammatory signaling networks, thereby impairing ovulation, oocyte competence, endometrial receptivity, and fertility outcomes. Emerging evidence linking gut dysbiosis, altered enterohepatic estrogen metabolism, and chronic low-grade inflammation with infertility progression has also been discussed within a systems-biology framework.Collectively, the available evidence strongly supports the concept that female infertility should no longer be interpreted as an isolated ovarian disorder but rather as a systems-level metabolic–endocrine condition profoundly influenced by modifiable nutritional and lifestyle determinants. The review further highlights the translational significance of integrated lifestyle intervention, vitamin D optimization, metabolic regulation, and microbiome-targeted therapeutic strategies in advancing precision reproductive medicine and improving fertility outcomes.
Female infertility is increasingly being recognized as a complex metabolic–endocrine systems disorder arising from the intricate interplay among endocrine dysregulation, metabolic imbalance, genetic susceptibility, environmental exposure, and adverse lifestyle behaviour.[1] Among the diverse etiological contributors, ovulatory dysfunction remains one of the predominant causes of infertility, accounting for nearly 85% of cases, and is strongly influenced by sedentary living and excessive consumption of calorie-dense ultra-processed foods.[1,2] These factors profoundly impair fecundity, the intrinsic biological capacity for reproduction essential for maintaining reproductive homeostasis across populations.[3] Declining fecundity is therefore increasingly associated not only with intrinsic reproductive abnormalities but also with altered behavioural, nutritional, and environmental exposures characteristics of modern lifestyles. [3]
Accumulating evidence indicates that most ovulatory disorders characterized by chronic anovulation, hyperandrogenism, and menstrual irregularities are closely associated with PCOS, one of the most prevalent metabolic–reproductive disorders affecting women of reproductive age.[4,5] Beyond ovarian dysfunction, obesity, unhealthy dietary patterns, environmental toxicants, endocrine disruptors, and chronic metabolic stress adversely affect both the quantity and quality of oocytes, thereby compromising reproductive competence and fertility outcomes.[6] Emerging studies further suggest that sedentary behaviour and inadequate dietary intake of vitamin D substantially contribute to vitamin D deficiency (VDD)-associated reproductive dysfunction and PCOS progression.[7,8] According to the World Health Organization (WHO), nearly one in six individuals of reproductive age experiences infertility globally, with ovarian, tubal, uterine, endocrine, and metabolic abnormalities representing major contributing factors in women.[6] In addition to metabolic and endocrine disturbances, genetic abnormalities such as monosomy X, chromosomal deletions, duplications, and imbalanced X-autosome rearrangements may result in premature depletion of primordial follicles and gonadal dysgenesis.[9] Impaired granulosa cell signalling, abnormal follicular communication, and skewed X-chromosome inactivation (XCI) further contribute to accelerated germ cell depletion and primary ovarian insufficiency. [9]
Modern urbanization and technological dependence have dramatically increased physical inactivity worldwide, with nearly one-third of the global population failing to engage in adequate physical activity.[10] Prolonged office work, excessive screen exposure, social media dependence, and lack of exercise-supportive environments have collectively promoted chronic sedentary behaviour.[10-16] Such inactivity profoundly disrupts metabolic homeostasis by impairing protein transporter activity, altering lipid metabolism, reducing lipoprotein lipase activity, and dysregulating the insulin-like growth factor (IGF) axis, ultimately lowering insulin sensitivity and metabolic flexibility. [10] Sedentary behaviour additionally contributes to hypertension, endothelial dysfunction, altered sympathetic activity, and vascular impairment, all of which negatively influence reproductive physiology.[10-13] Increasing evidence indicates that restricted skeletal muscle activity and chronic physical inactivity significantly reduce ovulatory efficiency, conception potential, and reproductive fitness.[2,17-20] Conversely, moderate-to-vigorous physical activity improves cardiovascular health, insulin sensitivity, ovarian endocrine function, mental well-being, ovulation, and pregnancy outcomes.[2,21-25] Exercise-mediated activation of endothelial nitric oxide synthase (eNOS) and adenosine monophosphate-activated protein kinase (AMPK) enhances vascular circulation, fatty acid oxidation, glucose utilization, and metabolic balance, thereby exerting protective effects on reproductive physiology and ovarian function. [9-16]
Parallel to sedentary behaviour, unhealthy dietary transition and excessive consumption of junk food and ultra-processed diets have emerged as major contributors to female reproductive dysfunction. Foods enriched with refined sugars, saturated fats, cholesterol, sodium, and artificial additives stimulate dopamine-mediated reward pathways, promoting addictive eating behaviour and long-term metabolic dysregulation.[11-14] Chronic intake of high-glycaemic and energy-dense diets promotes obesity, insulin resistance, dyslipidemia, and endocrine imbalance while simultaneously depriving the body of essential micronutrients and antioxidant support. [11] Such dietary patterns are strongly associated with menstrual irregularities, dysmenorrhea, obesity, diabetes, and PCOS-associated infertility.[12,13] Moreover, unhealthy dietary behaviour disrupts hypothalamic–pituitary–ovarian axis (HPOA) signalling and impairs hormonal synchronization essential for ovulation and reproductive cyclicity. [12,13] Nutritional imbalance, fasting, and inadequate intake of proteins and essential amino acids further dysregulate nutrient-sensing pathways including forkhead box O (FOXO) transcription factors, which play critical roles in oxidative stress regulation, metabolic adaptation, ovarian aging, and reproductive longevity. [14,26-28]
Collectively, the growing interaction among sedentary lifestyle, unhealthy dietary practices, metabolic dysfunction, vitamin D deficiency, chronic inflammation, and PCOS biology strongly supports the concept that female infertility should be interpreted within a broader metabolic–endocrine systems framework rather than as an isolated ovarian disorder. These interconnected molecular and lifestyle-associated disturbances highlight the urgent need for integrated preventive, nutritional, metabolic, and lifestyle-based therapeutic strategies to improve reproductive health and fertility outcomes in women.
Rationale and Scopes of the Review
Despite growing evidence on the role of lifestyle factors in reproductive health, there remains a lacuna of guidelines, and personalised-tailored recommendations for physical activity and dietary interventions exist according to the baseline fitness level of patients, health status, and infertility-related diagnosis for the management and mitigation of infertility. Moreover, existing studies often focus on isolated aspects rather than providing an integrative understanding of molecular, physiological, and clinical interactions. These gaps hinder healthcare providers from offering clear, evidence-based recommendations on optimal exercise intensity, frequency, and dietary patterns to maximize the conception rates. Therefore, this review aims to comprehensively analyse the impact of sedentary lifestyle and junk food consumption on female fertility, highlighting mechanistic pathways, clinical implications, and potential therapeutic strategies by highlighting the intricacy of VDD-PCOS crosstalk from our previous study outcomes.
Methodology
Literature search strategy
A systematic and comprehensive literature search was conducted across major scientific databases, including PubMed, ScienceDirect, and PubMed Central (PMC), to ensure broad coverage of relevant studies. The search strategy was designed to capture both experimental and observational research, as well as review articles, thereby providing a multidimensional understanding of the topic. Emphasis was placed on peer-reviewed publications to ensure the reliability and scientific validity of the included data.
Keywords and time frame
The search incorporated specific keywords such as “female fertility,” “fecundity,” “sedentary lifestyle,” “junk food,” and “reproductive health,” combined using Boolean operators to refine results. The time frame spanned from January 2003 to March 2026, allowing inclusion of both foundational studies and recent advancements. This extensive temporal coverage facilitated the identification of evolving trends and emerging concepts in reproductive health research.
Study selection
Studies were selected based on relevance to the topic, methodological rigor, and clarity of outcomes. Only articles published in English were included to maintain consistency in interpretation. Both human and mechanistic studies were considered to integrate clinical observations with molecular insights. This approach ensured a balanced and comprehensive synthesis of evidence (Figure 1).
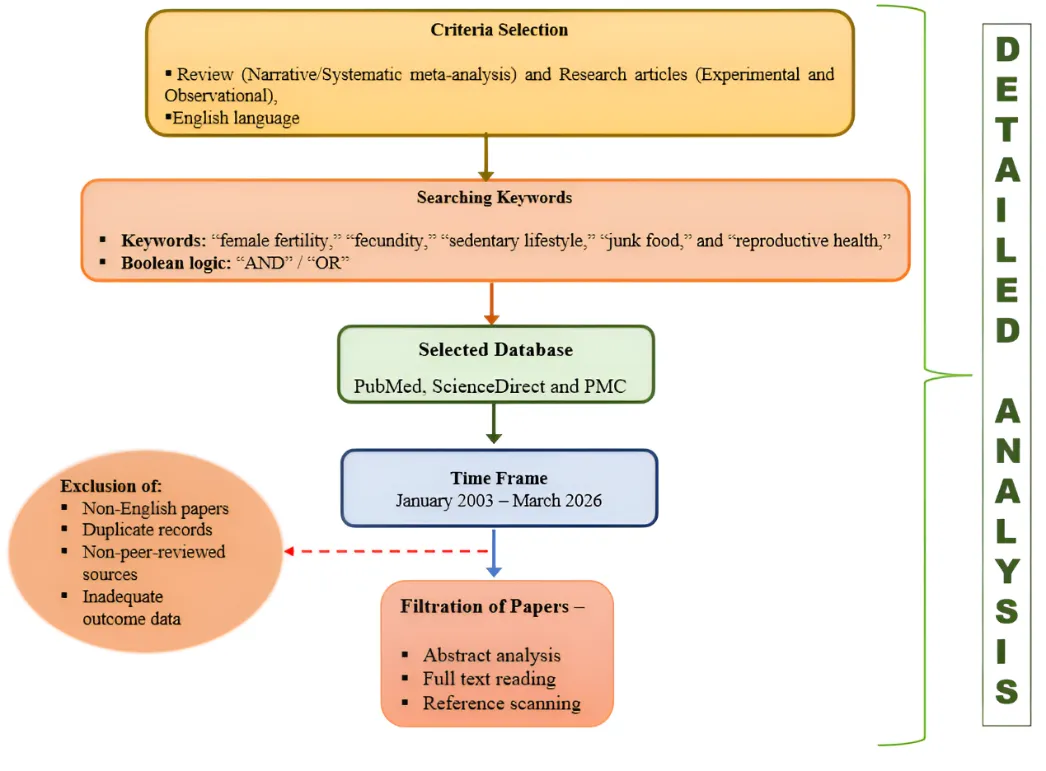
Figure 1: Overview of systematic literature search and study selection process.
Panel 1— Study types included: The search intentionally targeted multiple study designs narrated in English: experimental (in vitro, animal), observational (cohort, case‑control, cross‑sectional), and review articles. Emphasis on peer‑reviewed publications increased confidence in methodological quality and reliability of reported findings. Both human clinical studies and mechanistic investigations were included to integrate clinical outcomes with underlying biological mechanisms.
Panel 2 — Search strategy and keywords: A comprehensive search strategy combined specific keywords — “female fertility,” “fecundity,” “sedentary lifestyle,” “junk food,” and “reproductive health” — using Boolean operators (AND, OR) to refine retrieval and capture both focused and related articles. The search was restricted to publications in English and spanned the period June 1998 to March 2026, permitting inclusion of foundational studies and recent advances.
Panel 3: Major scientific databases (PubMed, ScienceDirect, PubMed Central) were queried to ensure broad coverage of biomedical and life‑science literature. These sources capture peer‑reviewed primary research, reviews, and mechanistic studies relevant to reproductive health.
Left panel — Exclusion criteria duplicated records, non‑peer‑reviewed sources, and studies lacking adequate outcome data.
Panel 4 — Screening and inclusion criteria: Retrieved records were screened for relevance to the research question, methodological rigor (study design, sample size, controls), and clarity of outcomes. Inclusion criteria required English language and direct relevance to female reproductive outcomes or mechanistic pathways linking lifestyle/nutrition to fecundity.
DISCUSSION
Reframing female infertility: beyond a linear reproductive model
Female infertility should no longer be interpreted as an isolated ovarian or gynecological disorder; rather, it represents a multifactorial metabolic–endocrine systems disorder arising from the continuous interaction among endocrine imbalance, metabolic dysfunction, ovarian impairment, oxidative stress, chronic low-grade inflammation, micronutrient deficiency, genetic susceptibility, and adverse environmental influences. Among the various etiological contributors, ovulatory dysfunction remains one of the predominant causes of infertility, with polycystic ovary syndrome (PCOS) representing the principal metabolic–endocrine disorder associated with chronic anovulation, impaired folliculogenesis, menstrual irregularities, hyperandrogenism, and reduced fecundity. Increasing evidence strongly indicates that reproductive dysfunction in PCOS extends far beyond ovarian morphology alone and instead reflects a complex systemic metabolic disturbance involving insulin resistance, adipokine dysregulation, mitochondrial dysfunction, inflammatory activation, and oxidative injury. [12,18,19,21-23,28,29]
Endocrine and metabolic aspects in PCOS-associated female infertility
At the molecular and endocrine level, hyperinsulinemia functions as one of the central pathogenic triggers underlying PCOS-associated infertility. Elevated circulating insulin concentrations stimulate ovarian theca cells, resulting in excessive androgen biosynthesis while simultaneously suppressing hepatic synthesis of sex hormone-binding globulin (SHBG), thereby increasing circulating free androgen concentrations. This hyperandrogenic endocrine milieu disrupts granulosa cell aromatase activity, impairs follicular maturation, and culminates in follicular arrest and chronic anovulation. Disturbed gonadotropin dynamics further aggravate reproductive dysfunction, particularly through dysregulated luteinizing hormone (LH) and follicle-stimulating hormone (FSH) secretion secondary to altered gonadotropin-releasing hormone (GnRH) pulsatility.[12,18,19,21-23,28,29] Such endocrine imbalance destabilizes hypothalamic–pituitary–ovarian axis (HPOA) regulation, adversely affecting ovulatory cyclicity, steroidogenesis, endometrial receptivity, and overall reproductive competence. Metabolic dysfunction represents another major hallmark of PCOS-associated infertility. Insulin resistance, obesity, dyslipidemia, altered adipokine secretion, and impaired glucose metabolism collectively contribute to a hostile metabolic environment unfavourable for normal ovarian physiology. Excess visceral adiposity acts not only as an energy-storage organ but also as a metabolically active endocrine tissue capable of secreting pro-inflammatory adipokines and cytokines including tumour necrosis factor alpha (TNF-α), interleukin-6 (IL-6), resistin, and leptin.[12,18,19,21-23,28,29] These mediators interfere with insulin receptor signalling pathways and steroidogenic balance, thereby perpetuating hyperinsulinemia, androgen excess, and endocrine dysfunction. Altered adipokine signalling additionally impairs follicular microenvironment integrity, oocyte maturation, and implantation potential. Consequently, PCOS-associated infertility should increasingly be interpreted as a manifestation of systemic metabolic dysregulation rather than a disorder confined solely to ovarian pathology.
Oxidative stress, and inflammatory dysregulation in PCOS-associated female infertility
Oxidative stress has also emerged as a major mechanistic contributor to reproductive dysfunction in PCOS. Increased production of reactive oxygen species (ROS) together with reduced antioxidant defense capacity disrupts cellular redox homeostasis within ovarian tissues. Excessive ROS accumulation damages granulosa cells, impairs mitochondrial integrity, alters meiotic spindle formation, and compromises oocyte competence. Oxidative injury additionally affects membrane lipid stability, protein structure, and DNA integrity within reproductive tissues, thereby accelerating follicular atresia and ovarian aging. Importantly, oxidative stress and insulin resistance exhibit a bidirectional relationship in PCOS, where hyperglycemia and lipid overload promote ROS generation while oxidative stress further aggravates insulin signalling impairment and endocrine dysfunction. [12,18,19,21-23,28,29] Mitochondrial dysfunction represents another critical pathological feature linking metabolic imbalance with infertility in PCOS. Mitochondria play an essential role in ATP generation, calcium homeostasis, steroidogenesis, and regulation of apoptotic pathways required for follicular development and oocyte maturation. Impaired mitochondrial oxidative phosphorylation reduces adenosine triphosphate (ATP) production within oocytes, negatively affecting meiotic competence, chromosomal stability, embryonic developmental potential, and follicular viability. Simultaneously, defective mitochondrial metabolism enhances ROS accumulation, thereby intensifying oxidative stress and inflammatory activation within the ovarian microenvironment. Such mitochondrial impairment ultimately compromises reproductive potential and fertility outcomes. Chronic low-grade inflammation further acts as a major mediator connecting metabolic dysfunction with endocrine and reproductive abnormalities in PCOS. Increased circulating inflammatory cytokines including TNF-α and IL-6 disrupt insulin-signalling pathways, interfere with ovarian steroidogenesis, and impair granulosa cell communication.[12,18,19,21-23,28,29] Inflammatory activation additionally compromises endothelial function and ovarian vascularization, thereby reducing oxygen and nutrient delivery to reproductive tissues. These alterations collectively impair follicular growth, ovulation, implantation, and endometrial receptivity. Therefore, the pathophysiology of PCOS-associated infertility should not merely be viewed through the lens of hormonal imbalance, but rather as the cumulative consequence of interconnected metabolic, endocrine, inflammatory, oxidative, and mitochondrial dysregulation collectively shaping female reproductive physiology and fertility outcomes.
Collectively, these findings strongly support the concept that infertility associated with PCOS should be interpreted within a broader systems-biology framework involving continuous interactions among endocrine pathways, metabolic homeostasis, micronutrient status, oxidative stress, mitochondrial integrity, genetic predisposition, and environmental exposures. This evolving perspective shifts the understanding of female infertility from a localized ovarian pathology toward a systemic metabolic–endocrine disorder profoundly shaped by modifiable lifestyle and nutritional determinants.
Vitamin D deficiency–VDR axis - a potential driver of PCOS-associated female infertility
An important mechanistic axis emerging from the present review is the intricate relationship among vitamin D deficiency (VDD), vitamin D receptor (VDR) polymorphisms, metabolic dysfunction, oxidative stress, inflammatory activation, and PCOS-associated infertility. Beyond its classical role in calcium and skeletal homeostasis, vitamin D functions as a pleiotropic secosteroid hormone regulating multiple endocrine, metabolic, immunological, mitochondrial, and reproductive signalling pathways essential for female reproductive physiology.[18,19,21-25] The biologically active form of vitamin D, 1,25-dihydroxyvitamin D₃ [1,25(OH)₂D₃], exerts its genomic effects through binding to the VDR, a ligand-activated nuclear transcription factor expressed in ovarian granulosa cells, theca cells, endometrial tissue, placenta, pituitary gland, and hypothalamic regions involved in reproductive regulation.[18,19,21-25] Following ligand binding, the VDR heterodimerizes with retinoid X receptor (RXR) and interacts with vitamin D response elements (VDREs) located within promoter regions of the target genes, thereby regulating transcriptional activity associated with steroidogenesis, folliculogenesis, insulin signalling, inflammatory modulation, cellular differentiation, and metabolic homeostasis.[18,19,21-30] Emerging evidence strongly suggests that VDD and altered VDR signalling may function as major upstream drivers of the metabolic–endocrine disturbances underlying PCOS and its associated infertility. Impaired vitamin D signalling disrupts ovarian physiology at multiple levels, including follicular recruitment, granulosa cell proliferation, oocyte maturation, and steroid hormone synthesis, thereby increasing susceptibility to chronic anovulation, follicular arrest, diminished ovarian reserve, and infertility progression. [18,19,21-32] Altered regulation of CYP19A1-mediated aromatase activity, anti-Müllerian hormone (AMH) signalling, and follicle-stimulating hormone receptor (FSHR) responsiveness further destabilizes estrogen–androgen balance, contributing to hyperandrogenism and PCOS/PMOS-associated reproductive dysfunction. [19,21-27] The close association among VDD, AMH dysregulation, insulin resistance indices, and endocrine imbalance strongly supports vitamin D as both a biomarker and a potential therapeutic target in metabolic–reproductive disorders. [21-25,33-40]
Vitamin D - metabolic, endocrine regulator in PCOS
At the metabolic level, VDD significantly aggravates insulin resistance, adipokine imbalance, obesity, dyslipidemia, and hyperinsulinemia, thereby creating a hostile endocrine milieu unfavourable for ovulation, fertilization, implantation, and embryonic development.[18,19,21-28,41-48] Reduced vitamin D-mediated activation of PI3K/Akt signalling impairs insulin receptor phosphorylation, glucose uptake, and cellular metabolic regulation, ultimately promoting hyperinsulinemia-driven ovarian androgen excess. [21-25,49-55] Elevated insulin concentrations subsequently stimulate ovarian theca cells to enhance androgen biosynthesis while suppressing hepatic synthesis of sex hormone-binding globulin (SHBG), thereby increasing circulating free androgen levels and perpetuating follicular arrest and chronic anovulation. VDD-associated adipokine dysregulation additionally interferes with leptin and adiponectin signalling, further intensifying metabolic dysfunction, endocrine imbalance, and ovarian impairment.[56-65]
Vitamin D - oxidative stress, inflammatory dysregulation, and gut dysbiosis in PCOS
Oxidative stress and mitochondrial dysfunction also appear to be critically linked with impaired vitamin D signalling in PCOS-associated infertility. Defective VDR-mediated regulation disrupts mitochondrial oxidative phosphorylation and reduces ATP generation required for spindle formation, chromosomal stability, follicular maturation, and oocyte competence.[21-25,66-72] Simultaneously, increased accumulation of reactive oxygen species (ROS) promotes granulosa cell apoptosis, oxidative DNA damage, follicular atresia, and premature ovarian aging. Oxidative stress further interferes with insulin-signalling pathways and steroidogenic regulation, thereby amplifying endocrine dysfunction and metabolic instability. Consequently, VDD-associated oxidative injury may represent one of the central mechanisms connecting metabolic dysregulation with impaired reproductive potential in PCOS. Chronic low-grade inflammation represents another major pathological axis influenced by VDD and VDR polymorphisms. Vitamin D normally exerts potent immunomodulatory and anti-inflammatory effects by suppressing inflammatory cytokine production and regulating immune homeostasis. Deficiency states, however, promote inflammatory activation through increased expression of pro-inflammatory mediators including tumour necrosis factor alpha (TNF-α), interleukin-6 (IL-6), and interleukin-1β (IL-1β), thereby aggravating insulin resistance, endothelial dysfunction, oxidative stress, and ovarian steroidogenic imbalance.[18,19,21-28,73-82] Emerging evidences additionally suggests that VDR polymorphisms, particularly FokI and BsmI variants, influence inflammatory responsiveness, systemic vitamin D bioavailability, metabolic phenotype, and susceptibility to reproductive dysfunction, thereby highlighting a critical gene–nutrient interaction axis in female infertility.[21-25] Another important mechanistic dimension linking VDD with infertility involves gut dysbiosis and intestinal immune dysfunction. Vitamin D signalling through VDR regulates intestinal epithelial barrier integrity, tight junction protein expression, mucosal immunity, microbial diversity, and gut metabolic homeostasis. [79-82] Deficiency states impair gut barrier function, resulting in increased intestinal permeability or “leaky gut,” which facilitates translocation of lipopolysaccharides and endotoxins into systemic circulation.[79-82] This metabolic endotoxemia activates toll-like receptor-4 (TLR4) and nuclear factor kappa B (NF-κB)-mediated inflammatory pathways, leading to chronic low-grade inflammatory activation and worsening insulin resistance, oxidative stress, and ovarian dysfunction.[79-82] VDD-associated gut dysbiosis may additionally disturb microbial estrogen metabolism, enterohepatic circulation, short-chain fatty acid (SCFA) production, neurotransmitter synthesis, and hypothalamic–pituitary–ovarian axis (HPOA) regulation, thereby indirectly impairing ovulatory cyclicity, menstrual regulation, endometrial receptivity, and implantation potential. [79-82]
Collectively, the cumulative molecular evidence strongly supports the concept that vitamin D deficiency and VDR polymorphisms are not merely associated biomarkers, but potential mechanistic drivers of the metabolic, endocrine, oxidative stress, inflammatory, mitochondrial, and gut-microbiota-associated dysregulation underlying PCOS and its associated infertility. These interconnected disturbances reinforce the emerging concept that female infertility should be interpreted within a broader systems-biology framework shaped profoundly by gene–nutrient–microbiome interactions, sedentary indoor lifestyle, inadequate sunlight exposure, unhealthy dietary behaviour, and modifiable environmental determinants. [18,19,21-28,79-82]
Sedentary lifestyle: molecular driver, not just a risk factor
Physical activity: metabolic, endocrine, and neurophysiological regulation of reproductive function
Regular physical activity plays a fundamental role in maintaining female reproductive health through its integrated effects on metabolic homeostasis, endocrine regulation, vascular physiology, and neuroendocrine balance. Exercise significantly improves insulin sensitivity, which is particularly important in women with metabolic disturbances such as PCOS, obesity, and insulin resistance-associated ovulatory dysfunction.[38-42] Improved insulin signalling reduces hyperinsulinemia-mediated ovarian androgen production, thereby lowering hyperandrogenism and restoring normal ovulatory cycles and follicular maturation. [38-42] In addition, physical activity promotes healthier body composition and reduces adiposity-related endocrine disturbances that adversely affect ovarian physiology and fertility potential.[38-42] Exercise also regulates gonadotropin dynamics by stabilizing the pulsatile secretion of GnRH, which is essential for balanced LH and FSH secretion during folliculogenesis. [38-42] Enhanced peripheral insulin sensitivity prevents excessive ovarian theca cell stimulation and reduces androgen biosynthesis, thereby improving granulosa cell activity and oocyte maturation.[38-42] Furthermore, exercise modulates adipokine signalling, particularly through increased adiponectin and improved leptin regulation, which contribute to anti-inflammatory effects, metabolic stability, and a healthier ovarian microenvironment.[38-42] At the molecular level, physical activity activates key metabolic pathways involved in cellular energy regulation and reproductive physiology. Exercise-induced activation of AMPK promotes fatty acid oxidation, improves glucose uptake, and enhances metabolic flexibility, thereby restoring endocrine balance and ovarian function.[43,44] Simultaneously, exercise stimulates eNOS, improving vascular function and ovarian blood circulation, which support follicular development, endometrial receptivity, and implantation potential. [41,42,45,46] Improved tissue perfusion additionally enhances oxygen and nutrient delivery to reproductive tissues, contributing to improved fertility outcomes. Physical activity further exerts protective effects through regulation of oxidative stress and inflammatory pathways. Exercise promotes mitochondrial biogenesis via activation of peroxisome proliferator-activated receptor gamma coactivator-1 alpha (PGC-1α), thereby improving oxidative metabolism and reducing ROS accumulation.[47,48] Reduced oxidative stress preserves oocyte quality and follicular integrity. In parallel, regular exercise decreases pro-inflammatory cytokines such as TNF-α and IL-6 while enhancing anti-inflammatory mediators, thereby reducing chronic low-grade inflammation associated with infertility and metabolic dysfunction.[49,50] Improved insulin receptor phosphorylation and activation of phosphatidylinositol 3-kinase/protein kinase B (PI3K/Akt) signalling pathways further strengthen insulin responsiveness and ovarian metabolic regulation. [51]
Physical activity and psychological benefits
Beyond metabolic and endocrine regulation, exercise significantly influences psychological and neuroendocrine health, both of which are closely linked with reproductive function. Infertility is frequently associated with anxiety, depression, stress, and reduced quality of life. Physical activity improves emotional well-being through exercise-induced release of endorphins and brain-derived neurotrophic factor (BDNF), which enhance mood, cognitive function, and stress resilience. [45] Regular exercise also reduces cortisol levels and normalizes hypothalamic–pituitary–adrenal axis (HPAA) activity, thereby counteracting stress-induced suppression of GnRH pulsatility and ovulatory dysfunction.[33,40,52] Furthermore, exercise enhances serotonergic and dopaminergic signalling, improving emotional regulation and reducing infertility-associated psychological burden. [53,54] Improved sleep quality and stabilization of circadian rhythms associated with regular physical activity additionally influence melatonin secretion, antioxidant defense, and hormonal synchronization essential for reproductive cyclicity and oocyte quality. [55,56]
Experimental and clinical evidence supporting exercise in fertility improvement
Experimental, observational, and clinical studies consistently support the beneficial role of physical activity in improving female reproductive health and fertility outcomes.[56-65] Randomized controlled trials (RCTs) demonstrate that structured exercise interventions significantly improve ovulation rates, menstrual regularity, endocrine balance, and pregnancy outcomes, particularly among overweight women and individuals with PCOS.[56-58] Improved insulin sensitivity and reduction of hyperinsulinemia-driven androgen excess appear to be major mechanisms underlying restoration of ovulatory function in these populations.[38-40] Clinical investigations further indicate that exercise-mediated improvements in adiposity, inflammatory status, vascular function, and hormonal balance collectively enhance follicular development, endometrial receptivity, and implantation success.[41,42] Longitudinal lifestyle intervention studies also reveal that combining exercise with dietary modification produces superior improvements in insulin sensitivity, metabolic stability, ovulatory function, and reproductive outcomes compared with isolated interventions alone.[60-65] These findings strongly support the concept that reproductive dysfunction is closely linked with modifiable metabolic and lifestyle-associated factors. Experimental evidence additionally highlights the importance of exercise-induced mitochondrial adaptation and oxidative stress regulation in ovarian physiology. Enhanced mitochondrial function and reduced ROS accumulation improve oocyte competence and protect reproductive tissues from oxidative damage associated with obesity, insulin resistance, and chronic inflammation. [47-50] Studies examining molecular signalling pathways further demonstrate that exercise modulates AMPK and PI3K/Akt signalling, both of which are critically involved in steroidogenesis, glucose metabolism, follicular survival, and ovarian endocrine regulation. [37-45,43-51] Reduction in stress, anxiety, and depressive symptoms following regular physical activity has been associated with improved HPOA regulation and restoration of reproductive endocrine balance. [68-70] Exercise-induced normalization of cortisol secretion and circadian rhythm stability may therefore indirectly enhance ovulatory function and fertility outcomes. [33,40,55,56]
However, existing evidence also emphasizes that the reproductive effects of exercise follow a dose-dependent relationship. Moderate-intensity aerobic activity appears most beneficial, whereas excessive exercise, prolonged endurance training, or severe caloric restriction may induce hypothalamic suppression, luteal phase defects, and functional hypothalamic amenorrhea.[59-61] Energy deficiency states associated with excessive physical exertion disrupt GnRH pulsatility and ovarian hormonal regulation, ultimately impairing ovulation and fertility.[60,61] Variability in reproductive outcomes across studies further suggests that factors such as baseline body mass index (BMI), metabolic status, age, and hormonal profile significantly influence individual responses to exercise interventions. [60-65]
Collectively, current evidences establish physical activity as a major protective regulator of female reproductive health. Through coordinated metabolic, endocrine, inflammatory, vascular, mitochondrial, and neuropsychological mechanisms, regular moderate exercise improves ovarian physiology, hormonal balance, ovulation, implantation potential, and fertility outcomes. These findings reinforce the importance of individualized and precision-based lifestyle interventions in reproductive medicine, particularly for women affected by PCOS and lifestyle-associated metabolic dysfunction (Table 1). [56-65]
|
Table 1: Effects of physical activity on female reproductive health |
||||
|
Assessment of physical activity |
Study design |
Finding(s) |
Possible mechanism(s) |
Reference(s) |
|
Vigorous to mild exercise controlled caloric intake to calorie deficit |
Randomized controlled trial (premenopausal eumenorrheic women, n=34) |
Moderate and severe energy deficit leads experienced luteal phase defect of menstrual cycles (85%) and anovulation (35%) |
|
[62] |
|
Sedentary women and active runners running |
Cross-sectional study (eumenorrheic women, n=35) |
In 9% of sedentary group luteal phase was defective |
|
[63] |
|
Physical activity lowers the likelihood of infertility. |
Comprehensive systematic review and meta-analysis
|
An inverse correlation between varying levels of physical activity and infertility. A moderate to high level of physical activity significantly decreased the overall risk of infertility, identifying this level of physical activity as a prevalent protective factor. |
|
[64] |
|
A 4-month exercise program with a physical therapist (Tailored: content, and frequency) |
Randomized parallel design (n=43), PCOS women (overweight or obese) |
Higher (65%) ovulationary rate and spontaneous pregnancy (35%) in the exercise group |
|
[65] |
AMPK=adenosine monophosphate-activated protein kinase, NPY=neuropeptide Y, AgRP=agouti-related peptide, LH=luteinizing hormone, CL=corpus luteum, P4=progesterone, LPD=luteal phase defect, PCOS= polycystic ovary syndrome
Junk food, fast food, and ultra-processed diets: impact on female reproductive health
Unhealthy foods - Neuroendocrine, metabolic, and molecular disruption of reproductive function
Frequent consumption of junk food, fast food, and ready-to-eat ultra-processed diets has emerged as a major lifestyle-associated contributor to female reproductive dysfunction and infertility. These dietary patterns, characterized by excessive intake of refined sugars, saturated fats, trans fats, sodium, food additives, and calorie-dense nutrient-poor ingredients, profoundly disturb endocrine, metabolic, inflammatory, and neurophysiological pathways essential for normal reproductive function.[66-72] Evidence increasingly suggests that unhealthy dietary behaviour does not merely coexist with infertility-related disorders but actively participates in the pathogenesis of ovulatory dysfunction, menstrual irregularities, and PCOS-associated reproductive impairment.[12,18,21-23,28] One of the central mechanisms linking junk food consumption with infertility is the development of insulin resistance and chronic hyperinsulinemia. High glycaemic load diets induce repeated insulin surges that stimulate ovarian theca cells to produce excessive androgens while simultaneously suppressing hepatic synthesis of SHBG, thereby increasing circulating free androgen levels. [12,18,21-23,28] This hyperandrogenic environment disrupts follicular maturation, impairs granulosa cell function, and promotes follicular arrest and chronic anovulation, which are hallmark features of PCOS-associated infertility.[12,18,21-23,28] In addition, altered GnRH pulsatility and disruption of hypothalamic–pituitary–ovarian axis (HPOA) regulation further destabilize ovulatory cyclicity and menstrual function (Table 2). [66-68]
|
Table 2: Effects of junk food on female reproductive health |
||||
|
Assessment of junk food |
Study design |
Finding(s) |
Possible mechanism(s) |
Reference(s) |
|
High consumption of ultra-processed foods is associated with female infertility |
Cross-sectional study (n=3060) in National Health and Nutrition Examination Survey |
Among women of reproductive age, a high intake of ultra-processed foods is linked to female infertility. Body mass index (BMI) serves as a mediator in the relationship between ultra-processed foods consumption and female infertility. |
|
[69] |
|
The relationship between the consumption of junk food and the body mass index of adolescent girls, as well as the associated menstrual irregularities, will be examined and compared with a control group. |
Cross-sectional study (n=200) |
The intake of junk food has a detrimental impact on the menstrual cycle; however, further research is required to validate the correlation between BMI, the consumption of salty snacks, and frozen meat products with menstrual irregularities. |
|
[70] |
|
Skipping breakfast |
Questionnaire survey (n=315) |
Menstrual disorders in young college students |
|
[71] |
|
The quantity or quality of carbohydrates in one's diet is linked to ovulatory infertility. |
Married and premenopausal women=18555 |
The quantity and quality of carbohydrates in the diet may play a significant role in influencing ovulation and fertility among healthy women. |
|
[72] |
|
Nutritional geometry methods applied to Drosophila lines that vary solely in their mitochondrial DNA (mtDNA), with the objective of determining whether there exists nutrient-dependent mitochondrial genetic variation affecting male reproduction. |
Drosophila melanogaster |
The interaction between mitochondrial DNA and dietary habits in relation to fitness indicates that mtDNA is involved in the regulation of fitness that is dependent on diet. |
|
[72] |
|
The fertility of couples undergoing treatment with a daily tablet containing a patented blend of vitex agnus-castus (vitex) extract, lepidium meyenii (maca) extract, and active folate, either alone or in conjunction with a gel capsule comprising vitamins, minerals, oligo-elements, as well as docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) omega 3 fatty acids. |
Clinical trial (n=189) |
The patented formulation, which includes a mixture of vitex, maca, and active folate, helps to regulate the menstrual cycle, promotes ovulation, and enhances the chances of conception. |
|
[72] |
GnRH= gonadotropin‑releasing hormone, FSH/LH=follicle-stimulating hormone/luteinizing hormone
At the molecular level, junk food consumption profoundly alters nutrient-sensing and metabolic regulatory pathways involved in reproductive physiology. Excessive caloric intake and poor-quality diet dysregulate AMPK, mechanistic target of rapamycin (mTOR), forkhead box O (FOXO), and fibroblast growth factor 21 (FGF21) signalling pathways, all of which coordinate cellular metabolism, oxidative stress responses, aging, and ovarian function. [73-78] AMPK normally functions as a cellular energy sensor that promotes metabolic balance and preserves cellular integrity under low-energy conditions, whereas excessive nutrient availability and overactivation of mTOR signaling promote metabolic imbalance and ovarian dysfunction. [76-78] FOXO transcription factors play critical roles in oxidative stress resistance, apoptosis regulation, and maintenance of oocyte quality, while FGF21 contributes to systemic energy homeostasis and reproductive adaptation during metabolic stress.[57-62,73-78] Dysregulation of these interconnected pathways disrupts the balance between metabolism and reproduction, thereby accelerating reproductive decline and infertility progression.[76-78] Chronic intake of ultra-processed food also promotes oxidative stress and systemic inflammation through accumulation of advanced glycation end-products (AGEs), lipid overload, and inflammatory activation.[66-72,79-82] Increased production of ROS damages ovarian tissues, impairs oocyte quality, and compromises follicular microenvironment integrity.[34,35] Simultaneously, visceral adiposity associated with unhealthy dietary behaviour acts as an endocrine organ that secretes pro-inflammatory cytokines such as TNF-α, IL-6, and resistin, which interfere with insulin receptor signalling and ovarian steroidogenesis.[34,35,83,84] This chronic inflammatory state aggravates endocrine dysfunction, hyperandrogenism, and ovulatory failure while reducing implantation success and fertility potential (Figure 2). [34,35,83,84]
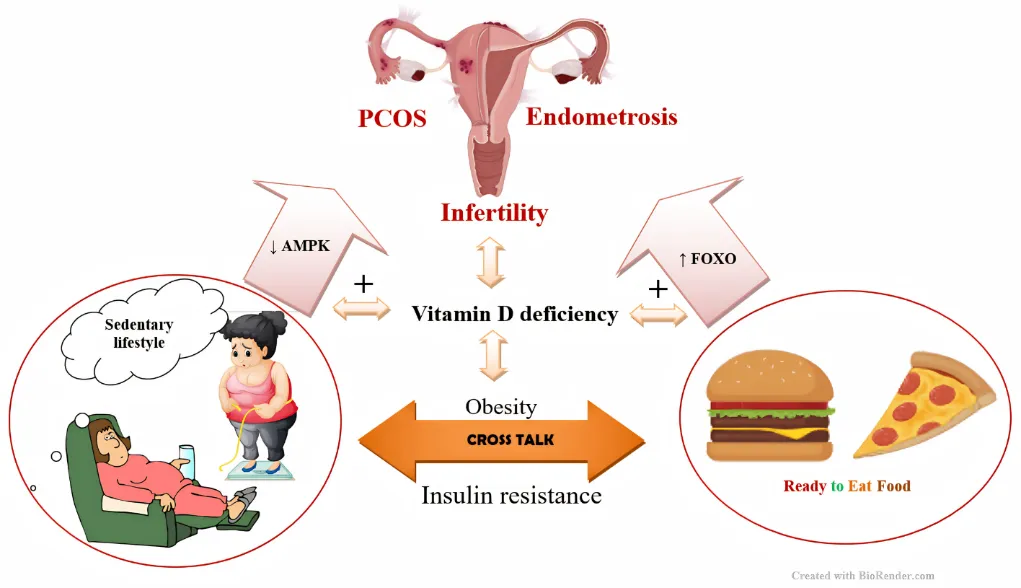
Figure 2: Schematic representation of the effect of sedentary lifestyle, junk food on molecular pathways linking PCOS, endometriosis, and infertility. Lifestyle and metabolic risk factors: sedentary lifestyle, high intake of junk food, and vitamin D deficiency are shown as the determinants. These factors promote systemic metabolic dysfunction, including insulin resistance and obesity. The metabolic consequences drive nutrient-sensing and stress-response nodes of altered AMPK activity and altered FOXO transcription factor signaling. The altered AMPK/FOXO pathways lead to PCOS manifestations and persistence of endometriosis. PCOS=polycystic ovary syndrome, AMPK = adenosine monophosphate-activated protein kinase, FOXO=Forkhead box transcription factors. ↓= decrease, ↑=increase, +=stimulation
Unhealthy foods - Gut Dysbiosis and reproductive pathophysiology
Emerging evidence identifies gut microbiota dysbiosis as a major mechanistic link between unhealthy dietary behaviour, metabolic dysfunction, chronic inflammation, and female infertility.[79-82] Frequent consumption of junk food, fast food, and ultra-processed diets rich in saturated fats, refined sugars, artificial additives, and low-fiber content profoundly alters gut microbial diversity and composition, thereby disrupting intestinal metabolic homeostasis.[79-82] Such dietary patterns reduce beneficial microbial populations involved in short-chain fatty acid (SCFA) production while simultaneously promoting the proliferation of pro-inflammatory gram-negative bacteria. This microbial imbalance compromises intestinal barrier integrity by disrupting tight junction proteins, leading to increased intestinal permeability or “leaky gut” phenomenon.[79-82] Enhanced intestinal permeability facilitates translocation of lipopolysaccharides and other endotoxins into systemic circulation, resulting in metabolic endotoxemia and activation of chronic low-grade inflammatory pathways.[79-82] LPS-mediated activation of toll-like receptor-4 (TLR4) signalling stimulates nuclear factor kappa B (NF-κB)-dependent inflammatory cascades, increasing production of pro-inflammatory cytokines such as TNF-α, IL-6, and interleukin-1β (IL-1β).[79-82] These inflammatory mediators interfere with insulin receptor signalling pathways, aggravating insulin resistance and hyperinsulinemia, which are central pathogenic mechanisms underlying PCOS-associated infertility and ovulatory dysfunction.[79-82] Hyperinsulinemia further stimulates ovarian theca cells to enhance androgen biosynthesis while suppressing hepatic SHBG synthesis, thereby increasing free androgen concentrations and promoting follicular arrest and chronic anovulation. Gut dysbiosis additionally affects reproductive endocrinology through modulation of estrogen metabolism and enterohepatic circulation. Altered microbial β-glucuronidase activity influences estrogen deconjugation and reabsorption, thereby disrupting circulating estrogen levels and hormonal homeostasis essential for folliculogenesis, ovulation, and endometrial receptivity.[79-82] Disturbed gut microbial composition may also impair synthesis of essential metabolites involved in neurotransmitter regulation, including serotonin, dopamine, and gamma-aminobutyric acid (GABA), thereby indirectly influencing HPOA regulation and GnRH pulsatility.[79-82] At the ovarian level, chronic systemic inflammation and oxidative stress associated with dysbiosis compromise follicular microenvironment integrity and oocyte competence. Increased ROS generation impairs mitochondrial function within ovarian cells, reducing ATP production required for oocyte maturation and embryonic development.[79-82] Inflammatory cytokines additionally disrupt granulosa cell steroidogenesis and follicular signalling pathways, thereby impairing ovulation and implantation potential. Dysbiosis-associated metabolic disturbances also alter adipokine secretion, particularly leptin and adiponectin signalling, further aggravating endocrine imbalance and reproductive dysfunction. Another critical aspect involves the role of endocrine-disrupting chemicals, food preservatives, emulsifiers, artificial sweeteners, and trans fats commonly present in ultra-processed foods.[79-83] These compounds may directly interfere with hormone receptor signalling, steroidogenic enzyme activity, and epigenetic regulation of reproductive genes. Experimental studies suggest that such dietary components influence DNA methylation, histone modification, and microRNA expression associated with metabolic regulation, inflammation, and ovarian physiology.[79-82] Furthermore, disturbed circadian eating behaviour frequently associated with fast food consumption disrupts hormonal synchronization involving LH, cortisol, and melatonin secretion, thereby destabilizing menstrual cyclicity and reproductive endocrine regulation. [69,70,72,84]
Collectively, current molecular and experimental evidence strongly supports gut dysbiosis as a central mediator linking unhealthy dietary patterns with infertility, PCOS progression, chronic inflammation, oxidative stress, and endocrine dysfunction. These findings highlight the potential therapeutic significance of microbiota-targeted nutritional interventions, dietary modification, and restoration of intestinal metabolic homeostasis in improving female reproductive health and fertility outcomes. [79-82,85]
Experimental and clinical evidence linking unhealthy diets with infertility
Experimental, epidemiological, and clinical studies consistently demonstrate a strong association between unhealthy dietary patterns and adverse reproductive outcomes. [12,18,21-23,28,66-72,86] Observational studies indicate that women with frequent consumption of junk food and fast food exhibit higher prevalence of menstrual irregularities, dysmenorrhea, oligomenorrhea, premenstrual syndrome, obesity, and PCOS-associated infertility.[12,18,21-23,28,87] Diets rich in refined carbohydrates and trans fats have also been associated with reduced ovulatory fertility and impaired endocrine balance.[87-90] Clinical evidence further suggests that regular intake of ultra-processed foods increases the risk of insulin resistance, dyslipidemia, obesity, and metabolic syndrome, all of which adversely affect ovarian physiology and reproductive competence.[83,84] Elevated triglycerides, reduced high-density lipoprotein (HDL) levels, and ectopic lipid accumulation impair endothelial function and ovarian blood flow, thereby negatively influencing follicular development, fertilization, and implantation processes. [34,35,91] Studies additionally report that women consuming fast food more than once daily experience significantly higher infertility risk and poorer reproductive outcomes compared with individuals following balanced dietary practices. [66-72] Epidemiological studies in adolescents and young women indicate that excessive junk food consumption may contribute to earlier onset of menarche, which is associated with long-term endocrine and metabolic consequences including increased risk of PCOS and infertility later in life.[12,18,21-23,28] Experimental studies also reveal that diets high in saturated fats and refined sugars alter prostaglandin metabolism, particularly increasing pro-inflammatory prostaglandin F2α (PGF2α), thereby contributing to uterine hypercontractility, dysmenorrhea, and menstrual disturbances.[69,85] Importantly, several interventional and nutritional studies demonstrate that dietary modification can improve reproductive outcomes by restoring metabolic and endocrine homeostasis.[66-72] Balanced diets enriched with antioxidants, fiber, omega-3 fatty acids, vitamins, and micronutrients improve insulin sensitivity, reduce oxidative stress, and support ovarian function.[86,87,92] Dietary restriction and nutritional optimization further activate protective metabolic pathways involving FOXO and AMPK signalling, thereby improving mitochondrial function, reducing inflammatory burden, and preserving ovarian reserve. [75,76,88]
However, variability in study design, dietary assessment methods, and population characteristics limits direct comparison across studies.[86,87,93] Despite these limitations, current evidence strongly supports the concept that junk food and ultra-processed dietary patterns represent significant modifiable risk factors for female reproductive dysfunction. Collectively, the available experimental and clinical findings reinforce the importance of dietary regulation, nutritional awareness, and lifestyle-based interventions as central preventive and therapeutic strategies for improving fertility outcomes and reproductive health in women. [12,18,21-23,28,86,87]
PCOS- PMOS: a nexus of lifestyle–genetic interaction
The multidimensional metabolic, endocrine, inflammatory, and reproductive disturbances associated with PCOS strongly support the recently proposed nomenclature shift toward “Polyendocrine Metabolic Ovarian Syndrome (PMOS),” which more accurately reflects the systemic nature of the disorder rather than limiting it to ovarian morphology alone. The findings discussed in this review demonstrate that insulin resistance, chronic inflammation, vitamin D deficiency, adipokine imbalance, and lifestyle-associated metabolic dysfunction collectively contribute to reproductive impairment, emphasizing the broader metabolic complexity underlying the syndrome. Furthermore, the beneficial impact of healthy dietary practices and regular physical activity on endocrine, metabolic, and reproductive homeostasis reinforces the concept that PMOS is fundamentally a multisystem metabolic–reproductive disorder influenced by modifiable lifestyle factors.[18,19,21-29,38-65,94-96] Exercise-induced activation of AMPK promotes fatty acid oxidation, improves glucose uptake through enhanced GLUT4 expression, and restores metabolic balance. These changes contribute to normalization of ovarian steroidogenesis, improved follicular maturation, and restoration of ovulatory cycles. Exercise additionally stimulates eNOS activity, improving vascular function and blood circulation to reproductive tissues. Enhanced ovarian perfusion supports follicular development and endometrial receptivity, thereby improving implantation potential and pregnancy outcomes. At the molecular level, physical activity promotes mitochondrial biogenesis through activation of PGC-1α, enhancing oxidative metabolism and reducing ROS accumulation.[18,19,21-29,38-65,94-96] Exercise also suppresses inflammatory pathways by reducing TNF-α and IL-6 levels while increasing anti-inflammatory mediators. Improved insulin receptor phosphorylation and activation of PI3K/Akt pathways further restore insulin signalling and ovarian function. An equally important aspect highlighted in this review is the neuroendocrine and psychological benefit of exercise. Physical activity modulates HPAA activity, reduces cortisol levels, improves serotonergic and dopaminergic signalling, and enhances release of endorphins and BDNF. These neuropsychological improvements reduce infertility-associated stress and indirectly restore reproductive endocrine balance. [18,19,21-29,38-65,94-96]
Evidence summarized in this review consistently indicates that moderate-intensity exercise improves ovulation rates, menstrual regularity, hormonal balance, and pregnancy outcomes, particularly in overweight and PCOS populations. However, the review also acknowledges that excessive exercise and severe caloric restriction may induce hypothalamic suppression and anovulation, emphasizing the need for balanced and individualized physical activity recommendations. Healthy dietary habits similarly exert protective effects on reproductive physiology by restoring metabolic and endocrine homeostasis. Nutrient-dense and balanced diets improve insulin sensitivity, reduce inflammation, and provide essential micronutrients required for oocyte maturation, hormonal synthesis, antioxidant defense, and reproductive tissue integrity. Dietary interventions modulate nutrient-sensing pathways including FOXO, mTOR, and AMPK, thereby promoting mitochondrial function, cellular repair, oxidative stress resistance, and preservation of ovarian reserve. Caloric optimization and balanced nutrition improve metabolic signalling and create a favourable endocrine environment for ovulation, fertilization, and implantation. The review further emphasizes that combined lifestyle interventions involving structured exercise, healthy dietary modification, micronutrient optimization, and weight regulation yield superior reproductive outcomes compared with isolated interventions. Such integrated approaches improve insulin sensitivity, reduce hyperandrogenism, normalize menstrual cyclicity, and enhance fertility potential. [56-65,73-78,88,94-96]
Future perspective: from association to precision-based reproductive intervention
The evidence synthesized throughout this review strongly establishes female infertility as a systems-level metabolic–endocrine disorder arising from continuous interactions among genetic susceptibility, endocrine imbalance, metabolic dysfunction, micronutrient deficiency, environmental exposure, and lifestyle behavior. Among the major contributors, PCOS/PMOS emerges as one of the most significant infertility-associated conditions characterized by insulin resistance, hyperandrogenism, chronic inflammation, oxidative stress, mitochondrial dysfunction, and impaired folliculogenesis.[12,18-29,34,35,73-78,83,84,86,87] The interconnected influence of junk food consumption, sedentary lifestyle, gut dysbiosis, and vitamin D deficiency further highlights that reproductive dysfunction cannot be interpreted solely within the boundaries of ovarian pathology, but rather as a multisystem metabolic disorder profoundly shaped by modifiable environmental and nutritional factors. The future of reproductive medicine must therefore advance beyond associative observations toward mechanistically driven, precision-based, and translational frameworks. Large-scale longitudinal and multi-omics studies integrating genomics, epigenomics, metabolomics, transcriptomics, and microbiome profiling are urgently required to decode the complex molecular networks linking lifestyle-associated metabolic dysfunction with infertility progression. Such approaches may facilitate identification of predictive biomarkers for early detection, risk stratification, disease progression, and individualized therapeutic targeting. [12,18-29,34,35,73-78,83,84,86,87]
Future research should particularly prioritize gene–environment and gene–nutrient interaction models involving vitamin D signalling, VDR polymorphisms, insulin resistance pathways, oxidative stress regulators, inflammatory mediators, and nutrient-sensing networks such as AMPK, mTOR, FOXO, and PI3K/Akt pathways. These mechanistic insights will strengthen the development of nutrigenomics-based and lifestyle-oriented precision medicine strategies for infertility and PCOS/PMOS management. Equally important is the need for well-designed randomized controlled trials evaluating integrated lifestyle interventions combining structured physical activity, dietary optimization, micronutrient supplementation, circadian regulation, and behavioural therapy. Considering the marked heterogeneity across metabolic phenotypes, genetic backgrounds, and socio-cultural environments, future reproductive healthcare must increasingly adopt individualized and personalized intervention models rather than uniform therapeutic protocols.[12,18-29,34,35,73-78,83,84,86,87]
Emerging technologies including artificial intelligence-driven predictive analytics, wearable metabolic monitoring systems, and digital reproductive health platforms should also be incorporated into fertility management to enable continuous lifestyle surveillance and real-time therapeutic modulation. From a broader public health perspective, infertility should be recognized as a lifestyle-linked non-communicable disorder requiring preventive policy-level interventions emphasizing nutritional awareness, physical activity, environmental safety, early metabolic screening, and reproductive health education. Such integrative and preventive strategies may substantially reduce the growing global burden of infertility while improving long-term reproductive and metabolic health outcomes in women. [43-51,38-42,52-65,90-96]
CONCLUSION
Female infertility can no longer be viewed through a fragmented lens of isolated endocrine or structural abnormalities; rather, it must be recognized as a systems-level disorder governed by the dynamic interplay of genetic, molecular, metabolic, and lifestyle determinants. The present synthesis unequivocally establishes that sedentary behaviour and unhealthy dietary patterns are not peripheral influences but central drivers of reproductive dysfunction, operating through IR, chronic inflammation, oxidative stress, and endocrine disruption. These pathways converge on critical regulatory axes—including the HPOA, adipokine signalling, and nutrient-sensing networks—ultimately impairing ovulation, oocyte quality, and implantation potential. Importantly, the interaction between intrinsic factors such as chromosomal integrity, gene regulation, and ovarian reserve with extrinsic modulators like physical inactivity and nutrient imbalance defines the phenotypic expression and severity of infertility. Conditions such as PCOS exemplify this convergence, where metabolic dysregulation, micronutrient deficiencies (notably vitamin D), and genetic susceptibility collectively shape reproductive outcomes. Thus, infertility should be redefined not merely as a reproductive disorder but as a metabolic–endocrine continuum influenced by modifiable lifestyle behaviours. This paradigm mandates a decisive shift in both clinical and research approaches—from reactive treatment strategies to preventive, integrative, and systems-based interventions. Lifestyle optimization is not an adjunct but a primary therapeutic axis, capable of restoring physiological equilibrium and enhancing reproductive potential. The evidence presented herein compels clinicians, researchers, and public health systems to reposition lifestyle as a cornerstone in the management and prevention of female infertility.
In essence, the next frontier lies in transforming our understanding of infertility from a condition to be treated into a biological state to be predicted, prevented, and precisely modulated.
REFERENCES

Sanchari Chakraborty, Barnali Ray Basu, Sedentary Lifestyle, Ultra-Processed Diets, and Vitamin D Deficiency – the Epigenetic Drivers of Metabolic–Endocrine and Gut-Dysbiosis in PCOS Associated Female Infertility, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1845-1874, https://doi.org/10.5281/zenodo.20591465
 10.5281/zenodo.20591465
10.5281/zenodo.20591465