
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Assistant Professor, Bharat School of Pharmacy, Mangalpally, Ibrahimpatnam, Ranga Reddy District,Telangana, India
2,4,5Department of Pharmacy Practice, Bharat School of Pharmacy, Mangalpally, Ibrahimpatnam, Ranga Reddy District, Telangana, India.
3Department of Paediatrics, Durgabai Deshmukh Hospital and Research Centre, Vidyanagar, Hyderabad, Telangana, India.
Introduction:Enteric fever remains a major public health concern in developing countries, particularly among children, due to inadequate sanitation and the emergence of antimicrobial resistance. Ceftriaxone is widely used for the treatment of enteric fever; however, combination therapy with azithromycin may provide improved clinical outcomes. This study aimed to evaluate the safety and efficacy of injection ceftriaxone monotherapy versus injection ceftriaxone combined with oral azithromycin dual therapy in paediatric patients with enteric fever. Materials and Methods: A comparative prospective study was conducted in the Department of Paediatrics at Durgabai Deshmukh Hospital and Research Centre over a period of six months. A total of 100 paediatric patients aged 1–15 years diagnosed with enteric fever were included. Patients received either ceftriaxone monotherapy (n=51) or ceftriaxone plus oral azithromycin dual therapy (n=49). Demographic data, clinical symptoms, laboratory investigations, Widal test results, white blood cell counts, and fever trends were collected and analyzed using appropriate statistical methods. A p-value of <0.05 was considered statistically significant. Results and Discussion: Both treatment groups showed improvement in clinical outcomes. No significant differences were observed in gender distribution, chief complaints, baseline temperature, or Widal test positivity. However, the dual therapy group demonstrated significantly faster fever reduction on Day 2 (p=0.001) and Day 3 (p<0.001) compared with the monotherapy group. White blood cell counts were significantly higher in the dual therapy group on Day 3 (p=0.010),indicating better recovery and immune response. Safety profiles were comparable between both treatment regimens, with no significant increase in adverse effects observed in the dual therapy group. Conclusion: Ceftriaxone plus oral azithromycin dual therapy was found to be more effective than ceftriaxone monotherapy in achieving faster fever clearance and improved clinical recovery in paediatric enteric fever patients. The combination regimen may be considered a superior therapeutic option, particularly in areas with increasing antimicrobial resistance.
Enteric fever, comprising typhoid and paratyphoid fever, is a systemic infectious disease caused primarily by Salmonella enterica serovar Typhi and Salmonella enterica serovar Paratyphi. The disease remains a significant public health problem in developing countries, particularly in regions with inadequate sanitation, poor hygiene practices, and limited access to safe drinking water. Children are among the most affected populations, contributing substantially to the global burden of morbidity associated with enteric fever.
Despite advances in healthcare, enteric fever continues to pose therapeutic challenges due to the emergence of multidrug-resistant and extensively drug-resistant strains of Salmonella. Antimicrobial therapy remains the cornerstone of treatment, with ceftriaxone and azithromycin being among the most commonly prescribed antibiotics. Ceftriaxone, a third-generation cephalosporin, has demonstrated good efficacy against susceptible strains and is widely used in hospitalized patients. Azithromycin, a macrolide antibiotic, has also shown effectiveness against enteric fever and offers the advantage of excellent intracellular penetration and activity against resistant organisms.
The increasing prevalence of antimicrobial resistance has raised concerns regarding treatment failures, delayed clinical recovery, and disease relapse. Consequently, combination therapy using ceftriaxone and azithromycin has been proposed as a potential strategy to enhance therapeutic outcomes, achieve faster symptom resolution, and reduce the risk of resistance development. However, evidence comparing the effectiveness and safety of ceftriaxone monotherapy with ceftriaxone plus azithromycin dual therapy in paediatric enteric fever remains limited.
Therefore, the present study was undertaken to evaluate and compare the safety and efficacy of injection ceftriaxone monotherapy versus injection ceftriaxone combined with oral azithromycin dual therapy in paediatric patients with enteric fever. The study hypothesized that dual therapy would provide superior clinical outcomes, including faster fever clearance and improved recovery, while maintaining a comparable safety profile to monotherapy.
MATERIALS AND METHODS STUDY DESIGN
A comparative prospective study was conducted to evaluate the safety and efficacy of Injection Ceftriaxone monotherapy versus Injection Ceftriaxone combined with Oral Azithromycin dual therapy in paediatric patients diagnosed with enteric fever.
STUDY SETTING
The study was carried out in the inpatient and outpatient departments of Paediatrics at Durgabai Deshmukh Hospital and Research Centre, Hyderabad, Telangana, India, a 300-bedded multispecialty teaching hospital.
STUDY DURATION
The study was conducted over a period of six months.
STUDY POPULATION
A total of 100 paediatric patients diagnosed with enteric fever were enrolled in the study. Patients were allocated into two treatment groups based on the prescribed therapeutic regimen:
DRUGS USED IN THE STUDY
Injection ceftriaxone
Generic Name: Ceftriaxone Sodium
Dosage Form: Intravenous/Intramuscular Injection Class: Third-Generation Cephalosporin Antibiotic
Oral Azithromycin
Generic Name: Azithromycin
Dosage Form: Oral Suspension/Tablet Class: Macrolide Antibiotic
INCLUSION CRITERIA
EXCLUSION CRITERIA
DATA COLLECTION
Relevant data were collected from patient case records, laboratory investigation reports, prescriptions, and interviews with patient attendants. Demographic characteristics, clinical symptoms, treatment details, laboratory findings, and treatment outcomes were documented using a structured data collection form.
EFFICACY ASSESSMENT
Treatment efficacy was evaluated based on:
STATISTICAL ANALYSIS
Data were entered into Microsoft Excel and analyzed using appropriate statistical methods. Continuous variables were expressed as mean ± standard deviation, whereas categorical variables were expressed as frequencies and percentages.
The following statistical tests were applied:
ETHICAL CONSIDERATIONS
The study was conducted only after obtaining approval from the Institutional Ethics Committee of Durgabai Deshmukh Hospital and Research Centre. Written informed consent was obtained from the parents or legal guardians of all participating children before inclusion in the study.
Ethics Approval Number: Year of Approval:RESULTS AND DISCUSSION
A total of 100 paediatric patients diagnosed with enteric fever were included in the study. Among them, 51
patients received Injection Ceftriaxone monotherapy and 49 patients received Injection Ceftriaxone combined with Oral Azithromycin dual therapy.
DISCUSSION:
Enteric fever continues to be a major cause of morbidity among paediatric patients in developing countries. Effective antimicrobial therapy is essential to achieve rapid symptom resolution and prevent disease-related complications.
The present study compared the efficacy and safety of Injection Ceftriaxone monotherapy with Injection Ceftriaxone plus Oral Azithromycin dual therapy in paediatric patients with enteric fever.
The findings demonstrated that both treatment regimens were effective; however, dual therapy produced superior clinical outcomes in terms of fever reduction and recovery rate.
The absence of significant differences in gender distribution, chief complaints, baseline temperature, and Widal test positivity suggests that both treatment groups were clinically comparable at the beginning of the study. This strengthens the validity of the treatment outcome comparison.
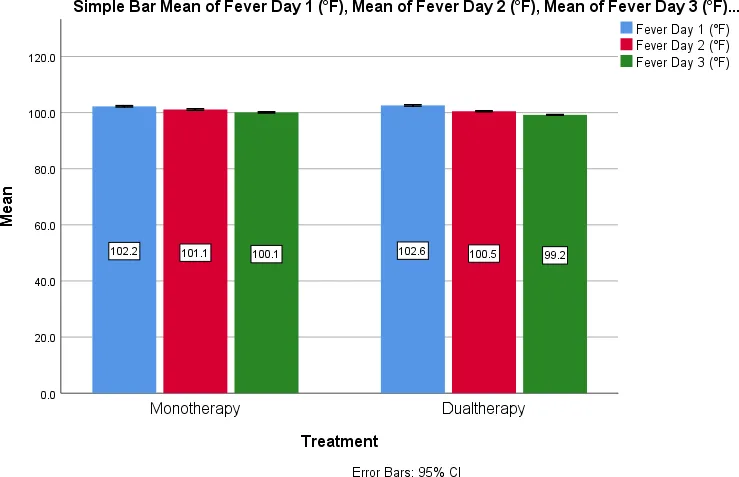
One of the most important observations was the significantly faster reduction in fever among patients receiving dual therapy. By the second and third days of treatment, fever reduction was significantly greater in the dual therapy group. Rapid fever clearance is an important indicator of therapeutic success and patient recovery in enteric fever.
CONCLUSION:
The present comparative prospective study evaluated the safety and efficacy of Injection Ceftriaxone monotherapy versus Injection Ceftriaxone combined with Oral Azithromycin dual therapy in pediatric patients with enteric fever. Both treatment regimens were found to be effective and well tolerated; however, the dual therapy regimen demonstrated superior clinical outcomes.
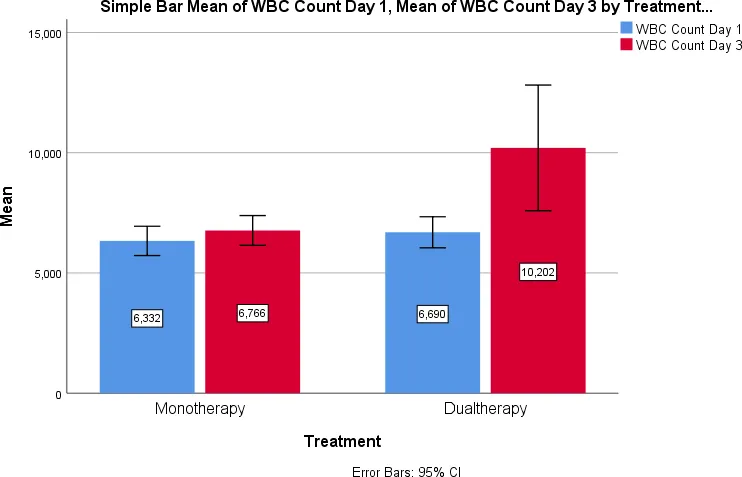
Patients receiving ceftriaxone plus azithromycin showed faster fever clearance and better clinical recovery compared with those receiving ceftriaxone monotherapy. The dual therapy group also exhibited significant improvement in white blood cell counts during treatment, indicating enhanced therapeutic response. Furthermore, the addition of azithromycin did not result in any significant increase in adverse effects, confirming the safety of the combination regimen.
The findings of this study suggest that ceftriaxone plus azithromycin dual therapy may be a more effective treatment strategy for pediatric enteric fever, particularly in regions where antimicrobial resistance is increasing. Although ceftriaxone monotherapy remains a useful therapeutic option, combination therapy appears to offer improved clinical benefits, reduced risk of treatment failure, and faster recovery.
Therefore, ceftriaxone combined with azithromycin can be considered a preferred therapeutic approach for the management of enteric fever in children, especially in patients at higher risk of resistant infections. Further multicenter studies with larger sample sizes are recommended to validate these findings and strengthen clinical treatment guidelines.
ACKNOWLEDGEMENT:
The authors express their sincere gratitude to the Department of Paediatrics, Durgabai Deshmukh Hospital and Research Centre, Hyderabad, for providing the necessary facilities and support to conduct this study. The authors are thankful to the physicians, nursing staff, hospital administration, and all study participants and their parents/guardians for their cooperation throughout the study period.
The authors also acknowledge the guidance and support provided by the faculty members of the Department of Pharmacy Practice in the successful completion of this research work.
CONFLICT OF INTEREST
The authors have no conflicts of interest regarding this investigation.
TABLES
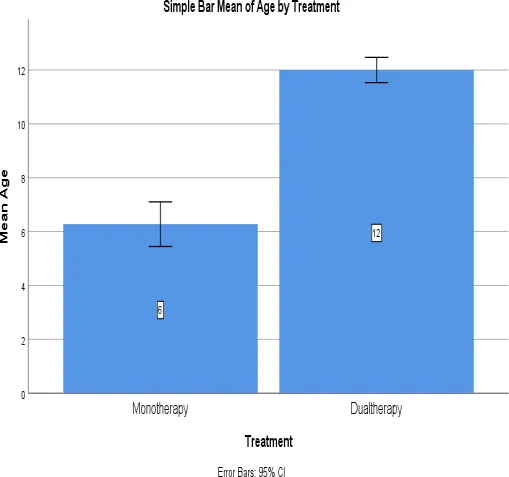
TABLE-1: Effectiveness of mono therapy verses dual therapy across different age groups
|
Age |
Treatment |
Mean |
Std. Deviation |
P value |
|
1-10 |
Monotherapy |
6.27 |
2.947 |
<0.001 |
|
11-15 |
Dual therapy |
12.00 |
1.633 |
The table and bar graph shows that comparision of treatment effects between two Age groups [1-10] years and [11-15] years
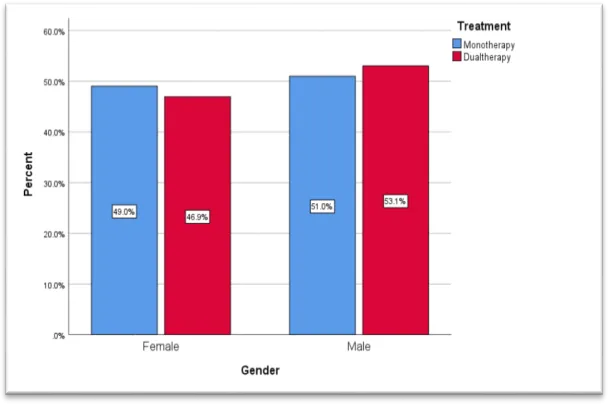
TABLE-2: Gender Distribution in Monotherapy and Dual Therapy Groups
|
Gender |
Treatment |
Total |
P value |
|
|
Monotherapy No. (%) |
Dual therapy No. (%) |
|||
|
Female |
25 (49) |
23 (46.9) |
48 |
0.835 |
|
Male |
26 (51) |
26 (53.1) |
52 |
|
|
Total |
51 |
49 |
100 |
|
The table and bar chart presents a monotherapy and dual therapy treatment distribution based on gender
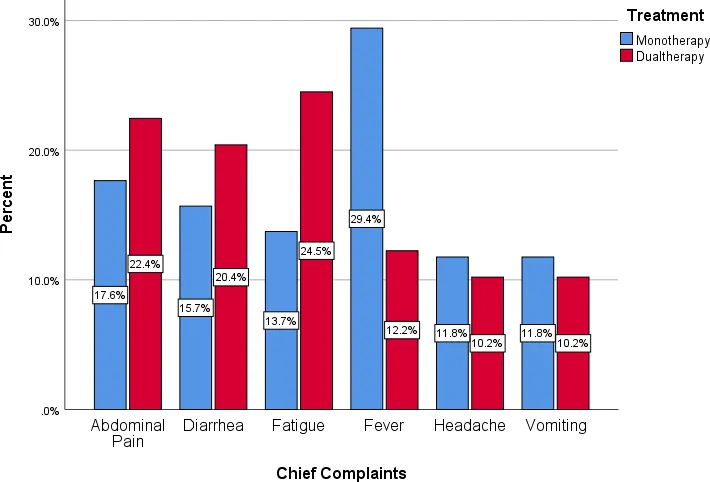
TABLE-3: Comparison of Chief Complaints Between Monotherapy and Dual Therapy Groups
|
Chief complaints |
Treatment |
Total |
P value |
|
|
Monotherapy No. (%) |
Dual therapy No. (%) |
|||
|
Abdominal pain |
9 (17.6) |
11 (22.4) |
20 |
0.332 |
|
Diarrhea |
8 (15.7) |
10 (20.4) |
18 |
|
|
Fatigue |
7 (13.7) |
12 (24.5) |
19 |
|
|
Fever |
15 (29.4) |
6 (12.2) |
21 |
|
|
Headache |
6 (11.8) |
5 (10.2) |
11 |
|
|
Vomiting |
6 (11.8) |
5 (10.2) |
11 |
|
|
Total |
51 |
49 |
100 |
|
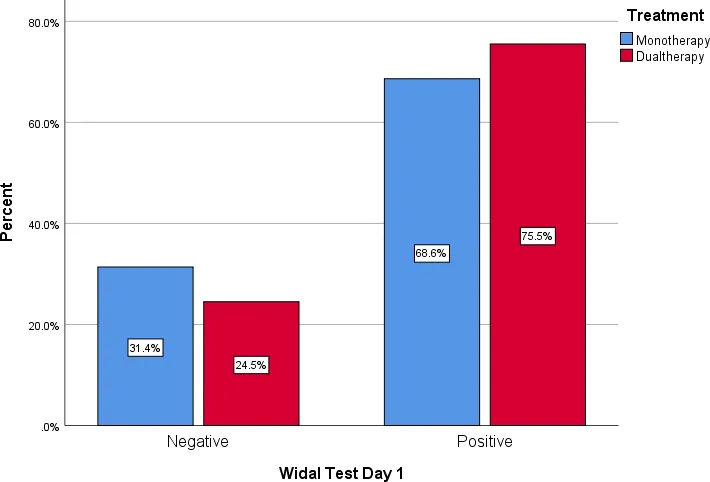
TABLE-4 :Comparison of Widal Test Results Between Monotherapy and Dual Therapy Groups
|
Widal test |
Treatment |
Total |
P value |
|
|
|
||||
|
Monotherapy No. (%) |
Dual therapy No. (%) |
|||
|
Negative |
16 (31.4) |
12 (24.5) |
28 |
0.443 |
|
Positive |
35 (68.8) |
37 (75.5) |
72 |
|
|
Total |
51 |
49 |
100 |
|
|
|
Treatment |
Mean |
Std. Deviation |
P value |
|
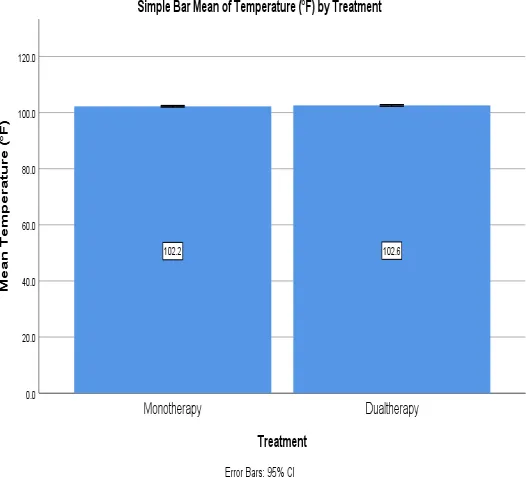
Fever Day 1 (°F) |
Monotherapy |
102.247 |
.9754 |
0.100 |
|
Dualtherapy |
102.569 |
.9633 |
||
|
Fever Day 2 (°F) |
Monotherapy |
101.122 |
1.0323 |
0.001 |
|
Dualtherapy |
100.498 |
.7273 |
||
|
Fever Day 3 (°F) |
Monotherapy |
100.090 |
.8750 |
<0.001 |
|
|
Dualtherapy |
99.218 |
.5696 |
The table and bar graph present data on fever (in °F) for two treatment groups—Monotherapy and Dualtherapy-over three days. The first day fever temperatures in the groups treated with monotherapy and combination treatment were 102.247°F and 102.569°F, respectively, with a standard deviation of 0.9754 and 0.9633, respectively.
With a p-value of 0.100, the first day fever levels did not differ significantly between the two regimens. This suggests that at the beginning of treatment, both approaches had a similar impact on body temperature.
On Day 2, the mean fever temperature decreased in both groups.The monotherapy group had a mean temperature of 101.122°F (Standard deviation : 1.0323), while the dual therapy group had a lower mean temperature of 100.498°F (Standard deviation: 0.7273). The p-value was 0.001, indicating a statistically significant difference. This suggests that by the second day, dual therapy was more effective in reducing fever compared to monotherapy.
ABBREVIATIONS:
|
EF |
Enteric Fever |
|
S |
Salmonella |
|
NTS |
Non typhoidal salmonella |
|
iNTS |
Invasive non typhoidal serovars |
|
CBC |
Complete blood count |
|
IV |
Intravenous |
|
IP NO |
In -patient number |
|
OP NO |
Out –patient number |
|
DOA |
Date of admission |
|
DOD |
Date of discharge |
REFERENCES





Swathi Boddupally*, Goreti Shivani, DR.Gangadhara Rao, Jetram Omprakash Reddy, Jakkula Vagdevi, To Study The Safety And Efficacy Of Injection Ceftriaxone Monotherapy Versus Injection Ceftriaxone Plus Oral Azithromycin Dual Therapy In Enteric Fever, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 3214-3224. https://doi.org/ 10.5281/zenodo.21390541
 10.5281/zenodo.21390541
10.5281/zenodo.21390541