
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Institute of Chemical Technology, Mumbai, Indian Oil Odisha Campus, Bhubaneswar
2 GES'S Sir Dr. M. S. Gosavi College of Pharmaceutical Education and Research, Nashik
3 Birla Institute of Technology and Science, Pilani, Hyderabad Campus, India
Transdermal Drug Delivery Systems (TDDS) have emerged as a promising, non-invasive platform for achieving controlled and sustained release of therapeutics through the skin. They bypass hepatic first-pass metabolism, improve patient compliance, and allow for precise modulation of plasma drug levels. This review comprehensively discusses the design, mechanisms, evaluation, and recent advances in TDDS. Starting from an overview of conventional drug delivery challenges and the evolution of transdermal patches, the article explores the anatomical and physiological aspects of the skin relevant to drug permeation, as well as the principles governing transdermal transport. Emphasis is placed on the ideal drug characteristics, types of patches, formulation components, and manufacturing methodologies used to optimise therapeutic outcomes. Furthermore, detailed insights into evaluation parameters, including physicochemical, in vitro, and in vivo assessments, ensure the quality, safety, and efficacy of the systems. The review also highlights recent technological innovations such as nanocarriers, microneedle-assisted systems, iontophoretic devices, hydrogel-based smart polymers, and 3D-printed personalised patches, which are redefining the landscape of transdermal therapy. Marketed products and futuristic perspectives are discussed to demonstrate the translational potential of TDDS in modern pharmacotherapy. The integration of nanotechnology, artificial intelligence, and bio-responsive materials marks the advent of intelligent transdermal systems capable of real-time, patient-specific drug delivery, heralding a new era in personalised medicine.
Overview of Drug Delivery Systems
Drug delivery systems are specialised technologies designed to transport therapeutic compounds in the body to achieve desired pharmacological outcomes while minimising side effects. Traditional oral and parenteral routes have long been dominant; however, they often suffer from limitations such as first-pass metabolism, variable bioavailability, and patient non-compliance. Modern pharmaceutical science has therefore focused on novel delivery systems, including controlled-release, targeted, and transdermal drug delivery to improve therapeutic efficacy and convenience. These systems aim to optimise drug concentration at the target site and maintain it for a sustained period, thereby enhancing patient adherence and clinical outcomes [1].
Need for Transdermal Drug Delivery
The transdermal route offers a promising alternative to conventional methods by enabling systemic delivery of drugs through the skin. This non-invasive approach bypasses hepatic first-pass metabolism, reduces gastrointestinal irritation, and provides sustained drug release. Moreover, it enhances patient compliance by eliminating the need for frequent dosing or painful injections. Transdermal systems are particularly valuable for drugs requiring steady plasma concentrations, such as hormones, cardiovascular agents, and analgesics. Furthermore, transdermal delivery minimises systemic toxicity and allows for easy termination of therapy by removing the patch, providing an additional safety advantage [2].
Historical Development of Transdermal Patches
The concept of delivering drugs through the skin dates back centuries, with early formulations including medicated ointments and plasters. However, the modern era of transdermal delivery began in the late 20th century. The first FDA-approved transdermal product, Transderm-Scop, released in 1979, delivered scopolamine for motion sickness prevention [3]. This milestone paved the way for subsequent innovations such as Nitro-Dur (nitroglycerine patch) for angina pectoris, Catapres-TTS (clonidine patch) for hypertension, and Nicoderm CQ (nicotine patch) for smoking cessation. Over the decades, the technology evolved from simple monolithic designs to sophisticated multilayered and iontophoretic systems, capable of controlled and enhanced drug permeation [4].
Marketed Transdermal Products
Today, the global market for transdermal patches exceeds several billion dollars, reflecting their widespread clinical acceptance. Notable examples include Fentanyl patches for chronic pain management, Estraderm for hormone replacement therapy, Lidoderm for localised analgesia, and Rivastigmine patches for Alzheimer’s disease [5]. Recent innovations have introduced microneedle-assisted patches, such as Zosano’s Qtrypta for migraine treatment, and wearable smart patches capable of feedback-controlled drug release. These advancements signal a transformative shift toward patient-centric, intelligent transdermal systems that combine convenience, safety, and precision dosing [6, 7].
In summary, transdermal drug delivery systems (TDDS) represent a critical advancement in pharmaceutical technology, bridging the gap between efficacy and patient comfort while paving the way for personalised medicine and digital therapeutics.
Structure of Skin
The skin, the body’s largest organ, serves as the primary interface between the internal environment and the external world. It covers an area of approximately 1.5-2.0 m² in adults and accounts for nearly 15% of total body weight [8]. Structurally, the skin is composed of three major layers - the epidermis, dermis, and hypodermis, each playing distinct roles in protection, sensation, and thermoregulation. Its multi-layered nature makes it both an effective barrier and a potential route for drug administration, depending on how the barrier is manipulated or bypassed. The skin’s outermost layer, the stratum corneum, is primarily responsible for restricting the penetration of exogenous substances, which poses a significant challenge for transdermal drug delivery [9].
Epidermis
The epidermis is the thin, avascular outer layer of the skin that primarily consists of keratinocytes arranged in several sublayers. The basal layer, stratum basale, contains proliferative cells that migrate upwards to form the stratum corneum through keratinisation. The total thickness of the epidermis ranges from 50 to 150 μm, depending on the body site [10]. While it lacks blood vessels, it is essential for maintaining skin integrity and acts as the primary site for drug diffusion in transdermal delivery. The intercellular lipid matrix and keratinised cells of the epidermis together regulate the partitioning and permeability of drug molecules [11].
Dermis
Beneath the epidermis lies the dermis, a dense connective tissue layer rich in collagen fibres, blood vessels, lymphatics, and nerve endings. It is about 2-3 mm thick and provides mechanical strength and elasticity to the skin. For transdermal delivery, once the drug permeates the stratum corneum and viable epidermis, it diffuses into the dermis, where it can be absorbed into systemic circulation via the capillary networks. The dermis thus serves as a reservoir and a conduit for systemic drug transport, making its microvascular density a critical determinant of transdermal absorption efficiency [12].
Hypodermis
The hypodermis (subcutaneous tissue) is primarily composed of adipose tissue and loose connective tissue. It cushions underlying structures, stores energy, and helps regulate body temperature. Although it does not play a direct role in permeability, its vascularisation can influence systemic uptake of drugs that have penetrated deeper skin layers [13]. Additionally, the hypodermis serves as an important depot for lipophilic drugs, allowing for sustained release from transdermal formulations.
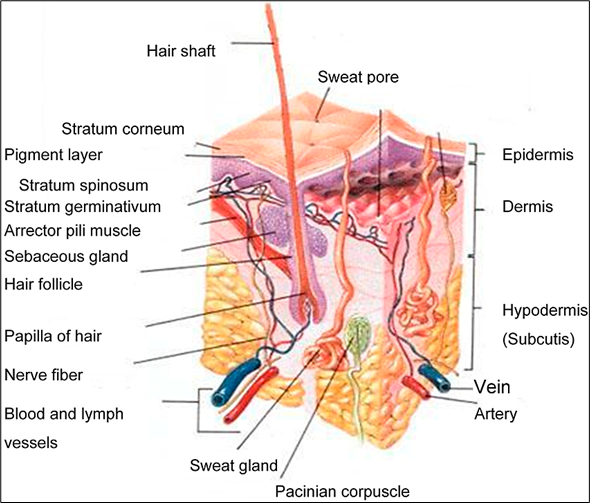
Figure 1. Schematic cross-section of human skin showing pathways for transdermal transport.
Role of Stratum Corneum as a Barrier
The stratum corneum (SC) is the principal barrier to transdermal drug permeation. It consists of flattened, anucleated keratinocytes (corneocytes) embedded in a lipid matrix, a structure often described by the “brick and mortar” model. Despite being only 10-20 μm thick, the SC presents formidable resistance due to its densely packed keratin and lipids [14]. The permeability of this layer depends on lipid composition, hydration, and the presence of penetration enhancers. Overcoming or temporarily disrupting the SC barrier through methods such as iontophoresis, microneedles, or chemical enhancers is a major focus of transdermal research [15].
Factors Affecting Skin Permeability
Several physiological and physicochemical factors govern drug permeation through the skin. Key determinants include skin hydration, age, body site, skin temperature, and disease state. Hydrated skin exhibits higher permeability due to lipid disordering, whereas thick or keratinised regions (e.g., palms, soles) show reduced penetration. Drug-related properties such as molecular weight (<500 Da), lipophilicity (log P between 1-3), and dose concentration also influence diffusion rates. Furthermore, the presence of chemical enhancers like ethanol or surfactants can increase permeability by altering lipid fluidity or protein conformation within the SC [16]. Understanding and optimising these factors is essential in designing efficient transdermal systems capable of achieving therapeutic plasma concentrations without compromising skin integrity.
Transdermal drug delivery operates on the fundamental principle of allowing therapeutic molecules to traverse the skin barrier in a controlled manner to reach systemic circulation. The process is governed by the physicochemical properties of the drug, the anatomy of the skin, and the design of the delivery system. Successful permeation requires that the drug not only penetrate the stratum corneum but also diffuse through the viable epidermis and dermis without significant degradation or loss of activity [17].
Mechanism of Drug Permeation
Drug transport through the skin primarily occurs via passive diffusion, following Fick’s first law, which states that the rate of diffusion is directly proportional to the concentration gradient across the membrane [18]. Accordingly, the steady-state flux (J) is expressed as:
J=D⋅K⋅ΔCh
Where D is the diffusion coefficient of the drug in the skin, K is the partition coefficient between the skin and the vehicle, ΔC is the concentration difference across the membrane, and h is the membrane thickness.
Three principal routes of transdermal permeation have been identified:
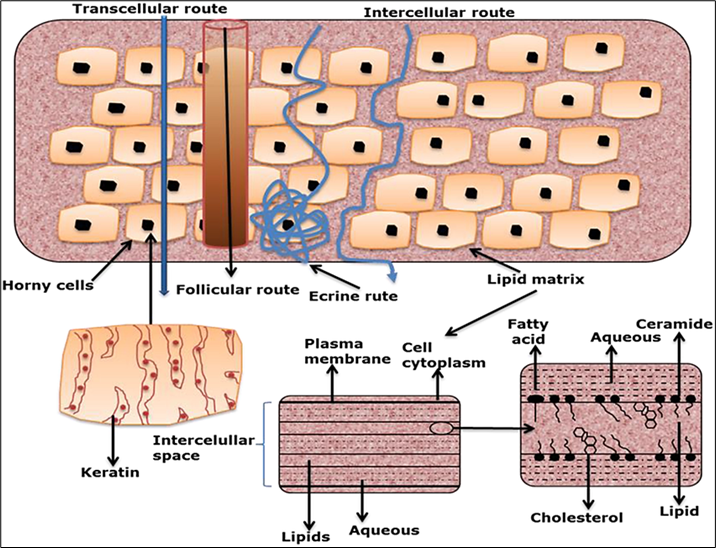
Figure 2. Transcellular and intercellular routes of drug delivery via the skin
Among these, the intercellular route is the most dominant for most small, lipophilic molecules. The overall permeation rate depends on the balance between lipophilicity and hydrophilicity of the drug, as extremely lipophilic drugs tend to remain within the stratum corneum, while highly hydrophilic drugs struggle to partition into it [20].
Kinetics of Transdermal Absorption
Transdermal absorption typically follows a lag phase, during which the drug accumulates in the stratum corneum before reaching a steady-state flux. The steady-state condition is achieved when the rate of drug input through the skin equals the rate of clearance into systemic circulation. Factors such as temperature, hydration, and vehicle composition can significantly affect both the lag time and steady-state flux. Moreover, advanced systems can modulate these kinetics through controlled-release matrices or permeation enhancers, allowing for constant plasma levels over extended durations [21].
Enhancement Strategies
Since the stratum corneum poses significant resistance to drug transport, enhancement techniques are crucial for improving transdermal delivery efficiency. These include chemical enhancers (e.g., ethanol, surfactants, terpenes), physical methods (e.g., iontophoresis, sonophoresis, microneedles), and novel carrier systems (e.g., liposomes, niosomes, and transferosomes). Physical enhancement techniques temporarily disrupt the skin barrier or use external energy to facilitate drug penetration, whereas vesicular carriers improve drug solubilization and diffusion across lipid domains [22].
Emerging hybrid methods that combine chemical and physical enhancement are gaining prominence, as they achieve synergistic effects while maintaining skin safety and reversibility [23]. Overall, the principles of transdermal delivery revolve around understanding the interplay between skin physiology, drug physicochemical properties, and the design of delivery systems to achieve efficient, controlled, and patient-friendly drug administration [24].
For a drug to be effectively delivered through the transdermal route, it must possess specific physicochemical and pharmacokinetic properties that allow it to penetrate the skin barrier and maintain therapeutic plasma concentrations. The ideal candidate for transdermal delivery should be potent, stable, and compatible with both the skin and the components of the patch system [25]. These characteristics ensure optimal absorption, sustained release, and minimal irritation or degradation during administration.
Physicochemical Characteristics
The success of transdermal drug delivery largely depends on a drug’s molecular size, lipophilicity, solubility, and melting point. Drugs with a molecular weight below 500 Da have the best potential for passive skin permeation, as larger molecules face difficulty crossing the stratum corneum. An ideal drug should exhibit a balanced partition coefficient (log P) between 1 and 3, which ensures sufficient solubility in both the lipidic and aqueous layers of the skin [26]. Drugs that are too hydrophilic fail to partition into the stratum corneum, while those too lipophilic may remain trapped within it, preventing systemic absorption.
A melting point below 200°C is preferred because higher melting points generally correspond to lower solubility and reduced diffusion through the skin [27]. The drug should also have a moderate dose requirement (typically less than 10 mg per day), as high-dose drugs may necessitate unreasonably large patch sizes to deliver the required amount.
Pharmacokinetic and Pharmacodynamic Requirements
From a pharmacokinetic perspective, an ideal transdermal drug should have a short biological half-life and require sustained plasma concentrations to maintain therapeutic efficacy. Drugs that undergo extensive first-pass hepatic metabolism, such as nitroglycerine, clonidine, and oestradiol, are excellent candidates because transdermal administration circumvents hepatic degradation, enhancing systemic bioavailability [28]. Additionally, the drug should exhibit a low therapeutic plasma concentration (typically in the nanogram to microgram per millilitre range), as this ensures that a small, continuous flux through the skin can maintain efficacy.
Pharmacodynamically, drugs suitable for transdermal delivery should have predictable dose-response relationships and minimal local irritation potential. They should not cause sensitisation, erythema, or allergic reactions upon prolonged contact with the skin. The therapeutic effect should also persist even after patch removal, allowing for smoother plasma concentration decline without abrupt withdrawal effects [29].
Table 1. Criteria for Drug Selection in Transdermal Delivery
|
Parameter |
Ideal Range/ Characteristic |
Significance |
Example Drugs |
|
Molecular weight |
< 500 Da |
Smaller molecules diffuse easily through the stratum corneum |
Nitroglycerin, Fentanyl |
|
Partition coefficient (log P) |
1 – 3 |
Ensures adequate lipophilic–hydrophilic balance for permeation |
Clonidine, Oestradiol |
|
Aqueous solubility |
≥ 1 mg/mL |
Allows sufficient dissolution in skin fluids for diffusion |
Nicotine, Rivastigmine |
|
Melting point |
< 200°C |
Lower melting point improves solubility and diffusivity |
Buprenorphine, Testosterone |
|
Dose requirement |
≤ 10 mg/day |
Permits delivery of therapeutic dose via limited patch area |
Scopolamine, Clonidine |
|
Half-life (t½) |
Short (2–8 h) |
Enables sustained plasma levels through controlled release |
Fentanyl, Nitroglycerin |
|
Therapeutic index |
Wide |
Reduces risk of toxicity during prolonged exposure |
Oestradiol, Nicotine |
|
First-pass metabolism |
Extensive |
Enhances systemic bioavailability through skin bypass |
Nitroglycerin, Oestradiol |
|
Skin irritation potential |
Minimal |
Ensures patient comfort and compliance |
Clonidine, Buprenorphine |
Examples of Drugs Suitable for Transdermal Delivery
Several drugs meet these criteria and have been successfully formulated into transdermal systems. Nitro-glycerine (anti-anginal), clonidine (antihypertensive), fentanyl (opioid analgesic), oestradiol (hormone therapy), and nicotine (smoking cessation aid) are classic examples. Others, such as rivastigmine for Alzheimer’s disease and buprenorphine for pain management, have also shown high transdermal efficiency due to their appropriate lipophilic-hydrophilic balance and potency.
Furthermore, newer bioactive molecules like donepezil and insulin analogues are being explored using microneedle and iontophoretic patches to overcome molecular size limitations. This growing range of successful candidates underlines the importance of rational drug selection guided by both molecular design and skin permeability science.
In essence, drugs that are potent, stable, moderately lipophilic, and have low dose requirements are best suited for transdermal delivery. The continued evolution of formulation technologies, such as chemical enhancers, vesicular carriers, and microarray systems, promises to expand the range of drugs that can be effectively delivered through the skin [30, 31].
Transdermal patches are classified based on their structural design, mechanism of drug release, and technological sophistication. Each type is engineered to control the rate and extent of drug delivery through the skin, ensuring consistent therapeutic levels. Over time, advancements in materials science and polymer technology have led to the development of various patch systems tailored to different drugs and patient needs [32].
The reservoir-type patch is one of the earliest and most widely used designs. It consists of a drug reservoir enclosed between an occlusive backing layer and a semipermeable membrane that regulates the rate of drug diffusion. The membrane maintains a constant drug release rate, typically following zero-order kinetics, ensuring a steady plasma concentration over time. A rate-controlling membrane separates the drug solution or gel from the adhesive layer that contacts the skin. This design is used in marketed products such as Transderm-Nitro (nitroglycerin) and Catapres-TTS (clonidine) patches [33]. However, manufacturing complexity and the potential risk of dose dumping if the membrane fails are notable limitations.
In matrix-type patches, the drug is uniformly dispersed within a polymer matrix that serves both as a carrier and a rate-controlling medium. Drug release occurs by diffusion through the polymer, typically following first-order kinetics, where the release rate decreases with time as the concentration gradient diminishes [34]. This design simplifies manufacturing and enhances patch flexibility. Examples include Nitro-Dur (nitroglycerin) and Estraderm MX (oestradiol) patches. The simplicity and stability of this system have made it one of the most popular forms for modern transdermal products [35].
The drug-in-adhesive patch incorporates the drug directly into the adhesive layer that contacts the skin, eliminating the need for a separate reservoir or matrix layer. This configuration allows for close contact with the skin, improving adhesion and patient comfort. Drug release occurs through diffusion from the adhesive into the skin, and release rates can be modulated by varying adhesive composition and drug loading [36]. Examples include Nicoderm CQ (nicotine) and Daytrana (methylphenidate) patches. The simplicity, flexibility, and cost-effectiveness of this design make it particularly suitable for drugs requiring moderate dosing and extended wear time [37].
These systems combine features of both matrix and reservoir designs by incorporating multiple layers with distinct functional roles, typically one or more drug-containing layers and separate rate-controlling membranes. This configuration allows for biphasic release profiles, such as an initial burst followed by sustained delivery [38]. The Lidoderm (lidocaine) patch, for instance, provides rapid onset analgesia followed by prolonged relief. Such designs are valuable for conditions requiring quick symptom management followed by maintenance dosing.
Certain modern patches deliver volatile or ionic drugs, such as nicotine vapours or ionised molecules. Vapour patches, like Nicotrol, deliver nicotine through controlled volatilisation, while ion-exchange systems use charged polymers to regulate release through reversible ionic interactions [39]. These technologies enhance stability and precision for drugs with complex release kinetics.
The micro-reservoir system integrates features of reservoir and matrix types, where the drug is suspended in microscopic polymer reservoirs distributed within an adhesive matrix. This design offers both controlled and sustained release characteristics and improved physical stability [40]. The polymeric network encapsulates microdroplets of drug solution, allowing for smooth diffusion and minimal leakage risk. Such patches are being explored for high-potency drugs like opioids and hormonal agents.
Recent developments have introduced smart transdermal systems equipped with microelectronics, sensors, or microneedles that actively enhance drug transport. Microneedle patches create microchannels in the stratum corneum, enabling efficient delivery of large or hydrophilic molecules such as insulin and vaccines. “Smart patches” integrate sensors that monitor physiological parameters (e.g., glucose levels) and adjust release rates accordingly, marking a step toward personalised medicine [41]. Products such as Zosano’s Qtrypta (zolmitriptan microneedle patch) exemplify the clinical transition of these advanced systems.
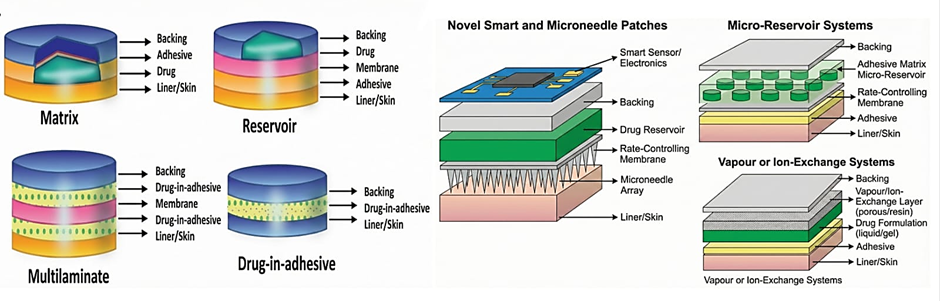
Figure 3. Illustrations of common transdermal patch designs
A transdermal patch is a sophisticated, multi-layered drug delivery device designed to deliver therapeutic agents through the skin at a controlled rate. Each layer plays a specific functional role to ensure efficacy, safety, and patient comfort. The proper selection of materials and their compatibility with both the drug and skin are vital for optimal patch performance [42]. The general structure of a transdermal patch comprises five essential components: backing layer, drug reservoir or matrix, rate-controlling membrane (if present), adhesive layer, and release liner.
The backing layer forms the outermost surface of the patch and provides mechanical support and protection from the external environment. It prevents drug loss, protects the system from moisture and oxygen, and ensures structural integrity throughout the wear period. Ideal backing materials should be impermeable, flexible, and non-reactive with the drug and excipients. Common materials include polyethene (PE), polyvinyl chloride (PVC), polyethene terephthalate (PET), and aluminised films [43]. For example, the Nitro-Dur patch uses a polyester film as a backing material due to its durability and low permeability to gases.
The drug reservoir or matrix is the core of the transdermal system and determines the release kinetics.
Commonly used polymers include ethylene-vinyl acetate (EVA), polyisobutylene (PIB), hydroxypropyl methylcellulose (HPMC), and polyvinylpyrrolidone (PVP). These polymers provide flexibility, stability, and controlled release. For enhanced solubility and stability, plasticisers (e.g., dibutyl phthalate) or stabilisers (e.g., BHT) are sometimes incorporated [45].
The rate-controlling membrane, typically present in reservoir systems, regulates the drug’s release rate and ensures a steady diffusion profile. This membrane maintains zero-order kinetics, preventing sudden increases in drug flux that could cause toxicity. Materials used for this purpose include EVA copolymers, polyurethane, and silicone membranes. The membrane’s permeability is determined by polymer composition, thickness, and plasticiser content [46]. For instance, Catapres-TTS employs an EVA membrane to control clonidine release over seven days.
The adhesive layer serves the dual function of affixing the patch to the skin and facilitating drug transport. In drug-in-adhesive systems, it also acts as the carrier matrix. Therefore, the adhesive must possess excellent biocompatibility, strong adhesion, and easy removability without residue. Common types include acrylic, silicone, and polyisobutylene adhesives. Acrylic adhesives offer strong adhesion and drug compatibility, whereas silicone adhesives provide superior flexibility and are preferred for sensitive skin [47]. The choice of adhesive also affects the rate of drug diffusion, as some adhesives can act as semi-permeable membranes controlling drug flux.
The release liner is a temporary protective layer that covers the adhesive surface before application. It prevents contamination and preserves drug integrity during storage. The liner is typically coated with fluoropolymer (Teflon), siliconized polyester, or polyethene-coated paper to ensure easy removal without disrupting the adhesive or drug layer [48]. Since the release liner is removed before application, it must be chemically inert and should not absorb or react with the drug.
To overcome the formidable barrier of the stratum corneum, penetration enhancers are incorporated into the patch. These substances temporarily increase skin permeability by disrupting lipid structure or protein conformation. Common examples include ethanol, oleic acid, propylene glycol, dimethyl sulfoxide (DMSO), and terpenes [49]. Other functional additives such as plasticisers, antioxidants, and stabilisers are included to enhance mechanical strength, prevent oxidation, and ensure formulation stability.
Table 2. Key Components of TDDS.
|
Component |
Primary Function |
Common Materials Used |
|
Backing Layer |
Protects the patch, prevents drug loss |
PET, PVC, PE, Al-foil |
|
Drug Reservoir/Matrix |
Stores and controls drug release |
EVA, PVP, HPMC, PIB |
|
Rate-Controlling Membrane |
Maintains steady-state release |
EVA, polyurethane, silicone |
|
Adhesive Layer |
Ensures skin contact; may contain a drug |
Acrylic, silicone, PIB adhesives |
|
Release Liner |
Protects the adhesive before use |
Fluoropolymer or siliconized paper |
|
Penetration Enhancers |
Enhance skin permeability |
Ethanol, oleic acid, DMSO |
In essence, the success of a transdermal system depends not only on the drug but also on the harmonious interaction between its components. Each layer must be engineered for stability, compatibility, comfort, and controlled release. Modern patch formulations increasingly use biocompatible polymers and smart adhesives to improve wearability, flexibility, and therapeutic reliability, reflecting the growing trend toward patient-friendly drug delivery designs [50].
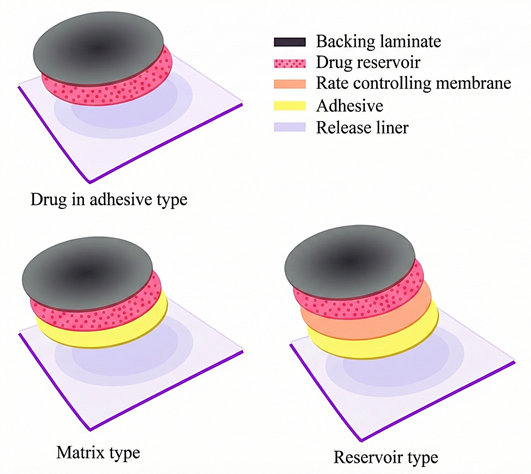
Figure 4. Layered structure of a varies transdermal patches
The preparation of transdermal patches requires careful design to achieve consistent drug content, uniform thickness, mechanical integrity, and controlled release characteristics. Several techniques are used depending on the type of patch (matrix, reservoir, or drug-in-adhesive) and the physicochemical nature of the drug. The process generally involves selecting suitable polymers, solvents, and additives, followed by film casting, drying, lamination, and cutting into desired sizes [51]. Below are the commonly employed methods for formulating transdermal systems.
The solvent evaporation method is the most widely used technique for preparing matrix-type and drug-in-adhesive patches.
In this process, the polymer is dissolved in a volatile organic solvent such as chloroform, methanol, or ethanol. The drug and excipients (plasticisers, permeation enhancers, stabilisers) are then incorporated and mixed thoroughly to form a homogeneous solution. The mixture is poured onto a flat, levelled surface (usually a glass plate or mercury surface) and allowed to dry at room temperature or under controlled conditions to evaporate the solvent.
The dried film is then peeled off, cut into uniform patches, and laminated with a backing layer. This method is simple and cost-effective but requires careful control to prevent solvent residues and ensure uniform drug distribution. For example, Nitro-Dur (nitroglycerine) patches are typically prepared using this approach [52].
In the melt extrusion method, polymers and drugs are blended and melted together, eliminating the need for organic solvents. The molten mixture is then passed through an extruder or rollers to form a thin, uniform film that solidifies upon cooling. This solvent-free method minimises toxicity risks and enhances reproducibility, making it suitable for large-scale manufacturing.
Thermoplastic polymers such as ethylene-vinyl acetate (EVA), polyethene, and polycaprolactone are commonly used. The process allows precise control over thickness and drug loading but is limited to thermostable drugs that can withstand elevated temperatures without degradation [53].
This technique is primarily employed for drug-in-adhesive systems, where the drug is directly blended with an adhesive polymer such as acrylic or silicone to form a uniform mixture. The mixture is spread evenly onto a release liner and dried to remove any residual solvent or air bubbles. The backing layer is then laminated, and the patch is cut to the desired size.
The main advantage of this method is its simplicity and ability to maintain strong adhesion between the patch and skin. However, uniform dispersion of the drug in the adhesive matrix is critical to prevent dosing variability [54].
Recent innovations have introduced electrospinning technology for creating ultrafine nanofiber mats used in next-generation patches. In this method, a polymer-drug solution is subjected to a high-voltage electric field, producing nanoscale fibres that are collected on a backing substrate. These nanofiber patches offer large surface areas, high drug loading, and tunable release rates, making them suitable for both systemic and localised delivery. Electrospun patches of lidocaine, ketoprofen, and insulin have shown superior permeability compared to traditional systems [55].
For advanced patches, microfabrication techniques such as moulding, photolithography, or 3D printing are used to integrate microneedles or microchannels into the patch matrix. These structures enhance permeability by transiently breaching the stratum corneum barrier.
Such fabrication methods allow precise control over microneedle geometry, drug loading, and release kinetics, enabling delivery of macromolecules like peptides, proteins, and vaccines. Products such as Zosano’s Qtrypta employ this hybrid fabrication approach [56].
Other emerging methods include:
These advanced methods enhance control over drug distribution, reduce manufacturing waste, and open possibilities for patient-specific patch designs.
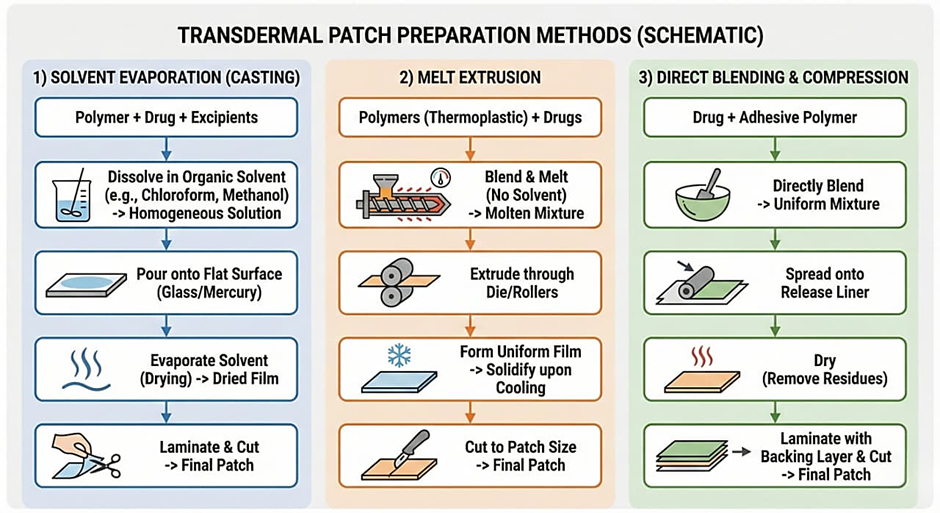
Figure 5. Methods of Preparation of Transdermal Patches
Evaluation of transdermal patches is a critical step in ensuring that the final product exhibits desired mechanical strength, drug release performance, adhesion properties, permeation efficiency, and stability.
The preliminary evaluation of transdermal patches encompasses assessment of physical appearance, thickness uniformity, weight variation, drug content uniformity, and moisture characteristics, as these parameters directly affect performance and reliability. The colour, clarity, smoothness, and flexibility of the patch surface are visually inspected, while thickness is measured at multiple points using a digital micrometre to ensure even distribution and predictable drug diffusion. Weight variation is determined by recording the individual weights of standardized patch sections, and drug content uniformity is analysed using UV spectrophotometry, HPLC, or LC-MS, ensuring content variation within ±5% of the mean for consistent therapeutic output. The moisture content and uptake, assessed via desiccation and controlled humidity exposure, provide insights into the patch’s flexibility, stability, and microbial safety, where excess moisture can lead to contamination or adhesive failure, and too little can cause brittleness [58].
This test measures the mechanical flexibility and durability of patches. The patch is repeatedly folded at the same point until it breaks, and the number of folds required is recorded as the folding endurance. A high folding endurance indicates good mechanical strength and flexibility, properties essential for patient comfort during application.
Using a texture analyser or universal testing machine, the tensile strength and per cent elongation at break are measured. These parameters reflect the mechanical resistance of the patch under stress during handling and application. The ideal patch should possess sufficient tensile strength to prevent tearing yet remain flexible enough to conform to skin contours [59, 60].
Adhesion testing ensures the patch maintains proper contact with the skin throughout the intended duration without causing irritation or detachment. The three main parameters evaluated are:
The in vitro performance of transdermal patches is assessed using Franz diffusion cells to study both drug release and skin permeation. Drug release is tested through synthetic membranes in phosphate buffer (pH 7.4) at 32 ± 0.5 °C, with samples analysed by spectrophotometric or chromatographic methods and fitted to kinetic models such as zero-order, first-order, Higuchi, or Korsmeyer-Peppas to determine release mechanisms. In permeation studies, human or animal skin is used to quantify drug diffusion across the stratum corneum, enabling calculation of flux (J), permeability coefficient (Kp), and lag time (Tlag) to predict in vivo absorption and therapeutic performance [62].
In vivo studies assess the pharmacokinetic and pharmacodynamic behaviour of the patch. Parameters such as Cmax, Tmax, AUC, and steady-state plasma concentrations are compared to conventional dosage forms to establish bioequivalence. Skin irritation and sensitisation tests are also performed in animal models or human volunteers to confirm dermatological safety. The Draize test and patch test are commonly used for irritation assessment [63].
Stability testing follows ICH guidelines (Q1A-Q1F), where patches are stored at controlled temperature and humidity conditions (25°C/60% RH, 40°C/75% RH). At specific intervals, samples are analysed for drug content, mechanical properties, moisture levels, and release profile to determine shelf life and packaging requirements [64].
Proper packaging with moisture- and oxygen-impermeable materials such as aluminium foils is essential for maintaining patch integrity.
Additional evaluations include:
From mechanical durability to bioavailability profiling, each test provides crucial insight into formulation optimisation. The use of modern analytical tools, such as atomic force microscopy, confocal Raman imaging, and biophysical skin models, further enhances the understanding of transdermal transport dynamics and product reliability.
Table 3. Evaluation Parameters for Transdermal Patches
|
Parameter |
Purpose/ Objective |
Method/ Instrument |
Acceptable Criteria/ Remarks |
|
Physical appearance |
Assess colour, flexibility, and surface uniformity |
Visual inspection |
Smooth, uniform, flexible surface |
|
Thickness uniformity |
Ensure consistent drug diffusion |
Digital micrometre (multiple sites) |
Minimal variation (±5%) |
|
Weight variation |
Confirm uniform drug distribution and coating |
Analytical balance |
Within ±5% deviation |
|
Drug content uniformity |
Quantify active ingredient in patch |
UV spectrophotometry, HPLC, LC-MS |
Within ±5% of mean content |
|
Moisture content |
Evaluate flexibility and stability |
Desiccation or oven drying method |
Low but sufficient for flexibility |
|
Moisture uptake |
Assess hygroscopic nature |
Controlled humidity chamber |
Minimal weight gain; avoid tackiness |
|
Folding endurance |
Determine mechanical strength |
Manual repeated folding until break |
>200 folds (typically acceptable) |
|
Tensile strength |
Measure film strength and elasticity |
Texture analyser or tensile tester |
0.5–2.0 kg/cm² depending on polymer |
|
Flatness and smoothness |
Ensure patch consistency |
Visual/micrometric observation |
100% flatness; no wrinkles or air pockets |
|
Water vapour transmission rate (WVTR) |
Assess moisture permeability |
Gravimetric method |
Consistent with polymer type |
The incorporation of nanotechnology has led to a new generation of nanocarrier-based patches, including liposomes, niosomes, solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), and polymeric nanoparticles. These carriers enhance drug solubility, skin penetration, and controlled release. For example, liposomal and ethosomal systems have shown superior permeation for hydrophilic drugs by altering the lipid structure of the stratum corneum. Transferosomes, or ultra-deformable vesicles, allow penetration through narrow pores without rupturing, enabling delivery of large molecules such as insulin or vaccines.
Nanoparticle-laden patches also provide targeted delivery and reduced systemic toxicity, making them ideal for localised treatment of pain, inflammation, and cancer [66, 67].
Microneedle (MN) technology represents one of the most impactful advances in transdermal delivery. These microprojections painlessly pierce the stratum corneum, creating transient microchannels that allow both small and macromolecular drugs to diffuse effectively.
Microneedles are fabricated from biodegradable polymers, silicon, or metals, and can be coated, hollow, or dissolving in nature. Dissolving microneedles made from polymers such as polyvinylpyrrolidone (PVP) or hyaluronic acid release the drug as they dissolve within the skin.
Commercially, products like Zosano Pharma’s Qtrypta® (zolmitriptan) for migraine and MicronJet® for insulin and vaccine delivery demonstrate successful clinical translation [68]. The future promises smart microneedle systems with integrated sensors for real-time feedback and controlled release.
Iontophoresis enhances transdermal delivery by applying a mild electric current to drive charged drug molecules across the skin, while electroporation employs short, high-voltage pulses to create temporary pores in the lipid matrix of the stratum corneum.
These technologies enable controlled, on-demand delivery of peptides, hormones, and even vaccines. For instance, LidoSite®, an iontophoretic lidocaine patch, provides rapid local anaesthesia without needles. Future designs are integrating wearable electronic controllers that modulate current intensity, offering personalised and programmable drug administration [68].
Sonophoresis utilises ultrasound waves to temporarily disrupt the skin barrier and enhance drug permeation by increasing lipid fluidity. Thermal ablation, on the other hand, uses microheaters or lasers to create micropores in the stratum corneum by vaporising small regions without damaging deeper tissues.
These methods allow efficient transdermal delivery of biologics, DNA vaccines, and hormones, providing needle-free alternatives with faster onset and improved bioavailability. Phoresor® systems and ViaDerm® are examples of commercially viable sonophoretic and thermal-based technologies [69].
Recent focus has been on stimuli-responsive (“smart”) hydrogels that alter their physical or chemical properties in response to temperature, pH, or glucose levels. Such systems enable feedback-controlled release, making them ideal for chronic conditions like diabetes.
For instance, glucose-responsive insulin patches embedded with phenylboronic acid-based hydrogels automatically modulate insulin release based on blood glucose concentration. Wearable smart patches integrated with sensors and microprocessors represent the future of personalised medicine [70].
The advent of 3D printing technology has enabled the creation of customised patches with precise control over drug loading, geometry, and release kinetics. 3D printing allows layer-by-layer fabrication of multi-drug systems and complex architectures for combination therapy. These digitally fabricated patches can be tailored to individual patient needs, enhancing therapeutic precision and compliance. Studies on 3D-printed hydrogel microneedles and controlled-release polymer films have demonstrated potential for personalised treatments in dermatology and hormone therapy [71].
The integration of artificial intelligence (AI) and Internet of Things (IoT) into transdermal systems has paved the way for “digital therapeutics. Smart wearable patches now monitor physiological parameters such as heart rate, glucose levels, and drug plasma concentrations, adjusting release rates accordingly.
AI algorithms analyse this data to optimise dosing schedules, improving safety and treatment outcomes. The BioIntelliSense BioSticker® and Chrono Therapeutics’ SmartStop® nicotine patch are examples of connected health technologies that merge drug delivery with real-time monitoring [72].

Figure 6. Representative Examples of Commercial Transdermal Drug Delivery Systems (TDDS).
Several transdermal products have achieved commercial success owing to their convenience, safety, and controlled delivery. Some notable examples include:
Table 4. Marketed Transdermal Products
|
Product Name (Brand) |
Active Drug |
Therapeutic Category / Indication |
Patch Type / Design |
Manufacturer / Company |
|
Transderm-Scop® |
Scopolamine |
Motion sickness |
Reservoir |
Novartis Consumer Health |
|
Catapres-TTS® |
Clonidine |
Hypertension |
Reservoir |
Boehringer Ingelheim |
|
Nitro-Dur® / Nitrodisc® |
Nitroglycerin |
Angina pectoris |
Matrix |
Key Pharmaceuticals / Schering-Plough |
|
Minitran® / Deponit® |
Nitroglycerin |
Angina prophylaxis |
Drug-in-adhesive |
Schwarz Pharma |
|
Duragesic® |
Fentanyl |
Chronic pain management |
Reservoir |
Janssen Pharmaceuticals |
|
Neupro® |
Rotigotine |
Parkinson’s disease / Restless leg syndrome |
Drug-in-adhesive |
UCB Pharma |
|
Nicoderm CQ® / Habitrol® |
Nicotine |
Smoking cessation |
Matrix |
GlaxoSmithKline / Novartis |
|
Estraderm® / Climara® / Vivelle-Dot® |
Estradiol |
Hormone replacement therapy |
Reservoir / Matrix |
Novartis / Bayer |
|
Androderm® |
Testosterone |
Male hypogonadism |
Reservoir |
Allergan |
|
Exelon® Patch |
Rivastigmine |
Alzheimer’s disease / Dementia |
Matrix |
Novartis Pharma |
|
Daytrana® |
Methylphenidate |
Attention Deficit Hyperactivity Disorder (ADHD) |
Drug-in-adhesive |
Noven / Novartis |
|
Lidoderm® |
Lidocaine (5%) |
Localized neuropathic pain |
Drug-in-adhesive |
Endo Pharmaceuticals |
|
BuTrans® / Transtec® |
Buprenorphine |
Moderate to severe pain |
Matrix |
Purdue Pharma / Grunenthal |
|
EMSAM® |
Selegiline |
Major depressive disorder |
Drug-in-adhesive |
Somerset Pharmaceuticals |
|
Tulobuterol Patch® (Hokunalin Tape) |
Tulobuterol |
Asthma / COPD |
Matrix |
Abbott / Shionogi Pharma |
|
Qtrypta® |
Zolmitriptan |
Migraine management |
Microneedle-assisted |
Zosano Pharma |
|
Secuado® |
Asenapine |
Schizophrenia |
Drug-in-adhesive |
Noven Pharmaceuticals |
|
Ionsys® |
Fentanyl (iontophoretic) |
Postoperative pain |
Iontophoretic system |
ALZA / Janssen |
|
Twirla® |
Ethinyl estradiol + Levonorgestrel |
Contraception |
Matrix |
Agile Therapeutics |
|
Xelstrym® |
Dextroamphetamine |
ADHD |
Drug-in-adhesive |
Noven Therapeutics |
|
Buvidal® Patch (Under evaluation) |
Buprenorphine (nanocarrier-based) |
Opioid dependence |
Advanced polymer matrix |
Camurus AB |
|
Smartpatch™ (Prototype) |
Insulin (microneedle + hydrogel) |
Diabetes mellitus |
Smart microneedle system |
Zhenjiang University / BioSerenTech |
These marketed systems exemplify the versatility of transdermal technology across therapeutic classes, including analgesics, cardiovascular drugs, hormones, and neurological agents [73].
The future of transdermal delivery lies in personalised, responsive, and digitalised systems. The convergence of biomaterials engineering, nanotechnology, and artificial intelligence is shaping next-generation patches capable of real-time monitoring, automatic dose adjustment, and sustained, painless administration.
Furthermore, gene and vaccine delivery via transdermal routes is under intense research, with microneedle-mediated DNA vaccination already showing success in preclinical and clinical trials [74]. The continuous evolution of this field promises to make transdermal systems central to the next era of non-invasive, smart therapeutics.
CONCLUSION
The evolution of transdermal drug delivery from simple adhesive patches to advanced, technology-driven systems represent one of the most significant advancements in pharmaceutical science. Conventional oral and parenteral routes often face limitations such as poor bioavailability, systemic side effects, and low patient adherence. In contrast, transdermal systems offer a non-invasive, convenient, and controlled alternative that enhances therapeutic efficiency and patient comfort.
Recent advances have extended the boundaries of TDDS beyond small molecules to include peptides, proteins, and vaccines, facilitated by microneedles, nanocarriers, and smart polymeric systems. Marketed products like Duragesic® (fentanyl), Neupro® (rotigotine), and Qtrypta® (zolmitriptan) showcase the clinical viability of these systems. Emerging technologies, particularly AI-driven, sensor-integrated patches, are paving the way for responsive, on-demand delivery platforms that monitor physiological conditions and adjust dosing automatically.
In conclusion, TDDS has transformed from a supplementary route to a mainstream modality in drug administration. The future lies in personalised, digitalised, and intelligent transdermal systems, combining biocompatible materials with data-driven control for optimised therapeutic outcomes. Continuous interdisciplinary collaboration among pharmacologists, materials scientists, and biomedical engineers will be key to realising the full potential of transdermal drug delivery in next-generation healthcare.
REFERENCES


Prajwal Sinkar, Ishwar Patil, Siddhesh Marda, Transdermal Drug Delivery Systems: Design, Mechanisms, Evaluation, and Emerging Technological Advances in Transdermal Patches, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 2306-2330. https://doi.org/10.5281/zenodo.18340119
 10.5281/zenodo.18340119
10.5281/zenodo.18340119