
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
R. G. Sapkal college of pharmacy, Anjaneri, Trimbakeshwar, Nashik-422213.
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disease characterised by hyperglycaemia due to insulin resistance and decreased insulin secretion. The disease is related to a number of acute and chronic complications such as diabetic ketoacidosis, retinopathy, nephropathy, neuropathy and cardiovascular disorders. Recent advances in biomarkers and precision medicine have led to better early diagnosis and personalised treatment strategies. Traditional Indian medicinal plants like Symplocos racemosa, Acorus calamus and Azadirachta indica have also exhibited promising anti-diabetic activity. This review summarises the pathophysiology, complications, novel therapeutic strategies and the role of herbal medicines in the management of diabetes.
1.1 Definition of diabetes mellitus
A metabolic condition known as chronic hyperglycaemia is brought on by either insufficient insulin secretion, reduced insulin action, or both. Notably, insulin is a crucial anabolic hormone that influences the protein, lipid, and carbohydrate metabolism.[1]Some of the characteristics of diabetes mellitus is a poor or insufficient insulin secretory response, which results in glucose absorption. Because it leads to The most prevalent endocrine illness, hyperglycaemia diabetes mellitus, sometimes known as a "sugar," is typically caused by insufficient or absent insulin or, less frequently, by impaired insulin function. [2] The polypeptide hormone insulin, which controls blood glucose levels and facilitates glucose absorption and utilisation, is secreted by the beta cells of the pancreatic islets of Langerhans.[3]According to the International Diabetes Federation, there are around 40.9 million people with diabetes in India.[2]The WHO reported in 2014 that 8.5% of adults over the age of 18 had diabetes. 48% of the 1.5 million deaths caused by diabetes in 2019 were in those under the age of 70. Furthermore, an additional 460,000 death from kidney illness were linked to diabetes, and increased blood glucose levels were responsible for almost 20% of deaths from cardiovascular disease. Diabetes-related standardised death rates increased by 3% between 2000 and 2019. Diabetes-related mortality increased by 13% in lower-middle-income nations.On the other hand, between 2000 and 2019, the global risk of dying from any of the four main non-communicable diseases—cardiovascular disease, cancer, chronic respiratory illness, or diabetes—between the ages of 30 and 70 decreased by 22%.The screening of all reputable and accessible research and review publications in the diabetic literature served as the basis for the search parameters used here.[1]
2. Type 2 Diabetes mellitus:pathophysiology and complications
Insulin sensitivity is an aspect of type 2 diabetes, which is caused by insulin resistance, decreased insulin production, and eventually the loss of pancreatic β-cells. As a result, the muscles,fat cells, and liver receive less glucose.
The breakdown of fat is accelerated by hyperglycaemia. Impaired α-cell function has recently been connected to the aetiology of type 2 diabetes.[2]The body's ability to maintain physiological glucose levels is limited when β-cell dysfunction occurs because insulin secretion is decreased. However, IR causes the liver to produce more glucose and the muscle, liver, and adipose tissue to absorb less glucose. β-cell dysfunction is typically more severe than IR, even though both processes occur early in the pathophysiology and contribute to the development of the disease. However, hyperglycaemia is increased when both IR and β-cell dysfunction are present, which accelerates the development of type 2 diabetes.[4] Type 2 diabetes is a complicated, progressive illness that affects several organs and is marked by a number of metabolic abnormalities (figure1). [5]
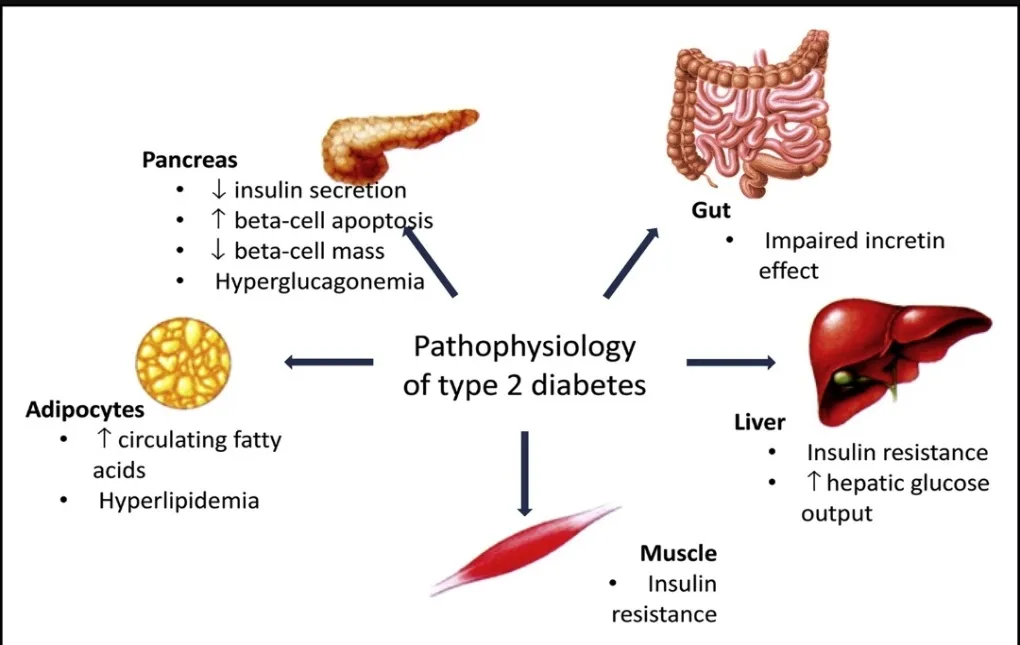
Fig.1 Pathophysiology of type 2 diabetes mellitus
2.1 Insulin resistance (IR)
The physiological definition of insulin resistance is the ability of certain tissues to react to normal insulin levels; as a result, higher than normal insulin levels are necessary to sustain the normal functions of insulin. Notably, insulin-resistant tissues do not exhibit the glucose-regulating effects of insulin at normal plasma levels, including the suppression of HGP and lipolysis, cellular uptake of plasma glucose, and net glycogen synthesis . These tissues are thought to be essential to analysing the mechanisms underlying insulin resistance because skeletal muscle is a quantitatively central tissue for insulin-stimulated glucose disposal and liver and adipose tissue are qualitatively critical sites for glucose-induced insulin signalling.[6]
2.2 insulin resistance in skeletal muscle
"Myokines" are a class of chemicals (cytokines and peptides) secreted by skeletal muscle that have autocrine, paracrine, or endocrine hormone-like effects. Skeletal muscle is increasingly acknowledged as an endocrine organ as a result. The interaction between skeletal muscle and many organs, such as white and brown adipose tissue, the liver, the pancreas, the heart, arteries, bones, and the brain, is crucially dependent on such active secretion. Notably, myocytes produce and release a number of myokines in reaction to muscle contractions.[8]
2.3 insulin resistance in Adipose Tissue and Liver
By inhibiting hepatic glucose synthesis and encouraging the storage of glucose as glycogen, the liver regulates the post-prandial glucose level. Increased hepatic gluconeogenesis is the primary cause of fasting hyperglycaemia in people with type 2 diabetes. Impaired lipolysis in adipose tissue and the liver's inability to inhibit the transcription factor FOXO1 are the main causes of this. Furthermore, impairments in insulin's capacity to promote glycogen synthesis are linked to IR. It is noteworthy that throughout fasting and eating, hepatic IR decreased the amount of hepatic glycogen metabolism. Tyrosine kinase activity is reduced in people with type 2 diabetes mellitus, just as it is in the liver and muscle. shows how obesity-induced IR causes ectopic lipid accumulation in several organs through inter-organ communication involving muscle, liver, adipose tissue, pancreas, gut, and adipose tissue.[9]
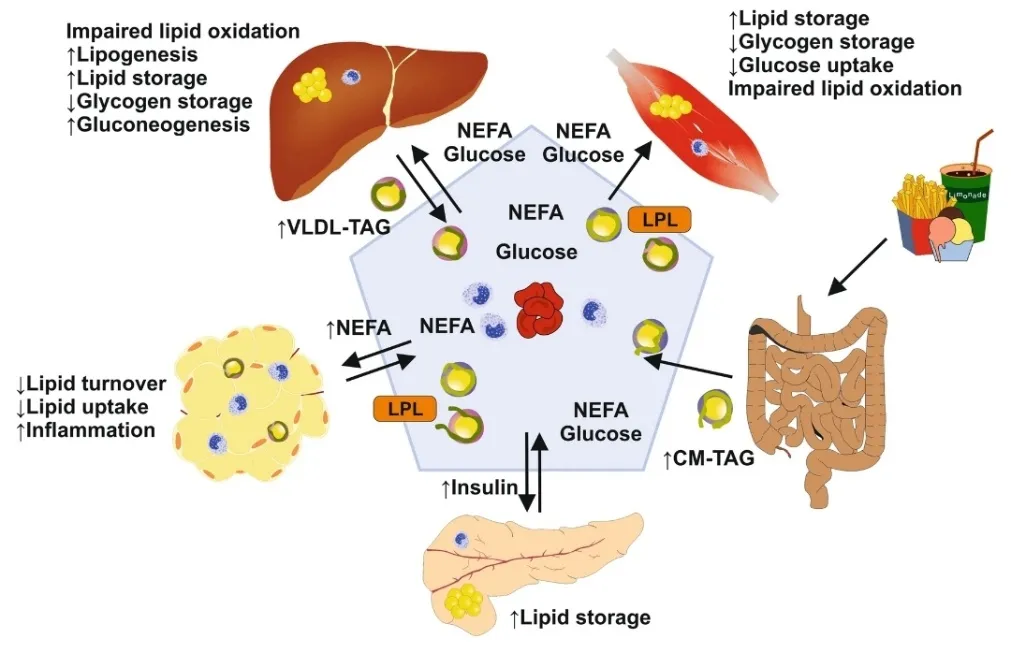
Fig.2 Cellular and Molecular Mechanism of Insulin Resistance
Inter-organ communication in insulin resistance caused on by obesity. Increased absorption of triacylglycerol (TAG) by chylomicron triacylglycerol particles (CM-TAG) from the intestine is caused by lipid overload and overnutrition. Elevated TAG is then transported into other organs, including the liver, muscles, and pancreas, by very low-density lipoprotein-TAG and lipoprotein lipase (LPL), if the absorption and storage capacity of adipose tissue is exceeded. Further, this results in increased levels of triacylglycerol and non-esterified fatty acids (NEFA) in the blood. Impaired lipid oxidation eventually causes fat to build up in many organs, insulin resistance to develop, and noticeably elevated blood glucose levels.[9]
3. Complications
T2DM patients are more susceptible to different forms of both short- and long-term complications. the complications include macrovascular diseases (hypertension, hyperlipidaemia, heart attacks, coronary artery disease, strokes, cerebral vascular disease, and peripheral vascular disease), microvascular diseases (retinopathy, nephropathy, and neuropathy) and cancers.
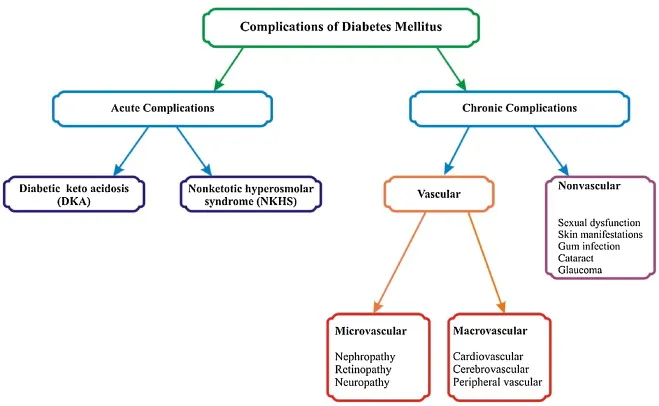
Fig.3.Complication of Diabetes Mellitus
3.1 Acute complications-
3.1.1 Diabetic ketoacidosis (DKA)-
A serious side effect of diabetes is diabetic ketoacidosis, which is caused by insufficient insulin in the body, which raises blood glucose levels and produces ketones. Since diabetic ketoacidosis can result in potentially fatal consequences such cerebral oedema, acute respiratory distress syndrome, and sepsis, it is a medical emergency that needs to be treated right away.[10]
3.1.2. Management of DKA-
1. collecting blood for a metabolic profile prior to starting intravenous fluids; 2. infusing 1-L of 0.9% sodium chloride over the course of one hour after taking the first blood samples; 3. ensuring the potassium level is greater than 3.3 mEq/L prior to starting insulin therapy; and 4. starting insulin therapy only after the first steps have been completed.[11]
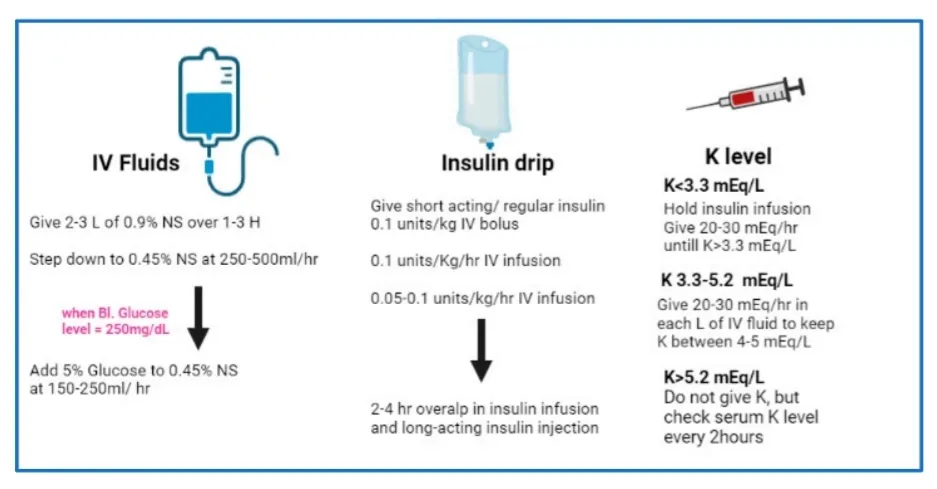
Fig.4. Schematic representation of a simplified protocol for management of patients with DKA. Abbreviations: NS, normal saline, H, hour, Bl. blood, K potassium, IV intravenous
3.1.3. Non-ketotic hyperosmolar syndrome (NKHS)-
Although it is quite relatively rare, non-ketotic hyperosmolar syndrome (NKHS), which results in severe hyperosmolar dehydration without substantial ketoacidosis, can be more deadly than DKA.[11] NKHS are regarded as common diabetic emergencies that require immediate diagnosis and treatment.[12]
3.1.4.Management of (NKHS)
1. Restoration of tissue perfusion and circulation volume.
2. Replacing lost fluids and making up for overall fluid imbalances.
3. Correcting serum hyperosmolarity and hyperglycemia
4. Replacing decreased electrolytes.[13]
4.CHRONIC COMPLICATION
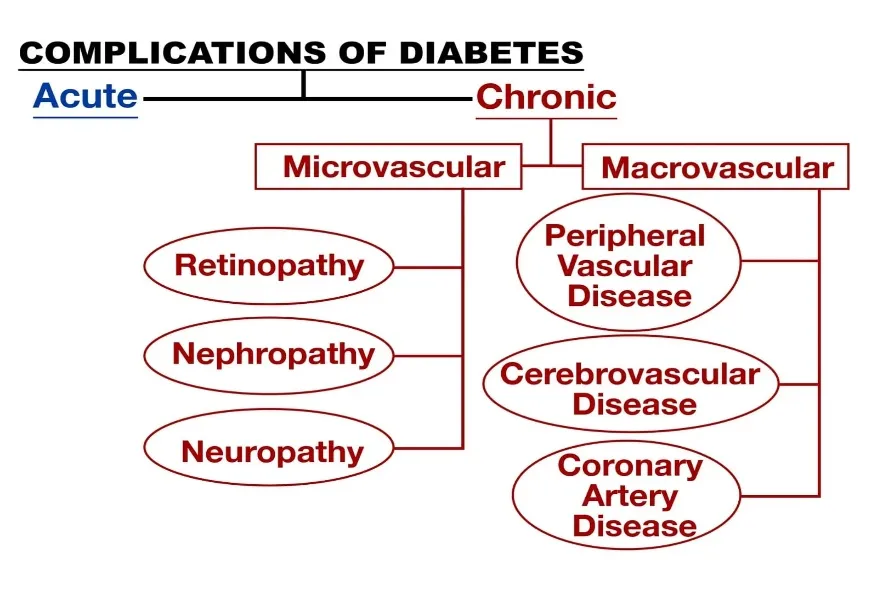
Fig.5.Schematics flow chart of complications of diabetes.
4.1 Microvascular complications-
4.1.1.Diabetic retinopathy(DR)-
Diabetes-related DR is a prominent cause of blindness and vision loss in diabetics. DR is a disorder where continuous hyperglycaemia causes the retinal vasculature to become gradually dysfunctional, resulting in structural damage to the neuronal retina.[14] Retinal nerve damage may exist prior to vascular alterations. Optical Coherence Tomography (OCT) can be used to diagnose the thickening of the retinal nerve fibres layer caused by photoreceptor and retinal ganglion cell apoptosis.[15] Risk factors for DR include poor glycaemic management, a longer history of diabetes, hypertension, dyslipidaemia (total and low-density lipoprotein cholesterol), anaemia, smoking, and microalbuminuria.[16]
4.1.2.Diabetic nephropathy(DN)-
Long-term diabetes mellitus is the cause of DN, a progressive kidney disease. It is characterised by hypertension, chronic albuminuria (the presence of albumin in the urine), and a slow drop in GFR(Glomerular Filtration Rate). Kidney damage is caused by a number of interrelated processes in the complex pathophysiology of DN.[17] For DN, risk variables were classified as either modifiable or non-modifiable. Dyslipidaemia, glycaemic control, and hypertension are modifiable variables. Moreover, smoking is another accessible risk factor. Race, age, gestation, genetic profile, and sex are non-modifiable characteristics.[18]
4.1.3.Diabetic neuropathy(DN)-
With an entire life prevalence of over 50% among individuals with diabetes, diabetic neuropathy (DN) is a significant and prevalent consequence of the disease.[19] Amputations of the legs and diabetic foot ulcers (DFU) are two serious consequences of diabetic neuropathy.[20] diabetes neuropathy encompasses a variety of conditions, such as DSPN, autonomic neuropathy, diabetes radiculo-plexopathy, mononeuropathies, and treatment-induced neuropathies. More than 75% of instances of diabetic neuropathy are caused by the most prevalent type, chronic symmetrical length-dependent sensorimotor polyneuropathy (DSPN).[21]
4.2 Macrovascular complications-
4.2.1 Peripheral vascular disease-
A progressive circulatory disorder called peripheral vascular disease (PVD) decreases the blood flow, especially in the limbs.[21] In addition to being common, PVD may be fatal. It is frequently brought on by atherosclerosis, a condition in which plaque constricts blood arteries and may cause clots to form.[22] PVD risk factors include smoking and high blood pressure, Atherosclerosis ,Diabetes , Elevated cholesterol ,Over 60 age.[23]
4.2.2 .Cerebrovascular Disease-
Diabetes-related cerebral vascular diseases that result in intracranial large and small vessel diseases are known as diabetic cerebrovascular diseases. These diseases are caused by metabolic problems of sugar, fat, and various nutrients. Cerebral blood vessel disorders affect between 20% and 40% of people with type 2 diabetes.[24]
4.2.3.Coronary artery disease-
Cardiovascular disease is highly prevalent in people with diabetes mellitus.[25] Segmental atherosclerotic lesions affecting several arterial branches are a hallmark of coronary artery disease, indicating extensive macrovascular involvement.[26] Antihypertensives, lipid-lowering medications, and regular low-dose aspirin administration are complicated interaction therapy used to prevent premature cardiovascular events.
5.Biomarkers-
Clinicians can detect high-risk patients even before clinical manifestations appear by using biomarkers, which are observable indications of biological processes that properly represent underlying pathophysiological alterations. Biomarkers are showing promise as a way to fill in the gaps left by traditional scoring systems and as a potential entry point for precision stroke care.[27] A biomarker is a naturally occurring particle that is present in blood, other bodily fluids, or tissue that acts as a signal for an infection, disease, other solid or undesirable handling.[28]
6. Precision medicine –
The field of precision medicine assesses how genetic, behavioural, and environmental variables contribute to the development of disease. It specifically assessed how these variables might impact the emergence of illnesses and the effects they have, as well as how they respond to food, lifestyle, and medication use.[29] Through the integration of individual genetic, environmental, and clinical variables, precision medicine seeks to optimise diabetes diagnosis, prediction, prevention, and therapy.[30]
7.Traditional Indian herbal drugs with the potential to treat diabetic Mellitus
Approximately 60% of people on the planet utilise traditional medicines made from therapeutic herbs. The use of Indian herbal remedies and plants, especially in India, to cure diabetes is the main topic of this article. Diabetes is a dangerous condition that affects people worldwide and from all areas of life. It has been shown to be a major health concern in India, especially in urban areas. Herbal formulations are preferred because of their low cost and absence of side effects, even if there are many ways to lessen the detrimental effects of diabetes and its subsequent issues. A list of herbal remedies and medicinal plants with anti-diabetic and other therapeutic properties that are used to treat diabetes.[31]
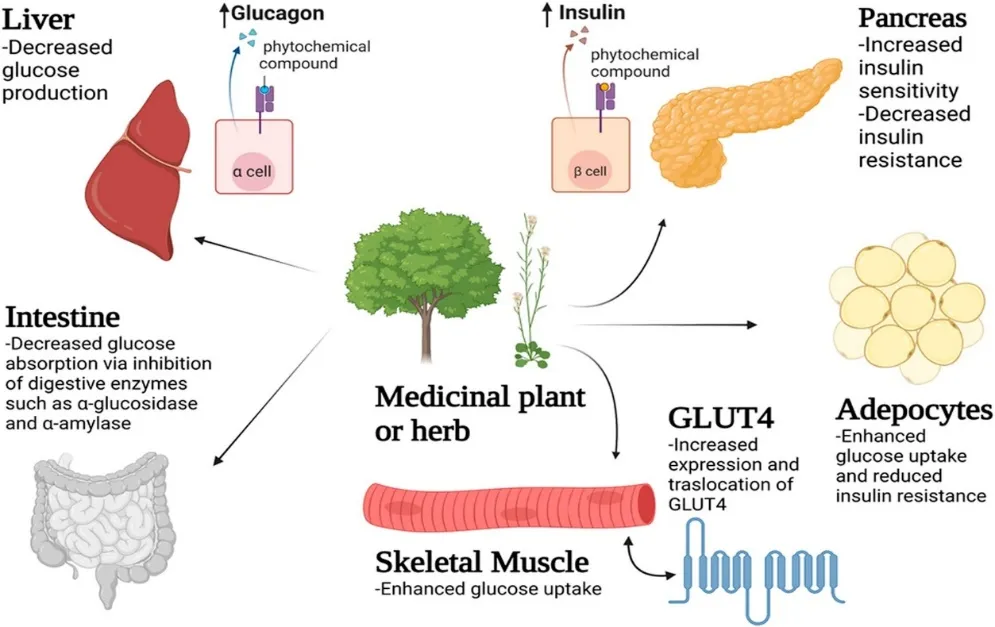
Fig.6. The mechanism of decreasing blood glucose levels by medicinal plants and herbs on different tissues and organs such as the liver, intestine, pancreas, skeletal muscle and adipose tissues.[32]
7.1Neem plant (Azadirachta indica)
Siddha and Ayurvedic practitioners think that neem medicines have anthelmintic, antifungal, antidiabetic, antibacterial, antiviral, contraceptive, and sedative properties. Neem oil is used as a lubricant, insecticide, and drug for diseases like tuberculosis and diabetes. Limonoids, diterpenek, triterpenes, terta-terpenoids, sulphur compounds, flavonol glycosides, and other substances are among its chemical components. The neem plant (Azadirachta indica) contains nimbolide, a terpenoid. The impact of nimbolide at 50 mg/kg for 60 days was examined. The study's findings demonstrated that nimbolide treatment reduced inflammatory mediators TNF-α, IL-1β, and IL-6 by downregulating TLR4 and NF-κB expression. Additionally, it reduces the elevated levels of MMP-9 and VEGF in STZ diabetic rats. Nimbolide's effects were similar to those of the common medication metformin, indicating that it may be used to treat DR.[33]
7.2 Lodhra (symplocos racemosa)
The Racemosa Symplocos Roxb is 6 to 8.5-meter-tall and widely distributed in India's plains and lower hills. Lodhra bark possesses antibacterial, styptic, astringent, and anti-inflammatory qualities. Ayurvedic formulations containing Colloturine, Harman (Loturine), Loturidine, and Proanthocyanidin-3-monoglucofuranosides of 7-Omethyl- and 4'-Omethyl-leucopelargonidin were mostly made from the bark of the Lodhra (Symplocos racemosa). The plant is also known to produce ellagic, betulinic, oleanolic, and acetyl oleanolic acids. The very astringent glycosides that were separated from the stembark's ethanolic extract are thought to be the cause of the bark's therapeutic qualities.[34] In treated diabetic rats, the methanolic extract of stem bark significantly lowers the levels of liver glycogen and plasma insulin.[34]
7.3 Vekhand (Acorus calamus)
Known as "sweet flag" or "calamus," Acorus Calamus Linn is a semiaquatic perennial in the plant family Acoraceae.[35] Saponins, flavonoids, and essential oils are among the constituents of the A. Calamus Rhizome.[35] Oral administration of A. calamus methanolic extract significantly restored blood glucose levels in streptozotocin-induced diabetic rats, according to an antidiabetic study. Biological parameters such as blood glucose, LDL and HDL cholesterol, glucose 6 phosphatase, fructose 1,6 bisphosphatase, and hepatic marker enzymes decreased after 21 days of extract treatment in streptozotocin-induced diabetic rats, while plasma insulin, tissue glycogen, and glucose 6 phosphate dehydrogenase levels significantly increased when compared to the diabetic control. Their research concludes that A. calamusin streptozotocin-induced diabetic rats exhibit antihyperglycemic action.[36]
CONCLUSION
Type 2 diabetes mellitus is a complex progressive disease which if not well managed can lead to serious complications. Early diagnosis, good glycaemic control, biomarker-based monitoring and precision medicine approaches can improve patient outcomes. Moreover, some medicinal plants such as Symplocos racemosa, Acorus calamus and Azadirachta indica also have potential complementary therapeutic benefits. Further research is needed to identify safer and more effective ways to prevent and treat diabetes.
REFERENCES
doi: 10.1016/j.biopha.2023.115734
doi: 10.1016/j.biopha.2023.115734

Priyanka Pachorkar, Dr. Rishikesh Bachhav, Vaishnavi Shindikar, Type 2 Diabetes: Pathophysiology and Management of Diabetic Complication and Herbal Therapeutics, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 5155-5164, https://doi.org/10.5281/zenodo.20769569
 10.5281/zenodo.20769569
10.5281/zenodo.20769569