
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1235Research Scholar at Department of Pharmaceutics, Dr. Shivajirao Kadam College of Pharmacy, Kasabe - Digraj, Maharashtra, India
4Research Scholar at Department of Pharmaceutics, Maratha Vidya Prasarak Samaj College of Pharmacy Nashik, Maharashtra, India
Glucagon-like peptide-1 receptor agonists are highly effective therapeutic agents for the management of type 2 diabetes mellitus & obesity due their glucose-dependent insulinotropic activity, appetite suppression, & cardiometabolic benefits. However, their clinical use has traditionally been limited injectable formulations because of poor oral bioavailability resulting from enzymatic degradation, acidic gastric conditions, low intestinal permeability, & extensive first-pass metabolism. The development of orally administered glucagon like peptide-1 receptor agonists represents a major advancement in peptide drug delivery but remains scientifically challenging. Biological/physicochemical barriers to oral delivery of GLP-1 and innovative formulation strategies designed to overcome these obstacles, including absorption enhancers, enzyme?inhibitors, nanocarriers, gastroretentive formulations and multi-mechanistic delivery systems are critically reviewed in this article. Furthermore, safety concerns, regulatory aspects and future perspectives for the oral preparation of glucagon-like peptide-1 receptor?agonists are discussed emphasizing the importance to develop creative as well as patient-friendly administration forms.
The gastrointestinal tract’s enteroendocrine L-cells secrete the incretin hormone glucagon-like peptide-1 in response dietary intake, playing a critical role in maintenance of glucose homeostasis. Following nutrient ingestion, glucagon like peptide-1 is released in circulation & coordinates metabolic responses through endocrine, paracrine, & neuroendocrine mechanisms [1]. Physiologically, glucagon like peptide-1 improves postprandial glycaemic control & overall energy balance by enhancing glucose-dependent insulin secretion from pancreatic β-cells, suppressing glucagon release from α-cells, delaying gastric emptying, & promoting satiety via central nervous system signalling pathways [2]. Beyond glycaemic regulation, glucagon like peptide-1 signalling has been shown exert beneficial effects on β-cell preservation, insulin sensitivity, inflammatory pathways, & cardiovascular physiology, underscoring its multifaceted role in metabolic health. However, the direct therapeutic application of native glucagon like peptide-1 is severely limited by its extremely short plasma half-life, primarily resulting from rapid enzymatic degradation by dipeptidyl peptidase-4 & renal clearance. These limitations have necessitated the development of more stable & long-acting glucagon like peptide-1 analogues for clinical use [3].One of the most successful therapeutic classes for the management of type 2 diabetes mellitus & obesity is glucagon like peptide-1 receptor agonists, which were developed overcome the intrinsic limitations of endogenous glucagon like peptide-1. By selectively activating the glucagon like peptide-1 receptor & resisting enzymatic degradation, these agents prolong systemic exposure & enhance therapeutic efficacy [4]. Through strategic structural modifications such as amino acid substitution, lipid conjugation, or fusion carrier molecules, glucagon like peptide-1 RAs achieve sustained glycaemic control with a reduced risk of hypoglycaemia due their glucose-dependent mechanism of action. In addition, improving glycaemic parameters, glucagon like peptide-1 RAs induce clinically significant & durable weight loss, improve cardiometabolic risk profiles, & confer protective effects on cardiovascular & renal outcomes, leading their prioritization in contemporary clinical treatment guidelines for metabolic diseases [5].
The majority of glucagon like peptide-1 receptor agonists are currently administered via subcutaneous injection, which poses a substantial barrier patient acceptance & long-term adherence despite their strong clinical efficacy & favorable safety profile. Injectable therapies are frequently associated with discomfort, needle aversion, inconvenience, & psychological burden, all of which can negatively influence treatment initiation & persistence, particularly in chronic conditions requiring lifelong therapy [6]. Reduced adherence in real-world clinical settings can compromise therapeutic effectiveness & attenuate the long-term benefits observed in controlled clinical trials. Consequently, there has been growing interest in the development of orally administered glucagon like peptide-1 receptor agonist formulations that combine the robust efficacy of this drug class with the convenience, familiarity, & patient preference associated with oral dosage forms [7].Because of the complex & hostile environment of the gastrointestinal tract, oral delivery of peptide-based therapeutics has long been considered extremely challenging. Peptides are intrinsically unstable macromolecules with high hydrophilicity & poor intestinal epithelial permeability, resulting in minimal absorption following oral administration. In addition, the presence of acidic gastric conditions, abundant proteolytic enzymes, & the protective mucus barrier further compromises peptide stability & transport within the gastrointestinal tract [8]. Nevertheless, recent advances in pharmaceutical formulation science, excipient design, & delivery technologies have renewed interest in oral peptide delivery. These developments have challenged long-standing assumptions regarding the feasibility of oral peptide therapeutics by demonstrating that pharmacologically relevant systemic exposure can be achieved for large & structurally complex biomolecules through appropriate formulation strategies & optimized dosing regimens [9].
Despite these advances, the oral administration of glucagon like peptide-1 receptor agonists remains highly challenging. These peptides exhibit poor lipophilicity & relatively high molecular weights (3–4 kDa), which severely restrict passive diffusion across the intestinal epithelial barrier. In addition, glucagon like peptide-1 receptor agonists are highly susceptible degradation by gastric acid & gastrointestinal proteolytic enzymes present in both the stomach & small intestine, while the intestinal mucus layer further limits absorption by trapping peptide molecules & restricting their diffusion ward the epithelial surface [10]. Even when epithelial uptake occurs, extensive first-pass hepatic metabolism markedly reduces the fraction of drug reaching the systemic circulation. Consequently, these combined biological & physiological barriers result in extremely low & highly variable oral bioavailability [11].A wide range of formulation strategies has been investigated overcome the multifactorial barriers associated with the oral delivery of glucagon like peptide-1 receptor agonists. These approaches include molecular modifications enhance peptide stability & membrane interactions, gastroretentive formulations prolong residence time at favorable absorption sites, nanocarrier-based systems protect peptides & facilitate transport, enzyme inhibitors reduce proteolytic degradation, & absorption enhancers transiently increase epithelial permeability [12]. While each strategy offers distinct advantages, they are also associated with limitations related safety, interindividual variability, manufacturing complexity, scalability, & regulatory acceptance.
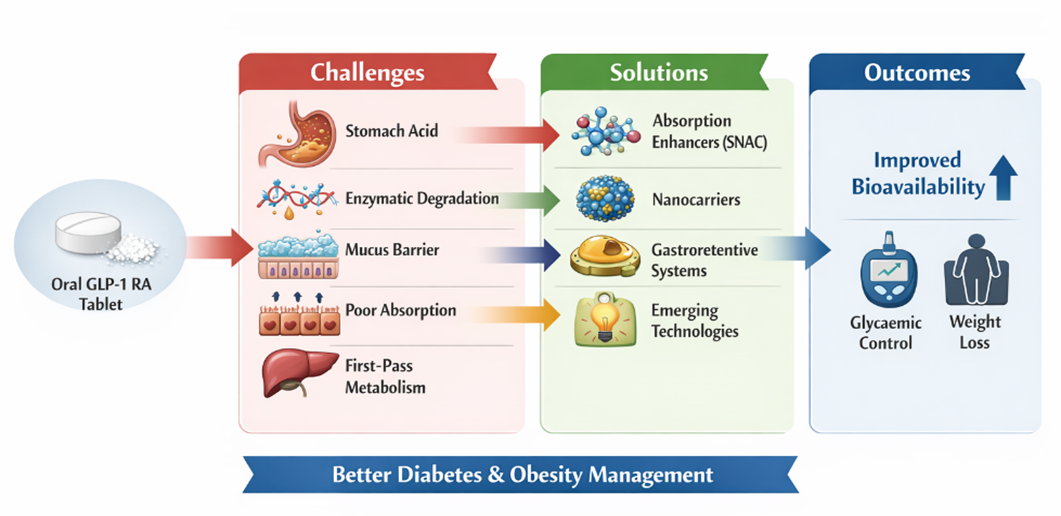
Fig 1: Oral Delivery of GLP-I Receptor Agonists
Consequently, effective oral peptide delivery often requires the integration of multiple complementary technologies rather than reliance on a single formulation intervention, particularly for therapies intended for long-term administration [13].It is imperative critically assess current developments in oral glucagon like peptide-1 receptor agonist delivery given the fast-rising worldwide burden of type 2 diabetes mellitus & obesity, as well as the expanding need for non-injectable biologic medicines [14]. Direct future research & development efforts, a thorough grasp of the biological obstacles, formulation techniques, clinical performance, & translational difficulties are crucial. This kind of assessment is required make sure that new oral glucagon like peptide-1 receptor agonist technologies strike the best possible balance between patient convenience, safety, efficacy, & regulatory viability. Therefore, with a focus on translational relevance & future directions, this review attempts methodically investigate the difficulties related oral delivery of glucagon like peptide-1 receptor agonists & critically discuss established & emerging formulation strategies intended overcome these challenges [15].
2. GLP-1 Receptor Agonists: An Overview
A significant class of incretin-based medications known as glucagon-like peptide-1 receptor agonists imitates the physiological effects of endogenous glucagon like peptide-1 [16]. These medications are very successful in treating type 2 diabetes mellitus (T2DM) & obesity because they increase glucose-dependent insulin secretion, restrict glucagon release, postpone stomach emptying, decrease hunger, & encourage clinically substantial weight loss [17].However, endogenous glucagon like peptide-1 has a very short plasma half-life of less than two minutes due its quick degradation by dipeptidyl peptidase-4 (DPP-4). Synthetic glucagon like peptide-1 receptor agonists have been designed with structural alterations that provide improved stability & extended systemic activity in order get around this restriction [18].
By attaching glucagon like peptide-1 receptors expressed in several tissues, such as the pancreas, gastrointestinal tract, central nervous system, kidney, & cardiovascular system, Glucagon like peptide-1 receptor agonists produce their pharmacological effects. When these receptors are activated, glucagon secretion is suppressed & glucose-dependent insulin secretion is stimulated via cyclic adenosine monophosphate (cAMP)-mediated signalling pathways [19]. Additionally, by acting on cerebral satiety centres, Glucagon like peptide-1 receptor agonists decrease hunger & postpone gastric emptying, which results in lower energy intake & long-term weight loss. Large cardiovascular outcome studies have indicated that these medicines have cardioprotective effects, such as reduced inflammation & enhanced endothelial function, in addition improving β-cell activity & survival. Glucagon like peptide-1 receptor agonists are now considered essential treatments in the treatment of contemporary diabetes due their combined metabolic & cardiovascular advantages [20].Glucagon like peptide-1 receptor agonists are made withst& enzymatic degradation & prolong their duration of action from a pharmacokinetic & pharmacological st&point. accomplish this goal, a number of molecular techniques have been used, such as fusion large carrier proteins like immunoglobulin Fc fragments, amino acid substitutions provide resistance dipeptidyl peptidase-4 (DPP-4) cleavage, & fatty acid acylation encourage reversible albumin binding [21]. further improve molecule stability & systemic exposure, other strategies like PEGylation & peptide backbone modification have also been investigated. Because of these structural changes, elimination half-lives are noticeably longer, which permits fewer doses & better patient convenience. As a result, long-acting glucagon like peptide-1 receptor analogues have half-lives ranging from several days around one week, allowing for simple once-weekly dosage regimens, while short-acting glucagon like peptide-1 receptor agonists usually require several daily injections [22].
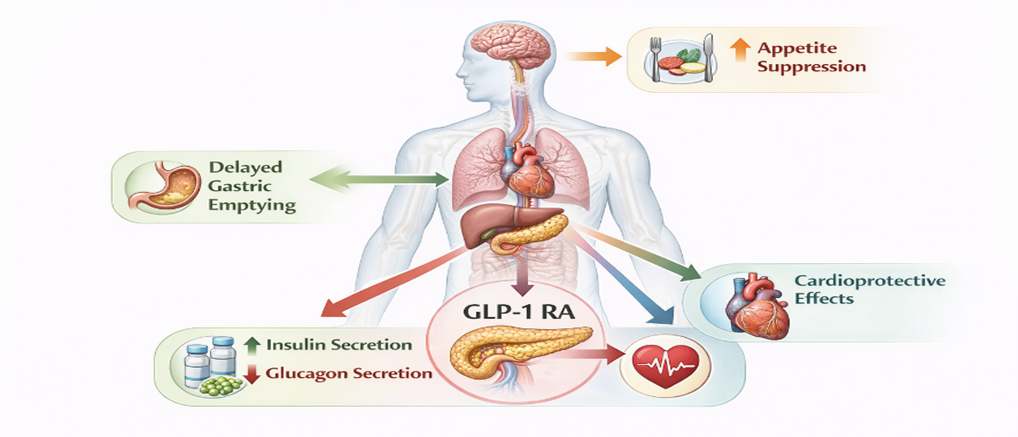
Fig 2: Mechanism of Action Of GLP-I Receptor Agonists
Exenatide, liraglutide, dulaglutide, semaglutide, & lixisenatide are among the glucagon like peptide-1 receptor agonists that are presently authorised for clinical usage [23]. A combined glucose-dependent insulinotropic polypeptide (GIP) & glucagon like peptide-1 receptor agonist is another more recent pharmaceutical development that has shown better glycaemic management & improved weight-loss results when compared conventional glucagon like peptide-1 receptor agonists. Because of the differences in these medicines' molecular structures, pharmacokinetic characteristics, & dosage frequency, customised treatment selection based on patient requirements & clinical response is possible [24].The creation of a glucagon like peptide-1 receptor agonist that may be taken orally is one of the most important developments in peptide-based treatments [25]. The integration of an absorption-enhancing excipient system intended shield the peptide from gastrointestinal breakdown & promote epithelial uptake made this accomplishment possible. This strategy's effective clinical translation has encouraged more research in non-injectable biologic medicines & offered proof-of-concept for the oral delivery of complicated peptide medications [26].
Despite their clinical success, glucagon like peptide-1 receptor agonists present substantial challenges for oral delivery. These peptide-based molecules possess relatively high molecular weights in the range of 3–4 kDa, exhibit pronounced hydrophilicity & poor lipophilicity, & are highly susceptible enzymatic degradation in the acidic gastric environment as well as throughout the intestinal tract. Furthermore, their epithelial permeability is extremely low, & they are subject extensive first-pass metabolism, all of which severely limit oral bioavailability [27]. These combined barriers explain why most glucagon like peptide-1 receptor agonists are available exclusively as injectable formulations & why extensive formulation innovation was required achieve clinically viable oral peptide therapies. As a result, oral distribution of glucagon like peptide-1 receptor agonists continues be a significant pharmacological problem & motivates research in sophisticated formulation techniques, such as molecular structural alterations, absorption enhancers, nanocarrier-based systems, & gastroretentive platforms [28].
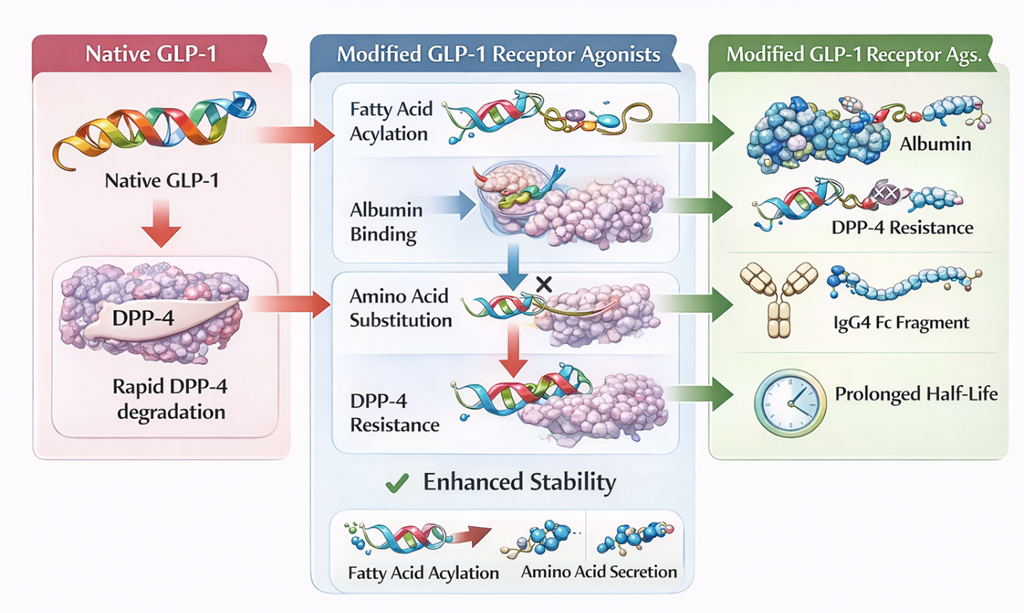
Fig 3: Structural Modifications of GLP-I Receptor Agonists
3. Challenges in Oral Delivery of GLP-1 Receptor Agonists
3.1. Overview of Biological & Physiological Barriers Oral GLP-1 Delivery
Glucagon like peptide-1 receptor agonists' biological origin, physicochemical characteristics, & the intricate environment of the gastrointestinal tract present a number of interconnected obstacles for oral delivery [29]. Together, these obstacles lead incredibly poor & highly variable oral bioavailability, which restricts the practical viability of traditional oral dose forms for peptide-based treatments [30].
3.2. Enzymatic Degradation in the Gastrointestinal Tract
Enzymatic breakdown in the gastrointestinal tract is one of the main obstacles the oral administration of glucagon like peptide-1 receptor agonists [31]. Peptide-based compounds known as glucagon like peptide-1 receptor agonists are extremely vulnerable proteolytic enzymes, including trypsin, chymotrypsin, & elastase in the small intestine & pepsin in the stomach. A sizable portion of the given dose experiences quick enzymatic cleavage even before it reaches the absorptive epithelium, which results in a loss of biological activity. A significant barrier obtaining therapeutically relevant plasma concentrations after oral treatment is this widespread presystemic breakdown [32].
3.3. Acidic Gastric pH–Induced Instability
Peptide integrity is further jeopardised by acidic stomach pH in addition enzymatic nstability [33]. Peptide denaturation, aggregation, & hydrolysis can be caused by the harsh stomach environment, which has a pH range of roughly 1–3. This is especially true for structurally complicated compounds like glucagon like peptide-1 receptor agonists. Delayed drug release frequently moves the site of exposure the colon, where significant enzymatic breakdown continues, even if enteric coating techniques may offer some protection against gastric acidity. Therefore, pH-related instability continues be a major obstacle the effective oral administration of peptide-based treatments [34].
3.4. Poor Intestinal Epithelial Permeability
Poor epithelium permeability is another significant barrier the oral administration of glucagon like peptide-1 receptor agonists [35]. Glucagon like peptide-1 receptor agonists have very little passive diffusion through the intestinal epithelium because of their high molecular weight (around 3–4 kDa), strong hydrophilicity, & several hydrogen-bond-forming functional groups. While transcellular transport is limited by low lipophilicity & the lack of particular transport mechanisms, paracellular transport is severely restricted by tight junctions between epithelial cells. As a result, glucagon like peptide-1 receptor agonists' effective permeability coefficients are insufficient enable significant systemic absorption after oral treatment [36].
3.5. Mucus Barrier–Mediated Limitation of Drug Transport
Another physiological barrier the oral administration of glucagon like peptide-1 receptor agonists is the mucus barrier. Large, hydrophilic molecules are trapped by the intestinal mucus layer, which acts as a viscoelastic gel restrict their diffusion wards the epithelial surface [37]. Before reaching absorptive cells, peptide therapies like glucagon like peptide-1 receptor agonists may become stuck or degrade in the mucus layer, further decreasing oral bioavailability. Furthermore, variations in systemic exposure & irregular absorption patterns can be caused by interindividual differences in mucus composition & thickness [38].
3.6. First-Pass Metabolism & Hepatic Clearance
Moreover, even with effective epithelial absorption, first-pass metabolism dramatically lowers systemic exposure. The portal circulation carries peptides that have been absorbed via the intestinal epithelium the liver, where they may undergo further metabolic breakdown prior entering the systemic circulation. The extremely low absolute bioavailability of oral glucagon like peptide-1 receptor agonists, which usually stays below 1% in the absence of specialised delivery technology, is further exacerbated by this occurrence [39].
3.7. Patient-Related & Physiological Variability Affecting Oral Absorption
Glucagon like peptide-1 receptor agonist oral delivery results are also significantly influenced by physiological & patient-related factors. Drug absorption & systemic exposure can be significantly impacted by gastrointestinal transit time, the presence or absence of food, variations in stomach emptying, & interindividual variations in digestive enzyme expression & epithelium integrity [40]. For instance, reduce pharmacokinetic variability & improve absorption, oral glucagon like peptide-1 receptor agonist formulations frequently need be delivered under tightly regulated circumstances, such as while fasting & with a small amount of water. These specifications draw attention the practical & patient-related difficulties that oral peptide treatment presents in actual clinical settings [41].
Table No 1: Physicochemical & Biological Barriers to Oral Delivery of GLP-1 RAs
|
Sr. No. |
Barrier Category |
Specific Barrier |
Impact on Oral Bioavailability |
Reference |
|
1 |
Enzymatic |
Pepsin, trypsin, chymotrypsin |
Rapid peptide degradation |
[42] |
|
2 |
pH-related |
Gastric acidity (pH 1–3) |
Denaturation & hydrolysis |
[43] |
|
3 |
Physicochemical |
High MW (3–4 kDa), hydrophilicity |
Poor membrane permeability |
[44] |
|
4 |
Epithelial |
Tight junction restriction |
Limited paracellular transport |
[45] |
|
5 |
Mucus |
Mucus entrapment |
Reduced epithelial access |
[46] |
|
6 |
Metabolic |
First-pass hepatic metabolism |
Reduced systemic exposure |
[47] |
|
7 |
Physiological |
Food effect, GI transit variability |
High PK variability |
[48] |
3.8. Implications for the Need of Advanced Oral Delivery Strategies
Together, these physiological, physicochemical, & biological limitations highlight the need for sophisticated formulation techniques & explain why the majority of glucagon like peptide-1 receptor agonists are currently injected. Innovative strategies, such as absorption enhancers, enzyme inhibitors, nanocarrier-based systems, gastroretentive formulations, & peptide structural modifications—all of which are covered in depth in later sections of this review—are needed overcome these obstacles [49].
4. Formulation Strategies for Oral Delivery of GLP-1 Receptor Agonists:
4. 1. Rationale & Overview of Advanced Oral Formulation Approaches
Numerous formulation techniques have been studied get over the many biological & physicochemical obstacles related the oral administration of glucagon like peptide-1 receptor agonists. These methods are intended lengthen gastrointestinal residence time, improve epithelial permeability, shield peptide molecules from chemical & enzymatic destruction, & ultimately increase systemic bioavailability [50]. Successful oral delivery frequently necessitates the integration of several complimentary technologies rather than relying on a single formulation intervention due the inherent complexity of peptide-based medicines [51].
4. 2. Absorption Enhancers: Clinical Success & Limitations of SNAC-Based Systems
The use of absorption enhancers, which momentarily improve intestinal permeability & promote transcellular or paracellular transport of peptide molecules, is one of the most therapeutically sophisticated formulation techniques for oral delivery of glucagon like peptide-1 receptor agonists. Due its successful use in an oral glucagon like peptide-1 receptor agonist formulation, sodium N- [8-(2-hydroxy benzoyl) amino] caprylate (SNAC) has drawn a lot of attention among these. According reports, SNAC works by promoting transcellular absorption across the gastric epithelium, increasing the apparent lipophilicity of the peptide, & locally raising the pH of the stomach lessen acid-mediated peptide breakdown [52]. Even though the absolute oral bioavailability is usually less than 1%, this multifactorial approach allows for measurable systemic exposure. However, the need for relatively high SNAC concentrations & stringent fasting conditions draws attention significant drawbacks, such as absorption variability & possible safety issues with long-term permeation enhancer usage [53].
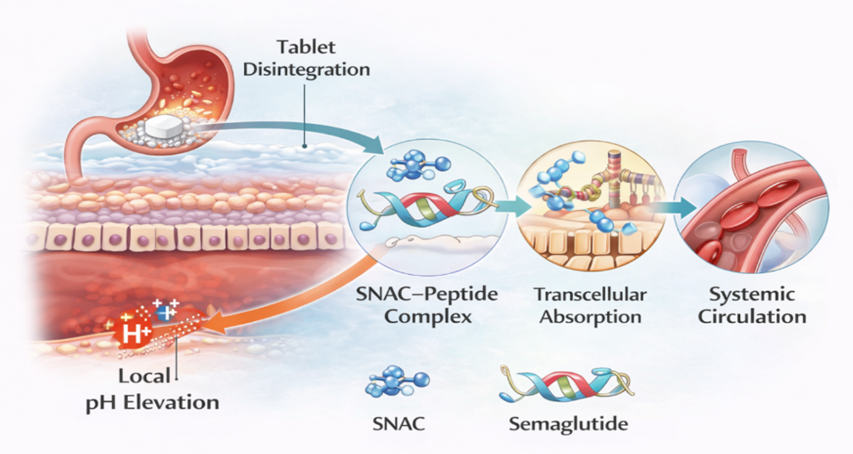
Fig 4: SNAC-Based Absorption Mechanism for Oral Semaglutide
4. 3. Alternative Absorption Enhancers & Permeation-Modulating Agents
Other kinds of absorption enhancers, such as medium-chain fatty acids, bile salt derivatives, chelating agents like ethylenediaminetetraacetic acid (EDTA), & surfactants, have been thoroughly studied for oral peptide administration in addition SNAC. Through processes like temporary relaxation of tight junctions, enhanced membrane fluidity, & modification of transporter or efflux activity, these drugs improve peptide absorption [54]. Concerns about epithelial damage, long-term safety, & high interindividual variability in absorption have hindered the clinical translation of such strategies, especially for chronic therapies like glucagon like peptide-1 receptor agonists, even though they have shown notable improvements in peptide permeability in preclinical models [55].
4. 4. Enzyme Inhibition Strategies to Reduce Gastrointestinal Proteolysis
Incorporating enzyme inhibitors lessen proteolytic breakdown in the gastrointestinal system is another crucial formulation technique. It has been demonstrated that protease inhibitors, such as pepstatin A, soybean trypsin inhibitor, & aprotinin, shield peptide medicines from enzymatic cleavage & improve oral bioavailability [56]. Chronic suppression of digestive enzymes, however, raises questions about possible immunogenicity, gastrointestinal damage, & poor nutritional absorption. For the oral delivery of glucagon like peptide-1 receptor agonists, enzyme inhibitors are therefore typically considered supplementary formulation components rather than standalone treatments [57].
4. 5. Nanotechnology-Based Delivery Systems for Enhanced Stability & Permeability
A promising platform for the oral administration of peptide therapies is nanotechnology-based delivery systems. glucagon like peptide-1 receptor agonists can be encapsulated by polymeric nanoparticles, lipid-based carriers, & hybrid delivery methods, preserving them from enzymatic degradation & promoting transport across the intestinal epithelium. Because of their biocompatibility, biodegradability, & adjustable drug release characteristics, polymers including poly (lactic-co-glycolic acid) (PLGA), chitosan, & Eudragit have been thoroughly studied [58]. Particularly, chitosan-based nanoparticles have significant mucoadhesive properties & can temporarily open epithelial tight junctions, improving peptide medication paracellular delivery. Furthermore, lipid-based nanocarriers such solid lipid nanoparticles & nanostructured lipid carriers may enhance systemic exposure & decrease first-pass hepatic metabolism by promoting lymphatic absorption & improving peptide stability [59].
4. 6. Gastroretentive Delivery Systems for Prolonged Gastric Exposure
Another significant formulation strategy that is especially pertinent glucagon like peptide-1 receptor agonists is gastroretentive delivery methods, particularly for oral formulations that show preferential absorption in the stomach. The purpose of dosage forms such mucoadhesive formulations, expandable systems, & floating tablets is increasing the length of drug exposure at the absorption site by extending the gastric residence time [60]. These devices can increase the possibility of peptide absorption while lowering exposure intestinal proteolytic enzymes by keeping prolonged contact with the stomach mucosa. However, obtaining consistent & predictable performance of gastroretentive systems continues be significantly hampered by variations in stomach motility, gastric emptying rates, & patient-dependent physiological parameters [61].
4. 7. Combination & Multifunctional Formulation Strategies
For the oral administration of peptide therapies, combination approaches that incorporate several protective & permeation-enhancing mechanisms are being investigated more & more. These methods include combinations of enteric coatings, pH-modifying excipients, or nanoparticulate carrier systems with absorption enhancers [62]. These multipurpose delivery systems are intended minimise the safety hazards connected with the use of large quantities of specific excipients while simultaneously achieving synergistic increases in peptide stability & epithelial permeability. Because it allows for a balanced optimisation of efficacy, safety, & translational potential, this integrated formulation technique is becoming more & more popular in the development of next-generation oral peptide therapies [63].
4. 8. Emerging & Device-Assisted Oral Delivery Technologies
For peptide therapies, a number of innovative oral administration methods are now being researched in addition traditional formulations. Increase oral peptide uptake & stability inside the gastrointestinal tract, proprietary carrier-based absorption platforms & protein oral delivery systems use optimised combinations of permeation enhancers & protective matrices [64]. Although these technologies have great potential improve oral bioavailability, significant concerns regarding scalability, manufacturing complexity, cost-effectiveness, & long-term safety must be carefully evaluated before they can be widely applied in clinical settings [65].
4. 9. Current Status & Future Perspectives in Oral GLP-1 Formulation Development
As demonstrated by the successful commercialisation of an oral glucagon like peptide-1 receptor agonist, formulation techniques for the oral delivery of glucagon like peptide-1 receptor agonists have generally advanced significantly. However, limited absolute bioavailability, stringent dosage requirements, & persistent safety concerns related long-term administration continue limit current methods [66]. Future development & wider clinical use of oral glucagon like peptide-1 receptor agonists will depend on ongoing innovation centred on the creation of safer permeation-enhancing technology, enhanced peptide stability, & more patient-friendly dosage regimes [67].
Table No 2: Formulation Strategies for Oral GLP-1 Receptor Agonists
|
Sr. No. |
Strategy |
Mechanism |
Advantages |
Limitations |
Reference |
|
1 |
Absorption enhancers (SNAC) |
↑ Transcellular transport |
Clinically validated |
Low bioavailability, fasting required |
[68] |
|
2 |
Enzyme inhibitors |
Protease inhibition |
Protect peptide |
Safety concerns |
[69] |
|
3 |
Nanoparticles |
Encapsulation & protection |
Enhanced stability |
Scale-up challenges |
[70] |
|
4 |
Gastroretentive systems |
Prolong gastric residence |
Site-specific absorption |
GI variability |
[71] |
|
5 |
Mucoadhesive systems |
Increased contact time |
Improved uptake |
Mucus trapping risk |
[72] |
|
6 |
Combination systems |
Synergetic effects |
Higher efficiency |
Formulation complexity |
[73] |
5. Clinically Advanced Oral GLP-1 Receptor Agonist Formulations
5. 1. Clinical Translation & Proof-of-Concept for Oral Peptide Delivery
An important development in the realm of peptide medication delivery is the effective clinical translation of oral glucagon like peptide-1 receptor agonists. Orally administered glucagon like peptide-1 receptor agonists, in contrast traditional injectable formulations, necessitate extremely complex formulation techniques get over substantial first-pass metabolism, low epithelial permeability, & gastrointestinal degradation [74]. Recent developments have shown that clinically significant therapeutic effects can be attained through optimised formulation design in conjunction with meticulously regulated dosage methods, even while absolute oral bioavailability is still low [75].
5. 2. Multifunctional Excipient Systems for Protection & Absorption Enhancement
Clinically sophisticated oral glucagon like peptide-1 receptor agonist formulations usually rely on multifunctional excipient systems that improve epithelium absorption while simultaneously shielding peptide molecules from enzymatic & acidic breakdown. These systems frequently use transcellular transport channels, temporary changes in membrane fluidity, & localised manipulation of stomach pH [76]. Even while absolute bioavailability levels often stay below 1%, these formulations offer systemic exposure sufficient elicit pharmacodynamic effects comparable parenteral delivery by fostering a favourable milieu that improves peptide stability & absorption [77].
5. 3. Formulation-Assisted Site-Specific Absorption Strategies
Site-specific absorption is another distinguishing feature of sophisticated oral glucagon like peptide-1 receptor agonist formulations. Some formulations are specifically made encourage absorption in the upper gastrointestinal tract, where residence time can be more effectively controlled & enzymatic exposure may be relatively reduced, as opposed primarily depending on intestinal uptake, which is linked extensive enzymatic activity & restrictive epithelial barriers [78]. This approach emphasises how crucial it is targeting particular gastrointestinal areas with formulation assistance in order improve systemic exposure & oral peptide absorption [79].
5. 4. Clinical Efficacy & Dependence on Controlled Dosing Conditions
Glycated haemoglobin (HbA1c) levels & body weight have consistently decreased in clinical trials of oral glucagon like peptide-1 receptor agonists, demonstrating that oral administration can achieve therapeutic efficacy when accompanied by suitable formulation technologies. Strict dosing guidelines, such as administering the medication when fasting & limiting water & post-dose food intake, are crucial for these clinical results [80]. In order produce oral peptide medicines that are both successful & patient-friendly, it is necessary strike a careful balance between formulation performance & patient convenience [81].
5. 5. Limitations, Variability, & Safety Considerations in Clinical Use
Despite these developments, oral glucagon like peptide-1 receptor agonist formulations with clinical validation continue have a number of significant drawbacks. Significant obstacles still include the need for comparatively high quantities of functional excipients, notable interindividual variability in absorption, & sensitivity gastrointestinal physiological circumstances [82]. Furthermore, rigorous regulatory assessment & post-marketing surveillance are required due long-term safety concerns associated with chronic exposure permeation-enhancing excipients. When taken as a whole, these elements highlight the necessity of ongoing innovation targeted at increasing patient adherence oral peptide therapy, lowering dosage restrictions, & strengthening formulation robustness [83].
5. 6. Impact on the Future of Oral Biologic & Peptide Therapeutics
All things considered, the clinical success of sophisticated oral glucagon like peptide-1 receptor agonist formulations has shown strong evidence that oral peptide delivery is feasible. Expectations for non-injectable biologic medicines have changed as a result of these advancements, which have also sparked larger research initiatives apply comparable formulation techniques additional therapeutic peptides [84]. Crucially, the rational design of next-generation oral delivery systems with better safety profiles, increased therapeutic efficacy, & higher patient acceptance is still influenced by the lessons discovered throughout the development & clinical translation of existing formulations [85].
6. Emerging Technologies for Oral Delivery of GLP-1 Receptor Agonists
Conventional formulation methods for oral glucagon like peptide-1 receptor agonist delivery are still limited by low absolute bioavailability, stringent dosage requirements, & safety issues related long-term exposure permeation-enhancing excipients, despite recent clinical advancements. As a result, a variety of cutting-edge methods are being actively investigated enhance the oral administration of glucagon like peptide-1 receptor agonists. While preserving long-term safety & lerability, these next-generation approaches seek improve peptide stability, boost epithelial transport efficiency, decrease interindividual variability in drug absorption, & promote patient comfort [86].Peptide structure engineering is one exciting field of study for oral glucagon like peptide-1 receptor agonist administration. It has been demonstrated that rational peptide sequence modification, including amino acid replacement, cyclisation, lipid conjugation, & backbone stabilisation, can increase resistance enzyme degradation while maintaining receptor affinity & biological activity [87]. Fatty-acid conjugation is one of these tactics that works well because it increases reversible albumin binding & lengthens the duration of systemic circulation, which helps partially offset oral absorption. These molecular optimisation techniques serve as a useful supplement formulation-based distribution methods & lessen reliance on strong permeation enhancers [88].Recently, deep eutectic systems & ionic liquids have drawn more interest as innovative excipient platforms for oral peptide administration. By creating short-lived, non-covalent complexes with the therapeutic molecule, these systems can improve membrane permeability, physicochemical stability, & peptide solubility [89]. Additionally, by modifying membrane fluidity & decreasing peptide aggregation at the epithelial interface, ionic liquid-based formulations may promote transcellular transport. Even though these methods are still in the early stages of development, they offer a flexible & adjustable way enhance oral peptide absorption & show promise for oral biologic formulations of the future [90].Another significant new trend in oral peptide delivery is the development of muco-penetrating & mucus-modulating delivery devices. Muco-penetrating nanoparticles are specifically designed quickly diffuse through mucus & reach the epithelial surface, in contrast conventional mucoadhesive formulations that increase gastrointestinal residence duration but may retain peptides within the mucus layer. Surface modification with hydrophilic polymers, like polyethylene glycol, improves epithelial access & decreases sticky interactions with mucus components. In preclinical research, these systems have shown increased absorption consistency & decreased interindividual variability, underscoring their potential improve oral peptide delivery reliability [91].In order provide site-specific & regulated release of peptide therapies after oral administration, stimuli-responsive delivery devices are also being actively investigated. In order start drug release at the best absorption locations, these systems are made react physiological triggers such changes in pH, enzyme activity, or redox conditions within the gastrointestinal tract [92]. Stimuli-responsive formulations can improve absorption efficiency while reducing premature breakdown in harsh gastrointestinal environments by coordinating peptide release with advantageous local physiological conditions. These intelligent delivery methods are a major step wards precision oral peptide therapy & have great potential increase the efficacy & dependability of biologics taken orally [93].Device-assisted oral administration systems that physically get beyond restrictions on epithelial permeability are among the more revolutionary strategies. Early-stage research has shown encouraging results for ingestible devices that may orient themselves within the gastrointestinal tract & deliver peptide therapies straight across the mucosal barrier. These methods provide the possibility of greater & more reliable systemic bioavailability by doing away with the need for chemical permeation enhancement or passive diffusion. Widespread clinical adoption is still hampered by serious issues with patient acceptance, cost-effectiveness, manufacturing scalability, & device complexity [94].Lastly, AI-assisted formulation design & computer modelling are becoming effective methods for improving oral peptide delivery systems. Key factors including peptide stability, epithelial permeability, & drug–excipient interactions can be predicted by machine learning & data-driven models, which speeds up formulation development & lessens the need for experimental trial-&-error methods [95]. Future oral glucagon like peptide-1 receptor agonist formulations is anticipated be rationally designed & optimised through the integration of in silico modelling with experimental & clinical data, allowing for more effective, reliable, & patient-centered delivery methods [96].
7. Regulatory & Quality Considerations for Oral GLUCAGON LIKE PEPTIDE-1 Receptor Agonist Formulations
Because of their peptide composition, intricate formulation techniques, & dependence on absorption-enhancing technologies, the development of oral glucagon like peptide-1 receptor agonists poses particular regulatory & quality problems. Regulatory bodies, including significant international organisations, demand a thorough assessment of these products' safety, effectiveness, & quality characteristics, going above & beyond what is usually required for traditional small-molecule oral medications [97]. Because oral peptide therapies are more complex, special attention is paid the safety of novel excipients, long-term exposure permeation enhancers, formulation resilience, & consistency of clinical performance [98].
The safety of excipients & permeation enhancers used increase oral absorption is a key regulatory concern in the development of orally administered glucagon like peptide-1 receptor agonists. Regulatory bodies need thorough explanations of the mechanism of action, reversibility, & long-term safety of oral glucagon like peptide-1 receptor agonist formulations since many of them rely on excipients that momentarily change membrane permeability or epithelial integrity [99]. Long-term clinical safety studies & comprehensive non-clinical toxicology evaluations are required support regulatory approval of such excipients due concerns about epithelial damage, local inflammation, & possible changes in gastrointestinal function [100].Glucagon like peptide-1 receptor agonists & other oral peptide formulations should be developed using Quality-by-Design (QbD) principles. Peptide integrity, impurity profile, stability under gastrointestinal circumstances, & batch-batch uniformity are examples of critical quality qualities that need be precisely defined & strictly regulated. Regulatory bodies place special emphasis on thorough knowledge & control of degradation pathways like hydrolysis, oxidation, aggregation, & enzymatic cleavage throughout the whole product lifecycle, from manufacture clinical use, because peptide therapeutics are inherently physicochemically unstable [101].Pharmacokinetic variability is a significant regulatory problem for oral glucagon like peptide-1 receptor agonist formulations from the standpoint of bioavailability. Due variations in gastrointestinal physiology, stomach emptying rates, digestive enzyme activity, & patient adherence particular dosage circumstances, these products often show substantial inter- & intra-subject variability. Therefore, in order ensure dependable clinical performance, regulatory authorities require well-designed clinical pharmacokinetic & pharmacodynamic studies show consistent exposure–response relationships & justify dosing instructions, including fasting requirements & food & water intake restrictions [102].Immunogenicity testing is another crucial regulatory factor in the creation of oral glucagon like peptide-1 receptor agonists. Despite the fact that glucagon like peptide-1 receptor agonists typically have a low intrinsic immunogenic potential, oral administration may pose extra dangers because of partial peptide degradation, chemical modification, or the creation of new peptide-related contaminants. In order guarantee long-term safety & identify any clinically significant immune reactions connected long-term oral administration, regulatory rules require thorough immunogenicity investigation throughout clinical development as well as ongoing post-marketing surveillance [103].
CONCLUSION
Glucagon like peptide-1 receptor agonist oral administration is a significant advancement in peptide-based treatments, providing a patient-friendly substitute for injectable formulations & resolving persistent adherence issues. Recent developments have shown that clinically significant therapeutic efficacy can be attained through logical formulation design & optimised dosing strategies, even with low absolute oral bioavailability, despite significant biological & physicochemical barriers, such as enzymatic degradation, poor epithelial permeability, mucus entrapment, & extensive first-pass metabolism. Successful oral administration has been made possible by advances in formulation science, particularly the use of absorption enhancers, multifunctional excipient systems, nanotechnology-based carriers, & gastroretentive techniques.However, stringent dosage guidelines, interindividual pharmacokinetic variability, & safety concerns over long-term exposure permeation-enhancing excipients continue restrict currently authorised formulations. Peptide structural engineering, muco-penetrating systems, stimuli-responsive platforms, device-assisted delivery, & artificial intelligence-guided formulation design are examples of emerging technologies that are anticipated further progress the field wards oral peptide therapies that are safer, more reliable, & patient-centered.From a regulatory standpoint, early regulatory involvement, thorough safety review, & strict application of Quality-by-Design principles are necessary for successful development. All things considered, the advancements made with oral Glucagon like peptide-1 receptor agonists will probably influence the creation of non-injectable biologics in the future & alter expectations regarding the oral administration of complex peptide treatments.
REFERENCES
https://doi.org/10.1016/j.molmet.2021.101351
https://doi.org/10.1016/j.molmet.2019.09.010
https://doi.org/10.3390/ijms23073451
https://doi.org/10.1111/bph.15462
https://doi.org/10.2147/PPA.S463354
https://doi.org/10.1007/s11136-021-02808-2
https://doi.org/10.1038/s41392-024-02107-5
https://doi.org/10.3390/pharmaceutics16111353
https://doi.org/10.1002/ddr.21404
10.1016/j.addr.2021.03.011
https://doi.org/10.1093/bjsopen/zrad077
https://doi.org/10.1038/s41598-021-01750-0
https://doi.org/10.1111/bph.15647
https://doi.org/10.3390/biom15050622
https://doi.org/10.3389/fendo.2022.863184
10.1186/s12902-022-01036-0
https://doi.org/10.2147/DDDT.S506957
https://doi.org/10.1007/s11154-022-09735-8
10.1002/oby.21107
10.2196/69466
https://doi.org/10.2147/DDDT.S166765
https://doi.org/10.4155/ppa.14.15
https://doi.org/10.1016/j.apsb.2025.10.026
10.34172/apb.2024.009
https://doi.org/10.1080/17576180.2025.2535954
https://doi.org/10.1002/ddr.21832
https://doi.org/10.1007/s13346-025-01978-7
10.3748/wjg.v30.i23.2964
https://doi.org/10.1016/j.jconrel.2020.05.030
https://doi.org/10.1016/j.ijpharm.2018.09.055
https://doi.org/10.3390/molecules25194479
https://doi.org/10.1371/journal.pone.0128065
https://doi.org/10.3390/membranes9110153
https://doi.org/10.1002/j.2040-4603.2018.tb00025.x
https://doi.org/10.1016/j.addr.2023.114966
https://doi.org/10.3390/cimb43030113
https://doi.org/10.1038/s41573-019-0053-0
https://doi.org/10.3390/ijms25020815
https://doi.org/10.2337/cd22-0118
https://doi.org/10.1080/17425247.2022.2051476
https://doi.org/10.1080/1061186X.2023.2271680
https://doi.org/10.3390/antib11010001
https://doi.org/10.1016/j.bmc.2017.08.028
https://doi.org/10.3390/scipharm93020026
https://doi.org/10.1186/s12951-025-03677-4
doi: 10.34172/apb.2024.016
10.5958/0974-360X.2021.00098.6
https://doi.org/10.1016/j.jconrel.2018.08.032
DOI: 10.2174/1381612821666150531163944
https://doi.org/10.1007/s10989-021-10193-0
https://doi.org/10.1016/j.nxnano.2025.100195
https://doi.org/10.1016/bs.pmbts.2024.11.003
https://doi.org/10.1021/mp500809f
https://doi.org/10.1016/j.apsb.2019.01.004
https://doi.org/10.1016/j.drudis.2021.01.020
https://doi.org/10.4155/tde-2020-0068
https://doi.org/10.1080/1061186X.2021.1894434
10.1055/s-0035-1559654
https://doi.org/10.1111/bcp.12557
https://doi.org/10.1111/imm.12622Digital Object Identifier (DOI)
https://doi.org/10.1007/s40262-018-0668-z
https://doi.org/10.1007/s42000-023-00488-w
https://doi.org/10.1210/clinem/dgae719
https://doi.org/10.1080/17425247.2021.1942838
https://doi.org/10.3390/pharmaceutics13101722
https://doi.org/10.1007/s10989-025-10763-6
doi: 10.24870/cjb.2017-000107
https://doi.org/10.1038/srep18039
10.1211/PJ.20202 07874.
https://doi.org/10.3390/ph18101498
https://doi.org/10.1007/s42114-024-01053-8
https://doi.org/10.1080/17425247.2021.1825375
https://doi.org/10.1016/j.molmet.2021.101351
https://doi.org/10.1016/j.molmet.2019.09.010
https://doi.org/10.3390/ijms23073451
https://doi.org/10.1111/bph.15462
https://doi.org/10.2147/PPA.S463354
https://doi.org/10.1007/s11136-021-02808-2
https://doi.org/10.1038/s41392-024-02107-5
https://doi.org/10.3390/pharmaceutics16111353
https://doi.org/10.1002/ddr.21404
10.1016/j.addr.2021.03.011
https://doi.org/10.1093/bjsopen/zrad077
https://doi.org/10.1038/s41598-021-01750-0
https://doi.org/10.1111/bph.15647
https://doi.org/10.3390/biom15050622
https://doi.org/10.3389/fendo.2022.863184
10.1186/s12902-022-01036-0
https://doi.org/10.2147/DDDT.S506957
https://doi.org/10.1007/s11154-022-09735-8
10.1002/oby.21107
10.2196/69466
https://doi.org/10.2147/DDDT.S166765
https://doi.org/10.4155/ppa.14.15
https://doi.org/10.1016/j.apsb.2025.10.026
10.34172/apb.2024.009
https://doi.org/10.1080/17576180.2025.2535954
https://doi.org/10.1002/ddr.21832
https://doi.org/10.1007/s13346-025-01978-7
10.3748/wjg.v30.i23.2964
https://doi.org/10.1016/j.jconrel.2020.05.030
https://doi.org/10.1016/j.ijpharm.2018.09.055
https://doi.org/10.3390/molecules25194479
https://doi.org/10.1371/journal.pone.0128065
https://doi.org/10.3390/membranes9110153
https://doi.org/10.1002/j.2040-4603.2018.tb00025.x
https://doi.org/10.1016/j.addr.2023.114966
https://doi.org/10.3390/cimb43030113
https://doi.org/10.1038/s41573-019-0053-0
https://doi.org/10.3390/ijms25020815
https://doi.org/10.2337/cd22-0118
https://doi.org/10.1080/17425247.2022.2051476
https://doi.org/10.1080/1061186X.2023.2271680
https://doi.org/10.3390/antib11010001
https://doi.org/10.1016/j.bmc.2017.08.028
https://doi.org/10.3390/scipharm93020026
https://doi.org/10.1186/s12951-025-03677-4
doi: 10.34172/apb.2024.016
10.5958/0974-360X.2021.00098.6
https://doi.org/10.1016/j.jconrel.2018.08.032
DOI: 10.2174/1381612821666150531163944
https://doi.org/10.1007/s10989-021-10193-0
https://doi.org/10.1016/j.nxnano.2025.100195
https://doi.org/10.1016/bs.pmbts.2024.11.003
https://doi.org/10.1021/mp500809f
https://doi.org/10.1016/j.apsb.2019.01.004
https://doi.org/10.1016/j.drudis.2021.01.020
https://doi.org/10.4155/tde-2020-0068
https://doi.org/10.1080/1061186X.2021.1894434
10.1055/s-0035-1559654
https://doi.org/10.1111/bcp.12557
https://doi.org/10.1111/imm.12622Digital Object Identifier (DOI)
https://doi.org/10.1007/s40262-018-0668-z
https://doi.org/10.1007/s42000-023-00488-w
https://doi.org/10.1210/clinem/dgae719
https://doi.org/10.1080/17425247.2021.1942838
https://doi.org/10.3390/pharmaceutics13101722
https://doi.org/10.1007/s10989-025-10763-6
doi: 10.24870/cjb.2017-000107
https://doi.org/10.1038/srep18039
10.1211/PJ.20202 07874.
https://doi.org/10.3390/ph18101498
https://doi.org/10.1007/s42114-024-01053-8
https://doi.org/10.1080/17425247.2021.1825375




Patil Rajvardhan, Patil Snehit, Kadam Swapnil, Sulgudle Shivraj, Dr. Gejage Santosh, Oral Delivery Challenges & Formulation Strategies for Glucagon Like Peptide-1 Receptor Agonists, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1819-1841. https://doi.org/10.5281/zenodo.18620126
 10.5281/zenodo.18620126
10.5281/zenodo.18620126