
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Periodontology and Oral Implantology, National Dental College and Hospital, Dera Bassi, Punjab, India.
INTRODUCTION: Chronic periodontitis is an inflammatory disease-causing destruction of the supporting structures of the teeth, leading to periodontal pocket formation and attachment loss. Scaling and Root Planing (SRP) is the gold standard non-surgical periodontal therapy; however, residual periodontal pathogens may limit its effectiveness. Natural herbal agents with antimicrobial, antioxidant, and anti-inflammatory properties are increasingly being used as adjuncts to periodontal therapy. Grape Seed Extract (GSE), derived from Vitis vinifera, possesses antioxidant and collagen-protective properties that may enhance periodontal healing. Therefore, the present study was conducted to evaluate the efficacy of GSE as an adjunct to SRP in the management of chronic periodontitis using clinical periodontal parameters. AIMS AND OBJECTIVE:1. To assess the efficacy of Grape seed extract in the treatment of Stage II Grade B periodontitis. 2. To clinically compare and evaluate the reduction in periodontal pockets with Scaling and Root Planing + Placebo and Scaling and Root Planing + Grape Seed Extract in cases of Stage II Grade B periodontitis. MATERIALS AND METHODS: A randomized clinical study was conducted on 10 patients (20 sites) aged 18–50 years, with two sites selected per patient. The sites were divided into two groups: Test group – scaling and root planing (SRP) + grape seed extract (GSE), and Control group – SRP + placebo. Clinical parameters including Gingival Index (GI) by Loe and Silness (1963), Plaque Index (PI) by Silness and Loe (1964), Probing Pocket Depth (PPD), and Clinical Attachment Level (CAL) were recorded at baseline, day 7, and day 28. GSE (97% concentration; BRM Herbals) with a pH of 5.85 was diluted to 2000 µg/mL. The freshly prepared solution was delivered into the periodontal pocket using a syringe with a blunt cannula. RESULTS: Both groups showed reduced plaque and gingival index scores from baseline to day 7. Only the Grape Seed Extract group showed significant improvement in probing depth and clinical attachment level from baseline to 28 days. CONCLUSION: The study seeks to establish whether adjunctive use of Grape Seed Extract with Scaling and Root Planing provides superior clinical outcomes compared to SRP alone, potentially offering a safe and effective herbal therapeutic strategy in periodontal disease management.
Chronic periodontitis is a multifactorial inflammatory disease characterized by progressive destruction of the supporting structures of the teeth, including gingiva, periodontal ligament, cementum, and alveolar bone. The disease is initiated by microbial dental plaque and modified by the host immune-inflammatory response, which may ultimately lead to tooth mobility and tooth loss if untreated. Mariotti A and Hefti defined periodontal health as the absence of clinically detectable inflammation with stable periodontal attachment.¹
Non-surgical periodontal therapy (NSPT), particularly Scaling and Root Planing (SRP), is considered the gold standard treatment for chronic periodontitis. SRP removes supra- and subgingival plaque, calculus, and diseased cementum, thereby reducing microbial load and inflammation. Cobb CM highlighted the effectiveness of SRP in improving periodontal parameters, while Aimetti M emphasized the importance of mechanical debridement in controlling periodontal disease progression.²˒³ However, certain periodontal pathogens such as Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans, Treponema denticola, and Tannerella forsythia may persist within periodontal tissues despite therapy. Das AC and colleagues demonstrated the significant role of periodontal pathogens in disease progression, thereby supporting the need for adjunctive therapeutic approaches.⁶
To improve treatment outcomes, various adjunctive therapies such as antimicrobials, host modulation agents, essential oils, platelet-rich plasma, and herbal products have been introduced. Das AC reported beneficial effects of adjunctive doxycycline in periodontal therapy.⁴ Similarly, Azad MF and Ameer LA demonstrated improved periodontal healing with adjunctive therapies.⁷˒⁸
Natural herbal agents have gained attention because of their antimicrobial, antioxidant, and anti-inflammatory properties with minimal side effects. Nagasri M showed that curcumin improved periodontal outcomes, while Moghaddam AA demonstrated beneficial effects of Aloe vera gel as an adjunct to SRP.⁹˒¹⁰
Grape Seed Extract (GSE), derived from Vitis vinifera, is rich in polyphenols and proanthocyanidins with potent antioxidant, antimicrobial, and anti-inflammatory properties. GSE inhibits matrix metalloproteinases, protects collagen from degradation, suppresses osteoclastic activity, and promotes tissue healing. Owing to these properties, GSE may serve as a promising adjunct to SRP in improving periodontal healing and clinical outcomes. Therefore, the present study was designed to evaluate the efficacy of GSE as an adjunct to SRP in chronic periodontitis treatment.
MATERIALS AND METHODS
SOURCE OF DATA
A total of 10 patients were selected from the Outpatient Department of Periodontology and Oral Implantology, National Dental College and Hospital, Dera Bassi, Punjab, India. Each patient was given a detailed verbal and written description of study . Before starting the study, ethical approval from the institutional review board of National Dental College, Dera Bassi was obtained for conducting the study.
INCLUSION CRITERIA
EXCLUSION CRITERIA
METHODOLOGY
At the beginning of the study, 10 patients diagnosed with Stage II Grade B periodontitis were randomly divided into two groups with 10 patients/20 sites in each group.
Test Site -10 patients treated with scaling and root planing along with placement of grape seed extract into deepest periodontal pocket
Control Site - 10 patients treated with scaling and root planing along with placebo.
Preparation of Grape Seed Extract
Grape Seed Extract (pH 5.85) was available at a concentration of 97% (GSE liquid, BRM Herbals) and was further diluted to the concentration of 2000 µg/mL.
After scaling and root planning, the test site was treated with freshly prepared mixture of diluted grape seed extract. The grape seed extract was delivered to the deepest periodontal pocket using a syringe with blunt canula. Periodontal dressing (Coe-Pak) was placed and re-application of diluted grape seed extract was done in a similar manner after one week (7th day).
The control site was treated with scaling and root planning along with along with placement of placebo into the deepest periodontal pocket.
CLINICAL PARAMETERS
The following clinical parameters was recorded at baseline, 7th day, 28th day in both the sites:
STATISTICAL ANALYSIS
The parameters were tabulated and put to statistical analysis. The data for the present study were analysed using SPSS Statistical software 23.0 version. The intergroup comparison for the difference of mean score between the groups was done using independent t tests whereas the intra group comparison was done using paired t-test. The Shapiro–Wilk test was used to investigate the distribution of the data and Levene’s test to explore the homogeneity of the variables.
RESULTS
TABLE 1: INTERGROUP COMPARISION OF ALL CLINICAL PARAMETERS IN BWTWEEN TEST AND CONTROL GROUP AT VARIOUS TIME INTERVAL
|
Time Interval |
Gingival Index (GI) |
Plaque Index (PI) |
Probing Pocket Depth (PPD) |
Clinical Attachment Level (CAL) |
|
Baseline |
Control: 1.36 ± 0.09 Test: 1.36 ± 0.09 |
Control: 1.25 ± 0.11 Test: 1.25 ± 0.11 |
Control: 5.00 ± 0.11 Test: 5.00 ± 0.11 |
Control: 5.20 ± 1.03 Test: 5.20 ± 1.03 |
|
7th Day |
Control: 1.04 ± 0.08 Test: 1.04 ± 0.08 |
Control: 1.06 ± 0.12 Test: 1.06 ± 0.12 |
Control: 5.00 ± 0.12 Test: 4.00 ± 0.12 |
Control: 5.20 ± 1.03 Test: 4.60 ± 0.63 |
|
28th Day |
Control: 1.04 ± 0.08 Test: 1.04 ± 0.08 |
Control: 1.06 ± 0.12 Test: 1.06 ± 0.12 |
Control: 5.00 ± 0.12 Test: 4.00 ± 0.12 |
Control: 5.20 ± 1.03 Test: 4.60 ± 0.63 |
|
P Value |
1.000** |
1.000** |
0.001* |
0.001* |
Control Group – SRP + Placebo, Test Group – SRP + GSE
* Significant, ** Non-significant
RESULTS FOR INTERGROUP COMPARISION:
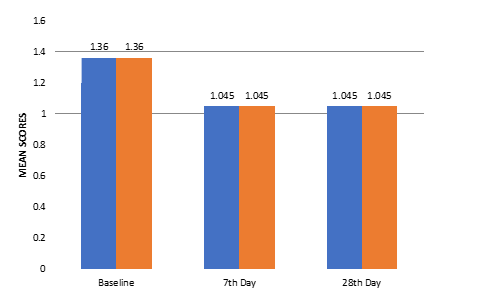
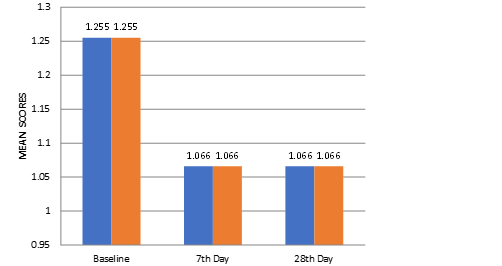
Intergroup comparison of clinical parameters between the Control Group (SRP + Placebo) and Test Group (SRP + GSE) showed no statistically significant difference in Gingival Index (GI) and Plaque Index (PI) scores at baseline, 7th day, and 28th day (P = 1.000).
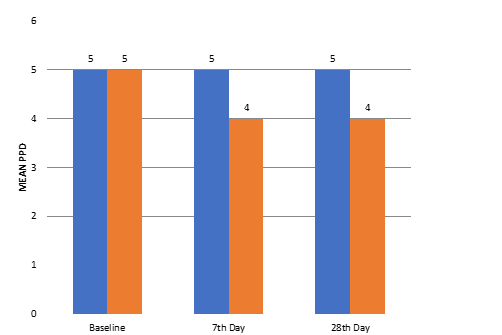
For Probing Pocket Depth (PPD), both groups showed similar values at baseline with no significant difference (P = 1.000). However, at the 7th day and 28th day, the Test Group demonstrated a statistically significant reduction in PPD compared to the Control Group (P = 0.001).
Similarly, Clinical Attachment Level (CAL) showed no significant difference between the groups at baseline (P = 1.000), whereas significant improvement was observed in the Test Group at the 7th day and 28th day compared to the Control Group (P = 0.001).
GRAPH 1: INTERGROUP COMPARISON OF GINGIVAL INDEX SCORES BETWEEN THE GROUPS AT DIFFERENT TIME INTERVALS
GRAPH 2: INTERGROUP COMPARISON OF PLAQUE INDEX SCORES BETWEEN THE GROUPS AT DIFFERENT TIME INTERVALS
GRAPH 3: INTERGROUP COMPARISON OF PROBING POCKET DEPTH BETWEEN THE GROUPS AT DIFFERENT TIME INTERVALS
GRAPH 4: INTERGROUP COMPARISON CAL BETWEEN THE GROUPS AT DIFFERENT TIME INTERVALS
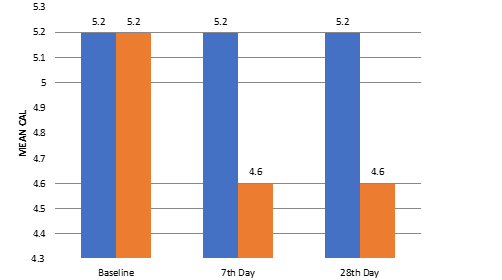
TABLE 2: INTRAGROUP COMPARIOSN OF GINGIVAL INDEX SCORES BETWEEN THE TIME INTERVALS
|
|
Time Interval |
Mean ± Std. Deviation |
Std. Error Mean |
P value |
|
Control Group |
Baseline |
1.36 ± 0.09 |
0.02963 |
|
|
7th Day |
1.04 ± 0.08 |
0.02630 |
< 0.001* |
|
|
28th Day |
1.04 ± 0.08 |
0.02630 |
= 1.000** |
|
|
Test Group |
Baseline |
1.36 ± 0.09 |
0.02963 |
|
|
7th Day |
1.04 ± 0.08 |
0.02630 |
< 0.001* |
|
|
28th Day |
1.04 ± 0.08 |
0.02630 |
= 1.000** |
* - Significant, ** - Non-significant
TABLE 3: INTRAGROUP COMPARIOSN OF PLAQUE INDEX SCORES BETWEEN THE TIME INTERVALS
|
|
Time Interval |
Mean ± Std. Deviation |
Std. Error Mean |
P value |
|
Control Group |
Baseline |
1.25 ± 0.11 |
.03686 |
|
|
7th Day |
1.06 ± 0.12 |
.03945 |
< 0.001* |
|
|
28th Day |
1.06 ± 0.12 |
.03945 |
= 1.000** |
|
|
Test Group |
Baseline |
1.25 ± 0.11 |
.03686 |
|
|
7th Day |
1.06 ± 0.12 |
.03945 |
< 0.001* |
|
|
28th Day |
1.06 ± 0.12 |
.03945 |
= 1.000** |
* - Significant, ** - Non-significant
TABLE 4: INTRAGROUP COMPARIOSN OF PROBING POCKET DEPTH BETWEEN THE TIME INTERVALS
|
|
Time Interval |
Mean ± Std. Deviation |
Std. Error Mean |
P value |
|
Control Group |
Baseline |
5.00 ± 0.11 |
0.036 |
|
|
7th Day |
5.00 ± 0.11 |
0.036 |
= 1.000** |
|
|
28th Day |
5.00 ± 0.11 |
0.036 |
= 1.000** |
|
|
Test Group |
Baseline |
5.00 ± 0.11 |
0.036 |
|
|
7th Day |
4.00 ± 0.12 |
0.039 |
< 0.001* |
|
|
28th Day |
4.00 ± 0.12 |
0.039 |
= 1.000** |
* - Significant, ** - Non-significant
TABLE 5: INTRAGROUP COMPARIOSN OF CAL BETWEEN THE TIME INTERVALS
|
|
Time Interval |
Mean ± Std. Deviation |
Std. Error Mean |
P value |
|
Control Group |
Baseline |
5.20 ± 1.03 |
0.326 |
|
|
7th Day |
5.20 ± 1.03 |
0.326 |
= 1.000** |
|
|
28th Day |
5.20 ± 1.03 |
0.326 |
= 1.000* |
|
|
Test Group |
Baseline |
5.20 ± 1.03 |
0.326 |
|
|
7th Day |
4.60 ± 0.63 |
0.200 |
< 0.001* |
|
|
28th Day |
4.60 ± 0.63 |
0.200 |
= 1.000** |
* - Significant, ** - Non-significant
RESULTS FOR INTRAGROUP COMPARISION:
In the intragroup comparison, both the Control Group and Test Group showed a statistically significant reduction in Gingival Index (GI) and Plaque Index (PI) scores from baseline to the 7th day (P < 0.001). However, no statistically significant difference was observed between the 7th day and 28th day scores (P = 1.000), indicating maintenance of improvement.
For Probing Pocket Depth (PPD), the Control Group did not show any statistically significant change throughout the study period (P = 1.000). In contrast, the Test Group exhibited a statistically significant reduction in PPD from baseline to the 7th day (P < 0.001), while no further significant change was observed between the 7th day and 28th day (P = 1.000).
Regarding Clinical Attachment Level (CAL), the Control Group showed no statistically significant improvement during the study period (P = 1.000). The Test Group demonstrated a statistically significant gain in CAL from baseline to the 7th day (P < 0.001), with no further statistically significant change between the 7th day and 28th day (P = 1.000).
DISCUSSION
The present study evaluated the effectiveness of Scaling and Root Planing (SRP) with and without adjunctive Grape Seed Extract (GSE) in the management of chronic periodontitis by assessing Gingival Index (GI), Plaque Index (PI), Probing Pocket Depth (PPD), and Clinical Attachment Level (CAL) at baseline, 7th day, and 28th day. The findings demonstrated that both groups showed improvement after treatment; however, the adjunctive use of GSE produced superior outcomes in periodontal pocket reduction and attachment gain.
The Gingival Index scores showed a significant reduction within both the control and test groups from baseline to the 7th day, indicating that SRP effectively reduced gingival inflammation. However, intergroup comparison revealed no statistically significant difference between the groups at any time interval (P = 1.000). These findings suggest that the addition of GSE did not provide any additional benefit over SRP alone in reducing gingival inflammation. Similar observations were reported by Cobb CM, who demonstrated that non-surgical periodontal therapy alone can substantially reduce gingival inflammation and improve periodontal health.⁵ Likewise, the findings are in accordance with the concept of periodontal health described by Mariotti A and Hefti, who emphasized the role of effective plaque control and mechanical debridement in resolving gingival inflammation.¹
Similarly, Plaque Index scores significantly decreased within both groups from baseline to the 7th day, but no statistically significant intergroup difference was observed throughout the study period. This indicates that both SRP + placebo and SRP + GSE were equally effective in reducing plaque accumulation, and GSE did not exhibit any additional plaque inhibitory effect. These findings are comparable with the study conducted by Aimetti M, who emphasized that meticulous SRP remains the cornerstone of plaque control and periodontal therapy.³
In contrast, Probing Pocket Depth (PPD) showed a statistically significant improvement in the test group receiving SRP + GSE. While the control group demonstrated no reduction in mean pocket depth throughout the study period, the test group exhibited a reduction from 5 mm at baseline to 4 mm by the 7th day, which was maintained up to the 28th day (P = 0.001). This finding suggests that GSE may enhance periodontal healing and tissue response when used adjunctively with SRP. Similar adjunctive benefits of host modulatory agents have been reported by Das AC and colleagues, where adjunctive therapy enhanced periodontal treatment outcomes beyond conventional SRP alone.⁴ Additionally, the anti-inflammatory effects observed in the present study are supported by the work of Ameer LA et al., who demonstrated that adjunctive anti-inflammatory therapies can improve periodontal pocket healing.⁸
Clinical Attachment Level (CAL) also showed significant improvement in the test group. The mean CAL reduced from 5.2 mm at baseline to 4.6 mm on the 7th and 28th day, whereas the control group showed no improvement. The statistically significant intergroup difference (P = 0.001) indicates that adjunctive GSE promoted better periodontal attachment gain than SRP alone. These results may be attributed to the collagen-stabilizing and antioxidant effects of proanthocyanidins present in grape seed extract, which are known to enhance tissue repair and reduce oxidative stress. Similar improvements in clinical attachment with adjunctive herbal therapies have been reported by Nagasri M et al., who observed enhanced periodontal healing with curcumin adjunctive therapy. ⁹ Likewise, Moghaddam AA and colleagues demonstrated that herbal adjuncts such as Aloe vera can significantly improve periodontal parameters when combined with SRP. ¹⁰
The results of the present study support the growing interest in adjunctive natural therapeutic agents in periodontal therapy. GSE possesses potent antioxidant, antimicrobial, and anti-inflammatory properties, which may help modulate the host response and promote periodontal healing. Although improvements in GI and PI were comparable between groups, the significant reduction in PPD and gain in CAL observed in the test group suggest that GSE may positively influence deeper periodontal tissue healing rather than merely reducing superficial inflammation or plaque accumulation.
However, the study has certain limitations. The sample size was relatively small, and the follow-up period was limited to 28 days. Long-term studies with larger populations are required to confirm the sustained benefits of GSE in chronic periodontitis management. Furthermore, microbiological and biochemical parameters were not evaluated, which could have provided additional evidence regarding the mechanism of action of GSE.
CONCLUSION
Within the limitations of the present clinical trial, it can be concluded that Grape Seed Extract, when used as an adjunct to Scaling and Root Planing, provides additional clinical benefits in the management of periodontitis compared to SRP alone. The antioxidant, antimicrobial, and anti-inflammatory properties of GSE appear to contribute to improved periodontal healing and reduction in pocket depth.
GSE may thus serve as a promising, safe, and cost-effective adjunctive agent in non-surgical periodontal therapy. Further long-term and multicenter studies are recommended to establish its role as a standard adjunct in periodontal treatment protocols.
REFERENCES


Dr. Numrah Haque, Dr. Rakshita Sharma, Dr. Navneet Kaur, Dr. Gurpreet Kaur, Clinical Efficacy of Grape Seed Extract as an Adjuvant to Scaling and Root Planing in Treatment of Stage II Grade B Periodontitis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 886-894. https://doi.org/10.5281/zenodo.20530051
 10.5281/zenodo.20530051
10.5281/zenodo.20530051