
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Yashodeep Institute of Pharmacy, Chh. Sambhajinagar
Anemia is the world's most prevalent nutritional disorder, affecting an estimated 1.62 billion people approximately 24.8% of the global population across all age groups, genders, and geographic regions. It is defined as a reduction in the concentration of hemoglobin, the oxygen-carrying red blood pigment, below the World Health Organization threshold values of 13 g/dL in adult men, 12 g/dL in non-pregnant adult women, and 11 g/dL in pregnant women and children aged 6 months to 5 years. Iron deficiency anemia (IDA) accounting for approximately 50% of all anemia cases globally is the single most common micronutrient deficiency in the world, and represents the leading preventable cause of impaired cognitive development in children, reduced physical work capacity in adults, and adverse maternal and perinatal outcomes in pregnant women. India bears a disproportionately heavy burden of anemia the National Family Health Survey (NFHS-5, 2019–2021) revealed that 57% of children aged 6–59 months, 67% of women aged 15–49 years, and 25% of men aged 15–49 years in India are anemic. Despite the availability of oral iron supplementation, compliance rates remain persistently low due to the well-documented gastrointestinal adverse effects of conventional iron salts nausea, vomiting, abdominal pain, constipation, and black stools which represent the primary reason for treatment discontinuation. This has generated substantial scientific interest in developing natural, better-tolerated iron delivery alternatives. Urtica dioica Linn. (Stinging Nettle, Family: Urticaceae) is a perennial medicinal plant with one of the highest documented natural iron contents among edible plants 3.5–4.2 mg of iron per 100 g fresh weight, or up to 36 mg per 100 g dry weight in some analyses combined with uniquely high concentrations of Vitamin C (ascorbic acid), chlorophyll, carotenoids, and flavonoids that synergistically enhance the bioavailability and absorption of its naturally chelated iron. Its traditional use in Ayurvedic, Greek, European, and folk medicine systems for the treatment of anemia, fatigue, and blood building extends across multiple civilizations and millennia
Anemia
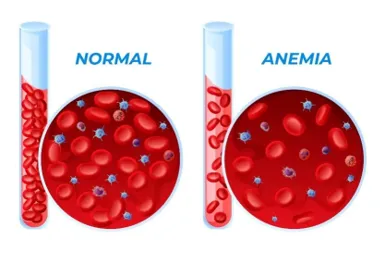
The word 'anemia' is derived from the Greek an- (without) and haima (blood) literally 'without blood' reflecting the ancient recognition of paleness, weakness, and debility as the most visible outward manifestations of a condition that has afflicted humanity across all civilizations and throughout recorded history. In modern clinical and public health terminology, anemia refers specifically to a reduction in the oxygen-carrying capacity of the blood measured by hemoglobin concentration, hematocrit, or red blood cell count falling below defined age- and sex-specific thresholds that results in tissue hypoxia and the consequent functional impairments of fatigue, reduced physical work capacity, impaired cognitive function, and in severe cases, cardiorespiratory compromise.
Anemia is without question the world's most prevalent nutritional and hematological disorder, with a global burden that is simultaneously staggering in its magnitude and urgently in need of more effective therapeutic solutions. The World Health Organization estimates that approximately 1.62 billion people 24.8% of the entire global population are anemic. This extraordinary prevalence places anemia ahead of virtually every other nutritional disorder, ahead of diabetes, ahead of hypertension, and among the leading causes of disability and reduced quality of life worldwide. Its effects span every dimension of human health physical, cognitive, reproductive, developmental, and economic making it one of the most consequential public health challenges of the 21st century.
Iron deficiency the most common nutritional deficiency in the world is responsible for approximately 50% of all anemia globally, and the combination of iron deficiency with or without anemia affects an estimated 2 billion people. Iron deficiency anemia is particularly prevalent in pre-school children (affecting 40–45% globally), pregnant women (38% globally), adolescent girls, and women of reproductive age populations characterized by high iron demands relative to dietary iron supply. The developmental consequences of iron deficiency anemia in children impaired motor development, reduced IQ, impaired school performance, and behavioral problems are partially irreversible even after iron repletion, making prevention and early treatment of paramount importance.
In India, anemia represents one of the most persistent and severe public health challenges despite decades of national nutrition programs. The National Family Health Survey 5 (NFHS-5, 2019–2021) the most recent nationally representative nutrition survey found that 57% of Indian children aged 6–59 months were anemic, 67% of women aged 15–49 years were anemic (an increase from 53% in NFHS-4), and 25% of Indian men aged 15–49 years were anemic. These numbers reflect the persistence of iron deficiency anemia despite the availability of conventional iron supplementation programs and point directly to the critical role of poor compliance with conventional iron supplements, driven by their notorious gastrointestinal adverse effects, as a major factor in treatment failure.
Types of Anemia:
a) Iron Deficiency Anemia (IDA):
Iron deficiency anemia is the most prevalent form globally accounting for approximately 50% of all anemia cases and the primary target of the Urtica dioica suspension formulated in this work. It results from an imbalance between iron supply (dietary absorption) and iron demand (erythropoiesis, growth, menstrual loss, pregnancy), producing progressive iron store depletion followed by impaired hemoglobin synthesis and microcytic, hypochromic anemia. Laboratory hallmarks: low hemoglobin, low MCV (< 80 fL), low MCH (< 27 pg), low serum ferritin (< 12 ng/mL), low transferrin saturation (< 16%), elevated TIBC, elevated sTfR. Clinical features: fatigue, pallor, dyspnoea on exertion, pica (craving non-food items), brittle nails (koilonychia), glossitis, angular stomatitis, and Plummer-Vinson syndrome in severe chronic cases.
b) Vitamin B12 Deficiency Anemia (Megaloblastic Anemia):
Vitamin B12 deficiency impairs DNA synthesis in rapidly dividing cells particularly erythroid precursors in the bone marrow producing the characteristic megaloblastic morphology: large, immature erythroid precursors with nuclear-cytoplasmic asynchrony (cytoplasm matures normally while nuclear maturation is arrested). The result is macrocytic anemia (MCV > 100 fL), hypersegmented neutrophils (> 5 lobes), and reticulocytopenia. Causes include strict vegetarianism (Vitamin B12 is found only in animal products), pernicious anemia (autoimmune destruction of gastric parietal cells eliminating intrinsic factor), gastrectomy, ileal disease, and prolonged metformin or proton pump inhibitor use.
c) Anemia of Chronic Disease (ACD):
Anemia of chronic disease also termed anemia of inflammation is the second most common anemia globally and the most common anemia in hospitalized patients. It occurs in the setting of chronic infections, inflammatory diseases (rheumatoid arthritis, SLE, inflammatory bowel disease), malignancies, and chronic kidney disease. The mechanism involves hepcidin upregulation by inflammatory cytokines (particularly IL-6) hepcidin degrades ferroportin, locking iron in macrophage stores and reducing intestinal iron absorption producing a 'functional iron deficiency' despite normal or elevated total body iron. ACD is normocytic or mildly microcytic with low serum iron, low TIBC, and elevated ferritin (differentiating it from true IDA).
d) Megaloblastic Anemia (Folate Deficiency):
Folate deficiency produces identical morphological changes to Vitamin B12 deficiency (megaloblastic anemia) through the same mechanism impairment of DNA synthesis due to inadequate 5,10-methylene-tetrahydrofolate for thymidylate synthesis. Unlike B12 deficiency, folate deficiency does NOT cause neurological complications. Causes include inadequate dietary intake (alcoholism, malnutrition), malabsorption (coeliac disease), increased demand (pregnancy, haemolytic anemia, rapid growth), and drug-induced (methotrexate, trimethoprim, phenytoin). Urtica dioica is a moderate source of dietary folate that can contribute to preventing folate-deficiency anemia alongside its iron-delivering properties.
e) Hemolytic Anemia:
Hemolytic anemias result from premature destruction of red blood cells at a rate exceeding the bone marrow's compensatory erythropoietic capacity. They are classified by the site of destruction (intravascular vs. extravascular), the mechanism (immune-mediated vs. non-immune), and the defect location (intrinsic within the RBC vs. extrinsic outside the RBC). Common causes include G6PD deficiency, hereditary spherocytosis, sickle cell disease, autoimmune hemolytic anemia, malaria, and traumatic hemolysis (prosthetic heart valves, TTP). Laboratory hallmarks: elevated reticulocyte count, elevated LDH, elevated indirect bilirubin, low haptoglobin, and positive direct antiglobulin test (DAT) in immune-mediated cases.
f) Aplastic Anemia:
Aplastic anemia is a potentially life-threatening bone marrow failure syndrome characterized by pancytopenia (anemia, leukopenia, and thrombocytopenia) and a hypocellular bone marrow devoid of normal hematopoietic precursors reflecting destruction or suppression of hematopoietic stem cells. Most cases (70–80%) are immune-mediated autoreactive T cells attacking hematopoietic stem cells while secondary causes include radiation, chemotherapy, toxins (benzene, chloramphenicol), viral infections (hepatitis viruses, EBV, HIV), and inherited bone marrow failure syndromes (Fanconi anemia).
g) Sickle Cell Anemia:
Sickle cell anemia is the most common severe monogenic disease worldwide, caused by a single missense mutation in the beta-globin gene (Glu6Val) producing the abnormal hemoglobin HbS. Under conditions of hypoxia, dehydration, or acidosis, HbS polymerizes within red blood cells, causing them to deform into the characteristic rigid, sickle-shaped morphology that impairs their passage through small blood vessels, causing painful vascular occlusive crises, chronic hemolysis, and progressive organ damage.
h) Thalassemia:
Thalassemias are a heterogeneous group of inherited hemoglobin disorders characterized by reduced or absent synthesis of one or more globin chains alpha-thalassemia (reduced alpha-globin synthesis) or beta-thalassemia (reduced beta-globin synthesis) causing hypochromic microcytic anemia of varying severity from asymptomatic (thalassemia trait) to severe transfusion-dependent disease (thalassemia major). India has one of the world's largest thalassemia burdens approximately 12,000 children with thalassemia major are born annually.
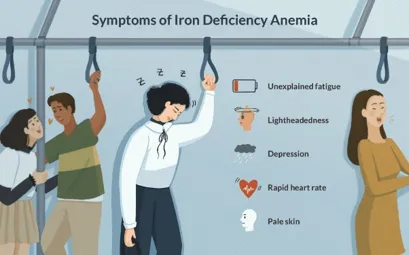
Symptoms of Anemia:
1. Persistent tiredness and reduced physical endurance from impaired oxygen delivery to muscles Fatigue:
2. Colorless appearance of skin, conjunctivae, nail beds, and oral mucosa from reduced hemoglobin Pallor:
3. Breathlessness on exertion or at rest in severe anemia from compensatory hyperventilation Dyspnoea:
4. Rapid heart rate as the cardiovascular system compensates for reduced oxygen-carrying capacity Tachycardia:
5. Lightheadedness and spinning sensation from cerebral hypoperfusion Dizziness:
6. Throbbing or pounding heartbeat from hyperdynamic circulation Palpitations:
7. Difficulty concentrating, poor memory, and reduced academic performance from cerebral hypoxia Cognitive impairment:
8. Spooning of nails (koilonychia), hair loss, and glossitis in chronic iron deficiency Signs of IDA:
SYMPTOMS
Causes of Anemia (Particularly Iron Deficiency Anemia):
1. Inadequate dietary iron intake plant-based diets low in bioavailable iron; poverty-related malnutrition
2. Blood loss menstruation (commonest cause in women), gastrointestinal bleeding, parasitic infections
3. Increased physiological iron demand pregnancy, lactation, rapid growth in infancy and adolescence
4. Malabsorption coeliac disease, gastric bypass surgery, achlorhydria reducing iron solubility
5. Helicobacter pylori infection competes for gastric Vitamin C, impairing iron absorption
6. Nutritional deficiencies Vitamin C, Vitamin B12, Folate, Vitamin A
7. Chronic diseases infections, inflammatory conditions elevating hepcidin and blocking iron
8. Vegetarian/vegan diet with no animal-source heme iron highest bioavailability source
9. Dietary inhibitors of iron absorption tea, coffee, phytates, calcium competing with iron at DMT1
10. Low socioeconomic status, food insecurity, and limited dietary diversity

SYMPTOMS
Pathophysiology:
A) Iron Deficiency Molecular and Cellular Mechanisms:
1. Negative iron balance develops when iron losses (menstrual blood, gastrointestinal) or demands (pregnancy, growth) exceed dietary iron absorption beginning the progressive depletion of reticuloendothelial iron stores.
2. As ferritin falls, erythroid precursors in the bone marrow upregulate TfR1 (transferrin receptor 1) expression to maximize iron capture from circulating transferrin but inadequate transferrin saturation means insufficient iron reaches developing erythroblasts.
3. Iron-deficient erythroblasts produce smaller erythrocytes with less hemoglobin the characteristic microcytic (MCV < 80 fL), hypochromic (MCH < 27 pg, MCHC < 32 g/dL) anemia of iron deficiency reflecting the diversion of available iron to heme synthesis at the cost of cell size.
4. In parallel, iron deficiency impairs the function of iron-containing enzymes cytochrome c oxidase (reducing ATP production), ribonucleotide reductase (impairing DNA synthesis), and multiple hydroxylases producing functional impairments independent of and preceding the development of frank anemia.
5. Urtica dioica powder delivers natural chelated plant iron in a form that is less irritating to the GI mucosa than ionic iron salts avoiding the ROS generation and epithelial damage that cause the GI side effects of conventional iron therapy while still providing bioavailable iron for heme synthesis.
B) Role of Vitamin C in Iron Absorption Enhancement:
1. Dietary non-heme iron from Urtica dioica exists primarily in the Fe³⁺ (ferric) oxidation state within the plant matrix combined with organic acid iron complexes and phytate iron.
2. In the acidic environment of the stomach (pH 1.5–3.5), Ascorbic Acid reduces Fe³⁺ to Fe²⁺ (ferrous) the only form transported by the intestinal iron absorptive channel DMT1 directly enabling iron absorption that would otherwise be limited by the insolubility of Fe³⁺ at intestinal pH.
3. Ascorbic Acid forms a soluble, stable chelate complex with iron (Fe²⁺-ascorbate) that remains in solution as the gastric contents enter the alkaline duodenum resisting precipitation by phytates, oxalates, tannins, and calcium that would otherwise sequester iron in insoluble complexes and prevent DMT1-mediated uptake.
4. The addition of 50–100 mg of Ascorbic Acid per meal increases non-heme iron absorption by 3–6 fold the most powerful single dietary intervention available for improving plant iron bioavailability. The Ascorbic Acid included in the suspension formulation (0.1 g per 30 g formulation) directly leverages this scientifically validated mechanism.
5. The natural co-presence of Vitamin C in Urtica dioica itself, supplemented by the Ascorbic Acid excipient and the Citric Acid pH adjuster in the formulation, creates a triple-layer iron absorption enhancement system that maximizes the bioavailability of the plant iron delivered by the suspension.
C) How the Suspension Formulation Optimizes Urtica dioica Delivery:
1. The dual suspending agent system Xanthan Gum (primary, 0.2–0.4 g) and Sodium CMC/Tragacanth (secondary, 0.1–0.3 g) creates a synergistic viscoelastic network in the aqueous continuous phase that suspends Urtica dioica powder particles uniformly throughout the preparation, preventing rapid sedimentation and ensuring dose uniformity per measured volume.
2. Xanthan Gum's unique pseudoplastic (shear-thinning) rheology provides high viscosity at rest (preventing sedimentation) and low viscosity during shaking and pouring (allowing easy redispersion and smooth flow into a measuring spoon) ideal properties for a pharmaceutical suspension that must be shaken before each dose.
3. Glycerin acts as a humectant that prevents moisture loss from the continuous phase, maintaining consistent suspension viscosity during storage, and as a wetting agent that ensures all Urtica dioica powder particle surfaces are completely wetted by the aqueous vehicle essential for preventing particle clumping.
4. Ascorbic Acid (antioxidant excipient) and EDTA (chelating agent) act synergistically to protect both the formulation stability (preventing oxidative browning of phytochemicals) and the iron in Urtica dioica from unwanted oxidation to poorly absorbed Fe³⁺ during storage.
5. The flavour (orange/vanilla) and sweetener (Sucrose/Sorbitol) system transforms the suspension from an unpalatable herbal preparation into an appealing, pleasant-tasting liquid that patients particularly children will willingly take daily, directly addressing the compliance deficit that undermines conventional iron supplementation programs.

URTICA DIOICA LEAF
AIM AND OBJECTIVE:
Aim: Formulation and Evaluation of Suspension of Urtica Dioica (Nettle) Powder to Treat Anemia.
Objective:
MATERIAL:
Drug: Urtica dioica Powder (Stinging Nettle aerial parts self-prepared, authenticated, and standardized for iron content).
Excipients: Sucrose IP / Sorbitol IP, Glycerin IP, Xanthan Gum IP (pharmaceutical grade), Sodium CMC IP / Tragacanth IP, Citric Acid IP (Monohydrate), Ascorbic Acid IP (Vitamin C), Sodium Benzoate IP, EDTA (Disodium edetate IP trace), Orange/Vanilla Flavour (food/ pharmaceutical grade), Food Color (FD&C approved, food grade), Distilled Water (freshly prepared).
Equipment: Mechanical Stirrer, Mortar and Pestle, Beaker (50 mL, 100 mL), Glass Rods, Measuring Cylinders, Graduated Cylinders (for sedimentation), Water Bath, Amber Glass Bottles (50 mL), Sieves (60 mesh), Hot Air Oven.
Instruments: Analytical Weighing Balance, pH Meter (calibrated), Brookfield Viscometer, UV-Visible Spectrophotometer, Atomic Absorption Spectrophotometer (for Fe content), Stability Chamber.
METHOD:
Step 1: Preparation of Urtica dioica Powder
1. Collect fresh Urtica dioica aerial parts (leaves and stems) during the pre-flowering stage peak nutritional content. Use protective gloves to handle due to stinging trichomes. Authenticate as Urtica dioica by characteristic morphology deeply serrated, opposite leaves with prominent midrib and venation; dense stinging trichomes on both leaf surfaces.
2. Wash thoroughly under running water, rinse with distilled water, and remove any damaged or diseased material.
3. Blanch briefly in boiling water for 30–60 seconds to neutralize the stinging trichomes by denaturing formic acid and histamine. This step eliminates the sting without significantly reducing the iron or phytochemical content.
4. Shade-dry the blanched plant material at room temperature for 10–14 days to preserve heat-labile Vitamin C content, OR dry in a hot air oven at 45°C for 48–72 hours (moderate temperature to balance moisture removal with Vitamin C preservation).
5. Grind the completely dried material using a mechanical grinder. Pass through a 60-mesh sieve to obtain a uniform, fine, dark-green powder.
6. Determine moisture content (LOD at 105°C) NMT 8% w/w.
7. Standardize for iron content by Atomic Absorption Spectrophotometry (AAS) or colorimetric 1,10-phenanthroline method, and for Vitamin C by iodometric titration.
8. Store in an airtight amber glass container at room temperature, protected from light and moisture
PLANT PROFILE:
Urtica dioica Linn. Stinging Nettle
Drug Name: Urtica dioica (Nettle Herb / Stinging Nettle)

URTICA DIOICA
Biological Source: The drug consists of the fresh or dried aerial parts (leaves and stems) of Urtica dioica Linn.
Family: Urticaceae
Common Names: Stinging Nettle / Common Nettle (English), Bichu-Buti / Bichu Ghas (Hindi), Kandali (Sanskrit/Uttarakhand), Grande Ortie (French), Brennnessel (German)
Chemical Constituents of Urtica dioica Anti-Anemia Relevant:
Iron Content Comparison:
|
Plant Source |
Iron (mg/ 100 g fresh) |
Iron (mg/ 100 g dry) |
Vitamin C (mg/ 100 g) |
|
Urtica dioica (Nettle) |
3.5–4.2 |
36–54 |
30–80 |
|
Spinach |
2.7 |
28–35 |
28 |
|
Moringa oleifera (leaves) |
4.0 |
28–40 |
220 |
|
Amaranth leaves |
2.3 |
20–25 |
43 |
|
Lentils (cooked) |
3.3 |
7.5 |
1.5 |
|
Ferrous Sulfate (for reference) |
— |
20% elemental Fe |
— |
Anti-Anemia Pharmacological Activity Summary:
|
Mechanism |
Active Compound |
Anti-Anemia Relevance |
|
Direct iron provision |
Organically chelated plant Fe²⁺/Fe³⁺ |
Provides bioavailable iron for heme synthesis |
|
Iron absorption enhancement |
Vitamin C (co-reduces Fe³⁺→Fe²⁺) |
Enhances non-heme iron bioavailability 3–6 fold |
|
Erythropoiesis support |
Folate, Vitamin B12-related, Chlorophyll |
Supports RBC maturation and DNA synthesis |
|
Antioxidant RBC protection |
Quercetin, Rutin, Vitamin C, Beta-carotene |
Protects erythrocytes from oxidative hemolysis |
|
Anti-inflammatory (anti-ACD) |
Quercetin, Kaempferol, Phytosterols |
Reduces hepcidin-elevating cytokines improves Fe absorption |
|
GI tolerance advantage |
Chelated plant iron (non-ionic) |
No reactive Fe²⁺ ions no GI oxidative stress |

URTICA DIOICA POWDER
EXCIPIENTS:
1. Sucrose IP / Sorbitol IP
Sucrose IP: α-D-Glucopyranosyl-(1→2)-β-D-fructofuranoside; C₁₂H₂₂O₁₁; MW 342.30 g/mol
Sorbitol IP: D-Glucitol; C₆H₁₄O₆; MW 182.17 g/mol sugar alcohol, suitable for diabetic patients
Category: Sweetening agent, Viscosity enhancer, Palatability improver, Vehicle co-component
Uses:
Primary sweetening agent effectively masks the characteristic dark-green, bitter-astringent taste of Urtica dioica powder that would be highly unacceptable to patients particularly children if unmasked. The degree of bitterness masking increases with sweetener concentration
Viscosity enhancer dissolved Sucrose/Sorbitol at 17–23% w/w concentrations significantly increases the viscosity of the aqueous continuous phase, slowing particle sedimentation rate and improving physical stability.
Sorbitol advantage over Sucrose Sorbitol is non-cariogenic and does not raise blood glucose, making it preferable in diabetic patients (particularly important as anemia frequently coexists with diabetes in India). Sorbitol also provides a mild humectant effect.
2. Glycerin IP
Official Name: Glycerin (IP, USP) / Glycerol (Ph. Eur.) | C₃H₈O₃ | MW 92.09 g/mol
Category: Humectant, Wetting agent, Stabilizer, Co-solvent, Viscosity contributor
Uses:
Humectant attracts and retains moisture in the suspension continuous phase, preventing drying of the formulation near the bottle neck and cap during storage.
Wetting agent reduces the contact angle between Urtica dioica powder particles and the aqueous vehicle, ensuring complete wetting of all particle surfaces essential for preventing powder particle aggregation and ensuring uniform dispersion.
Stabilizer contributes to the overall suspension viscosity and prevents caking of settled particles by coating them with a hygroscopic film that facilitates redispersion.
Fixed at 3.0 g in all formulations providing consistent humectant-wetting function across all three formulations.
3. Xanthan Gum IP (Primary Suspending Agent)
Official Name: Xanthan Gum (IP, USP, NF) produced by fermentation of glucose by Xanthomonas campestris
Chemical Nature: High-molecular-weight (2×10⁶ g/mol) anionic heteropolysaccharide cellulose backbone with trisaccharide side chains of mannose, glucuronic acid, and mannose
Category: Primary suspending agent, Viscosity enhancer (pseudoplastic), Stabilizer, Thickener
Description:
Colour: Cream-coloured, free-flowing powder.
Solubility: Disperses readily in hot or cold water forming highly viscous solutions; stable over wide pH and temperature ranges.
Rheology: Strongly pseudoplastic (shear-thinning) high viscosity at rest but flows easily on shaking.
Uses:
Primary suspending agent Xanthan Gum's extraordinary pseudoplastic rheology makes it the ideal primary suspending agent for pharmaceutical suspensions. At rest, its high viscosity (1000–2000 mPa·s at low shear) prevents rapid sedimentation of Urtica dioica particles. Upon shaking, its viscosity drops dramatically (to 50–100 mPa·s at high shear), allowing easy redispersion and smooth pouring.
Concentration varied (0.3 g), (0.4 g highest, expected best suspension stability), (0.2 g lowest, expected fastest sedimentation).
Synergistic with Sodium CMC/Tragacanth the combination of Xanthan Gum and Sodium CMC produces a stronger gel network and better suspension stability than either polymer alone, allowing lower concentrations of each to achieve equivalent stability.
Compatible with iron and vitamins Xanthan Gum does not interact with iron, Vitamin C, or Ascorbic Acid in the formulation.
4. Tragacanth IP (Secondary Suspending Agent)
Tragacanth: Natural gum from Astragalus species; complex polysaccharide mixture; swells in water forming viscous paste
Category: Secondary suspending agent, Co-thickener, Stabilizer
Uses:
Secondary suspending agent Sodium CMC/Tragacanth complements Xanthan Gum's suspension stabilizing effect, strengthening the three-dimensional polymer network in the continuous phase that suspends Urtica dioica particles.
Mild mucoadhesive Sodium CMC's mucoadhesive properties may prolong contact of the suspension with the gastrointestinal mucosa, providing additional residence time that could enhance iron absorption.
5. Citric Acid IP
Category: pH adjuster, Antioxidant synergist, Chelating agent, Taste enhancer, Iron solubility promoter
Uses:
pH adjuster maintains suspension pH at 4.0–5.5, creating a mildly acidic environment that: (a) maximizes iron solubility (Fe²⁺ precipitates above pH 6; Fe³⁺ precipitates above pH 3 the acidic pH keeps iron in solution); (b) maximizes Ascorbic Acid stability (Vitamin C is most stable in acidic medium); (c) enhances Sodium Benzoate preservation efficacy.
Iron absorption promoter Citric Acid itself acts as an iron chelator and absorption enhancer, forming soluble citrate-iron complexes that resist precipitation in the alkaline duodenum.
Antioxidant synergist chelates metal ions that catalyze oxidative degradation of Urtica dioica phytochemicals and Ascorbic Acid during storage.
Fixed at 0.1 g in all formulations.
6. Ascorbic Acid IP (Vitamin C)
Official Name: Ascorbic Acid (IP, USP) | C₆H₈O₆ | MW 176.12 g/mol
Category: Antioxidant, Iron absorption enhancer, Preservative co-agent, Therapeutic vitamin
Uses:
Iron absorption enhancer the most critical therapeutic excipient in the formulation. Ascorbic Acid at 0.1 g per 30 g suspension (0.33% w/w) provides approximately 3.3 mg Vitamin C per 1 g serving when combined with the Vitamin C naturally present in Urtica dioica, each dose delivers approximately 10–20 mg additional Vitamin C that directly enhances non-heme iron absorption by 3–6 fold through Fe³⁺ reduction and iron chelation.
Formulation antioxidant protects Urtica dioica's labile phytochemicals (quercetin, chlorophyll, carotenoids) from oxidative degradation during the shelf life of the suspension.
Therapeutic vitamin Vitamin C deficiency itself can contribute to anemia by impairing collagen synthesis (affecting erythropoietic microenvironment) and reducing iron absorption supplementary Vitamin C provides dual therapeutic benefit.
Fixed at 0.1 g in all formulations consistent iron absorption enhancement across F1, F2, F3.
7. Sodium Benzoate IP (Preservative)
Category: Primary antimicrobial preservative | 0.05 g per 30 g (0.17% w/w)
Uses:
Broad-spectrum antimicrobial preservation protects the suspension from microbial contamination during the 4–8-week use period after opening. Most effective in acidic media (pH < 4.5) where undissociated benzoic acid predominates Citric Acid and Ascorbic Acid maintain the formulation's acidic pH that maximizes Sodium Benzoate efficacy.
Fixed at 0.05 g in all formulations standard IP concentration for oral liquid preparations.
8. EDTA (Disodium Edetate IP Trace)
Category: Chelating agent, Antioxidant synergist, Metal sequestrant | 0.02 g per 30 g (0.067% w/w)
Uses:
Chelating agent EDTA chelates trace heavy metal ions (copper, zinc, manganese) that contaminate pharmaceutical preparations and catalyze the oxidative decomposition of Ascorbic Acid and other labile phytochemicals through Fenton-type reactions. By sequestering these metal catalysts, EDTA dramatically extends the shelf life of Ascorbic Acid and the iron-phytochemical complexes in the suspension.
CRITICAL DISTINCTION from iron chelation: At the low trace concentration used (0.02 g per 30 g), EDTA preferentially chelates contaminating heavy metals (Cu²⁺, Zn²⁺) rather than the therapeutic iron in Urtica dioica since iron is present at much higher concentrations than these trace metal contaminants. This selective chelation preserves the bioavailability of Urtica dioica iron while protecting Ascorbic Acid stability.
Fixed at 0.02 g in all formulations.
9. Flavor (Orange/Vanilla)
Category: Palatability enhancer, Taste-masking agent, Compliance improver

Uses:
Primary taste masker orange and vanilla flavors effectively mask the characteristic bitter, astringent, dark-green taste of Urtica dioica powder, transforming the suspension into a pleasant-tasting preparation that children and adults will willingly take daily without resistance directly addressing the compliance limitation that undermines iron supplementation programs.
Fixed at 0.2 g in all formulations consistent palatability enhancement.
CHEMICAL TEST (Identification of Urtica dioica and Key Excipients):
1. Iron Identification Ferrous Ion Test (Potassium Ferrocyanide Test)
Procedure: Acidify 2 mL of the suspension with dilute HCl. Add 2–3 drops of potassium ferrocyanide (K₄[Fe(CN)₆]) solution.
Observation: Formation of a characteristic Turnbull's blue (deep blue) precipitate confirms the presence of ferrous iron (Fe²⁺) from Urtica dioica powder the bioavailable form of iron for gastrointestinal absorption. The intensity of the blue color is proportional to Fe²⁺ concentration.
2. Iron Identification Ferric Ion Test (Potassium Thiocyanate Test)
Procedure: Add 2–3 drops of potassium thiocyanate (KSCN) solution to 1 mL of suspension extract in dilute HCl.
Observation: Formation of a blood-red coloration of ferric thiocyanate confirms the presence of ferric iron (Fe³⁺) from the plant matrix. Both Fe²⁺ and Fe³⁺ forms are present in Urtica dioica the ratio of the two depends on the redox environment (Ascorbic Acid maintains iron in Fe²⁺ form preferentially).
3. Vitamin C Identification (DCPIP Decolorization Test)
Procedure: Add 1 mL of 2,6-dichlorophenolindophenol (DCPIP) blue dye to 1 mL of suspension aqueous extract.
Observation: Immediate decolorization of the blue DCPIP to colourless confirms the presence of Ascorbic Acid (Vitamin C) the key iron absorption enhancing excipient in the suspension formulation.
4. Chlorophyll Identification (Urtica dioica Spectroscopic Test)
Procedure: Extract suspension in methanol and scan from 400–700 nm in UV-Visible spectrophotometer.
Observation: Characteristic absorption peaks at approximately 430 nm (Soret band strong) and 665 nm (Q band) confirm the presence of chlorophyll from Urtica dioica the green pigment responsible for the suspension's characteristic dark-green colour and structurally analogous to heme.
5. Xanthan Gum Identification (Ruthenium Red Test)
Procedure: Add 2–3 drops of Ruthenium Red (0.1% aqueous) solution to 1 mL of the suspension.
Observation: Development of a pink to red coloration confirms the presence of Xanthan Gum an acidic polysaccharide as the primary suspending agent. Ruthenium Red is a specific stain for anionic mucopolysaccharides and acidic polymers.
6. Sodium Benzoate Identification (Ferric Chloride Test Preservative)
Procedure: Acidify suspension extract with dilute HCl and add a few drops of ferric chloride (FeCl₃) solution.
Observation: Formation of a salmon-pink precipitate of ferric benzoate confirms the presence of Sodium Benzoate preservative in the formulation.
Phytochemical Screening of Urtica dioica Powder:
|
Sr. No. |
Phytochemical |
Method Used |
Observation |
Inference |
|
1 |
Iron (Fe²⁺) |
K₄[Fe(CN)₆] / Turnbull's Blue Test |
Deep blue precipitate |
Ferrous iron confirmed |
|
2 |
Iron (Fe³⁺) |
Potassium Thiocyanate (KSCN) Test |
Blood-red coloration |
Ferric iron confirmed |
|
3 |
Vitamin C (Ascorbic Acid) |
DCPIP Decolorization Test |
Immediate blue decolorization |
Vitamin C confirmed |
|
4 |
Chlorophyll |
UV-Vis scan (430 nm, 665 nm peaks) |
Characteristic dual absorption bands |
Chlorophyll confirmed |
|
5 |
Flavonoids (Quercetin/Rutin) |
Shinoda's Test |
Pink to orange-red color |
Quercetin/Rutin confirmed |
|
6 |
Tannins |
Ferric Chloride Test |
Dark blue-green coloration |
Tannins confirmed |
|
7 |
Xanthan Gum |
Ruthenium Red Test |
Pink-red coloration |
Primary suspending agent confirmed |
ADVANTAGES OF URTICA DIOICA SUSPENSION OVER CONVENTIONAL IRON SUPPLEMENTS:
|
Parameter |
Conventional Iron Salts (Ferrous Sulfate, Gluconate) |
Urtica dioica Suspension |
|
Iron source |
Synthetic ionic iron salts high free ionic Fe²⁺ |
Organically chelated plant iron naturally complexed |
|
GI side effects |
Very common nausea, vomiting, constipation, cramping |
Minimal plant matrix iron does not generate GI ROS |
|
Taste/ Palatability |
Metallic, astringent, very unpleasant |
Sweet, orange/vanilla flavoured no metallic taste |
|
Vitamin C |
Not included in most preparations |
Natural Vitamin C from plant + Ascorbic Acid excipient 3–6× absorption |
|
Additional nutrients |
Iron only |
Iron + Folate + Chlorophyll + Flavonoids + Carotenoids + Vitamins |
|
Antioxidant protection |
Absent ionic Fe²⁺ generates ROS |
Potent quercetin, rutin, Vitamin C, beta-carotene |
|
Compliance |
Poor (30–50% discontinue due to side effects) |
Excellent pleasant taste, no GI discomfort |
|
Anti-inflammatory |
Absent |
Quercetin, kaempferol reduce hepcidin-elevating cytokines |
|
Suitability for children |
Difficult unpleasant taste, GI effects |
Excellent sweet, flavoured, well-tolerated |
|
Suitability for diabetics |
Sucrose-containing preparations problematic |
Sorbitol option non-cariogenic, minimal glycemic impact |
|
Iron bioavailability |
High (as ionic Fe²⁺) but highly variable |
Enhanced by natural + added Vitamin C and chelating acids |
|
Cost and accessibility |
Inexpensive synthetic |
Natural Urtica dioica widely available across India |
EVALUATION PARAMETER:
1. Organoleptic Properties
The prepared suspensions are evaluated for appearance, colour, odour, taste, and overall sensory acceptability. A well-prepared Urtica dioica anti-anemia suspension should appear as a dark-green to olive-green suspension with an attractive orange or creamy-yellow appearance from the added food color uniformly dispersed with no visible large particle aggregates or unmixed powder clumps floating on the surface. The peppermint or orange/vanilla fragrance from the flavour system should be pleasant and sufficient to mask the characteristic herbal odour of Urtica dioica. The taste should be predominantly sweet with mild pleasant citrus or vanilla notes, with the bitter-astringent Urtica dioica taste acceptably masked by sucrose/sorbitol and flavour. No metallic taste a critical differentiator from conventional iron salt formulations should be present.
2. pH Determination
pH is measured using a calibrated digital pH meter at 25°C ± 0.5°C. The target pH range for the Urtica dioica anti-anemia suspension is 4.0 to 5.5 an acidic range chosen to: (a) maximize iron solubility from the Urtica dioica plant matrix (iron precipitates as insoluble Fe(OH)₃ above pH 6.0, significantly reducing bioavailability); (b) maintain Ascorbic Acid in its most stable reduced form (Vitamin C oxidizes much faster in neutral or alkaline media); (c) maximize Sodium Benzoate preservation efficacy (benzoic acid, the active antimicrobial form, predominates below pH 4.5); and (d) suppress microbial growth through the intrinsic antimicrobial effect of acidic conditions.
3. Viscosity
Viscosity is measured using a Brookfield RV Viscometer at 25°C ± 0.5°C at multiple rpm (5, 10, 20, and 50 rpm) to characterize the suspension's rheological profile. The suspension is expected to exhibit pseudoplastic (shear-thinning) behavior dominated by Xanthan Gum's pseudoplastic rheology with high viscosity at low shear (favoring physical stability during rest) and lower viscosity at high shear (allowing easy shaking and pouring). F2 with the highest combined suspending agent concentration (Xanthan 0.4 g + Sodium CMC 0.3 g = 0.7 g total) is expected to have the highest viscosity. Target: 200–800 mPa·s at 20 rpm for an acceptable oral suspension.
4. Sedimentation Volume and Redispersibility
Sedimentation volume (F) is measured by transferring 30 mL of shaken suspension into a graduated measuring cylinder and observing the volume of the sediment layer (Vu) at 1, 2, 4, 8, 24, 48, and 72 hours. Sedimentation Volume F = Vu/V₀. Higher F indicates better suspension stability. Redispersibility is assessed by counting the number of gentle inversions required to completely resuspend settled material after 24 hours standing target ≤ 5 inversions, indicating an easily redispersible flocculated sediment rather than a hard, difficult-to-resuspend cake. F2 with highest suspending agent total (0.7 g) is expected to have the highest sedimentation volume (slowest settling) and best redispersibility.
5. Density / Specific Gravity
Specific gravity of each suspension is determined using a calibrated pycnometer at 25°C. The density provides a quality control parameter since patients measure doses by volume (teaspoon), the actual iron dose per teaspoon depends on the suspension density
6. Drug Content Iron Content per Dose
Iron content in the suspension is determined by the Atomic Absorption Spectrophotometry (AAS) method (most accurate) or the colorimetric 1,10-phenanthroline method (reference method in IP for pharmaceutical iron analysis). A precisely measured volume of suspension (10 mL one dose) is digested with nitric acid and perchloric acid (5:1) to destroy the organic matrix and liberate all iron. After digestion and appropriate dilution, iron concentration is measured at 248.3 nm (AAS) or at 508 nm after color development with 1,10-phenanthroline at pH 3.5
7. Vitamin C Content
Vitamin C (Ascorbic Acid) content per dose is determined by iodometric back-titration a classical, IP-recognized method. A measured volume of suspension (10 mL) is extracted with 3% meta-phosphoric acid (which stabilizes Vitamin C against oxidation during analysis). The extract is titrated with standardized 0.01 M iodine solution using starch as indicator until the blue endpoint persists. Vitamin C content is expressed as mg per 10 mL dose. The total Vitamin C per dose (from the Ascorbic Acid excipient + naturally occurring Vitamin C in Urtica dioica powder) is the therapeutically relevant value and should be ≥ 10 mg per dose the minimum amount shown to significantly enhance iron absorption.
8. In-Vitro Antioxidant Activity (DPPH Assay)
The antioxidant activity of the Urtica dioica suspension contributed by quercetin, rutin, Vitamin C, chlorophyll, and beta-carotene from the plant powder plus the Ascorbic Acid and Citric Acid excipients is determined by the DPPH free radical scavenging assay. Serial dilutions in methanol are incubated with DPPH solution for 30 minutes in darkness; absorbance at 517 nm is measured.
9. Palatability Assessment
Palatability is evaluated by a panel of 10 healthy adult volunteers using a validated 5-point hedonic scale: 1 = Very unpleasant (unacceptable strong bitterness, herbal odour), 2 = Unpleasant (noticeable bitterness), 3 = Neutral (mild bitterness, tolerable), 4 = Pleasant (bitterness masked, sweet, flavoured), 5 = Very pleasant (sweet, attractive colour, pleasant flavour, no herbal aftertaste). Parameters assessed include overall taste, sweetness, flavour, colour appearance, texture in the mouth, and aftertaste. F3 (highest Sucrose/Sorbitol 7.0 g) is expected to achieve the highest palatability score. A mean score of ≥ 4.0 is considered clinically acceptable for daily long-term administration to anemia patients.
10. Stability Studies
Accelerated stability studies are conducted as per ICH Q1A(R2) guidelines at 40°C ± 2°C / 75% RH ± 5% for 3 months. Suspension samples stored in sealed amber glass bottles are evaluated at 0, 1, 2, and 3-month intervals for: (a) Appearance colour change (browning from Urtica dioica phytochemical oxidation), microbial contamination, or phase separation; (b) pH any increase above 5.5 indicates Ascorbic Acid oxidation or Sodium Benzoate degradation; (c) Viscosity changes indicate polymer degradation or syneresis; (d) Sedimentation volume and redispersibility; (e) Iron content by AAS stability of iron in the suspension matrix; (f) Vitamin C content the most sensitive stability indicator; Ascorbic Acid is highly susceptible to oxidative degradation at elevated temperature; (g) Antioxidant activity (DPPH IC50); and (h) Microbial limits as per IP.
CONCLUSION
Anemia, particularly iron deficiency anemia, remains one of the most widespread and persistent nutritional disorders of the 21st century, affecting an estimated 1.62 billion people globally and imposing a disproportionately heavy burden on developing nations like India, where the National Family Health Survey 5 (NFHS-5, 2019–2021) reported deeply concerning prevalence rates of 57% in children aged 6–59 months, 67% in women of reproductive age, and 25% in men — figures that reflect the continued failure of existing iron supplementation strategies to achieve adequate population-level impact. Despite decades of national nutrition intervention programs and the widespread availability of conventional synthetic iron supplements, treatment failure and poor compliance remain the central obstacles to successful anemia management, driven overwhelmingly by the well-documented gastrointestinal adverse effects of conventional ionic iron salts including nausea, vomiting, abdominal cramping, constipation, and metallic taste that collectively lead to treatment discontinuation in an estimated 30–50% of patients.
The present review systematically examined the scientific literature, ethnopharmacological evidence, nutritional data, and pharmaceutical formulation principles relevant to the development of a natural plant-based oral suspension from Amaranthus species (Amaranth / Rajgira) leaf powder as a herbal hematinic alternative for the management of iron deficiency anemia. The review established that Amaranth leaves, with their documented iron content of 20–25 mg per 100g dry weight combined with naturally occurring Vitamin C (43 mg/100g), folate, flavonoids, carotenoids, and chlorophyll, represent a scientifically credible, practically accessible, and therapeutically rational plant source of bioavailable iron that addresses the fundamental limitations of both synthetic iron preparations and other medicinal plant alternatives. Compared to Urtica dioica (Stinging Nettle), which served as the primary reference plant in this review, Amaranth offers comparable iron and Vitamin C content with significant practical advantages including complete absence of stinging trichomes requiring no blanching treatment, milder and less astringent organoleptic profile improving patient palatability and compliance prospects, faster drying and powder preparation, and substantially wider cultivation and commercial availability across the Indian subcontinent making it a more accessible and economically viable raw material for large-scale herbal supplement production.
The pharmaceutical rationale for formulating Amaranth leaf powder as an oral suspension rather than alternative dosage forms such as tablets, capsules, or dry powders is strongly supported by the reviewed literature. The suspension dosage form offers flexible and accurate dose adjustment essential for pediatric and geriatric anemia management, avoids the compaction and binding challenges associated with tableting highly fibrous plant powders, provides superior patient acceptability particularly in children who represent the most severely affected demographic in India, and allows the incorporation of multiple excipients serving simultaneous therapeutic and stabilizing functions within a single liquid vehicle. The reviewed formulation science literature confirmed that a dual suspending agent system combining Xanthan Gum as primary pseudoplastic suspending agent with Sodium CMC or Tragacanth as secondary co-thickener produces optimally stable pharmaceutical suspensions of plant powders, with Xanthan Gum's unique shear-thinning rheology providing high viscosity at rest to prevent sedimentation and low viscosity during shaking to allow easy redispersion — properties ideally suited to the physical characteristics of Amaranth leaf powder particles.
The review of iron absorption physiology and bioavailability enhancement strategies confirmed the critical therapeutic importance of co-administering Vitamin C alongside plant-source non-heme iron. Ascorbic acid reduces ferric iron (Fe³⁺) to the absorbable ferrous form (Fe²⁺), forms soluble iron-ascorbate chelate complexes that resist precipitation by dietary inhibitors such as phytates, oxalates, and tannins in the alkaline duodenum, and enhances non-heme iron absorption by 3–6 fold — representing the single most powerful dietary intervention available for improving plant iron bioavailability. The natural co-presence of Vitamin C within Amaranth leaf powder itself, supplemented by Ascorbic Acid as a formulation excipient and Citric Acid as both pH adjuster and additional iron chelation promoter, creates a scientifically integrated triple-layer iron absorption enhancement system that maximizes the therapeutic utility of the plant iron delivered by the suspension. The additional incorporation of EDTA at trace concentrations as a heavy metal chelating agent protecting Ascorbic Acid stability during storage further strengthens the formulation's long-term therapeutic consistency.
The phytochemical and pharmacological literature reviewed confirmed that Amaranth's anti-anemia activity extends beyond simple iron provision. Its folate content supports erythroid precursor DNA synthesis and prevents megaloblastic changes in developing red blood cells. Its flavonoid constituents — including quercetin and rutin — provide potent antioxidant protection of circulating erythrocytes against oxidative hemolysis, while their anti-inflammatory activity reduces hepcidin-elevating cytokines that would otherwise block iron absorption in inflammatory states. Its chlorophyll content, structurally analogous to the porphyrin ring of heme, has been proposed in the ethnopharmacological literature to contribute to blood-building activity through mechanisms beyond direct iron delivery. Collectively, these multiple complementary mechanisms of anti-anemia action position Amaranth as a nutritionally superior and pharmacologically multifunctional iron source compared to single-nutrient synthetic iron salt preparations.
REFERENCES


Rutik Antarkar, Vidya Kale, Formulation and Evaluation of Suspension of Urtica Dioica (Nettle) Powder to Treat Anemia, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 837-856. https://doi.org/10.5281/zenodo.20529160
 10.5281/zenodo.20529160
10.5281/zenodo.20529160