
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Womens college of pharmacy,peth vadgaon,Maharashtra, India.
Breast cancer is one of the most frequently diagnosed malignancies and a leading cause of cancer-related mortality among women worldwide. It is a multifactorial disease influenced by genetic, hormonal, environmental, and lifestyle-related risk factors. The increasing global prevalence of breast cancer highlights the importance of early detection, effective diagnosis, and advanced therapeutic interventions. This review provides a comprehensive overview of breast cancer, including its epidemiology, etiology, risk factors, pathophysiology, classification, signs and symptoms, and diagnostic techniques. Different subtypes of breast cancer, including invasive ductal carcinoma, luminal breast cancer, HER2-positive breast cancer, medullary carcinoma, and triple-negative breast cancer, are discussed in detail. Diagnostic approaches such as mammography, ultrasound, biopsy, magnetic resonance imaging (MRI), and computer-aided detection systems are highlighted for their significance in early detection and accurate diagnosis. The staging of breast cancer and commonly employed treatment strategies, including surgery, chemotherapy, radiotherapy, and targeted therapies, are also reviewed. Furthermore, the role of herbal medicine and traditional therapeutic approaches, including compounds such as curcumin, green tea polyphenols, piperine, and licorice, in breast cancer management is explored. The review emphasizes the importance of awareness, preventive strategies, and multidisciplinary treatment approaches to improve patient outcomes and reduce disease burden
Cancer is the uncontrolled growth of abnormal cells anywhere in the body. The abnormal cells are termed cancer cells, malignant cells or tumor cells. These cells can infiltrate normal body tissues. The most common type of cancer include breast cancer, prostate cancer, lungs cancer, colon cancer, melanoma etc. breast cancer is the type of
cancer that affects the breast. It is the most common invasive cancer in women, the second main cause of cancer death in women, after lung cancer. Advances in screening and treatment have improved survival rates dramatically since 19 to 68810. The chance of any woman dying from breast cancer is around 1 in 37, or 2.7%(1) The most prevalent illness that affects women worldwide is still breast cancer (2).
According to research, known genetic, physical, and lifestyle variables account for almost half of instances of breast cancer.(3) According to GLOBOCAN, almost 2.1 million women were diagnosed with the illness in 2018, and nearly 630,000 of them died from it. Significant advancements have been made in the diagnosis and treatment of breast cancer, despite the disease's ongoing rise in cases.(4)When normal cells have alterations or mutations in their DNA or RNA, cancer results. Radiation (such as X-rays, gamma rays, or ultraviolet light), viral, bacterial, or fungal infections, parasitic activity, inflammation, heat, chemicals in the air, water, or food, physical cell damage, free radicals, or the aging process of DNA and RNA can all cause these changes over time. Cancer may begin as a result of these mutations. According to some researchers, cancer is a "entropic disease," which means that it is associated with a breakdown in the body's capacity to maintain order and that external treatment is frequently required to help restore balance.(5) To aid in the treatment of breast cancer, researchers have created a variety of hybrid polymer nanoparticles in recent years. These microscopic particles are intended to deliver medications straight to cancer cells in addition to studying tumour indicators and detecting cancer in the body. Nanotechnology-based methods like these have a lot of potential for treating different types of cancer. (6) Mammography has been shown to help reduce the risk of dying from breast cancer and is a popular technique for screening for the illness. Over the past ten years, other screening methods have also been utilised and extensively researched, including as magnetic resonance imaging (MRI), which is even more sensitive than mammography.(7) Breast cancer occurs at different rates around the world, with Western nations having greater incidence rates than Eastern nations. However, due to lifestyle changes, an increase in longevity, and the adoption of Westernized dietary practices, the prevalence of breast cancer is quickly rising in low- and middle-income countries (8) Several studies have shown that several factors, including age, race, and socioeconomic status, genetic factors like BRCA mutations, hormonal factors like age at menarche, parity, and age at first full-term pregnancy, breastfeeding, and lifestyle-related factors like diet, physical activity, alcohol use, and tobacco use are all associated with an increased risk of breast cancer(9) Breast cancer is a multifactorial disease with major genetic, environmental, and behavioral/lifestyle components. The objective of the current review was to investigate the epidemiology and associated risk factors of breast cancer globally to comprehend its prevalence and aid in early detection. The main risk factors for breast cancer are genetic factors, specifically family history; diet, and obesity, as the quality of life in our country improves, women are getting more and more obese, and their diet tends to be more and more high-fat; smoking and drinking; the other is ionizing radiation; still have, specifically menstruation, bear, and whether lactation, these factors also can affect the occurrence of breast cancer. To lessen the impact exogenous hormones, have on the body, we should try to avoid using cosmetics that contain estrogen in our daily lives. Around these appeals, there has been a lot of debate. As a result, it is essential to thoroughly examine the risk factors for breast cancer using meta-methods to direct clinical prevention and treatment(10)
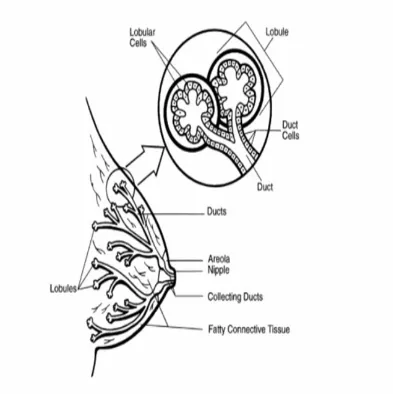
Fig 1. Structure Of Breast
EPIDEMIOLOGY OF BREAST CANCER
Different subtypes of breast cancer are distinguished by diverse epidemiological trends, making it a heterogeneous illness. (11) An estimated 1.7 million women worldwide received a breast cancer diagnosis in 2012, and approximately 521,900 of those women died from the disease that same year. (12) Compared to developed countries, developing countries diagnose twice as many cases of breast cancer in women aged 15 to 49. (13) Breast cancer is a rare malignancy in men, making up less than 1% of all cancer cases.(14) Ten In pregnant and postpartum women, breast cancer is the most prevalent type of cancer. Every year, about 1:3000 cases of breast cancer connected to pregnancy are identified (15). The incidence rate of breast cancer was linked to age over 50 in a case-control study (16).
Etiology
Endocrine factors
Everyone agrees that environmental variables are important in the development of mammary cancer. (17) It is unclear if other endogenous or exogenous factors work in concert with genetic factors in patients with a family history of breast cancer. There are some indications that this is the case. Fishman and associates (18,19)
Diet
There is conflicting, inconsistent, and inconsistent evidence regarding the impact of dietary variables on the risk of breast cancer (20,21 ,22). As a result, cutting back on dietary fat would be the best way to prevent breast cancer in the first place. There is a negative correlation between the percentage of calories from fish and the incidence of breast cancer, according to a comparison of diets in various nations. There are hints that some fish's omega-3 fatty acids may be protective (23). Excessive consumption of fat, particularly saturated fat, is linked to mortality (RR=1.3) and a poor prognosis for patients with breast cancer in the modern western diet (24).
Reproductive factors
Their breast cancer risk is believed to increase hormonal events that increase the lifetime exposure of estrogens to an individual. This includes menarche initiation before the age of 12 years, first live reception after the age of 30 years, and nulliparity and menopause after the age of 55 years(25)
Risk Factors of Breast Cancer
1. Genetic factors
Genetic predisposition is one of the most intellectually intriguing factors associated with increased risk for breast cancer. The growing knowledge base about the fundamental changes in gene structure and expression involved in tumorigenesis suggest that patterns of risk can be precisely defined on a person-by-person basis. Genetic predisposition is reflected in the approximately 20% of breast cancer patients who have a positive family history of breast cancer, and identified more specifically in the 5% of patients in whom a specific germline mutation has been identified (26)
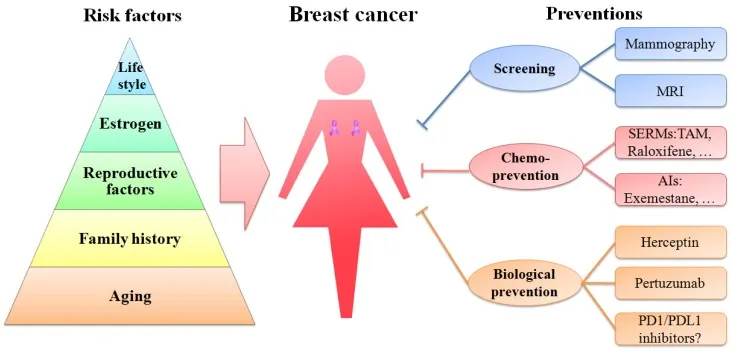
Fig 2. A Schematic Diagram Of Risk Factors Is Depicted In A Pyramid-Style Structure
2.Family history
Women, whose mother or sister has a breast cancer, are prone to this disease. A cohort study of over 113,000 women in UK demonstrated that women with one first-degree relative with breast cancer have a 1.75-fold higher risk of developing this disease than women without any affected relatives. Moreover, the risk becomes 2.5-fold or higher in women with two or more first-degree relatives with breast cancer (27)
PATHOPHYSIOLOGY OF BREAST CANCER
Breast cancer, like other cancers, is triggered by contact between an environment and a defective gene. Cell division in normal cells stops after the desired number; then cells enter their tissues by attaching to other cells (28) Experiments show that variations that can lead to breast cancer are associated with high estrogen levels. Immune system defects that are naturally responsible for killing malignant cells through a person's life and anomalous signalling of growth factors in the interaction between stromal cells and epithelial cells can enable the growth of cancerous cells (29) Lobes and ducts make up the breast. There are 15 to 20 parts called lobes in each breast. There are also smaller parts of each lobe called lobules. The tiny bulbs in dozens that make milk end up with lobules. Thin tubes called ducts bind the lobes, lobules, and bulbs. There are also blood and lymph vessels in each breast. The lymph vessels contain a watery fluid called lymph, which is nearly colorless. Among small lymph nodes, bean-shaped structures the lymph vessels hold lymph. The lymph nodes pumps the lymph and store the WBC that helps in preventing disease and infection. Lymph node communities are located in the vicinity of the breast, in the axilla, above the collarbone, and in the chest. Carcinoma can be defined as the tumors that are caused by the epithelial portion of the breast. The portion of the epithelium consists of cells that line the lobules along with the terminal ducts. These epithelial cells under natural conditions are responsible for the production of milk. The vast majority of all breast cancers produce the following carcinomas. Sarcomas are unusual diseases resulting from stromal (epithelial) breast materials (30)
Type / Classification of breast cancer
1. Invasive ductal carcinoma no specific type (IDC-NST)
The histological subtype IDC-NST is the most common, constituting about 40% to 75% of all invasive breast carcinomas. Usually, it has a wide scope of morphological variation and clinical behaviour(31) cells that break through the duct and lobular wall and invade the surrounding fatty and connective tissues of the breast. Cancer can be invasive without being metastatic (spreading) to the lymph nodes or other organs
2.Non-Invasive Breast Cancer
cells that are confined to the ducts and do not invade surrounding fatty and connective tissues of the breast. Ductal carcinoma in situ (DCIS) is the most common form of non-invasive breast cancer (90%). Lobular carcinoma in situ (LCIS) is less common and considered a marker for increased breast cancer risk. (32)
3. Luminal breast cancer
Luminal breast cancers are enriched for ER positive tumours, and include special type cancers such as tubular, cribriform, lobular and mucinous carcinomas. Luminal cancers form a continuous spectrum that can be arbitrarily divided into two subgroups based on the expression of proliferation related genes. Luminal A tumours are typically low grade with excellent prognosis, ER/PR positive and HER2 negative, with high expression of ER-related genes and low expression of proliferation related genes(33,34)
4. HER2 positive breast cancer
ER negative cancers comprise biologically distinct entities with different drivers that can be divided into two main groups – HER2 enriched and basal-like/ TNBC. The HER2 enriched group are driven by overexpression of HER2 and genes associated with related pathways or with the HER2 amplicon on chromosome 17q12. Before the introduction of HER2 targeted therapies they had the worst prognosis of all breast cancer subtypes. Although the majority of tumours within this subgroup (>80%) show HER2 gene amplification or HER2 protein overexpression on IHC, not all clinically defined HER2 positive tumours fall into this subgroup; many ER positive / HER2 positive tumours fall into the luminal B group mentioned above(35,36) ERBB2 is also known as the HER2/neu gene, where the “neu” component of the name refers to the rat/ mouse homolog of HER2(37)
5. Medullary carcinoma
Medullary carcinoma is an invasive breast cancer that designs a discrete margin normal tissue and medullary tissue(38)
6. Triple‑negative breast cancer
Breast cancer is at the present extensively documented that is a heterogeneous disorder with special sub-forms, distinguished by means of their dissimilar clinico-pathological characteristics, prevision and responses to management. Triple-negative breast cancer is described by the deficiency of progesterone receptor, human epidermal growth factor receptor 2 and estrogen receptor expression(39)
Sign and symptoms
The classic symptom for breast cancer is a lump found in the breast or armpit. Doing monthly breast self-exam (BSE) is a great way to be familiar with the breasts’ texture, cyclical changes, size, and skin condition. The general alerting features of breast cancer are such as swelling or lump (mass) in the breast, swelling in the armpit (lymph nodes), nipple discharge (clear or bloody), pain in the nipple, inverted (retracted) nipple, scaly or pitted skin on nipple, persistent tenderness of the breast, and unusual breast pain or discomfort. In Advanced stage (Metastatic) of disease underarm lymph nodes are present with other symptoms such as bone pain (bone metastases), shortness of breath (lung metastases), drop in appetite (liver metastases), unintentional weight loss (liver metastases), headaches, neurological pain or weakness(40)
Diagnosis
1.History and physical examination
The clinical history of patients with breast cancer is aimed at investigating cancer threat and demonstrating the occurrence or lack of manifestations indicative of breast illness(41) It must comprise age at menarche menopausal condition, earlier pregnancies and utiliza-tion of hormone replacement therapy after menopauseor utilization of oral contraceptives. Personal history aswell as family history should be carried out in detail. Per-sonal history includes age at diagnosis of breast cancer,previous breast biopsies and treatment of other cancerwith use of radiations. Family history includes historyof ovarian cancers and breast cancer in first degree rela-tives. Patents should be examined for particular mani-festations such as breast pain, weight loss, pain in bone,tiredness and nipple discharge (42)
2. Computer-aided detection/diagnosis system in mammography
In the analysis of mammograms, detection and diagnosis of breast cancer are extremely challenging tasks due to complexities like variability in appearance of abnormalities and hiding abnormal tissues in dense breasts. As cost-effective tools, computer-aided detection/diagnosis techniques can aid the radiologist by reducing interpretation error. Used as double readers, CAD systems can increase the accuracy of radiologists' final decision. The goal of the computer-aided detection schemes is to help radiologists to avoid overlooking abnormal features that are not visible on the screening image(43,44 ,45-47) that is made by a radiologist who uses the output from computerized analysis of medical images as a “second opinion” in detecting lesions and making diagnostic decisions. In the past several years, CAD systems have drawn much attention from both research scientists and radiologists because of the associated challenging research topics and potential clinical applications. There are two types of CAD systems based on mammographic technologies: one is based on the conventional screen-film mammographic technology and the other is based on digital mammographic technology. In the first type of CAD systems, the films are scanned, digitized, and saved on the computer for further examination. The second type of systems use full-field digital mammographic (FFDM) technology, which is expected to provide a higher signal-to-noise ratio, a higher detection quantum efficiency, a wider dynamic range, and a higher contrast sensitivity than digitized film mammograms (48)
3. Breast Ultrasound
Breast ultrasound sometimes called as sonography makes use of sound waves for internal examination of the body part. Basically, it works as a follow-up test for abnormalities by mammogram and provides guidelines for a needle biopsy of a lump. A handheld device called transducer is needed to put on the breast’s upper skin where a gel must be applied and moved across the breast showing the structure of the underlying tissue. Then, the sound waves are emitted and the generated echoes must be picked up by the transducer which bounces off the body tissues. The echoes are then converted into an image which needs to be labeled in regard to orientation and location in the breast. It produces both quantitative and qualitative diagnostic information based on a set of comprised methodologies(49)
4.History of vacuum-assisted breast biopsy (VABB)
VABB was developed in 1995 by Fred Burbank, a radiologist, and Mark Retchard, a medical device engineer, in an effort to overcome the shortcomings of core biopsies by using an automatic biopsy gun. Stereotactic VABB was introduced by Burbank and Parker in 1996 as a diagnostic tool to evaluate suspicious lesions visible on mammography. US-guided VABB was first performed by Zannis et al. in 1998. In Korea, VABB was introduced into several university hospitals and clinics in 2000. Next, radiologists at university hospitals adopted this procedure. Around 2002, VABB began generating publicity for its usefulness within academic circles because of efforts led by professors of surgery. At the time, there was much skepticism about the validity of other uses of VABB besides its diagnostic function. However, accumulated user experience and widespread use of 8-gauge (G) needles that made VABB easier led to more commonplace use of VABB for the therapeutic purpose of benign lesion removal. Later, the effectiveness of VABB became better known through the media and the internet. With breast examinations becoming common in women as young as their 20’s, excision of benign breast tumors by using VABB became more common. According to statistics provided by Park et al., of the 6,264 VABB procedures performed between January 2003 and April 2011, 61.5% of the cases were women in their 20s and 30s, demonstrating the public’s high interest in the procedure(50)
5. Biopsy
Breast cancer can only be accurately identified through a biopsy. The purpose of a biopsy is to remove tissues or cells from the patient’s body for laboratory testing. The pathologist’s report will determine whether or not cancer cells were discovered in the sample. The type of biopsy performed will depend on whether the lump is palpable, meaning you can feel it, or non-palpable, meaning you can’t. To locate the area to be tested, the doctor may use ultrasound or mammography. The majority of biopsies are performed in a hospital, and once they are complete, you can leave for home(51)
6,Diagnostic Breast MRI
MRI can also play a role in the diagnostic setting. For patients with skin changes consistent with serious breast disease, the guidelines recommend breast MRI be considered when biopsy of skin or nipple is found to be benign and the lesion is classiied as BI-RADS category 1 to 3. Because a benign skin punch biopsy in a patient with a clinical suspicion of inlammatory breast cancer (IBC) does not rule out malignancy, further evaluation is recommended (see page 1073). Evidence suggests that certain MRI features may facilitate diagnosis of IBC(52)
Staging of breast cancer
According to the report of breast cancer.org Stages of the breast cancer depends upon the size and type of tumor and how much the tumor cells have been penetrated in the breast tissues(53) Whereas stage 0 describes the non invasive and stage 4 describes the invasive kind of tumor. Descriptions of those tumor stages are
Stage 0
This is the non invasive stage of tumour which indicates that both cancerous and non cancerous cells are within the boundaries of that part of the breast in which the tumor begins to grow and no evidence found of their invasion in the surrounding tissues of that part, the example of this tumour stage is ductal cell carcinoma in situ (DCIS) (54) DCIS is a form of pure, noninvasive carcinoma and is most commonly identified by mammography showing microcalcifications confined to the breast ducts(55)
Stage 1
This stage describes as the invasive breast carcinoma and microscopic invasion is possible in this stage. It has two categories that are 1A and 1B stage. The category1A describes the tumor which measures up to 2 cm and none of the lymph nodes are involved in it while stage1B describes that small group of cancer cells larger than0.2 mm founds in lymph node(56)
Stage 2
Stage 2 also has two categories 2A and 2B. Stage 2Adescribes that the tumour is found in axillary lymph nodes or in sentinel lymph nodes but no tumor found in breast. The tumor can be smaller or larger than 2 cm but not more than 5 cm. However stage 2B describes that the tumor could be larger than 5 cm but can’t reach to the axillary lymph nodes(57).
Stage 3
It has been divided into three sub categories that are 3A,3B and 3C. Amongst which stage 3A describes that no tumor is found in breast but it can be found in 4–9 axil-lary lymph nodes or in sentinel lymph nodes while stage3B describes that the tumour can be of any size but have caused swelling or ulcer on the skin of the breast and can have spread up to 9 axillary lymph nodes or to sentinel lymph nodes stage 3B can be considered as inflammatory breast cancer which includes red, warm and swollen skin of the breast. However stage 3C describes the spread of tumor up to 10 or more than 10 axillary lymph nodes and it also have involved the lymph nodes above and below the clavicle (58).
Stage 4
This is the advanced and metastatic stage of cancer and this stage describes the spread to other organs of the body that is lungs, bones, liver brain etc (59) The 60% to 80% of patients with advanced breast cancer who develop metastases to the bones should be offered treatment with denosumab (Prolia) or bisphosphonates such as zoledronic acid (Reclast) or pamidronate (Aredia)(60)
Common Treatment Methods of Cancer
Surgery, chemotherapy and radiotherapy are considered as the most common methods of cancer treatment, although all of these treatment methods are not always useful and the clinical results are not acceptable.(61)
Treatment
Role of herbal medicine in cancer
From 200 to 1800 AD, following the teachings of Aristotle and Galen, which was believed that cancer, was a consequence of the coagulation of “black bile” till now when prevalence of biology has contributed to a 25% reduction in mortality [62], herbs play an important role in cancer symptom management, patients' quality of life and survival.
The main objectives of herbal therapies are:
The way herbal medicine fight cancer is significantly different from conventional chemical drugs, where no DNA mutation in surviving cell occurs. Specifically, natural compounds fight cancer by strengthening the immune system preventing the spread of cancer cells through inhibition of angiogenesis or growth of new blood vessels feeding the cancer cells, detoxifying the body and preventing further toxic build-up in the body, quenching free radicals that cause mutational changes that lead to cancer formation and supporting all targeted organs, especially those affected directly by the cancer. Besides creating an unfavourable environment for cancer growth is another benefit of herbal medicines, where, the ideal environment creates a high level of oxygen and temperature including increased metabolism rate, low sugar level and a high alkalinity space in the body [63].
Sources of traditional drugs
1.Herbal compound with anti-cancer activity
Phenolic compounds
Human diet includes a complex of herbal polyphenols. Studies have shown that these phenols hae cytotoxic effects on different tumors. Mechanisms of these compounds are carried out through apoptosis. Curcumin (Diferolelyl methane) is a phenol compound derived from rhizome of curcuma specie(64)
Turmeric
Experimental and clinical studies have demonstrated that turmeric, as well as its primary compound curcumin possess significant anti-cancer attributes, particularly in the context of BC(65) Scientific name of turmeric is Curcuma longa. Turmeric gives dark yellow color to food. Curcumin, the active ingredient of turmeric, is present in its rhizome and rootstock. Curcumin is known to have anticancerous activity due to its phenolic substances. Propagation of lung, breast, skin and stomach cancer is limited by turmeric (66) Curcuminoids are natural polyphenol compounds and there are three types namely diferuloylmethane (curcumin I), desmetoxicurcumin (curcumin II) and bisdemetoxicurcumin (Curcumin III). The primary curcuminoid is diferuloylmethane that has the highest concentration (77%) and gives turmeric its yellow color(67) Tumeric also contains sugars, resins, proteins as well as three main volatile oils (zingiberene, tumerone and atlatone) which possess pharmacological activity (68)
Green tea
Scientifically green tea is known as Camellia sinensis. Anticancer activity is attributed by polyphenolics compounds. Epigallocatechin (EGGG), a polyphenol is present in small amount in C. sinensis. Researchers have revealed that green tea possesses antitumor and anti-mutagenic activity. Cells are protected by EGGG from DNA damage produced by oxygen reactive species (69) The chemopreventive potential of green tea contrasts with the consistent results from animal models. Evidence of green tea consumption on breast cancer prevention and development is not supported by epidemiologic studies and the role of green tea consumption in breast cancer remains unclear. The results of antiproliferative effect of green tea extracts or its polyphenols from human studies are inconsistent and depend on the type of cancer(70)
Piperine
Piperine is a polyphenolic compound isolated from long and black peppers. Studies on the animal model show that piperine reduces the rate of lung cancer. Recently, piperine has been used as a chemosensitizer agent in combination with rapamycin to treat breast cancer(71)
Licorice
Scientific name: Glycyrrhiza glabra; Parts used: root. Dosage: 1 teaspoon of the root or subterranean stem, boiled in a covered container with 0.5 to 1.0 pints of water for about half an hour, at a slow boil. Allow the liquid to cool slowly in the closed container. Drink cold, 1 swallow or 1 tablespoon at a time, 1 to 2 cups per day. The multitude of pharmacological effects of licorice rhizomes and roots are practically all attributed to the presence of a triterpene saponin called glycyrrhizin, which is about fifty times sweeter than sugar, and has a powerful cortisone-like effect. Several cases have been reported in medical literature in which humans ingesting 6-8 ounces (a very large amount) of licorice candy daily for a period of several weeks are “poisoned” due to the cortisone-like effects of licorice extract in the candy. Proper treatment restores patients to normal. The above amount of this compound is very large compared with the relatively small amount found in supplements. In addition, Licorice rhizomes and roots have high mucilage content. When mixed with water, the resulting preparation has a very pleasant odor and taste, and acts as an effective demulcent on irritated mucous membranes, such as a sore throat. One study found that glycyrrhizin was as effective a cough suppressant as codeine. A experiment in 1991 with mice found that glycyrrhizin protected against skin cancer. The authors speculated that it might to be proved useful in protecting againstsome forms of human cancer as well. It is not surprising that licorice and glycyrrhizin have such wide applications. It should be noted that this chemical constitutes only 7% to 10% of the total root on a dry weight basis. Glycyrrhetic acid is obtained when acid hydrolysis is applied to the main component of licorice. This compound is extensively used in Europe for its anti-inflammatory properties, especially in Addison’s disease and peptic ulcer. Some European researchers concluded that glycyrrhetic acid may be preferred to cortisone because it is safer, especially when prolonged treatment isrequired. A study in 1990 demonstrated that glycyrrhetic acid exerts its activity not as a direct effect but by reducing the conversion of cortisol to cortisone, its biologically inactive product. The authors concluded that hydrocortisone, a “weak antiinflammatory agent,” can be greatly potentiated by the addition of 2% glycyrrhetic acid. To lessen the toxic effects of corticosteroids, the authors suggested that patients use hydrocortisone together with glycyrrhetic acid. Glycyrrhizin has also exhibited anti-viral activity. A study in 1979 demonstrated that glycyrrhizin inhibited EpsteinBarr virus, cytomegalovirus, and hepatitis B virus. In Japan, glycyrrhizin has long been successfully used to treat chronic hepatitis B. This has led to speculation that glycyrrhizin holds promise in the treatment of HIV. Side effects from the ingestion of large amounts of licorice have been reported. Glycyrrhizin in very large amounts can promote hypokalemia and hypertension. For these reasons people with heart problems and high blood pressure are advised to avoid consuming large quantities of licorice or its components[72-77].
Real-World Evidence from Traditional Chinese Medicine on Cancer
Clinical efficacy and safety have always been the core content of research in the field of traditional Chinese medicine. However, with the continuous deepening of research as well as its limitations, RCTs have been unable to meet the clinical demand of traditional Chinese medicine which is considered with unique diagnostic advantages. In recent years, how to scientifically and objectively evaluate the validity of traditional Chinese medicine in a real-world setting has become a hot topic in clinical research. As an important supplement to randomized controlled trials, real-world study is one of the approaches in line with the scientific research paradigm of TCM clinical research. Based on the characteristics of clinical diagnosis and treatment of traditional Chinese medicine, it collects a large amount of real-world data, as well as incorporates clinically meaningful outcomes, so as to mine and evaluate the efficacy and safety of traditional Chinese medicine in the real world.
Traditional Chinese medicine has remarkable effects on cancers in the clinical practice, either directly inhibiting the occurrence and development of tumors, or reducing the side effects caused by chemotherapy and radiotherapy, or reducing the dosage of other therapies. Kuo conducted a real-world analysis of 582,799 adult cancer patients in Taiwan based on whether they used traditional Chinese medicine. The main analysis was the use of traditional Chinese medicine, as well as specific medical visits. After the adjustment of age, gender, urbanization of residence, occupation, annual medical center visit, and annual nonmedical center visit, adjusted hazard ratios (aHR) for mortality were significantly lower among TCM users than those who do not get TCM. This study indicates that more attention should be paid to the use of traditional Chinese medicine in the clinical diagnosis and treatment of cancer patients [78]
CONCLUSION
Breast cancer remains one of the most prevalent and life-threatening malignancies affecting women worldwide, posing a significant challenge to global public health. The disease is multifactorial in nature, involving complex interactions among genetic predisposition, hormonal imbalance, environmental exposure, and lifestyle-related factors. Despite its increasing incidence, considerable progress has been made in understanding the epidemiology, pathophysiology, classification, and molecular mechanisms underlying breast cancer, leading to improved diagnosis and treatment outcomes. The availability of advanced screening and diagnostic methods such as mammography, ultrasound, biopsy, MRI, and computer-aided detection systems has greatly enhanced early detection, which plays a critical role in improving survival rates and reducing mortality.
Furthermore, advancements in therapeutic strategies including surgery, chemotherapy, radiotherapy, hormone therapy, targeted therapy, and immunotherapy have significantly improved disease management. The emergence of personalized medicine based on molecular subtypes such as luminal, HER2-positive, and triple-negative breast cancers has enabled more effective and patient-specific treatment approaches. In addition, growing evidence suggests that herbal medicines and natural compounds such as curcumin, green tea polyphenols, piperine, and licorice may offer complementary benefits in reducing treatment-associated side effects and supporting anticancer activity.
Overall, increasing awareness, regular screening, lifestyle modification, and early intervention remain essential for reducing the burden of breast cancer. Future research should focus on the development of more precise diagnostic biomarkers, safer therapeutic agents, and integrative treatment approaches to improve prognosis, quality of life, and long-term survival among breast cancer patients.
REFERENCES

Sanika Ingale, Pooja Koli, Dhanraj Jadge, A Comprehensive Review on Breast Cancer: Pathophysiology,Diagnosis, and Treatment Strategies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 745-762, https://doi.org/10.5281/zenodo.20526596
 10.5281/zenodo.20526596
10.5281/zenodo.20526596