
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
G. P. Pharmacy College, Vaniyambadi Main Road, Mandalavadi, Jolarpettai, Tirupattur 635851.
Transdermal Drug Delivery Systems (TDDS) have emerged as an effective and patient-friendly approach for delivering medications through the skin into the systemic circulation. These systems provide several advantages over conventional oral and injectable dosage forms, including avoidance of first-pass metabolism, sustained drug release, improved bioavailability, reduced dosing frequency, and enhanced patient compliance. The skin, while serving as a protective barrier, also presents challenges to drug permeation, making the understanding of skin structure and permeation mechanisms essential for successful transdermal formulation development.This review highlights the fundamental principles of transdermal drug delivery, including skin anatomy, pathways of drug permeation, and factors influencing drug absorption through the skin. It discusses the ideal characteristics of drugs suitable for transdermal administration, key formulation components such as polymers, adhesives, permeation enhancers, and backing membranes, as well as various preparation methods and evaluation parameters used in the development of transdermal patches. The review further explores therapeutic applications of transdermal systems in pain management, cardiovascular disorders, hormone replacement therapy, neurological conditions, and smoking cessation.Recent advancements involving nanotechnology-based carriers, microneedles, iontophoresis, sonophoresis, electroporation, and smart wearable drug delivery devices have significantly expanded the potential of TDDS. Despite certain limitations, including restricted drug selection and skin irritation concerns, continuous technological innovations are improving the efficiency and versatility of transdermal delivery systems. Overall, TDDS represent a promising and rapidly evolving drug delivery platform with significant potential to enhance therapeutic outcomes and support the future of personalized medicine
A transdermal drug delivery system (TDDS) is a specific device to deliver drugs through the skin into the blood stream, providing controlled and sustained therapeutic effects.
Allow the drug to penetrate the skin and reach the systemic circulation to produce the desired therapeutic effect. The quest for novel drug delivery systems has resulted in great progress in pharmaceutical sciences, including the field of Transdermal Drug Delivery Systems (TDDS). These systems, often referred to as "patches", are carefully formulated dosage forms designed to deliver a therapeutically effective amount of a drug through a patient's skin. The evolution of drug delivery systems has been driven by the need to optimize drug therapy. Conventional oral drug administration, while convenient, is often associated with limitations such as erratic absorption, hepatic first-pass metabolism, and the potential for gastrointestinal irritation. Such limitations can diminish drug bioavailability, necessitate frequent dosing regimens, and ultimately reduce patient compliance. In contrast, TDDS offer a potential alternative to the traditional delivery systems by providing sustained release of drug, avoiding first pass metabolism and reducing the fluctuations in plasma drug concentrations. The development of TDDS is a paradigm shift in drug delivery and has the potential to improve the therapeutic outcome of a wide variety of drugs. This review will discuss the basic principles of TDDS, advantages, limitations, mechanisms of drug permeation, critical components and recent advances in this dynamic field.
Early Topical Treatment Applications Topical treatments have been used for medicinal purposes for thousands of years, across cultures and civilizations. These early uses established the foundation for modern transdermal medication delivery systems. Here are some significant elements about the history and evolution of topical therapies.
1.1.1 Ancient Civilizations and Herbal Remedies
1.1.2 Medieval and Renaissance Periods
1.1.3 18th and 19th Centuries: Foundations of Modern Pharmacology
1.1.4 20th Century: Transition to Modern Transdermal Patches
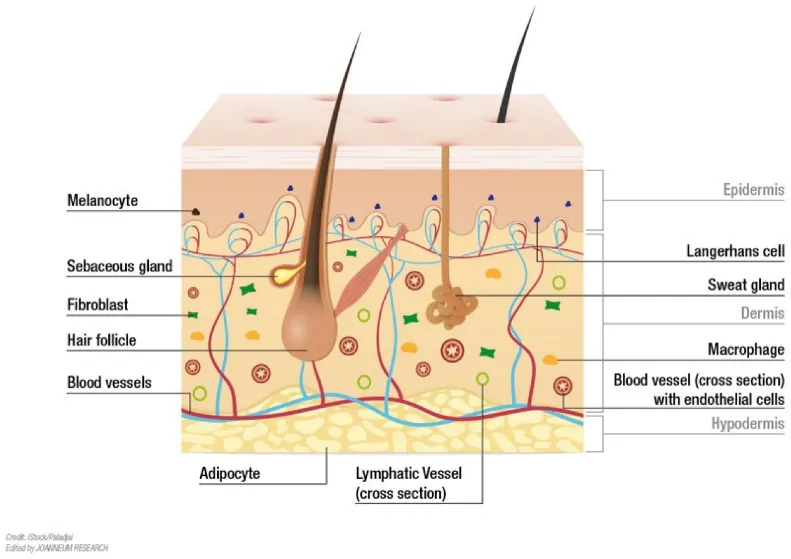
Figure 1: structure and physiology of skin
The graphic depicts the anatomical anatomy of human skin, including its three principal layers: epidermis, dermis, and hypodermis (subcutaneous tissue), as well as accompanying appendages and cellular components. Understanding skin anatomy is critical in the design and evaluation of transdermal drug delivery systems (TDDS), as the skin serves as both a protective barrier and a channel for drug absorption.
1.2.1 Epidermis: The epidermis is the skin's outermost layer and serves as the primary barrier to external agents. It contains:
Melanocytes are cells that produce melanin, which protects the skin from ultraviolet (UV) radiation.
Langerhans cells are specialized immune cells that play a role in antigen presentation and skin defence.
1.2.2 Dermis:
The dermis resides beneath the epidermis and is made up of connective tissue, blood vessels, nerves, and skin appendages. The components depicted in the illustration include Fibroblasts are cells that produce collagen and elastin, which provide structural support and elasticity to the skin.
Hair Follicles: Structures from which hair grows; they can act as alternate routes for drug entry.
Sebaceous Glands: Glands found near hair follicles that release sebum to moisturize the skin and hair.
Sweat glands: They are the glands that produce sweat and regulate body temperature.
Blood vessels: provide nutrition and oxygen to epidermal tissues and play an important role in systemic medication absorption following transdermal administration.
Macrophages: They are immune cells that phagocytose and defend tissues.
1.2.3 Hypodermis (subcutaneous tissue):
The hypodermis is the deepest skin layer and is mostly composed of: Adipocytes (Fat Cells) provide insulation, cushioning, and energy storage. Lymphatic Vessels: Aid in fluid drainage and immunological response. Larger blood arteries that link the skin to the systemic circulation.
The skin forms a selectively permeable barrier. Different medications infiltrate the skin at varying speeds. The flux (J) represents the amount of medication penetrated per unit area and time (typically µgcm−2h−1). The flow is defined by (a) the skin's permeability to the permeant and (b) the concentration gradient (∆C) of the permeant across the skin (typically µgmL−1), according to Eq. 1: J = Kp·∆C.
Eq. 1 defines skin permeability using the permeability coefficient, Kp (typically cmh−1). For passive drug absorption, the permeability coefficient is calculated by combining the partition coefficient (P), diffusion coefficient (D), and diffusional path length (h) in Eq. 2.
The physicochemical features of the permeant, such as molecular mass and hydrophilicity, significantly impact partitioning and diffusion processes, resulting in skin permeability (Eq. 2). Molecules that permeate the skin typically have a molecular mass of less than 500Da and are moderately hydrophilic, with an octanol-water partition coefficient (log Poctanol-water) of 1-3. Equation 3 [2] describes the quantitative link between skin permeability (Kp), molecular mass (MW), and hydrophilicity (log Poctanol-water). log Kp = 0.71 log Poctanol-water - 0.0061 MW - 2.74 (Eq. 3)
Other parameters that may impact skin permeability include hydrogen bond activity, molecular volume, melting point, and solubility. Mathematical models have been developed to understand how these characteristics affect skin permeability [3,4].
Permeation Pathways
A molecule can permeate through the skin via either the trans epidermal pathway (diffusing across the skin layers) or the appendageal pathway (through hair follicles or sweat ducts) (Fig. 2). The combined flux of these two pathways determines the overall observed flux across the skin.
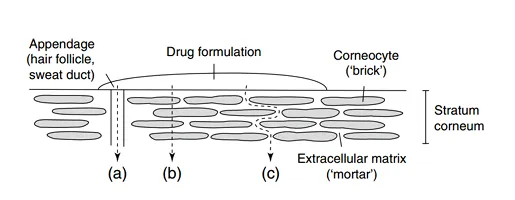
Figure 2: Drug permeation pathways in the skin (stratum corneum shown): (a) the ap pendageal route, (b) the transcellular route, and (c) the tortuous extracellular route. The transcellular and intercellular routes constitute the trans epidermal pathway.
Transdermal absorption (TA) is influenced by a complicated set of variables that work together. Clinical reaction to TDDS application is a step-by-step process:
1.4.1 Biological factor
Biological factors such as skin thickness, regional location, age, blood flow rate, and skin condition can all impact penetration and permeation.[5] Skin permeability can be affected by physical, chemical, and pathological factors, including UV, infrared, and ionizing radiation.[6,7] Mixtures of polar and non-polar solvents can delipidize skin, Create artificial shunts in the skin.[8] Using certain solvents can significantly reduce the skin's barrier function. The significance of drug metabolism in the skin has been overlooked in previous research. Recent results indicate that studying skin metabolism is important for designing and activating prodrugs.[9,10]
1.4.2 Physicochemical factors
Percutaneous absorption is influenced by the physicochemical properties of both the medication and the medium, in addition to the stratum comeum structure.[11,12] The things to consider are the drug's molecular characteristics and the vehicle. The TA of a drug depends on its molecular weight, size, structure, partition coefficient, pH, and concentration on the skin's surface,[13,14] as well as the nature and effect of the vehicle and other chemicals that may promote sorption. The impact of individual parameters on penetration and permeation is a crucial aspect of dermal/TDDS.[15,16]
1.5.1Advantages
1.5.2 Limitations
3.1 Drug (API)
The selection of APIs for transdermal delivery is critical. Ideal candidates are drugs with:
3.2 Polymer Matrix
The polymer matrix is an important component of transdermal patches because it contains the medicine and regulates its release. There are numerous polymers that can be employed, each with its own set of features to meet various drug delivery requirements. Examples of polymers used in transdermal patches are:
3.3 Permeation Enhancers
Permeation enhancers are chemicals that increase skin permeability, hence improving medication absorption. Common enhancers are:
3.4 Adhesives
Adhesives are crucial for ensuring the patch adheres to the skin. Commonly used adhesives include:
The backing layer provides structural support while also protecting the patch from environmental elements. It is often composed of:
Release liners protect the adhesive layer and are removed before patch application. They are usually composed of:
4.1 Asymmetric TPX Membrane Method:
The dry or wet inversion procedure is used to prepare them. In order to create a polymer solution, TPX is dissolved at 60°C in a mixture of solvent (cyclohexane) and non-solvent additives. After a full day at 40°C, the polymer solution is cast onto a glass plate. The glass plate must then be submerged right away in a coagulation bath (temperature maintained at 25°C) after the casting film has been evaporated for 30 seconds at 50°C. The membrane can be taken out after 10 minutes of immersion and allowed to air dry for 12 hours at 50°C in a circulation oven.
4.2 Circular Teflon Mould Method:
Baker and Heller discovered it in 1989. Polymeric solutions in varying amounts are utilized as organic solvents. Then the solution is separated into two halves. Dissolve a calculated amount of medication in one part and varied concentrations of enhancers in another. Mix the two parts together. A plasticizer (such as Di-Nbutylphthalate) is added to the drug polymer solution. Stir the mixture for 12 hours before pouring into a round Teflon mould. To manage solvent vaporization in a laminar flow hood model, position the moulds on a level surface and cover them with an inverted funnel. An airspeed of 0.5 m/s. The solvent is allowed to evaporate for 24 hours. After drying, the film should be stored for 24 hours at 25±0.5°C in a silica gel desiccator before evaluation to prevent aging effects.
4.3 Mercury Substrate Method:
In this process, the medication and plasticizer are dissolved in polymeric solution. Stir for 10-15 minutes to create a homogeneous dispersion. Pour into a leveled mercury surface and cover with an inverted funnel to control solvent evaporation.
4.4 By Using “IPM Membranes” Method:
The medication is distributed in a mixture of water and Carbomer 940 polymer (containing propylene glycol) and swirled for 12 hours using a magnetic stirrer. To neutralize and make the dispersion thick, add triethanolamine. To generate solution gel with low drug solubility in aqueous solution, use Buffer pH 7.4. The produced gel will be integrated into the IPM membrane.
4.5 By Using “EVAC Membranes” Method:
TDS preparation requires a rate control membrane consisting of 1% carbopol reservoir gel, polyethelene (PE), and ethylene vinyl acetate copolymer (EVAC). If the medicine is not soluble in water, use propylene glycol for gel formation. After dissolving the drug in propylene glycol, add carbopol resin and neutralize with a 5% w/w sodium hydroxide solution. The medicine (in gel form) is deposited on a backing layer that covers the desired area. To create a leak-proof device, lay a rate-controlling membrane over the gel and seal the borders with heat.[19]
5.1 Pre-Formulation Study
Physicochemical parameters include the drug's solubility, partition coefficient, pH, and melting point. Polymer selection ensures optimal adhesion, medication release and mechanical quantities
5.2 Physicochemical Evaluation
Appearance: smoothness, transparency, and homogeneity. Thickness: A micrometer or Vernier caliper was used to take the measurements. Weight Variation: Ensures consistent distribution of components.
5.3 Adhesion and Mechanical Properties
Tensile strength determines mechanical strength.
5.4 Permeation Studies
Skin permeation was assessed using excised animal or human cadaver skin in Franz diffusion cells. Enhancement studies: The effect of permeation enhancers is investigated.
5.5 In-vivo Evaluation Skin irritation or sensitization:
Therapeutic efficacy is measured in clinical trials.
5.6 Stability Studies
Followed ICH requirements in accelerated conditions (temperature and humidity) to guarantee patch integrity, adhesion, and medication content stability.
Physical approach: To open the skin's pores, physical enhancers physically engage with the skin in a variety of ways, causing harm to the skin's integrity. It was discovered that iontophoresis and permeation enhancers worked well together to deliver drugs.
Iontophoresis:
An electrode with the same charge as the drug molecules is placed on the skin, and a current of a few milliamperes (less than 0.5 mA) is applied. The electrode declines the drug molecules with the same charge through the skin to the electrode with the opposite charge, and the drug is delivered quickly. For improved outcomes, iontophoresis can be combined with chemicals, electrophoresis, or ultrasound.
SONOPHORESIS:
The medicine is delivered through the skin by breaking the lipid bilayer when sound waves with frequencies between 20 KHz and 10 MHz are applied to the skin for 15 seconds. When the medication is combined with a coupling agent, both the medication and the sound waves are transmitted through the skin. By eliminating first-pass metabolism, efflux transporters, digestive enzymes, and adverse circumstances associated with other oral administration, this method allows bioactive compounds to enter the systemic circulation directly.
CHEMICAL APPROACHES:
Chemical permeation enhancers and iontophoresis improve the penetration of antihypertensive agents through the skin. The combination of iontophoresis with permeation enhancers was shown to be promising in delivering atenolol across the skin, with the maximum penetration attained when oleic acid was used as a chemical enhancer with iontophoresis. The in vitro flux value (when oleic acid was paired with iontophoresis) was 0.71 mg/cm2/h, indicating that a therapeutically appropriate concentration can be achieved with 1.2cm2 of skin area.[21]
MULTIPLE OR DOUBLE EMULSION:
Multiple emulsion systems are new technologies with promise oral administration. Multiple emulsions, also known as emulsions of emulsions, are made up of liquid that is miscible with and sometimes identical with the continuous phase. This is made feasible via twofold emulsification, hence the name double emulsion. It contains both hydrophilic and lipophilic emulsifiers that are used to generate numerous emulsions.
Double emulsions aid to keep drug concentrations within the therapeutic range in lymph vessels. Drugs are transported to mesenteric lymph nodes rather than straight into the portal system because they are encapsulated by the oil phase, which has a higher lipophilic character and so is absorbed by lymphatic channels. Furthermore, w/o/w emulsions may serve as carriers for the delivery of polypeptide/protein drugs, which require both protection from gastric fluids and delivery via lymph nodes.
SOLID LIPID NANOPARTICLES (SLNS):
It is an aqueous colloidal dispersions made of biodegradable lipids. They can be found in emulsions, liposomes, and polymeric micro- and nanoparticles. SLNs have gained popularity due to their increased solubility and oral bioavailability through various mechanisms.[22]
Characterization procedures are critical in evaluating the quality, performance, and stability of transdermal patches. Here are some important characterisation techniques:
7.1 Physical Characterization:
7.2 Mechanical Characterization:
7.2.1 Adhesive Properties:
7.2.2 Drug Release Studies:
7.2.3 Microscopic Analysis:
7.3 Chemical Characterization:
Transdermal patches are used for a variety of medicinal purposes
8.1 Pain Management:
Patches containing fentanyl, lidocaine, or diclofenac offer long-lasting analgesia for chronic pain and cancer patients.
8.2 Hormone Replacement Therapy:
Estradiol and testosterone patches treat menopausal symptoms and hypogonadism, respectively.
8.3 Cardiovascular Disorder:
Medications for cardiovascular disorders include nitroglycerin patches for angina and clonidine patches for hypertension.
8.4 Central Nervous System Disorders:
Patches containing rivastigmine for Alzheimer's disease and methylphenidate for ADHD improve compliance in both geriatric and pediatric populations.
8.5 smoking cessation:
Nicotine patches can alleviate withdrawal symptoms and cravings during smoking cessation programs.
8.6 Contraception:
Scopolamine patches can help avoid motion sickness and post-operative nausea. Transdermal devices containing estrogen and progestin offer weekly contraceptive coverage.
Nanotechnology has shown promise in improving topical and transdermal drug delivery, particularly for biologics. Biologics are gaining popularity in transdermal administration due to their biological barriers that limit medication absorption. Novel therapeutics for inflammatory illnesses include tralokinumab, baricitinib, and anti-IL-4R antibodies. The FDA has approved ruxolitinib cream, the first topical JAK inhibitor, to treat mild to severe atopic dermatitis that cannot be effectively managed with conventional topical medicines.[32]
Hyaluronic acid-based solutions are becoming prominent in the pharmaceutical industry due to their high permeability and biocompatibility. Hyaluronic acid-based nanoparticles, ethosomes, and liposomal transdermal systems are utilized to treat anti-inflammatory illnesses such atopic dermatitis and psoriasis. Researchers are exploring physical penetration approaches for transdermal delivery, including sonophoresis, iontophoresis, and electroporation, in addition to microneedles. These approaches are widely regarded as effective, safe, and have a high medication bioavailability. Electroporation uses tiny electrical impulses to improve the entry of hydrophilic medicines into the stratum corneum. Sonophoresis uses ultrasonic waves at different frequencies to break the epidermal barrier and increase medication penetration. Iontophoresis uses an electric field to drive molecules into the skin, resulting in fast medication release for both charged and uncharged molecules. Low-frequency ultrasound promotes better drug penetration than high-frequency ultrasound. However, patient-specific models present hurdles in terms of cost and large-scale viability. These emerging approaches have the potential to transform transdermal drug delivery, providing patients with better treatment alternatives.[33]
While transdermal patch technology has several benefits in medication administration, it also has some problems and limits that prevent general adoption and efficacy [34,35]. Addressing these problems is critical for moving the field forward and realizing the full potential of transdermal patch technology. This section delves into some of the primary issues and constraints found during transdermal patch development and distribution.
11.1 Developing Advanced Skin Penetration Technologies:
New technologies like microneedles, iontophoresis, sonophoresis, electroporation, and thermal ablation are enhancing medication absorption through the skin barrier. These approaches can help transport big molecules like peptides, proteins, and vaccinations that were previously difficult to inject transdermally.
11.2 Integration of Nanotechnology:
Nanocarriers such as liposomes, niosomes, ethosomes, transferosomes, solid lipid nanoparticles, and nanostructured lipid carriers are thought to promote medication penetration, bioavailability, and controlled release. Transdermal systems based on nanotechnology have the potential to change chronic illness management.
11.3 Personalised medicines:
Future transdermal patches could be tailored to individual patients' needs, taking into account characteristics such as age, body weight, medical state, and genetic profile. Personalized patches can improve therapeutic success while reducing side effects.
11.4 Smart and Wearable Drug Delivery Systems:
The incorporation of sensors, microelectronics, and wireless communication technologies into transdermal patches is resulting in intelligent medication delivery systems.
These devices can monitor physiological factors and automatically alter drug release in response to patient needs.
11.5 Delivery of biopharmaceuticals:
The goal of the research is to enable transdermal administration of biologics such insulin, growth hormones, vaccines, monoclonal antibodies, and nucleic acid-based therapies. This development has the potential to eliminate the need for injections and enhance patient compliance.
11.6 Improved Treatment of Chronic Disease:
Future TDDS applications are predicted to include the management of diabetes, cardiovascular disease, neurological disorders, pain management, hormone replacement therapy, and cancer treatment via sustained and targeted medication delivery.
11.7 Improved patient compliance:
Transdermal methods provide painless administration, reduced dose frequency, and the prevention of gastrointestinal adverse effects. These benefits will continue to boost their use, especially among pediatric, geriatric, and chronic disease patients.
11.8 Combined Drug Delivery Systems:
Researchers are developing patches that can deliver many medications at once. Such methods may enhance therapy efficacy and simplify treatment regimens for complex disorders.
11.9 Sustainable and biodegradable materials:
The future of TDDS includes the development of ecologically friendly and biodegradable polymers that reduce waste and improve biocompatibility while maintaining drug delivery performance.
11.10 Expanded Vaccine Delivery:
Microneedle-based transdermal vaccination delivery methods have demonstrated substantial promise. They provide pain-free administration, greater immunological responses, and easier storage and transportation than traditional injections.
CONCLUSION
Transdermal drug delivery systems (TDDS) have emerged as a potential and successful alternative to traditional drug delivery methods, thanks to its capacity to provide regulated and sustained release of therapeutic substances through the skin. Transdermal patches are formulated by carefully selecting medicines, polymers, adhesives, plasticizers, and permeation enhancers to promote optimal drug release skin permeation. Various preparation processes and evaluation parameters are critical in ensuring that the generated patches are of high quality, safe, effective, and stable. The examination of transdermal patches using physicochemical, mechanical, and permeation tests aids in establishing their performance and therapeutic utility. Recent innovations such as microneedles, nanocarrier-based systems, iontophoresis, and smart transdermal technologies have considerably increased the scope of transdermal drug delivery, allowing for the administration of a broader range of medications with enhanced bioavailability and patient compliance. Despite problems such as restricted drug penetration, skin irritation, and formulation complications, ongoing research and technology advancements are overcoming these constraints. The increased interest in non-invasive drug delivery technologies and individualized medicine emphasizes the utility of transdermal patches in modern healthcare. As a result, transdermal patches constitute a valuable and expanding drug delivery platform with tremendous potential for future pharmaceutical development and therapeutic applications.
REFERENCES
P. Balamurugan, A Comprehensive Review on Transdermal Drug Delivery Systems: Principles, Formulation, Evaluation, Recent Advances and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6769-6782, https://doi.org/10.5281/zenodo.20928150
 10.5281/zenodo.20928150
10.5281/zenodo.20928150