
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,5 Pathgene Health Care Pvt.Ltd.1-212, Tiruchanoor Rd, Srinivasapuram, Padmavati Nagar, Tirupati, Andhra Pradesh 517503. India
3 Toxgene AR Biolabs Pvt.Ltd.Plot no 31,32,41&42, APIIC Industrian Park, Chandragiri, Tirupati,, Andhra Pradesh 517102. India.
4 Sri Maruthi Hospitals, Tirupati.
Tuberculosis (TB) remains one of the most significant infectious diseases worldwide and continues to pose a major public health challenge despite substantial advances in diagnosis and treatment. According to the World Health Organization (WHO) Global Tuberculosis Report 2024, TB has re-emerged as the leading cause of death from a single infectious agent, affecting millions of people annually, particularly in low- and middle-income countries. The disease is caused by Mycobacterium tuberculosis, a slow-growing intracellular pathogen capable of establishing latent infection and causing severe pulmonary and extrapulmonary manifestations. The persistence of TB is further complicated by factors such as HIV co-infection, socioeconomic disparities, delayed diagnosis, and the emergence of multidrug-resistant (MDR-TB) and extensively drug-resistant tuberculosis (XDR-TB). This review provides a comprehensive and up-to-date overview of tuberculosis, encompassing its global epidemiology, microbiological characteristics, immunopathogenesis, clinical manifestations, and current diagnostic approaches. Special attention is given to recent advances in molecular diagnostics, including nucleic acid amplification tests and whole-genome sequencing, as well as contemporary pharmacological treatments and novel anti-tubercular agents. Furthermore, emerging strategies such as host-directed therapies, vaccine development, and artificial intelligence-based screening and diagnostic tools are discussed. This review aims to serve as a consolidated scientific resource for researchers, healthcare professionals, and policymakers involved in tuberculosis prevention, diagnosis, treatment, and control.
Tuberculosis is a chronic, communicable disease caused by Mycobacterium tuberculosis, a highly adaptable intracellular pathogen that has co-evolved with humans for thousands of years [1]. Despite remarkable progress in medical science, tuberculosis continues to be a major global health concern, particularly in low- and middle-income countries [2]. The disease primarily affects the lungs, leading to pulmonary tuberculosis, but it also has the capacity to involve multiple extrapulmonary sites, including the lymphatic system, bones, central nervous system, and genitourinary tract [3,4,5]. This systemic potential contributes to its clinical complexity and diagnostic challenges. One of the defining features of tuberculosis is its ability to exist in two distinct states: active disease, which is symptomatic and transmissible, and latent infection, in which the bacteria remain dormant within the host without causing immediate clinical manifestations.The transmission of tuberculosis occurs predominantly through airborne particles known as droplet nuclei, which are expelled when individuals with active pulmonary TB cough, sneeze, speak, or even sing[6]. These microscopic particles can remain suspended in the air for prolonged periods, especially in enclosed, poorly ventilated environments. Consequently, overcrowding, inadequate ventilation, and prolonged exposure significantly increase the risk of infection [7]. Once inhaled, the bacilli reach the alveoli of the lungs, where they interact with the host immune system. While many individuals successfully contain the infection through immune mechanisms, a substantial proportion develop latent infection, which can later reactivate under conditions of immune compromise [8]. Despite sustained global control efforts, tuberculosis remains one of the leading causes of death from infectious diseases worldwide. According to recent reports by the World Health Organization, TB continues to rank above many other infectious diseases in terms of mortality, reflecting persistent gaps in detection, treatment, and prevention. The ongoing burden of TB is not merely a reflection of biological factors but is deeply intertwined with social and economic determinants of health. Poverty, malnutrition, limited access to healthcare, and lack of awareness significantly contribute to both susceptibility and disease progression[9,10,11]. These factors create a cycle in which vulnerable populations are disproportionately affected, thereby sustaining transmission within communities. The persistence of tuberculosis is multifactorial and involves a complex interplay between pathogen biology, host immune responses, and environmental influences. One of the most critical aspects of TB pathogenesis is the ability of M. tuberculosis to evade host immune defenses. Following phagocytosis by macrophages, the bacteria can inhibit normal intracellular killing mechanisms, allowing them to survive and replicate within host cells. This intracellular persistence facilitates the formation of granulomas, which are organized immune structures designed to contain the infection [12,13]. While granulomas are essential for controlling bacterial spread, they also serve as reservoirs for dormant bacilli, thereby contributing to latent infection and the potential for future reactivation. A nother important dimension of tuberculosis epidemiology is its strong association with immunocompromising conditions, particularly human immunodeficiency virus (HIV) infection. HIV significantly increases the risk of progression from latent to active TB by weakening cell-mediated immunity, which plays a central role in controlling M. tuberculosis. In addition to HIV, other conditions such as diabetes mellitus, chronic kidney disease, and malnutrition have been identified as important risk factors [14]. Lifestyle factors, including smoking and alcohol use, further exacerbate susceptibility by impairing immune function and lung integrity. In recent decades, rapid urbanization and increased global mobility have contributed to the spread of tuberculosis across geographical boundaries. Migration from high-burden regions to low-burden areas has introduced new challenges in TB control, including the need for effective screening and management of latent infection. Urban slums, characterized by overcrowding and poor living conditions, act as hotspots for transmission, emphasizing the role of social determinants in shaping disease patterns. Additionally, healthcare disparities, including limited access to diagnostic facilities and treatment services, hinder timely intervention and contribute to ongoing transmission. The emergence of drug-resistant forms of tuberculosis represents another major challenge in the global fight against the disease. Multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB) have arisen largely due to incomplete or inappropriate treatment, highlighting the importance of adherence to therapeutic regimens. These resistant forms require longer, more complex, and often more toxic treatment strategies, which further complicates disease management and increases healthcare costs. The growing prevalence of drug resistance underscores the need for improved treatment protocols, novel therapeutic agents, and robust public health interventions. In addition to biological and clinical challenges, tuberculosis control is influenced by health system factors, including diagnostic capacity, treatment infrastructure, and surveillance mechanisms. Early and accurate diagnosis is essential for effective disease control, yet many cases remain undetected or are diagnosed late, particularly in resource-limited settings. Advances in molecular diagnostics have improved detection rates, but their accessibility remains uneven across different regions. Strengthening healthcare systems and ensuring equitable access to diagnostic and treatment services are critical components of TB control strategies. In conclusion, tuberculosis remains a complex and multifaceted disease that continues to pose significant challenges to global health. Its persistence is driven by a combination of biological adaptability, socioeconomic factors, and healthcare limitations. Addressing these challenges requires a comprehensive approach that integrates biomedical research, public health interventions, and social policy measures. A deeper understanding of the disease and its determinants is essential for developing effective strategies aimed at reducing transmission, improving treatment outcomes, and ultimately achieving the goal of tuberculosis elimination.
2. GLOBAL EPIDEMIOLOGY AND BURDEN:
The global burden of tuberculosis continues to be a major public health concern, reflecting persistent challenges in disease control despite decades of coordinated international efforts. Tuberculosis remains widely distributed across the globe, with cases reported in nearly all countries, although the intensity of the burden varies considerably by region. According to recent assessments by the World Health Organization, TB affects millions of individuals annually and remains one of the leading causes of death from a single infectious agent. The widespread distribution of the disease underscores the need for sustained global commitment toward surveillance, prevention, and treatment strategies. A substantial proportion of tuberculosis cases is concentrated in low- and middle-income countries, particularly in regions of South-East Asia and sub-Saharan Africa. Countries such as India, Indonesia, China, Nigeria, and South Africa collectively account for a significant share of the global TB burden. The high incidence in these regions can be attributed to a combination of demographic, socioeconomic, and healthcare-related factors [16]. Rapid population growth, urbanization, and the expansion of densely populated settlements contribute to increased transmission dynamics. Furthermore, limited healthcare infrastructure and disparities in access to diagnostic and treatment services hinder effective disease management, allowing TB to persist within communities. Recent global estimates suggest that approximately ten million individuals develop tuberculosis each year, with a considerable number of cases remaining either undiagnosed or unreported. This gap between estimated incidence and reported cases highlights deficiencies in case detection and surveillance systems, particularly in resource-limited settings. In addition to incidence, mortality associated with tuberculosis remains alarmingly high, with over one million deaths reported annually [17]. Mortality rates are especially elevated in populations with limited access to timely diagnosis and effective treatment, emphasizing the importance of strengthening healthcare delivery systems. The epidemiology of tuberculosis is closely linked to a range of biological and social risk factors that influence both susceptibility to infection and progression to active disease. Among these, infection with human immunodeficiency virus (HIV) represents one of the most significant contributors to the TB burden. HIV compromises cell-mediated immunity, which is essential for controlling Mycobacterium tuberculosis, thereby increasing the likelihood of reactivation of latent infection. Co-infection with TB and HIV presents a major clinical challenge, as it complicates diagnosis, treatment, and patient outcomes. Regions with high HIV prevalence often report correspondingly high TB incidence rates, illustrating the synergistic relationship between these two diseases. In addition to infectious comorbidities, non-communicable diseases such as diabetes mellitus have emerged as important risk factors in TB epidemiology. Diabetes impairs immune function and alters host defense mechanisms, thereby increasing vulnerability to infection and disease progression. The rising global prevalence of diabetes, particularly in developing countries, is expected to further influence TB trends in the coming years. Similarly, malnutrition remains a critical determinant of TB risk, as it weakens the immune system and reduces the body’s ability to mount an effective response against the pathogen. Undernourished individuals are more likely to develop active disease and experience poor treatment outcomes. Lifestyle-related factors, including tobacco smoking and alcohol consumption, also play a significant role in the epidemiology of tuberculosis. Smoking damages the respiratory tract and impairs local immune defenses, increasing susceptibility to infection. Alcohol use, particularly chronic consumption, is associated with weakened immunity and poor adherence to treatment, both of which contribute to increased disease burden [18,19]. These behavioral factors often coexist with socioeconomic disadvantages, further amplifying the risk of TB in vulnerable populations. Socioeconomic determinants are central to understanding the global distribution of tuberculosis. Poverty remains one of the strongest predictors of TB incidence, as it is associated with overcrowded living conditions, poor nutrition, and limited access to healthcare services. Overcrowding facilitates the transmission of airborne infections, while inadequate ventilation increases the concentration of infectious particles in indoor environments. In many high-burden settings, individuals live in close proximity with limited access to basic amenities, creating ideal conditions for the spread of TB. Additionally, lack of education and awareness about the disease contributes to delayed healthcare-seeking behavior, resulting in prolonged periods of infectiousness and increased transmission. Healthcare system factors also significantly influence TB epidemiology. Delays in diagnosis, inadequate treatment regimens, and poor patient adherence contribute to ongoing transmission and the emergence of drug-resistant strains. In many regions, diagnostic facilities are either unavailable or inaccessible, leading to reliance on less sensitive methods and underdiagnosis of cases. Even when treatment is available, socioeconomic barriers such as cost, distance, and stigma may prevent individuals from completing therapy. These challenges highlight the importance of strengthening healthcare infrastructure and implementing patient-centered approaches to TB management. Another important aspect of the global TB burden is the increasing concern of drug-resistant tuberculosis. Multidrug-resistant TB and extensively drug-resistant TB have emerged as significant threats to disease control, particularly in areas with weak health systems and poor treatment adherence. The presence of drug-resistant strains not only complicates treatment but also increases transmission risk, as these forms of TB are more difficult to cure and require prolonged therapy. Addressing drug resistance requires coordinated efforts involving improved diagnostic capacity, effective treatment strategies, and robust monitoring systems. In recent years, global initiatives aimed at reducing the burden of tuberculosis have made notable progress, including expanded access to diagnostic tools, improved treatment coverage, and enhanced surveillance systems. However, progress remains uneven across regions, and significant gaps persist in achieving universal access to TB care. The ambitious targets set by international programs, such as the End TB Strategy, emphasize the need for accelerated efforts to reduce incidence and mortality rates. Achieving these goals will require not only biomedical interventions but also broader social and economic reforms aimed at addressing the underlying determinants of the disease. In conclusion, the global epidemiology of tuberculosis reflects a complex interplay of biological, social, and environmental factors that continue to drive disease transmission and persistence [20]. While significant advancements have been made in understanding and managing TB, the burden remains substantial, particularly in vulnerable populations. A comprehensive and integrated approach that addresses both medical and social determinants is essential for reducing the global impact of tuberculosis and moving toward its eventual elimination.
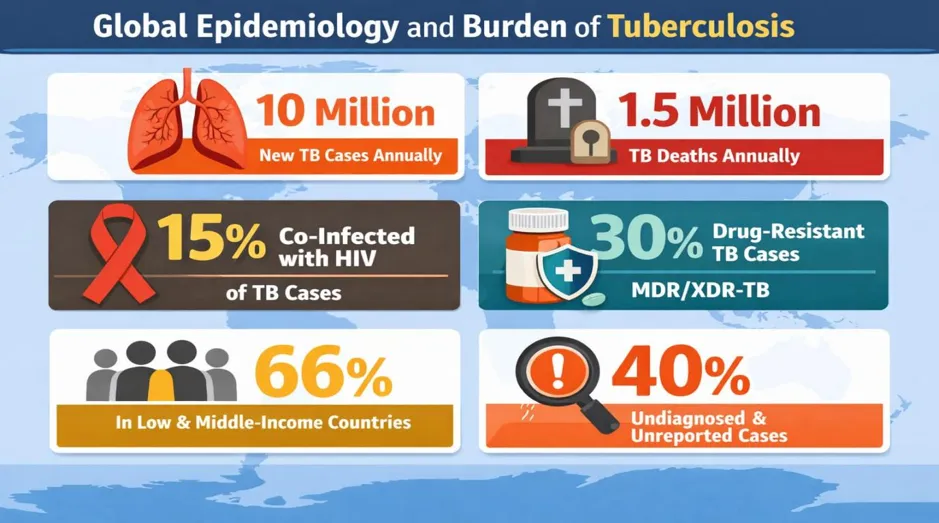
Figure: Global Epidemiology and Burden of Tuberculosis
3. ETIOLOGY AND MICROBIOLOGICAL FEATURES:
Mycobacterium tuberculosis is an acid-fast, aerobic bacillus characterized by a lipid-rich cell wall containing mycolic acids. This unique structure provides resistance to environmental stress and many antimicrobial agents [21,22]. The organism exhibits slow growth, with a generation time significantly longer than most bacteria, which contributes to delays in diagnosis and treatment [23]. The pathogen possesses several virulence factors that enable intracellular survival, including inhibition of phagosome-lysosome fusion and modulation of host immune signaling pathways. These mechanisms allow the bacteria to persist within macrophages, leading to chronic infection and immune evasion. [24]. The etiological agent responsible for tuberculosis is Mycobacterium tuberculosis, a member of the Mycobacterium tuberculosis complex, which includes closely related species such as M. bovis, M. africanum, and M. microti. Among these, M. tuberculosis is the principal pathogen causing disease in humans. It is an obligate aerobic, non-motile, rod-shaped bacillus that exhibits distinctive staining properties due to its unique cell wall composition. The organism is classified as acid-fast, meaning it retains certain dyes such as carbol fuchsin even after treatment with acid-alcohol, a characteristic that forms the basis of Ziehl–Neelsen staining widely used in diagnostic microbiology. One of the most defining structural features of M. tuberculosis is its complex and lipid-rich cell envelope. Unlike typical Gram-positive or Gram-negative bacteria, the mycobacterial cell wall contains a high concentration of long-chain fatty acids known as mycolic acids, which are covalently linked to an underlying arabinogalactan-peptidoglycan complex. This highly hydrophobic barrier imparts several critical properties to the organism, including resistance to desiccation, chemical damage, and many antimicrobial agents. The cell wall also contains glycolipids such as lipoarabinomannan (LAM), which play a key role in modulating host immune responses. The impermeability of this lipid-rich envelope significantly limits the entry of many antibiotics, contributing to the intrinsic resistance of M. tuberculosis and necessitating prolonged multidrug therapy for effective treatment. In addition to its structural complexity, M. tuberculosis is characterized by its remarkably slow growth rate. The organism has a generation time of approximately 15–20 hours, which is considerably longer than that of most bacterial pathogens. This slow replication contributes to the chronic nature of tuberculosis and poses challenges for laboratory diagnosis, as culture-based methods may require several weeks to yield results. The slow metabolic activity of the bacillus also reduces its susceptibility to antibiotics that target actively dividing cells, further complicating treatment. Moreover, M. tuberculosis can enter a non-replicating or dormant state under unfavorable conditions, allowing it to persist within the host for extended periods without causing active disease. A critical aspect of the microbiological behavior of M. tuberculosis is its ability to survive and replicate within host macrophages, which are typically responsible for eliminating invading pathogens. Upon inhalation, the bacilli are engulfed by alveolar macrophages through phagocytosis. However, instead of being destroyed, M. tuberculosis employs multiple strategies to evade intracellular killing. One of the key mechanisms involves the inhibition of phagosome-lysosome fusion, preventing the formation of an acidic and enzyme-rich environment that would normally degrade the pathogen. By maintaining a relatively neutral pH within the phagosome, the bacteria create a favorable niche for survival and replication. The pathogen also produces a variety of virulence factors that contribute to its persistence and pathogenicity. These include proteins and lipids that interfere with host immune signaling pathways, thereby modulating the host response to infection. For instance, certain secreted proteins can inhibit the production of pro-inflammatory cytokines, reducing the effectiveness of the immune response. Additionally, components of the cell wall, such as lipoarabinomannan, can alter macrophage activation and impair antigen presentation, further aiding in immune evasion. These interactions highlight the sophisticated strategies employed by M. tuberculosis to establish a long-term presence within the host. Another important feature of M. tuberculosis is its metabolic adaptability. The bacterium can utilize a wide range of carbon sources, including lipids and fatty acids, which are abundant within host cells. During infection, M. tuberculosis shifts its metabolism to exploit host-derived lipids, enabling it to survive in nutrient-limited environments such as granulomas. This metabolic flexibility is closely associated with the ability of the organism to enter a dormant state, characterized by reduced metabolic activity and increased resistance to stress. Dormant bacilli are less susceptible to conventional antibiotics, which primarily target actively growing cells, thereby contributing to the persistence of infection and the risk of reactivation. The genetic makeup of M. tuberculosis also plays a significant role in its pathogenicity. The genome of the bacterium is relatively large and encodes numerous genes involved in lipid metabolism, stress response, and virulence. Genetic variations among different strains can influence factors such as transmissibility, disease severity, and drug resistance. For example, mutations in genes encoding drug targets or activating enzymes can lead to resistance against first-line anti-tubercular drugs such as isoniazid and rifampicin. Understanding these genetic mechanisms is essential for the development of new diagnostic tools and therapeutic strategies. Environmental resilience is another characteristic that contributes to the epidemiological success of M. tuberculosis. Although the organism is sensitive to ultraviolet light and heat, it can survive for extended periods in dark and moist environments. This ability enhances its potential for transmission in crowded indoor settings where ventilation is poor. However, unlike many other pathogens, M. tuberculosis does not multiply outside the host, and its survival in the environment primarily serves as a means of maintaining infectivity rather than replication. Furthermore, the interaction between M. tuberculosis and the host immune system is dynamic and complex. The initial immune response involves innate mechanisms, including the activation of macrophages and dendritic cells. This is followed by the development of adaptive immunity, particularly the activation of T-helper 1 (Th1) cells, which produce interferon-gamma to enhance macrophage killing. Despite these responses, M. tuberculosis often succeeds in establishing a balance between bacterial survival and host defense, resulting in the formation of granulomas. These structures, while protective in limiting bacterial spread, also provide a niche for bacterial persistence. In summary, the etiological and microbiological characteristics of to Mycobacterium tuberculosis are central to its success as a pathogen. Its unique cell wall structure, slow growth rate, metabolic adaptability, and sophisticated immune evasion strategies enable it persist within the host and cause chronic infection. These features not only complicate diagnosis and treatment but also contribute to the global burden of tuberculosis. A detailed understanding of these properties is essential for the development of more effective diagnostic tools, therapeutic agents, and preventive strategies aimed at controlling and ultimately eliminating this enduring disease [25].
4. PATHOGENESIS AND HOST IMMUNE RESPONSE:
The pathogenesis of tuberculosis begins with inhalation of infectious droplet nuclei containing M. tuberculosis. Upon reaching the alveoli, the bacteria are engulfed by macrophages. In many cases, the host immune system mounts a cell-mediated response involving T lymphocytes and cytokines such as interferon-gamma and tumor necrosis factor-alpha. This immune response leads to the formation of granulomas, which serve to contain the infection. However, in individuals with weakened immunity, the bacteria proliferate, resulting in active disease characterized by tissue destruction and cavitation. Latent tuberculosis infection represents a state in which the bacteria remain dormant within granulomas, with the potential for reactivation under conditions of immune suppression. Recent studies highlight the heterogeneity of host responses, emphasizing that factors such as age, co-morbidities, and genetic predisposition influence disease progression and treatment outcomes. The pathogenesis of tuberculosis is a complex, multistep process that involves intricate interactions between Mycobacterium tuberculosis and the host immune system. Infection begins when aerosolized droplet nuclei containing viable bacilli are inhaled and deposited in the alveolar spaces of the lungs. At this initial stage, alveolar macrophages serve as the first line of defense by recognizing and engulfing the bacteria through phagocytosis. However, instead of being eliminated, M. tuberculosis has evolved mechanisms to survive within these cells by inhibiting phagosome-lysosome fusion and resisting intracellular killing. This allows the pathogen to replicate within macrophages and establish an early infection focus. The host immune response plays a critical role in determining the outcome of infection. Within a few weeks, antigen-presenting cells such as macrophages and dendritic cells migrate to regional lymph nodes, where they activate T lymphocytes, particularly CD4+ T-helper cells. These activated T cells release cytokines, including interferon-gamma (IFN-γ) and tumor necrosis factor-alpha (TNF-α), which enhance the antimicrobial activity of macrophages. This cell-mediated immune response is essential for controlling bacterial replication and limiting the spread of infection. Additionally, CD8+ T cells contribute by directly killing infected cells and releasing cytotoxic molecules. One of the hallmark features of tuberculosis pathogenesis is the formation of granulomas, which are organized aggregates of immune cells that serve to contain the infection. Granulomas typically consist of a central core of infected macrophages, including specialized forms such as epithelioid cells and multinucleated giant cells, surrounded by a layer of lymphocytes and a fibrotic capsule. While granuloma formation is a protective mechanism that restricts bacterial dissemination, it also provides a niche in which M. tuberculosis can persist in a dormant state. Within this environment, the bacteria can enter a non-replicating phase characterized by reduced metabolic activity, allowing them to evade immune clearance and resist antibiotic treatment. The progression from latent infection to active disease is influenced by the balance between bacterial virulence and host immunity. In individuals with a robust immune response, the infection is effectively contained, resulting in latent tuberculosis infection, which is asymptomatic and non-transmissible. However, when the immune system is compromised, the integrity of granulomas may be disrupted, leading to bacterial reactivation and active disease. This is often associated with caseous necrosis, tissue destruction, and the formation of cavities within the lungs, which facilitate the release of bacilli into the airways and enhance transmission. Host-related factors play a significant role in modulating the immune response to M. tuberculosis. Conditions such as HIV infection, diabetes mellitus, malnutrition, and aging can impair immune function and increase susceptibility to active disease. Genetic variations in immune response genes have also been implicated in influencing individual susceptibility and disease severity. Furthermore, environmental factors, including exposure intensity and duration, contribute to variations in disease outcomes. Recent research has highlighted the heterogeneity of host immune responses, suggesting that differences in cytokine profiles, immune cell activation, and inflammatory pathways can significantly impact disease progression and treatment outcomes. the pathogenesis of tuberculosis is governed by a dynamic interplay between the pathogen and the host immune system. While the immune response is essential for controlling infection, it also contributes to tissue damage and disease pathology. Understanding these mechanisms is crucial for the development of improved therapeutic strategies, including host-directed therapies aimed at enhancing protective immunity while minimizing immunopathology [26].
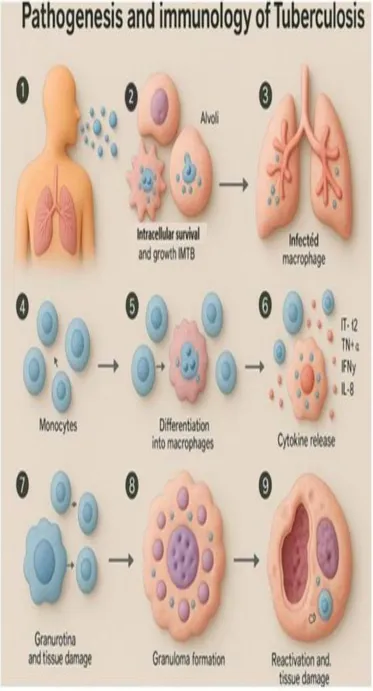
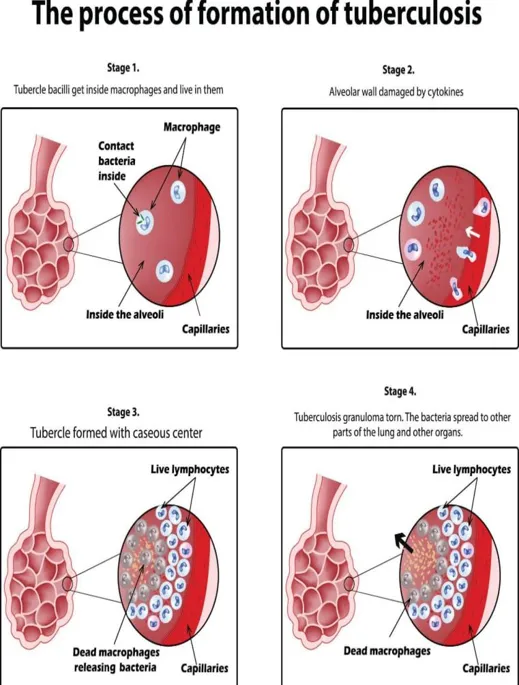
Figure 2: Pathogenesis of Tuberculosis
5. Clinical Manifestations:
Tuberculosis presents with a wide spectrum of clinical manifestations depending on the site of infection and immune status of the host. Pulmonary TB is the most common form and typically presents with chronic cough, sputum production, hemoptysis, fever, night sweats, and weight loss. Extrapulmonary TB can affect various organs, including lymph nodes, pleura, bones, and the central nervous system. These forms often present with non-specific symptoms, making diagnosis more challenging. The diversity in clinical presentation contributes to delays in diagnosis and increases the risk of disease transmission [27].
Table:1 Clinical Manifestations of Tuberculosis: [28,29].
|
Type of Tuberculosis |
Site of Involvement |
Common Clinical Features |
Pathophysiological Basis |
Diagnostic Challenges / Remarks |
|
Pulmonary TB |
Lungs (alveoli, bronchi) |
Persistent cough (>2–3 weeks), sputum production, hemoptysis, chest pain, breathlessness, fever, night sweats, weight loss |
Infection of lung parenchyma leads to inflammation, caseation, and cavitation, resulting in airway irritation and systemic symptoms |
Most infectious form; symptoms may mimic pneumonia or chronic bronchitis, leading to delayed diagnosis |
|
Lymph Node TB (Tuberculous lymphadenitis) |
Cervical and other lymph nodes |
Painless swelling of lymph nodes, gradual enlargement, possible suppuration or sinus formation, mild fever |
Local immune response leads to granuloma formation and caseous necrosis in lymph nodes |
Often misdiagnosed as reactive lymphadenopathy or malignancy; requires biopsy for confirmation |
|
Pleural TB |
Pleural space (lining of lungs) |
Chest pain, dry cough, dyspnea, pleural effusion, fever |
Hypersensitivity reaction to mycobacterial antigens causing fluid accumulation in pleural cavity |
Diagnosis may require pleural fluid analysis; low bacterial load makes detection difficult |
|
Skeletal TB (Bone and Joint TB) |
Spine (Pott’s disease), hips, knees |
Back pain, joint swelling, stiffness, restricted movement, deformities in advanced cases |
Hematogenous spread leads to destruction of bone tissue and intervertebral discs |
Often confused with arthritis or malignancy; slow progression delays diagnosis |
|
Central Nervous System TB (TB meningitis) |
Brain and meninges |
Headache, neck stiffness, vomiting, altered consciousness, seizures, neurological deficits |
Infection spreads to meninges causing inflammation, increased intracranial pressure, and neurological damage |
Medical emergency; early diagnosis is difficult due to non-specific early symptoms |
|
Genitourinary TB |
Kidneys, bladder, reproductive organs |
Dysuria, hematuria, flank pain, infertility in severe cases |
Hematogenous dissemination leads to granuloma formation in urinary and reproductive organs |
Frequently misdiagnosed as urinary tract infection; requires specialized tests |
|
Miliary TB |
Multiple organs (systemic spread) |
High fever, severe weakness, weight loss, respiratory distress, hepatosplenomegaly |
Dissemination through bloodstream leads to widespread tiny granulomas resembling millet seeds |
Difficult to diagnose; often seen in immunocompromised individuals |
|
Abdominal TB |
Intestines, peritoneum |
Abdominal pain, distension, diarrhea or constipation, weight loss, fever |
Infection leads to inflammation of intestinal wall or peritoneum, causing fluid accumulation and obstruction |
Mimics gastrointestinal disorders like Crohn’s disease or malignancy |
6. DIAGNOSTIC ADVANCES:
Accurate diagnosis of tuberculosis is critical for effective disease management. Traditional diagnostic methods such as sputum smear microscopy and culture remain widely used, although they have limitations in sensitivity and turnaround time [30]. Recent advancements in molecular diagnostics, including nucleic acid amplification tests, have significantly improved the speed and accuracy of TB detection. These methods can also identify drug resistance mutations, enabling early initiation of appropriate therapy. Emerging technologies such as artificial intelligence-based screening using cough sound analysis and imaging techniques have shown promising results in improving early detection, particularly in resource-limited settings [31]. Despite significant progress in global health initiatives, diagnostic delays continue to contribute to ongoing transmission and poor clinical outcomes. Traditionally, methods such as sputum smear microscopy and culture-based techniques have served as the foundation of tuberculosis diagnosis. While smear microscopy is rapid and inexpensive, its sensitivity is limited, particularly in cases with low bacterial load, such as pediatric and extrapulmonary tuberculosis. Culture methods, although considered the gold standard due to their high sensitivity and ability to detect viable organisms, are time-consuming and may require several weeks to yield results, thereby delaying treatment initiation. In recent years, the diagnostic landscape of tuberculosis has undergone a transformative shift with the introduction of molecular technologies. Nucleic acid amplification tests (NAATs), including cartridge-based systems, have revolutionized the detection of Mycobacterium tuberculosis by enabling rapid identification of bacterial DNA directly from clinical samples. These techniques not only provide results within a few hours but also offer improved sensitivity compared to conventional methods. Importantly, many molecular platforms are capable of simultaneously detecting genetic mutations associated with drug resistance, particularly resistance to rifampicin, which serves as a key marker for multidrug-resistant tuberculosis. This advancement allows clinicians to initiate targeted therapy at an earlier stage, significantly improving patient outcomes and reducing transmission. Beyond molecular diagnostics, immunological assays have also contributed to improved detection of tuberculosis infection. Interferon-gamma release assays (IGRAs) and tuberculin skin tests are commonly used to identify latent tuberculosis infection. While these tests are valuable for screening purposes, they do not differentiate between active and latent disease, highlighting the need for complementary diagnostic approaches. Emerging diagnostic innovations are further enhancing the ability to detect tuberculosis in diverse clinical settings. Advances in imaging technologies, including digital chest radiography and computed tomography, have improved the visualization of disease patterns, particularly in cases where microbiological confirmation is challenging. The integration of artificial intelligence (AI) into radiological analysis has demonstrated significant potential in automating the detection of characteristic TB lesions, thereby reducing diagnostic variability and supporting healthcare providers in resource-constrained environments. In addition to imaging, novel AI-driven tools are being developed to analyze cough sounds for early detection of tuberculosis. These non-invasive approaches leverage machine learning algorithms to identify acoustic patterns associated with the disease, offering a rapid and accessible screening method. Such innovations are particularly valuable in remote or underserved regions where access to advanced laboratory infrastructure is limited. Furthermore, biomarker-based diagnostics are gaining attention as potential tools for early and accurate detection. Research into host-derived biomarkers, including specific proteins, metabolites, and gene expression signatures, aims to distinguish between active and latent infection as well as predict disease progression. Although many of these approaches are still under investigation, they hold promise for the development of point-of-care diagnostic tests that are both rapid and highly accurate. In conclusion, the evolution of tuberculosis diagnostics reflects a shift toward rapid, sensitive, and decentralized testing strategies. The integration of molecular tools, artificial intelligence, and biomarker research represents a significant advancement in the fight against tuberculosis. However, ensuring equitable access to these technologies remains a critical challenge. Strengthening diagnostic capacity, particularly in high-burden regions, will be essential for achieving global tuberculosis control and elimination goals [32].
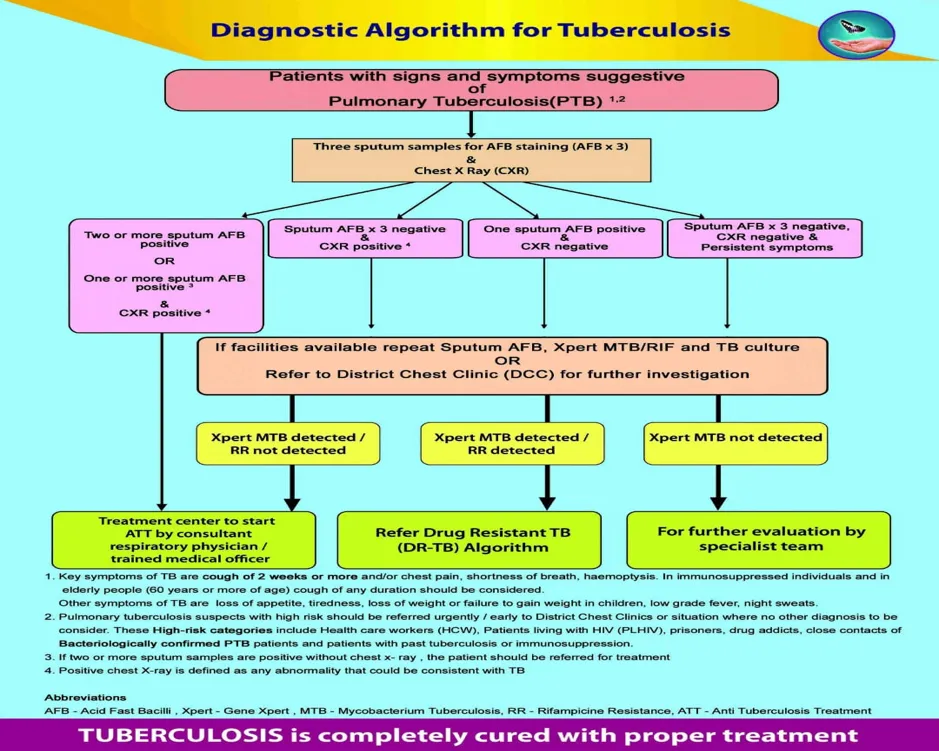
Figure 3: Diagnostic Algorithm for Tuberculosis
7. TREATMENT AND PHARMACOLOGICAL MANAGEMENT:
The treatment of tuberculosis involves prolonged multidrug therapy to ensure complete eradication of the pathogen and prevent resistance. Standard first-line therapy includes isoniazid, rifampicin, pyrazinamide, and ethambutol administered over a six-month period. Adherence to treatment is essential, as incomplete or irregular therapy can lead to relapse and the development of drug-resistant strains. Public health strategies such as directly observed treatment have been implemented to improve adherence and treatment outcomes. The management of tuberculosis is based on a comprehensive therapeutic approach that combines prolonged multidrug chemotherapy with supportive public health interventions. The primary objective of treatment is to achieve complete eradication of Mycobacterium tuberculosis, prevent disease relapse, interrupt transmission, and minimize the emergence of drug resistance. Due to the slow-growing nature of the pathogen and its ability to persist in a dormant state within host tissues, extended treatment regimens are required to ensure effective bacterial clearance. Standard treatment for drug-susceptible tuberculosis involves a combination of first-line antitubercular drugs administered over a period of at least six months. This regimen is divided into two phases: an intensive phase and a continuation phase. The intensive phase typically lasts for two months and includes four drugs—isoniazid, rifampicin, pyrazinamide, and ethambutol. This phase is aimed at rapidly reducing the bacterial load and controlling active disease. The continuation phase, which follows for an additional four months, generally includes isoniazid and rifampicin to eliminate residual bacilli and prevent relapse [33]. Each of these first-line drugs possesses a distinct mechanism of action that contributes to the overall effectiveness of the regimen. Isoniazid inhibits the synthesis of mycolic acids, which are essential components of the mycobacterial cell wall. Rifampicin acts by inhibiting bacterial RNA polymerase, thereby suppressing transcription. Pyrazinamide is particularly effective in acidic environments, targeting semi-dormant bacilli within macrophages. Ethambutol interferes with cell wall synthesis by inhibiting arabinosyl transferase enzymes. The use of combination therapy is critical, as it reduces the likelihood of the bacteria developing resistance to any single agent. Adherence to the prescribed treatment regimen is a crucial determinant of therapeutic success. Incomplete or irregular therapy can lead to treatment failure, relapse, and the emergence of drug-resistant forms of tuberculosis, such as multidrug-resistant (MDR) and extensively drug-resistant (XDR) TB. To address these challenges, public health strategies such as directly observed treatment (DOT) have been widely implemented. Under this approach, healthcare providers or trained personnel supervise patients during drug administration to ensure compliance and monitor for adverse effects. The management of drug-resistant tuberculosis is more complex and requires the use of second-line drugs, which are often less effective, more toxic, and more expensive. These regimens may include fluoroquinolones, injectable agents, and newer drugs such as bedaquiline and delamanid. Treatment duration for drug-resistant TB is significantly longer, often extending to 9–24 months depending on the resistance pattern and patient response. The introduction of shorter, all-oral regimens has shown promise in improving patient adherence and outcomes. Adverse drug reactions are an important consideration in tuberculosis therapy and may affect treatment adherence. Common side effects include hepatotoxicity, peripheral neuropathy, gastrointestinal disturbances, and visual impairment. Regular monitoring and early detection of adverse effects are essential to ensure patient safety and continuity of therapy. Additionally, special populations such as children, pregnant women, and individuals with co-morbid conditions require tailored treatment approaches to optimize efficacy and minimize risks. Recent advances in tuberculosis pharmacotherapy have focused on the development of shorter, more effective regimens and the incorporation of novel agents. Research into host-directed therapies aims to enhance the immune response and improve treatment outcomes. Furthermore, fixed-dose combination formulations have been introduced to simplify treatment regimens and reduce pill burden, thereby improving patient adherence. In conclusion, the pharmacological management of tuberculosis requires a multifaceted approach that integrates effective drug therapy, patient adherence strategies, and ongoing monitoring. Continued innovation in drug development and treatment strategies is essential to address the challenges posed by drug resistance and to achieve global tuberculosis control [34].
Table: Antitubercular Drugs and Their Characteristics [35].
|
Drug Class |
Drug Name |
Mechanism of Action |
Role in Therapy |
Major Adverse Effects |
Key Remarks |
|
First-line drugs |
Isoniazid |
Inhibits mycolic acid synthesis (cell wall) |
Core drug in all regimens |
Hepatotoxicity, peripheral neuropathy |
Highly bactericidal; requires pyridoxine supplementation |
|
|
Rifampicin |
Inhibits DNA-dependent RNA polymerase |
Backbone of short-course therapy |
Hepatotoxicity, drug interactions, orange discoloration |
Strong enzyme inducer affecting other drugs |
|
|
Pyrazinamide |
Disrupts membrane metabolism in acidic pH |
Active in intensive phase |
Hepatotoxicity, hyperuricemia |
Effective against dormant bacilli |
|
|
Ethambutol |
Inhibits arabinosyl transferase (cell wall) |
Prevents resistance development |
Optic neuritis, vision changes |
Requires vision monitoring |
|
Second-line drugs |
Fluoroquinolones (e.g., levofloxacin) |
Inhibits DNA gyrase |
Used in MDR-TB |
GI upset, tendon damage |
Key component of resistant TB regimens |
|
|
Injectable agents (e.g., amikacin) |
Inhibits protein synthesis |
Severe resistant cases |
Nephrotoxicity, ototoxicity |
Use limited due to toxicity |
|
Newer drugs |
Bedaquiline |
Inhibits ATP synthase |
MDR/XDR-TB treatment |
QT prolongation |
Oral drug; improves outcomes |
|
|
Delamanid |
Inhibits mycolic acid synthesis |
Resistant TB |
QT prolongation |
Used in combination regimens |
8. DRUG-RESISTANT TUBERCULOSIS:
Drug resistance represents one of the most significant challenges in TB control. Multidrug-resistant TB is defined by resistance to isoniazid and rifampicin, while extensively drug-resistant TB includes resistance to additional second-line drugs. Recent regional data indicate increasing trends in drug resistance, with significant proportions of cases showing resistance to at least one anti-TB drug. The emergence of resistance is primarily driven by inadequate treatment, poor adherence, and improper drug use. Molecular mechanisms of resistance involve genetic mutations in drug target genes, which reduce drug efficacy and complicate treatment. Drug-resistant Tuberculosis has emerged as one of the most formidable obstacles to global tuberculosis control, threatening decades of progress in disease management. Resistance to anti-tubercular drugs compromises treatment efficacy, prolongs infectiousness, increases healthcare costs, and contributes significantly to morbidity and mortality. The growing burden of resistant tuberculosis highlights the urgent need for improved diagnostic strategies, effective treatment regimens, and robust public health interventions. Multidrug-resistant tuberculosis (MDR-TB) is defined as resistance to at least isoniazid and rifampicin, the two most potent first-line drugs. Extensively drug-resistant tuberculosis (XDR-TB) represents a more severe form, characterized by additional resistance to key second-line agents, including fluoroquinolones and certain injectable drugs. More recently, the concept of pre-XDR TB has been introduced to describe strains with resistance to rifampicin and any fluoroquinolone, reflecting the evolving complexity of resistance patterns. These classifications underscore the progressive nature of drug resistance and its implications for treatment outcomes. The emergence and spread of drug-resistant tuberculosis are driven by multiple interrelated factors. Inadequate or incomplete treatment remains the most significant contributor, often resulting from poor patient adherence, suboptimal drug regimens, or interruptions in drug supply. Misuse of antibiotics, including incorrect dosing and inappropriate prescription practices, further accelerates the development of resistance. Additionally, healthcare system limitations, such as insufficient diagnostic capacity and delayed detection of resistance, contribute to ongoing transmission of resistant strains within communities. At the molecular level, drug resistance in Mycobacterium tuberculosis primarily arises through spontaneous genetic mutations in specific genes encoding drug targets or drug-activating enzymes. For instance, resistance to rifampicin is commonly associated with mutations in the rpoB gene, which encodes the beta subunit of RNA polymerase. Similarly, mutations in the katG gene or the inhA promoter region are linked to isoniazid resistance, affecting the activation or target binding of the drug [36,37]. Fluoroquinolone resistance is typically mediated by mutations in the gyrA and gyrB genes, while resistance to injectable agents may involve alterations in ribosomal components or associated pathways. These genetic changes reduce drug binding or activation, thereby diminishing therapeutic efficacy. The clinical implications of drug-resistant tuberculosis are profound. Patients with resistant forms of the disease often require prolonged treatment with second-line or newer drugs, which are generally less effective, more toxic, and more expensive than first-line therapies. Treatment duration may extend from several months to over a year, placing a significant burden on both patients and healthcare systems. Furthermore, adverse drug reactions are more frequent and severe in resistant TB regimens, leading to challenges in maintaining adherence and achieving successful outcomes. Recent advances in molecular diagnostics have improved the detection of drug resistance, enabling rapid identification of resistance-associated mutations. Techniques such as line probe assays and next-generation sequencing allow for early diagnosis and tailored treatment strategies. These tools are particularly valuable in high-burden settings, where timely detection of resistance can prevent the spread of resistant strains and improve patient prognosis. From a public health perspective, controlling drug-resistant tuberculosis requires a multifaceted approach. Strengthening treatment adherence through patient-centered care models, ensuring uninterrupted drug supply, and implementing effective infection control measures are critical components. Surveillance systems must be enhanced to monitor resistance trends and guide policy decisions. Additionally, ongoing research into novel therapeutics and shorter treatment regimens offers hope for more effective management of resistant TB in the future. In conclusion, drug-resistant tuberculosis represents a complex and evolving challenge that demands coordinated efforts at both clinical and public health levels. Addressing the underlying causes of resistance, improving diagnostic capabilities, and advancing treatment options are essential for reducing the global burden of this disease. Without sustained and comprehensive interventions, drug-resistant tuberculosis will continue to undermine global efforts toward tuberculosis elimination [38].
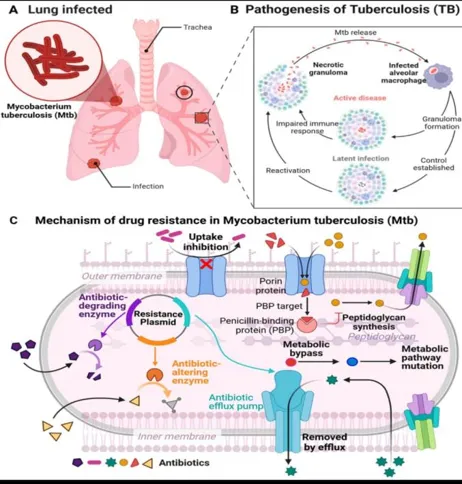
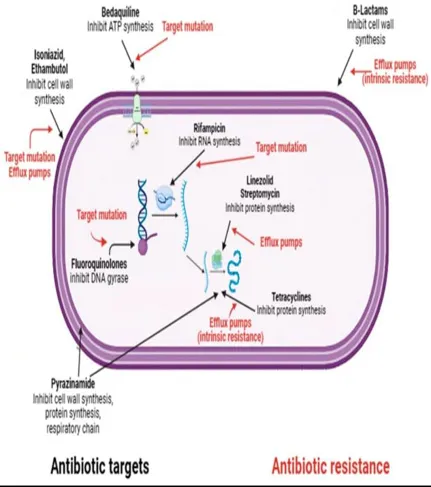
Figure 4: Mechanisms of Drug Resistance
Table 2: Type of Drug Resistance Tuberculosis:
|
Type of Resistance |
Definition |
Key Drugs Affected |
Molecular Basis |
Clinical Impact |
|
Mono-resistant TB |
Resistance to one first-line drug |
Isoniazid or Rifampicin |
Single gene mutation (e.g., katG) |
Requires modified regimen |
|
MDR-TB |
Resistance to at least isoniazid & rifampicin |
First-line core drugs |
katG, rpoB mutations |
Longer, complex treatment |
|
Pre-XDR TB |
MDR + resistance to fluoroquinolones |
Levofloxacin, moxifloxacin |
gyrA, gyrB mutations |
Limited treatment options |
|
XDR-TB |
MDR + fluoroquinolone + second-line drug resistance |
Injectable agents + FQs |
Multiple gene mutations |
Very high mortality risk |
9. PREVENTION AND CONTROL STRATEGIES:
Effective TB control requires a combination of medical and public health interventions. Vaccination with Bacillus Calmette–Guérin provides partial protection, particularly in children. Early detection and prompt treatment are critical in reducing transmission. Public health initiatives focusing on awareness, screening, and improved living conditions play a vital role in disease control. The WHO End TB Strategy emphasizes the need for integrated approaches combining healthcare delivery, research, and social interventions. The prevention and control of tuberculosis require a coordinated and multifaceted approach that integrates clinical management with robust public health interventions. Given the airborne nature of transmission and the complex interplay of biological and social determinants, effective control strategies must address both the source of infection and the conditions that facilitate disease spread. Over the years, global efforts have evolved from isolated treatment-focused approaches to comprehensive frameworks that emphasize prevention, early detection, and sustained community engagement. Vaccination remains one of the earliest and most widely implemented preventive measures against tuberculosis. The Bacillus Calmette–Guérin (BCG) vaccine has been extensively used for decades, particularly in countries with a high burden of disease. While BCG provides variable protection against pulmonary tuberculosis in adults, it is highly effective in preventing severe forms of the disease in children, such as miliary tuberculosis and tuberculous meningitis. Despite its limitations, BCG continues to play a crucial role in national immunization programs. Ongoing research is focused on developing more effective vaccines that can provide long-lasting immunity across all age groups, with several candidates currently in different stages of clinical trials. Early detection and prompt initiation of appropriate treatment are central to interrupting the chain of transmission. Active case finding, particularly among high-risk populations, has emerged as an important strategy to identify undiagnosed cases. Screening programs in vulnerable groups—such as individuals with HIV infection, close contacts of TB patients, and those living in overcrowded settings—facilitate early diagnosis and reduce the likelihood of disease progression and spread. The integration of advanced diagnostic tools, including molecular testing and digital radiography, has further enhanced the efficiency of screening and case detection. Treatment of active cases not only benefits the individual patient but also serves as a critical public health intervention by reducing infectiousness. Ensuring treatment adherence through patient-centered approaches is essential for achieving successful outcomes and preventing the development of drug resistance. Strategies such as directly observed therapy, digital adherence technologies, and community-based support systems have been implemented to improve compliance. In addition, preventive therapy for individuals with latent tuberculosis infection, particularly those at high risk of progression to active disease, represents an important component of control efforts. Public health initiatives play a pivotal role in addressing the broader determinants of tuberculosis transmission. Awareness campaigns aimed at educating communities about the symptoms, modes of transmission, and availability of treatment can reduce stigma and encourage early healthcare seeking behavior. Improving living conditions, including reducing overcrowding and enhancing ventilation in homes and workplaces, significantly decreases the risk of airborne transmission. Nutritional support programs are also important, as malnutrition weakens immune function and increases susceptibility to infection. The global response to tuberculosis is guided by comprehensive frameworks such as the End TB Strategy proposed by the World Health Organization. This strategy outlines ambitious targets for reducing TB incidence and mortality through a combination of integrated healthcare services, strengthened health systems, and intensified research and innovation. Key pillars of the strategy include patient-centered care, bold policies addressing social determinants, and the promotion of new tools such as vaccines, diagnostics, and therapeutics. Collaboration between governments, healthcare providers, researchers, and communities is essential to achieve these goals. In addition to traditional approaches, innovative technologies are increasingly being incorporated into tuberculosis control programs. Digital health platforms enable real-time monitoring of treatment adherence and facilitate communication between patients and healthcare providers. Artificial intelligence-based tools are being used to enhance screening and diagnostic accuracy, particularly in resource-limited settings. These advancements offer new opportunities to improve the efficiency and reach of TB control efforts. In conclusion, the prevention and control of tuberculosis require sustained commitment and a holistic approach that combines medical, social, and technological interventions. While significant progress has been made, challenges such as drug resistance, healthcare disparities, and socioeconomic inequalities continue to hinder global efforts. Strengthening prevention strategies, expanding access to care, and fostering innovation will be critical to achieving long-term control and eventual elimination of tuberculosis [39].
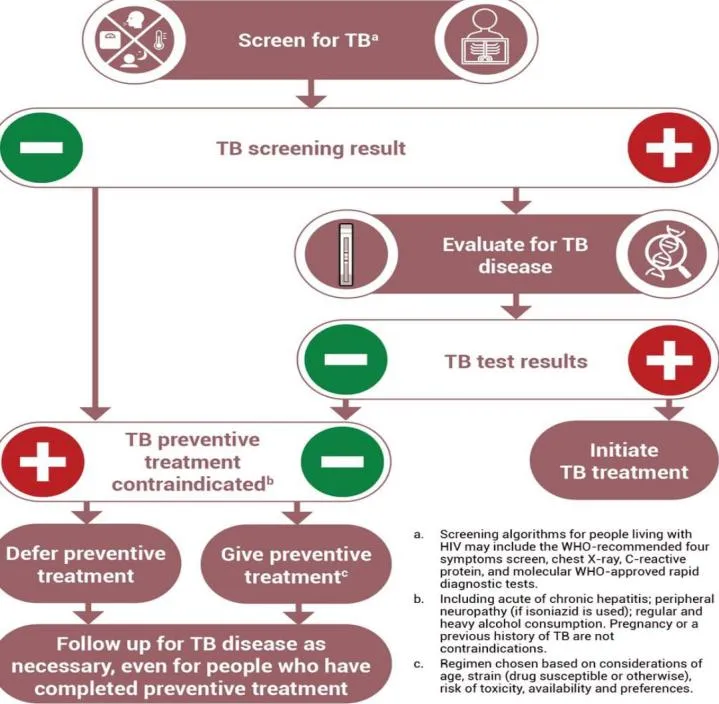
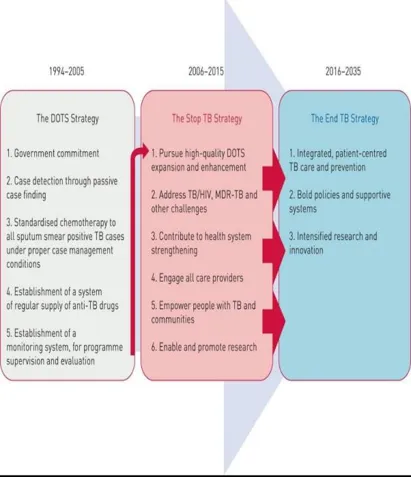
Figure 5: Prevention and Control Strategy Framework
10. RECENT ADVANCES AND FUTURE PERSPECTIVES:
Recent advances in tuberculosis research include the development of new drugs, improved diagnostic tools, and innovative treatment strategies. Novel agents such as bedaquiline and delamanid have shown effectiveness against drug-resistant TB. Additionally, host-directed therapies aimed at modulating the immune response are being explored as potential adjunct treatments. Advances in artificial intelligence and machine learning are also contributing to improved diagnostic accuracy and personalized treatment approaches. Despite these advancements, significant challenges remain, including funding limitations, healthcare disparities, and the need for more effective vaccines. Over the past decade, substantial progress has been made in tuberculosis research, driven by the urgent need to address persistent challenges such as drug resistance, diagnostic delays, and treatment complexity. These advances span multiple domains, including pharmacotherapy, diagnostics, immunology, and digital health technologies, collectively contributing to a more comprehensive and effective approach to tuberculosis control [40]. One of the most significant breakthroughs in recent years has been the development of novel antitubercular agents with activity against drug-resistant strains. Drugs such as bedaquiline and delamanid have introduced new mechanisms of action, targeting mycobacterial energy metabolism and cell wall synthesis, respectively. These agents have demonstrated improved outcomes in patients with multidrug-resistant and extensively drug-resistant tuberculosis when incorporated into combination regimens. The shift toward shorter, all-oral treatment regimens represents another important advancement, reducing treatment duration and minimizing the burden associated with injectable drugs. Ongoing research continues to explore additional compounds with enhanced efficacy and reduced toxicity, aiming to further optimize treatment strategies. In parallel, diagnostic innovations have transformed the detection and management of tuberculosis. Molecular technologies have significantly reduced the time required for diagnosis and enabled the identification of drug resistance at an early stage. The integration of next-generation sequencing has provided deeper insights into the genetic basis of resistance and transmission dynamics, facilitating more precise and individualized treatment approaches. Furthermore, advances in point-of-care diagnostics are improving access to rapid testing in resource-limited settings, thereby enhancing early case detection and reducing transmission. A promising area of research is the development of host-directed therapies (HDTs), which aim to enhance the host immune response rather than directly targeting the pathogen. These therapies focus on modulating inflammatory pathways, improving macrophage function, and reducing tissue damage associated with excessive immune activation. By complementing conventional antimicrobial treatment, host-directed approaches have the potential to shorten treatment duration, improve outcomes, and reduce the risk of relapse. Although still largely in the experimental stage, HDTs represent a paradigm shift in tuberculosis management. The application of artificial intelligence (AI) and machine learning has emerged as a transformative force in tuberculosis research and healthcare delivery. AI-based tools are increasingly being used to analyze radiological images, detect disease patterns, and support clinical decision-making. Automated interpretation of chest X-rays has demonstrated high accuracy in identifying tuberculosis-related abnormalities, particularly in settings where trained radiologists are scarce. Additionally, machine learning algorithms are being developed to predict treatment outcomes, assess disease severity, and personalize therapeutic regimens based on patient-specific data. These technologies have the potential to enhance efficiency, reduce diagnostic errors, and improve overall patient care. Despite these encouraging developments, several challenges continue to hinder progress toward tuberculosis elimination. Limited funding remains a major barrier, particularly in low- and middle-income countries where the burden of disease is highest. Healthcare disparities, including unequal access to diagnostic tools and treatment services, further exacerbate the problem. The need for more effective vaccines is another critical priority, as the currently available BCG vaccine offers limited protection against adult pulmonary tuberculosis. Continued investment in research, infrastructure, and global collaboration is essential to overcome these challenges. Looking ahead, the future of tuberculosis control will likely depend on the integration of multidisciplinary approaches that combine biomedical innovation with social and policy interventions. Strengthening health systems, expanding access to care, and addressing the underlying determinants of disease will be crucial for achieving sustainable progress. The development of next-generation vaccines, improved drug regimens, and advanced diagnostic tools offers hope for a future where tuberculosis is no longer a major public health threat [41].
11. CONCLUSION:
Tuberculosis remains a complex and persistent global health issue requiring coordinated efforts at multiple levels. While significant progress has been made in diagnosis and treatment, the emergence of drug resistance and ongoing transmission highlight the need for continued research and innovation. A multidisciplinary approach integrating medical, technological, and public health strategies is essential to achieve the global goal of TB elimination. Tuberculosis continues to represent a major global health challenge, characterized by its complex pathogenesis, diverse clinical manifestations, and significant socioeconomic impact. Despite decades of sustained efforts in control and prevention, the disease persists across many regions of the world, particularly in low- and middle-income countries. The enduring burden of tuberculosis reflects not only the biological resilience of Mycobacterium tuberculosis but also the influence of broader determinants such as poverty, malnutrition, overcrowding, and limited access to healthcare services. Substantial progress has been achieved in recent years, particularly in the areas of diagnostics and pharmacological management. The introduction of rapid molecular diagnostic tools has significantly improved early detection and enabled timely identification of drug resistance. Similarly, advancements in treatment strategies, including the development of new drugs and shorter regimens, have enhanced therapeutic outcomes and patient adherence. However, the growing prevalence of drug-resistant tuberculosis remains a critical concern, complicating treatment and threatening to reverse gains made in disease control. The persistence of tuberculosis transmission underscores the importance of strengthening public health systems and implementing comprehensive prevention strategies. Early case detection, effective treatment, and sustained patient adherence are essential components of reducing disease spread. In addition, addressing latent tuberculosis infection through preventive therapy can play a key role in awareness, and reducing stigma are equally important in ensuring community engagement and timely healthcare seeking behavior. Looking forward, the successful control and eventual elimination of tuberculosis will depend on a multidisciplinary approach that integrates biomedical innovation with social and policy-driven interventions. Continued investment in research is essential for the development of more effective vaccines, novel therapeutics, and advanced diagnostic tools. Emerging technologies, including artificial intelligence and host-directed therapies, offer promising avenues for improving disease management and personalizing treatment approaches. Furthermore, global collaboration and political commitment are crucial for sustaining progress. Strengthening healthcare infrastructure, ensuring equitable access to diagnostic and treatment services, and enhancing surveillance systems will be key to addressing disparities and achieving long-term control. International frameworks and coordinated efforts must continue to prioritize tuberculosis as a major public health concern. In conclusion, while notable advancements have been made, tuberculosis remains far from eradicated. A sustained, integrated, and innovative approach that combines medical, technological, and public health strategies is essential to overcome existing challenges. With continued commitment and collaboration, the global goal of tuberculosis elimination can become an achievable reality in the future.
REFERENCES




Syed Rahamthulla, P Shaik Shiya Farnaz, Sufia Sultana, M P Narasimha, Shaik Roqhayya, A Comprehensive Review on Tuberculosis: Pathogenesis, Diagnosis, Drug Resistance, and Emerging Therapeutics, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4825-4848. https://doi.org/10.5281/zenodo.20752742
 10.5281/zenodo.20752742
10.5281/zenodo.20752742