
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shantiniketan college of pharmacy, Dhotre
Anxiety disorders represent a major global health burden, yet current pharmacological treatments like SSRIs and benzodiazepines have significant limitations, including delayed onset, side effects, and dependency risks. Kava (Piper methysticum), a traditional Pacific botanical, offers a promising alternative. This review synthesizes evidence on kava’s anxiolytic efficacy, safety, and regulatory status. Modern clinical trials demonstrate that standardized, aqueous extracts of noble kava cultivars are effective for mild-to-moderate anxiety with a favorable side-effect profile, primarily causing transient dermopathy or gastrointestinal discomfort. The central safety controversy rare, idiosyncratic hepatotoxicity is now understood as a multifactorial issue linked to poor-quality raw materials (e.g., non-noble varieties, aerial plant parts), specific extraction methods, and individual metabolic susceptibilities, rather than an inherent property of kava itself. Risk mitigation strategies, including the use of noble cultivars, water-based extraction, and adherence to recommended daily doses (?250 mg kavalactones), are outlined. Despite robust traditional use and evolving scientific understanding, global regulations remain fragmented, ranging from complete bans in parts of Europe to regulated supplement status in the United States and quality-controlled frameworks in the Pacific. This reappraisal concludes that, with stringent quality controls and appropriate patient selection, kava represents a viable, evidence-based phytotherapeutic option for anxiety management.
Globally, mental disorders constitute a major public health challenge, with depressive and anxiety disorders representing the primary drivers of this burden [1]. These conditions are leading causes of disability and are responsible for massive annual economic losses, estimated at $925 billion in lost productivity (WHO, 2014). Despite this immense impact, global investment in mental health remains critically insufficient and inequitably distributed, creating a vast treatment gap [2]. The burden of these highly comorbid disorders varies widely across regions, influenced by economic, social, and healthcare factors [3]. As global dynamics evolve including economic development and ongoing societal pressures there is an urgent need for long-term, integrated projections of the burden of depression and anxiety to inform strategic healthcare planning and resource allocation for the coming decade [4]. The current evaluation of antidepressant effectiveness is severely limited by methodological issues with early symptom improvement detection and definition. The variable and late beginning of effect of conventional medicines, including several types of standard antidepressants, is a problem. A significant clinical response usually takes several weeks to manifest. The lack of established definitions for "rapid onset" or "early improvement," since current response and remission criteria were created for longer-term evaluation, exacerbates this delayed treatment window [5,6]. As a result, the majority of the information pertaining to early effects comes from post-hoc analysis of trials that were not adequately powered for such evaluations, which results in inconsistent and untrustworthy estimates of quick efficacy. Additionally, it is possible that traditional depression rating measures and the frequency of their use are not adapted to catch clinically significant improvement that takes place in a matter of hours or days. Leaving a significant gap in the conceptual understanding and assessment of fast antidepressant activity[7] Clinical difficulties with traditional pharmacological treatments for depression and anxiety are substantial. First-line treatments known as selective serotonin reuptake inhibitors (SSRIs) have a delayed onset of therapeutic activity; it frequently takes weeks for them to show clinically significant results. Although benzodiazepines are commonly used for quick symptom alleviation, there is a significant risk of tolerance, dependency, and withdrawal symptoms. Both drug classes have a significant load of adverse effects, including as sedation, weight gain, and sexual dysfunction with SSRIs and cognitive impairment and sleepiness with benzodiazepines, which often result in poor adherence [8]. Additionally, despite sufficient trials of several therapeutic drugs, a sizable percentage of patients have treatment-resistant characteristics, failing to reach remission. Together, these drawbacks highlight the necessity of alternate pharmacological approaches with better efficacy and tolerability [9,10]. Kava, traditionally known as Piper methysticum ("intoxicating pepper"), originated as a ceremonial and social beverage deeply embedded in the cultures of the Pacific Islands for millennia. Used to facilitate community bonding, spiritual connection, and conflict resolution, its psychoactive yet non-alcoholic properties fostered a state of calm, focused sociability. In the late 20th century, Western interest transformed this ethnobotanical elixir into a commercial herbal medicine, promoted for its natural anxiolytic properties. This transition from a communal, ritually prepared drink to a standardized, clinically studied extract encapsulates the broader journey of traditional plant medicines into the global phytopharmaceutical market[11,12]
A reappraisal of kava (Piper methysticum) is strongly supported by three key advancements:
|
Aspects |
Key Details |
Key impacts |
References |
|
Major Active Constituents |
Kavalactones (KLs): A group of ~18 related α‑pyrone compounds. The six major KLs are: Kavain, Dihydrokavain, Methysticin, Dihydromethysticin, Yangonin, and Desmethoxyyangonin. |
nxiolytic, muscle‑relaxant, and analgesic effects are primarily attributed to KLs, which modulate GABAergic, glutamatergic, and monoaminergic systems. KL profile determines the chemotype. |
[16,17] |
|
Chemotypes & Cultivars |
Defined by the rank order of the 6 major KLs (e.g., "463251"). |
Noble: Preferred for traditional use; milder, predictable effects, lower risk of adverse effects. |
[18] |
|
Other Constituents |
Flavokavains A, B, C (chalcones) and trace Piperidine Alkaloids (e.g., pipermethystine).
|
Flavokavain B (FKB) is implicated in in vitro hepatotoxicity, found in higher concentrations in aerial parts and some Tudei cultivars. Alkaloids are present in leaves/stems and are toxic. Safety depends on minimizing these constituents.
|
[19,20] |
|
Importance of Plant Part
|
Lateral (Peeled) Roots: Traditionally used; contain high KLs, low FKB. |
Use of aerial parts or poor‑quality "wild" kava is a major risk factor for hepatotoxicity. Modern safety mandates use of peeled lateral roots/rhizomes only. |
[21] |
|
Extraction Methods
|
1. Traditional Aqueous: Cold water extraction of dried, macerated root. |
Aqueous extract: Yields KLs with minimal FKB; correlates with long history of safe use. |
[22] |
|
Standardization |
Typically standardized to total kavalactone content (e.g., 70% KLs). |
Standardization to KL % ensures potency but does not guarantee a safe chemotype or low FKB content. The cultivar (Noble) and plant part (root) remain the most important quality markers. |
[23,24] |
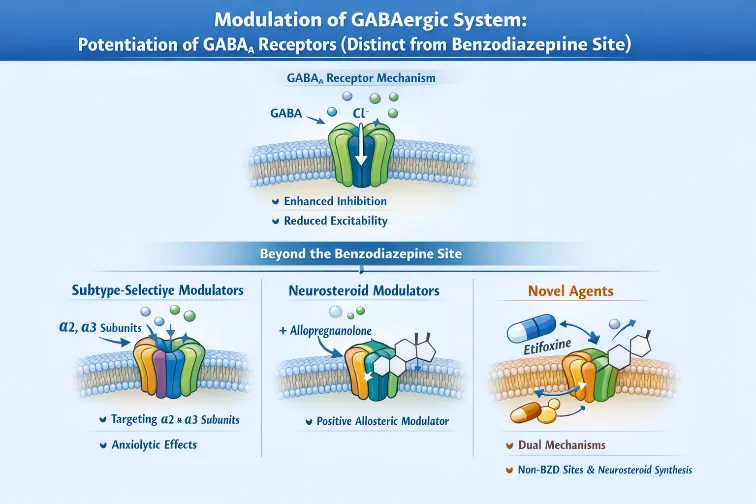
Anxiety disorders represent a major global health burden, and pharmacological treatments re Anxiety disorders represent a prevalent class of neuropsychiatric conditions characterized by excessive fear, heightened stress responses, and dysregulated emotional processing. Historically, the pharmacological treatment of anxiety has largely focused on enhancing inhibitory neurotransmission through γ-aminobutyric acid (GABA) receptors, particularly GABAA receptors targeted by benzodiazepines. However, contemporary research emphasizes a multi-target neuromodulation framework that extends beyond the classical GABA-centric view and incorporates glutamatergic modulation, especially involving N-methyl-D-aspartate (NMDA) receptors as part of anxiolytic mechanisms [25].
Classical View and Rationale
The inhibitory neurotransmitter GABA is the primary mediator of inhibitory tone in the central nervous system (CNS). GABAA receptors are ligand-gated chloride channels that, when activated, stabilize neuronal membranes through chloride influx and reduce excitatory firing. Enhancing this inhibition attenuates hyperexcitability underlying anxiety states[26].
Beyond the Benzodiazepine Site
Unlike classical benzodiazepines that potentiate GABAA receptor function by binding at the canonical benzodiazepine allosteric site, multiple novel anxiolytic compounds modulate GABAA function through distinct receptor subunits or alternative binding sites a mechanism associated with anxiolysis but reduced sedation and dependency risk [27].
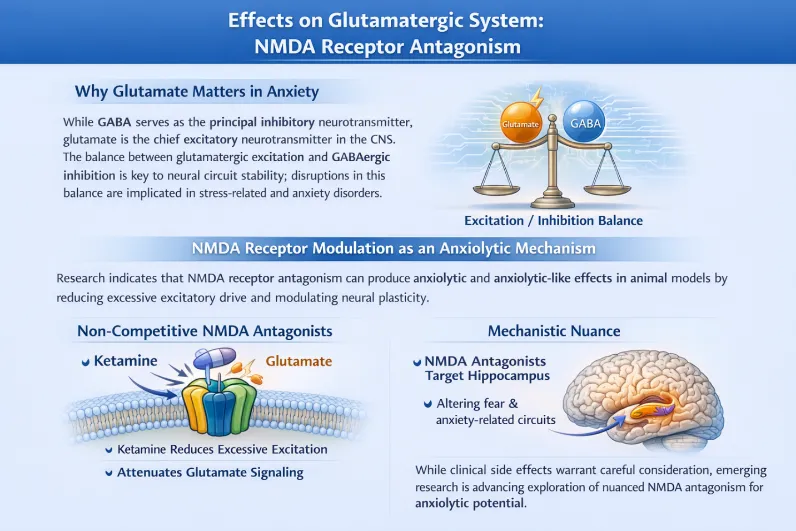
Why Glutamate Matters in Anxiety
While GABA serves as the principal inhibitory neurotransmitter, glutamate is the chief excitatory neurotransmitter in the CNS. The balance between glutamatergic excitation and GABAergic inhibition is key to neural circuit stability; disruptions in this balance are implicated in stress-related and anxiety disorders[30].
NMDA Receptor Modulation as an Anxiolytic Mechanism
Research indicates that NMDA receptor antagonism can produce anxiolytic and anxiolytic-like effects in animal models by reducing excessive excitatory drive and modulating neural plasticity.
Although NMDA antagonists carry side-effect considerations in clinical settings, emerging research motivates a deeper exploration of subunit-specific antagonism and nuanced modulation that might maximize anxiolytic benefits while minimizing adverse effects [32].
The current landscape of anxiolytic pharmacology reflects an evolution from mono-targeted GABA potentiation to multi-target strategies that integrate inhibitory enhancement with excitatory suppression and neural circuit modulation. This integrative approach acknowledges complexity in neural network dynamics underpinning anxiety and seeks pharmacological interventions that more comprehensively address excitatory–inhibitory imbalance.
Mechanistic Overview Monoamines in Anxiety:
The monoaminergic hypothesis posits that serotonin (5-HT), noradrenaline (NE), and dopamine (DA) regulate mood and emotional behavior by modulating synaptic transmission. Anxiolytic interventions often influence these neurotransmitters by inhibiting their reuptake transporters SERT, NET, and DAT or by preventing their enzymatic breakdown, thereby increasing synaptic availability and enhancing signaling within limbic and cortical circuits that regulate fear and stress responses.
Neuroinflammation in Anxiety:
Emerging evidence indicates that neuroinflammation contributes significantly to the pathophysiology of anxiety disorders. Chronic stress and inflammatory cytokines can alter neurotransmitter synthesis, release, and receptor expression, thereby influencing anxiety-related circuits.
• Monoamine–Inflammation Interplay: According to the review Monoamine Signaling and Neuroinflammation, monoaminergic systems interact with immune responses pro-inflammatory cytokines can modulate serotonin, norepinephrine, and dopamine metabolism, while monoamines themselves influence microglial activation and cytokine production, creating bidirectional control over neuroinflammatory states implicated in anxiety and other neuropsychiatric conditions[38].
• Anti-Inflammatory & Neuroprotective Actions: Agents with anti-inflammatory profiles including some natural flavonoids and phytochemicals show anxiolytic-like effects in preclinical models that are associated with suppressed pro-inflammatory cytokine release, reduced microglial activation, and increased neuronal viability.
Functional Implications:
Neuroprotective mechanisms may facilitate resilience to stress-induced structural and functional brain changes by preserving synaptic integrity, enhancing neurotrophic factors like BDNF, and attenuating oxidative damage processes now recognized as contributing to anxiety symptomatology alongside classical neurotransmitter imbalance [39].
Behavioral Models & Mechanistic Findings:
Preclinical studies using elevated plus maze, open-field tests, and stress paradigms demonstrate that pharmacological agents influencing monoamines, GABAergic function, or inflammatory pathways show anxiolytic-like behavioral effects in rodents [40].
Examples of preclinical findings include:
• Monoaminergic modulation:
Agents that increase extracellular serotonin and norepinephrine via reuptake inhibition or receptor modulation produce reduced anxiety-like behaviors in animal models, consistent with clinical anxiolytic effects seen in humans [41].
• Anti-Inflammatory effects:
Compounds with anti-inflammatory and antioxidant profiles (e.g., certain flavonoids) reduce anxious behaviors in rodents exposed to stress or inflammatory challenges, correlating with decreased neuroinflammation markers and improved neural health [42].
• Neuroprotective outcomes: In various rodent studies, agents that protect neurons from stress-induced damage also mitigate anxiety-like behavior, supporting the notion that neuroprotection is a component of anxiolytic mechanisms when inflammation and excitotoxicity are involved [43].
The body of clinical evidence evaluating kava (Piper methysticum) for anxiety has been synthesized in multiple systematic reviews and meta-analyses. A comprehensive meta-analysis of double-blind randomized controlled trials (RCTs) found that kava extract was associated with greater reductions in Hamilton Anxiety Rating Scale (HAM-A) scores compared with placebo across several studies, though the overall effect size was modest and based on relatively small samples (total n≈700).7 Trials included in this synthesis demonstrated mild, transient adverse effects similar to placebo, suggesting a generally favorable short-term safety profile[44]. Earlier meta-analyses (e.g., Pittler & Ernst, 2000) also reported that kava extract produced significant symptomatic anxiolytic effects vs placebo, with a weighted mean reduction in HAM-A scores in favor of kava, although methodological and sample size limitations reduced the strength of conclusions[45]. A more recent systematic review focused specifically on Generalized Anxiety Disorder (GAD) identified 12 clinical trials. While pooled estimates showed effect sizes favoring kava (standardized mean differences 0.59-0.99), results did not always reach statistical significance, and evidence was considered promising but insufficient to definitively confirm efficacy due to limited trial size and heterogeneity [46].
5.2. Key Randomized Controlled Trials (RCTs)
a. Trials Using Specific Kava Extracts (WS® 1490, LI 150)
WS® 1490 Extract Trials
LI 150 Extract Trial
These trials provide evidence that standardized extracts like WS® 1490 and LI 150 exhibit anxiolytic effects in placebo-controlled and active-controlled settings.
b. Efficacy in Generalized Anxiety Disorder (GAD)
RCTs specifically enrolling patients with GAD have shown mixed but promising outcomes. In the LI 150 trial, kava extract yielded anxiolytic effects comparable to buspirone and opipramol over 8 weeks in outpatients diagnosed with GAD. Systematic reviews focusing on GAD noted that while pooled effect sizes often favored kava, statistical significance was not always reached, and existing evidence remains insufficiently robust to establish definitive efficacy beyond placebo due to limited sample sizes and variability in trial design [49].
c. Efficacy in Non-Clinical, Situational, and Perimenopausal Anxiety
Direct RCT evidence in situational anxiety and perimenopausal anxiety is limited:
Kava extracts generally demonstrate anxiolytic effects that emerge gradually over several weeks, as seen in longer randomized trials where significant group differences often were noted after 8 weeks.
In comparison:
Despite a relative slower onset compared to benzodiazepines, kava is usually associated with a more favorable side-effect profile (e.g., less sedation, lower risk of dependence) in short-term use [51].
While existing clinical trials support short-term anxiolytic efficacy and good tolerability of standardized kava extracts, several key limitations constrain the strength of conclusions:
Future research with larger, longer, and rigorously controlled designs, including direct comparisons with first-line pharmacotherapies, is needed to clarify the clinical role of kava in anxiety disorders.
|
Aspect |
Category |
Details |
Practical Implications / Risk Mitigation |
References |
|
Common Side Effects |
Kava Dermopathy |
Dry, scaly, discolored skin from prolonged/high-dose use. Reversible upon discontinuation. Common in heavy traditional use (e.g., Fiji). |
Usually resolves after stopping kava. Not a sign of systemic toxicity. |
[53] |
|
|
Gastrointestinal Upset |
Nausea, diarrhea, mild digestive discomfort reported in trials and traditional use. |
Generally mild and transient. |
|
|
|
Headache |
Mild, often dose-dependent, typically occurs at initiation or with higher intakes |
Usually temporary. |
|
|
General Tolerability |
Conclusion |
At recommended anxiolytic doses (≤250 mg kavalactones/day), kava (especially aqueous extracts) is generally well-tolerated with transient, reversible side effect. |
Adherence to recommended doses minimizes common adverse events. |
[54] |
|
Hepatotoxicity Controversy |
Nature of Injury |
Idiosyncratic (rare, unpredictable, not dose-dependent). Severe cases (liver failure, transplant) reported in Western countries in the 1990s/2000s |
Risk is very low but severe. Cannot be predicted by dose alone |
[55,56] |
|
|
The "Pacific Paradox" |
Traditional Pacific Island populations consume very high doses of water-based kava but do not show proportional liver disease epidemics |
Suggested early on that traditional use was safer than Western extracts |
|
|
Proposed Causes of Liver Injury |
1. Raw Material Quality |
Use of non-noble cultivars (e.g., Tudei), aerial parts (leaves/stems), or mold-contaminated (aflatoxin) roots is a major suspect. |
Critical Factor: Always use noble cultivar root/rhizome material from reputable sources. |
[57,58 |
|
|
2. Extraction Method |
Early cases linked to organic solvents (acetone/ethanol), but causality assessments find injury across all extract types . Solvent alone is not the sole determinant. |
Prefer water-based (aqueous) traditional preparations, though not an absolute guarantee of safety |
|
|
|
|
Kava inhibits liver enzymes (CYP450), potentially causing interactions with drugs like acetaminophen, increasing toxic load |
Avoid concurrent use with medications metabolized by the liver, especially in those on multiple drugs. |
|
|
|
4. Genetic Predisposition |
Individual differences in metabolism may increase susceptibility, fitting the idiosyncratic model. No specific genetic markers confirmed. |
Explains rarity but offers no current screening test. |
|
|
Safety Recommendations |
The "Noble Kava" Doctrine |
Use only traditionally accepted, noble kava cultivars. Avoid non-noble (e.g., Tudei) varieties. |
Primary Mitigation Strategy: Sourcing noble kava is considered the most important safety measure |
[59,60] |
|
|
Extraction Preference |
Favor traditional water-based extraction methods over organic solvents to avoid concentrating lipophilic compounds |
Aligns with traditional practice and regulatory advisories. |
|
|
|
Dose Adherence |
Limit total daily intake to ≤ 250 mg of kavalactones. |
Based on clinical trial safety data for anxiolytic effect. |
|
|
|
Population Avoidance |
Contraindicated for individuals with: pre-existing liver disease, heavy alcohol use, or those taking multiple hepatotoxic medications. |
Identifies and protects the most at-risk groups. |
|
7. Regulatory Status and Contemporary Use Guidelines for Kava (Piper methysticum):
7.1. Current Global Regulatory Landscape
The regulatory status of kava varies widely between countries and regions, reflecting differing interpretations of its safety profile especially concerns about hepatotoxicity.
a. Europe
In the European Union, regulatory bodies such as the Committee on Herbal Medicinal Products (HMPC) determined that the benefit–risk balance for oral kava use in anxiety was unfavorable, and thus no EU herbal monograph was established for its medical use. Many EU members (e.g., United Kingdom) classify kava as a prohibited medicinal product, making its sale for human consumption illegal, though possession for personal use is sometimes permitted. Other countries like Poland have recently lifted bans on possession and import but still restrict commercial sale. In contrast, the Netherlands continues to prohibit most kava products for human use. These restrictions stem from case reports linking kava extracts to liver injury, particularly during the late 1990s and early 2000s, involving products marketed in Germany, Switzerland, and beyond [61].
b. North America
In the United States, kava is widely marketed as a dietary supplement, not as an approved drug. Under the Dietary Supplement Health and Education Act (DSHEA), products marketed before 1994 may remain on the market without formal safety approval, though labeling must follow Current Good Manufacturing Practices (cGMPs). The U.S. Food and Drug Administration (FDA) issued a consumer advisory in 2002 alerting the public to rare but severe liver injury reports linked to kava products and reiterated in a 2020 memorandum that kava is not Generally Recognized as Safe (GRAS) for conventional food use because of potential toxicity and drug interactions [62].
c. Oceania and Pacific Island Nations
In the South Pacific the traditional home of kava consumption export and quality-control legislation exist in countries like Vanuatu, where the Kava Act restricts export and use of non-noble kava varieties or unsuitable plant parts (leaves/stems). In Australia, commercial import and use are regulated through a National Code of Kava Management with import limits and daily kavalactone recommendations; some states previously had bans (e.g., Western Australia) that have since been lifted [63].
d. Other Regions
Various countries in Asia (e.g., Singapore) maintain bans on kava sales, while others such as Japan and South Korea reportedly restrict kava to prescription-only contexts (though official details vary). Global regulation reflects attempts to balance traditional use, public health safety, and commercial freedom amidst lingering concerns about rare hepatotoxicity [64].
7.2. Proposed Clinical Guidelines for Responsible Kava Use
Although formal clinical practice guidelines are limited, several evidence-based recommendations can be distilled from safety reviews and expert opinion to guide clinicians and consumers toward responsible use.
a. Patient Selection
Kava appears most appropriate for adults with mild to moderate anxiety or stress-related symptoms where conventional pharmacotherapy is not preferred or contraindicated. Traditional aqueous kava extracts have shown anxiolytic efficacy in controlled studies, but safety considerations remain paramount. Patients with pre-existing hepatic conditions (e.g., chronic liver disease), a history of alcohol misuse, or concurrent use of hepatotoxic drugs are at higher theoretical risk for adverse hepatic outcomes and should generally avoid kava or use it only under clinical supervision with close monitoring [65].
b. Product Selection Criteria
Quality control is critical in mitigating risk. Recommended criteria for selecting kava products include:
Experience from traditional use and clinical trials underscores that adherence to these quality parameters helps reduce incidence of adverse effects [66].
c. Dosing and Duration Recommendations
The Therapeutic Goods Administration (TGA) in Australia and similar advisory bodies recommend ≤ 250 mg of kavalactones per day to minimize toxicity risks. This dosing aligns with many clinical trials and expert reviews suggesting this threshold balances potential benefits with safety. Short- to medium-term use (e.g., up to 8–12 weeks) appears better-studied, with long-term safety data scarce; thus, extended use warrants periodic re-evaluation of benefit and risk [67].
d. Monitoring Advice
To enhance safety when kava is used clinically or as a supplement:
This structured monitoring approach borrows from recommendations in clinical safety literature and helps detect rare hepatotoxicity early [68].
REFERENCES



Deshmukh Rutuja*, Dr. Priyanka Sable, Sakshi Padole, A Pharmacological and Clinical Reappraisal of Piper methysticum (Kava) for Anxiety: Balancing Traditional Efficacy with Modern Safety, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 5015-5031. https://doi.org/ 10.5281/zenodo.20759922
 10.5281/zenodo.20759922
10.5281/zenodo.20759922