
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Department of Pharmacy Practice, Al Ameen College of Pharmacy, Bangalore, Karnataka.
2 Medical Director, St. Philomena’s Hospital, Bangalore, Karnataka
Gastrointestinal disorders refer to any conditions or diseases that occurs within the gastrointestinal tract. The impact of GI disorders may be psychological and stress provoking and the presence of stress and mood disorders can impact the state of GI disorder. Anxiety implicates in GI disorders especially IBS, GERD and PUD. The main objective of this study is to determine the prevalence of anxiety among patients with GI disorders, treatment pattern and to analyze the patients interest for receiving patient counselling. A prospective hospital based observational study was conducted for a period of 6 months at a tertiary care hospital. Hamilton's Anxiety scale was used as standard questionnaires to detect the prevalence of anxiety among the patients. During this study, a total of 80 patients with GI disorders were included, among these 48(60%) were male and 32(40%) were female; Mostly patients were middle aged; Majority of patients had higher BMI range; it was found that 39(48.75%) patients had GERD, 32(40%) had IBS and 9(11.25%) had PUD. Majority of patients with GERD and PUD were managed with PPI, commonly prescribed was Cap.Esomeprazole and Tab.Rabeprazole respectively, IBS patients were managed with Cap.Providac. Among the 80 patients,67(83.75%) had anxiety, specifically, anxiety was seen in 26(78.1%) IBS patients, 33(84.6%) GERD patients and all 9(11.25%) PUD patients;55(68.75%) patients had some profound stress as an exacerbating factor. Majority of patients had shown interest for receiving patient counselling.The study concludes that anxiety has high pevalence rate in GI patients which is neglected without giving due attention
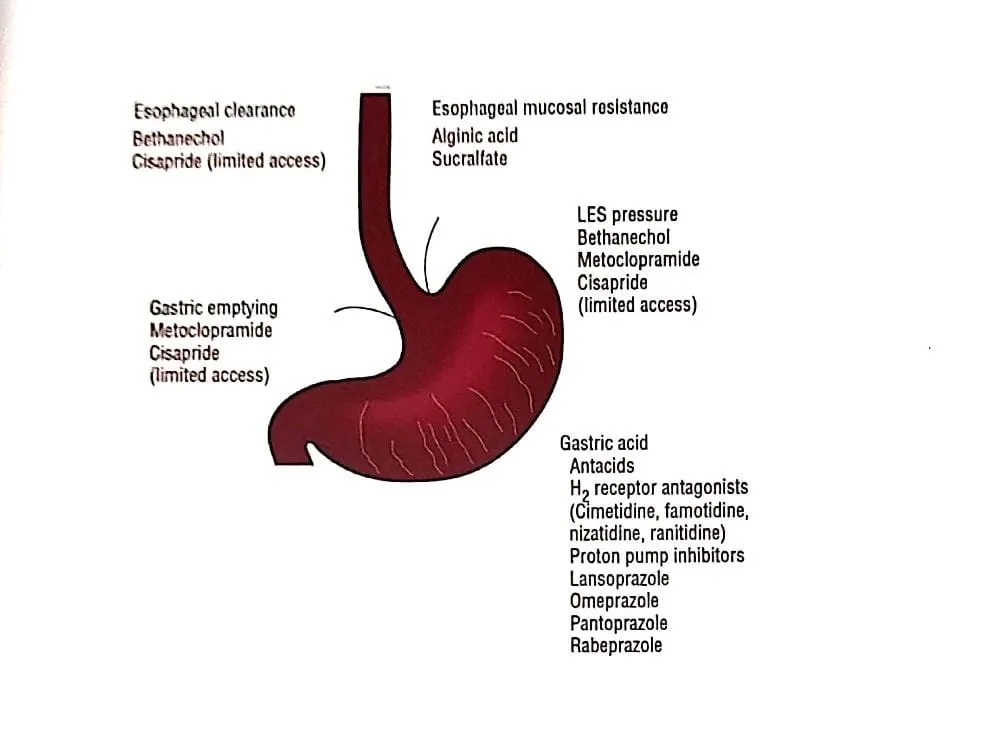
Gastrointestinal disorders are the terms used to refer any condition or disease that occurs within the gastrointestinal tract. Common gastrointestinal disorders include Gastroesophageal Reflux Disease(GERD), Irritable Bowel Syndrome (IBS), Peptic Ulcer Disease (PUD), Celiac disease, Constipation, Crohn's Disease, Diarrhea, Hemorrhoids and Anal Fissures, Ulcerative Colitis, Diverticular disease.[1] GERD is a condition that develops when there is a retrograde flow of stomach contents causing symptoms or complications.It can present as Nonerosive reflux disease (NERD) when typical symptoms of GERD occur in the absence of visible mucosal injury during endoscopy, or as erosive esophagitis ,when patients have histopathological changes in esophageal mucosa. The latter is also called reflux esophagitis. The typical symptom is heartburn. This most often occurs 30 min to 60 min after meals and upon reclining. Patients often report relief from antacids or baking soda. When patients present with this description of symptoms, the diagnosis can be established with a high degree of confidence.[2] IBS is defined by the American College of Gastroenterology as "Abdominal discomfort associated with altered bowel habits". Some people are more likely to have constipation, others diarrhea, while a few experiences both constipation and diarrhea at different times (mixed IBS) [1] PUD refers to a group of ulcerative disorders of the upper gastrointestinal (GI) tract that require acid and pepsin for their formation.[3]
1.2 Epidemiology
GERD is very common, with a prevalence of approximately 20% of adults in the western culture. Symptoms occur daily in approximately 7% of patients, weekly in 14% and monthly in 15% to 40% of all patients. Obesity also seems to increase the risk of GERD.[2] This study reports a weekly prevalence of 7.6% in the Indian population. The prevalence of GERD was 22.2% in southern India, and was more common among older subjects and men. Due to IBS 10 to 15% of people in the world are believed to be affected. In a community-based study conducted in various sites of Mumbai and Haryana among urban population of about 4000 persons IBS is seen prevalent in about 7.5% and 4% respectively.[4]The incidence of PUD in H. pylori-infected individuals is approximately 1 percent per year, a rate that is higher than for uninfected individuals. A systematic review of seven studies from developed countries indicated a population-based one-year prevalence of PUD of 0.1 to 1.5 percent based on physician diagnosis.[3]
1.3 Mental health disorders
Mental health disorders are conditions involving changes in emotion, thinking or behaviour (or a combination of these). Mental illnesses are associated with distress and/or problems functioning in social, work or daily activities.[5] Some of the main groups of mental disorders are: mood disorders (such as depression or bipolar disorder) anxiety disorders , personality disorders , psychotic disorders (such as schizophrenia) eating disorders, trauma-related disorders (such as post-traumatic stress disorder) substance abuse disorders.[6]
1.4 Anxiety
Anxiety disorders form a category of mental health diagnoses that lead to excessive nervousness, fear, apprehension, and worry. These disorders alter how a person processes emotion and behave, also causing physical symptoms. Mild anxiety might be vague and unsettling while severe anxiety may seriously affect day-to-day living.[7]
1.5 RELATIONSHIP BETWEEN GI DISORDERS AND MENTAL HEALTH DISORDERS (Anxiety/ Emotional stress)
In clinical studies there is a strong relationship between gastrointestinal symptoms and anxiety. Emotional stress and depression can down-regulate various parts of the immune system.[8] Anxiety may play a role in the development of GERD and in worsening of symptoms, although the connection between two is unclear. Some experts believe that a brain chemical cholecystokinin (CCK), which has been linked to panic and gastrointestinal disorders, may play a role in the prevalence of GERD in people with anxiety disorders. Moreover, theories suggest anxiety can slow digestion, increase stomach acid, resulting in increased muscle tension that can put pressure on the stomach.[9]In patients with GERD, increased levels of anxiety are associated with increased severity of retrosternal pain and heartburn and reduced quality of life.[10] It is possible that emotional stress induced behavioral risks such as smoking and the use of NSAIDs that in turn alters the inflammatory response or resistance to HP infection that may cause PUD otherwise the role of stress and how it affects PUD is complex and probably multifactorial correlation of IBS with Mental health disorders.Psychiatric interventions (pharmacologic or psychotherapy) have proved effectiveness in the improvement of IBS patients symptoms in functionality and there seems to be improvement in the general quality of life for the patient.[11]
Objectives
Primary objective
Secondary objective
Therefore, this study aims to shed light on the prevalence of anxiety disorders among patients with GI disorders, highlighting the significant impact of mental health on their overall condition. By understanding this relation, it underscores the importance of incorporating appropriate psychological support and therapeutic interventions to enhance patient outcomes and quality of life.
2. METHODOLOGY
Study Site: A tertiary care hospital
Study Period: 6 months
Study Design: Hospital based prospective observational study
Inclusion Criteria: All In-Patients and Out -patients of both genders above 15 years of age who were diagnosed with Irritable Bowel Syndrome as per ROME III Criteria, GERD and Peptic Ulcer as per ICD 10 guidelines.
Exclusion Criteria:
Sources of Data:
Procedure: Research students collected both In-patients and Out-patients data who met the inclusion criteria as mentioned and assessed for the prevalence of anxiety using the Hamilton's Anxiety Scale. The data collected was pooled and analysed for results.
Statistical Analysis: Descriptive statistics was used.
Ethical Approval: Ethical clearance was obtained from Institutional Ethics Committee of the hospital.
A prospective observational study was carried out at a tertiary care Hospital for a period of 6 months. A total of 80 patients were included in study after obtaining ethical clearance and informed consent, out of them 48(60%) were males and 32(40%) were females as showed in Fig. 1.This was in accordance with the study conducted by Arko Banerjee, et al[12]. Fig. 1 shows majority of patients were found to be middle aged but no significant effect of age on the prevalence of anxiety among these patients was observed. The patients were categorized based on their BMI it was found that there was no significant impact of BMI. The above two parameters were similar to the study conducted by Seyed Alireza Haji Seyed Javadi, et al[13]. Social history was considered to see its influence on the prevalence of anxiety in patients and in our study it was found, 46(57.5%) patients did not have any significant social history, 14(17.5%) patients had history of alcohol, 11(13.75%) were smokers,9(11.25%) had both smoking and alcohol history. The next parameter taken into consideration was based on the clinical admission of patients and it was observed that 74(92.5%) were Out-patients and 6(7.5%) were In-patients.
Out of 80 patients included in study 39(48.75%) patients had GERD, 32(40%) patients had IBS, and 9(11.25%) patients had PUD. Considering the comorbidities of patients, it was observed that 23 (29%) patients did not have an existing comorbidity. 19 (24%) patients had T2DM, 17 (21%) patients had hypertension, 7(9%) had IHD, 4 (5%) had anemia, others had seizure disorder, cholecystitis, CKD, migraine, bronchial asthma, dyslipidemia, hypothyroidism and rheumatoid arthritis respectively. Diagnosis of any disease/disorder needs both subjective and objective evidence. In accordance to this we found that confirmatory diagnosis was made based on gastro endoscopy, Colonoscopy, clinical decisions/expert opinion , both gastroscopy and abdominal scan.It is known that the etiology of PUD can be due to H. pylori infection or due to other factors like NSAIDs etc. Out of 9 patients 6 (66.7%) patients had PUD due to H. pylori and 3(33.3%) were due to other factors.
The management of GI disorders varies depending on the type. Fig. 4 shows, 48 (60%) patients received PPI, 16(20%) patients with only Probiotic Capsules (Cap. Providac) about 14 (17.5%) patients with Probiotic Capsules (Cap. Providac) + Rifaximin (T. Rifagut), 2 (2.5%) patients with Cap. Providac + Rifaximin + PPI. The pattern of prescribing medicines for specific GI disorders were also noted. Among 32 IBS 16 (50%) patients received Probiotic Capsules, 14 (43.75%) patients were given Probiotic Capsules + Rifaximin and 2 (6.25%) patients with Cap.Providac + Rifaximin + PPI. Among 39 GERD patients PPI were the main drug given for its treatment. The most commonly prescribed PPI for GERD was Cap.Esomeprazole for about 21(53.84%) patients, Tab.Pantoprazole was given to about 12(30.76%) patients and the rest 6(15.38%) patients received Tab. Rabeprazole. For all 9 PUD follow up patients Tab.Rabeprazole was prescribed as treatment. Hamilton Anxiety Scale (HAMA) was used to assess the prevalence of Anxiety among patients. Fig 2 shows out of 80 patients, 67 (84%) patients had anxiety which included 37 (46.25%) patients with mild anxiety, 11 (13.75%) with mild to moderate and 19 (23.75%) with moderate to severe and the rest 13 (16.25%) patients were normal. The distribution based on prevalence of anxiety were exclusively studied further among patients with IBS, GERD and PUD. Out of 32 IBS 14 (42.4%) patients had mild anxiety, 3 (9.1%) had mild to moderate anxiety and 9 (27.3%) with moderate to severe anxiety. Only 7 (21.2%) patients did not have anxiety. This was analogous to the study conducted by Mohamad Jafar Modabbernia, et al [14]. Majority of IBS patients with mild, mild to moderate and moderate to severe anxiety was observed to have the condition for the duration of less than 1 year. Almost one third of patients with IBS had anxiety disorder. This proves our study was parallel to the one done by Changchun lee, et al [15]. The presence of co-morbidities as an effect on anxiety among IBS patients were considered, as multiple disease condition with polypharmacy prescription might have direct/indirect effect on patient's mental health.
Out of 39 GERD patients, the prevalence of anxiety was observed for about 33 patients (84.6%) out of which, 17 (43.6%) patients had mild anxiety, 6 (15.4%) patients with mild to moderate anxiety, 10 (25.6%) with moderate to severe anxiety and 6 (15.4%) patients were normal. This was found to be akin with the studies of Salch Mohammad, et al.[16] and Pawan Rathi, et al, [17].(Fig 3) Further duration of disorder among GERD patients was considered, out of those 17 patients with mild anxiety 7 (41.1%) patients were newly diagnosed, 5 (29.4%) patients were diagnosed with GERD for less than 1 year, 4 (23.6%) with 1 to 5 years and 1 (5.9%) diagnosed for more than 5 years. Similarly, out of 6 patients with mild to moderate anxiety, 3 (50%) patients had GERD for 1-5 years of duration, 2 (33.3%) patients were newly diagnosed and 1 patient (16.7%) was diagnosed for less than 1 year and for the 10 patients with moderate to severe anxiety, 3(30%) patients were newly diagnosed with GERD, 3 (30%) patients had condition for more than 5 years, 2 (20%) for less than 1 year and 2 (20%) patients bad condition for 1-5 years. The presence of comorbidities was also considered for GERD patients with anxiety. Out of 9 PUD patients all had anxiety which included, 7 (77.8%) patients with mild anxiety and 2 (22.2%) patients with mild to moderate anxiety was. This result was in accordance with the study conducted by Wei-Yen Lim, et al[18]. The duration of the disorder was observed to be more than 5 years for patients with mild to moderate anxiety. For PUD patients with mild anxiety the duration of disorder observed was that, 2(28.6%)patients were newly diagnosed, 2 (28.6%) patients had condition for 1-5 years, 2 (28.6%)patients had for more than 5 years, and 1 (14.2%) patient for less than one-year duration. For PUD patients with anxiety the comorbidities observed was that, hypertension and IHD respectively, and TDM and Dyslipidemia. Anxiety was shown with stressful life events. Hence, anxiety symptoms should be specifically assessed and treated in GI disorder along with the other co-morbidities. In our study stress was found to be a common cause/exacerbation factor for anxiety. Out of 80 patients 55 (68.8%) patients reported having some profound stress factor for worsening their condition that affected their mood as well, and about 25(31.2%) patients did not have any stress. Patient counselling is one of the non-pharmacological therapy for patients with disturbed mental health but practically GI disorder patients were never assessed for their mental health. Keeping this point in mind the interest for counselling session was questioned to all our study subjects. Among 80 patients 53 (66%) patients showed interest for patient counselling and 27(34%) were not interested.
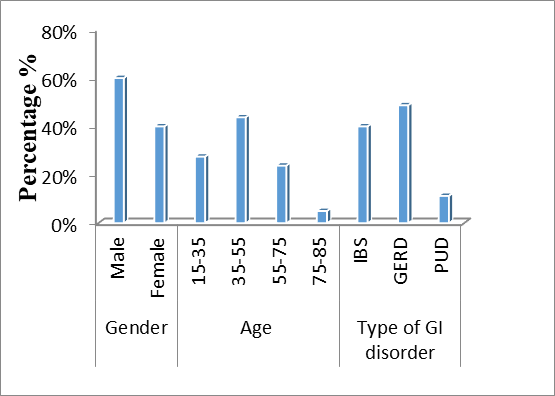
Fig 1: Distribution Based on Gender, Age in (years) and Type of GI Disorders
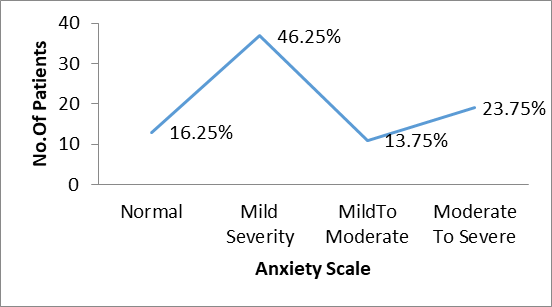
Fig 2: Distribution Based on Prevalence of Anxiety Among Patients with GI Disorders
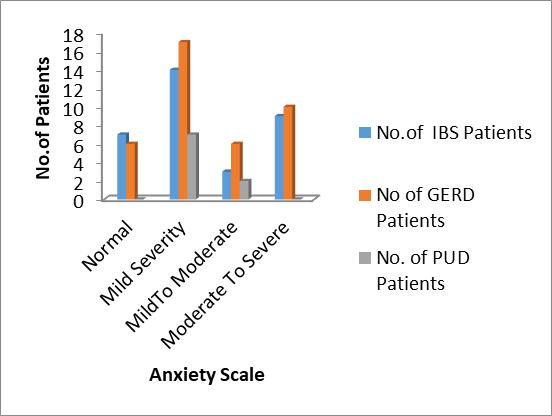
Fig 3: Distribution Based on Prevalence of Anxiety Among Patients with IBS, GERD and PUD
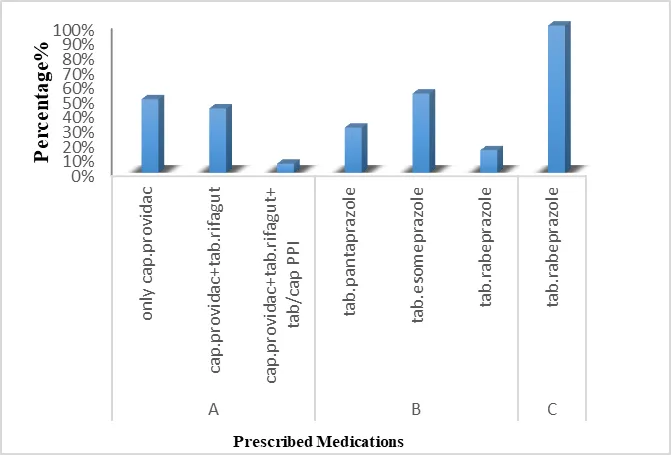
Figure 4: Distribution Based on the Pattern of Prescribed Medication for IBS ,GERD and PUD ; A,B and C are Pattern of Prescribed Medications For IBS, GERD and PUD respectively.
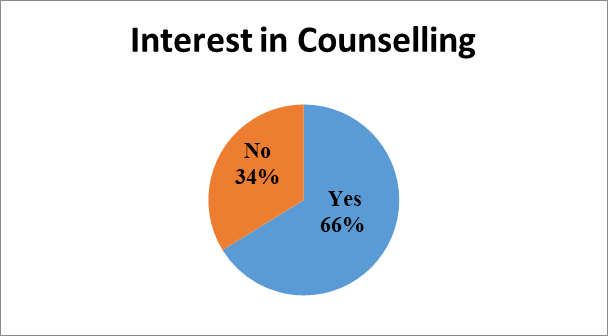
Figure 5: Distribution Based on Patients Interested in Counselling
CONCLUSION:
A 6-month observational study conducted at a tertiary care Hospital included 80 patients with gastrointestinal (GI) disorders, enrolled from both in-patient and out-patient departments. The study revealed a higher prevalence of GI conditions among middle-aged males with elevated BMI. GERD was the most common disorder, followed by IBS and PUD. PPI, particularly esomeprazole and rabeprazole, were commonly prescribed for GERD and PUD, while IBS was mainly managed with probiotics like cap.providac. Notably, 83.75% had anxiety, with significant psychiatric comorbidity seen across all GI conditions. Around two-thirds of patients reported profound stress, and many expressed interest in counselling services. The study concludes that anxiety is highly prevalent yet often overlooked in GI patients, underscoring the need for a multidisciplinary care approach to improve both physical and mental health outcomes.
ACKNOWLEDGEMENTS
We sincerely thank to our Guides and our hospital for providing clinical support and facilities, and our college for their guidance and encouragement. Their invaluable collaboration made this work possible.
Conflicts of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article
REFERENCES

: T. Vithya, Sakshi Pawar*, Ishrat Jahan, Maithreyi Thamattoor, Jampa Yangchen, Sahar Raiati, Shankar Prasad, A Study on Prevalence of Anxiety Disorder Among Patients with GI Disorder (Irritable Bowel Syndrome, Gastroesophageal Reflux Disease and Peptic Ulcer), Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, , 4469-4478. https://doi.org/ 10.5281/zenodo.20745283
 10.5281/zenodo.20745283
10.5281/zenodo.20745283