
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
NIMS Institute of Pharmacy, Jaipur Rajasthan
Stroke is a serious health emergency of both ischemic and haemorrhagic nature that has emerged as one of the most critical health-related problems in the world that causes irreversible and severe neurological damage. This review is a summary of the anti-stroke agents, their mechanism, their current clinical uses, and their future prospects. We talk of pharmacological interventions which have been well determined by the research to prevent stroke or neuroprotector to preserve the brain tissue which remains alive and to restore blood flow to the ischemic regions. Particular focus is paid to the acute management, such as thrombolytic agents such as alteplase, and secondary prevention techniques. The use of anti-stroke agents in stroke rehabilitation and recovery especially by neuroprotective agents and regenerative therapy including stem cell-based therapy and cerebral organoids is also discussed. Nevertheless, the review also implies the neurorestorative nature of traditional Chinese herbal medicines and emerging potential of nanotechnology-based drug delivery systems to enable targeted therapy despite these current barriers and constraints, whereby narrow therapeutic indices of acute therapies, problems with translating relevant preclinical results to success in clinic and complexities involved in optimization and safety testing of new emerging therapeutic approaches such as stem cell transplantation and nanomedicines remain. Resolving such difficulties, the future concerns are based on the dire necessity to conduct further researches on new, less harmful, and more efficient neurotherapeutic agents and more efficient approaches to treatment to reduce the severe effects of stroke.
Stroke or cerebral infarction is a serious medical emergency that has a far reaching effect on both respiratory and cardiovascular systems with many resulting in severe and permanent neurological damage[1]. It is a significant global health issue and one of the two greatest causes of mortality and morbidity, and its epidemiological and economic consequences are very high in the entire world [1,2,3,]. There are two broad groups of strokes; ischemic that develops in the case of the blockage of blood vessels, and haemorrhagic that develop as a result of cerebral blood vessel rupture[2]. Both of them result in the lack of necessary oxygen and glucose supply to brain tissue, which may cause the death of millions of neurons in a few minutes and further worsen the neurological damage[3]. Therefore, there is the need to develop highly effective anti-stroke drugs to reduce these dire effects. Pharmacological treatment normally aims at achieving three major goals namely prevention of stroke, neuroprotection to protect viable brain tissue and reperfusion of blood to ischemic regions [4]. The objectives of these treatments include maintenance of the ischemic penumbra, minimization of infarct size and sustained cerebral blood flow through the complex molecular events surrounding ischemia[5]. Despite some progress in the treatment methods particularly the use of thrombolytic drugs in case of an ischemic stroke, more effective and safer anti-stroke drugs are still being searched [3]. Complex pathophysiology of stroke and the challenges of the successful translation of promisingly preclinical results into an effective clinical application demonstrate how necessary further studies of new neurotherapeutic agents and a more efficient treatment regimen are[6,7] . Although several reviews have discussed stroke pathophysiology, thrombolytic therapy, and neuroprotection individually, limited reviews comprehensively integrate conventional anti-stroke agents with emerging therapeutic approaches such as stem cell therapy, gene-based therapeutics, mitochondria-targeted interventions, and nanotechnology-enabled drug delivery systems[8]. Furthermore, recent advances in regenerative medicine and precision-targeted therapies have not been critically evaluated alongside current clinical applications and translational challenges. Therefore, this review provides an updated and integrated overview of anti-stroke therapies, highlighting current evidence, therapeutic limitations, and future directions for improving stroke outcomes.
4. Classification and Pathophysiology of Stroke
4.1 Types of Strokes
4.1.1 Ischemic Stroke
The most common type is ischemic stroke, which is caused by the obstruction of a blood vessel in the brain leading to neurological deficits. This obstruction may be due to thrombus, embolus or stenosis of the artery [9]. It is a complicated disorder that has multiple etiologists such as macroangiopathy, cardio embolism and cerebral small-vessel disease. Some of the risk factors are hypertension, diabetes, hypercholesterolemia, smoking, obesity and traumatic brain injury. Early diagnosis and acute therapeutic measures, including thrombolysis, are required, with a time constraint[10]. Lifestyle change, including smoking cessation, healthy diet and blood pressure control is a long-term prevention method. It is also important to customize treatment depending on the cause of a stroke[11].
4.1.2 Hemorrhagic Stroke
A bleeding in the brain tissue is called haemorrhagic stroke, and it consists of 10-15 percent of all the strokes; the morbidity and mortality of haemorrhagic strokes are higher than ischemic strokes. It is usually presented as a subarachnoid or intracerebral bleeding. Ruptured cerebral vessels are the common cause of ICH in case of chronic hypertension that doubles to six times the risk [12]. Others are cerebral amyloid angiopathy, bleeding disorders, therapeutic anticoagulation, and vascular malformations. Haemorrhagic strokes are more-severe and the mortality rate is quite higher particularly during the first three months because of complications like the growth of hematoma and oedema[13,14].
4.2 Pathophysiological Mechanisms in Stroke
4.2.1 Cerebral Ischemia and Energy Failure
Far-reaching energy inadequacy brought about by inadequate oxygen and glucose (vital substances in the production of ATP) initiates cerebral ischemia. This causes an instant change to anaerobic glycolysis with low ATP production and accumulation of lactic acid and acidosis. The loss of ATP cannot sustain the essential ion pumps, including Na+K+ATPase, to keep neuronal membrane potentials normal, leading to disruptive Na+, calcium and K+ efflux[15]. The resultant excessive intracellular calcium overflow, which is caused by ion dyshomeostasis, results in excitotoxicity, increases the release of excess glutamate causes neuronal depolarization, and impairs mitochondrial activities, causing oxidative stress and subsequent formation of harmful reactive oxygen species[16]. These processes are interrelated causing cell death and neuronal damage which is irreversible. An area around it, called ischemic penumbra, is the area at risk that can be rescued in case blood flow is reinstated[17].
4.2.2 Excitotoxicity and Calcium Overload
Excitotoxicity and calcium overload are some of the mechanisms of neuronal damage in stroke. Ischemia disregards neuronal and astroglia membrane potentials, which cause a large elevation in the extracellular glutamate levels as a result of heightened release and lowered reuptake [18]. This glutamate surplus causes over-activation of ionotropic receptors which are predominantly, N-methyl-D-aspartate and alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptors, leading to an unregulated inflow of calcium ions into the cells[19]. This pathological increase in intracellular calcium leads to a degrading cascade in the activation of many catalytic enzymes, such as proteases (calpains and caspases), lipases, which subsequently degrades key cellular proteins and membrane systems. Also, the calcium overload causes mitochondrial dysfunction, which is depolarization, generation of reactive oxygen species, lipid peroxidation, and the opening of the mitochondrial permeability transition pore [20]. To this list of events, there are also additions that interfere with cellular energy production, produce toxic free radicals, and in the end cause neuronal damage and cell death by necrotic and apoptotic mechanisms. Although it is well known that these processes are involved, clinical studies of excitotoxicity and calcium overload inhibition using drugs like NMDA antagonists or calcium blockers have produced few positive effects or severe adverse effects[21] .
4.2.3 Oxidative Stress and Free Radical Generation
The pathophysiology of stroke includes oxidative stress and the formation of free radicals, which cause serious cell destruction. Ischemic and haemorrhagic strokes also cause an excessive formation of reactive oxygen and nitrogen species that interfere with the fine balance of redox in the brain[18]. Oxidative assault is especially susceptible to the brain, which has a high metabolic rate and lipids are very abundant. Ischemia leads to accumulation of ROS, and on reperfusion, blood flow restoration is associated with an increase in this stress due to the explosion of free radicals of various sources: mitochondria, NADPH oxidase[22]. This imbalance triggers lipid peroxidation, protein oxidation and DNA fragmentation thus triggering apoptotic pathways. Moreover, nitric oxide also reacts to produce highly toxic peroxynitrite which further damages cells, inflames and disrupts blood-brain barrier ultimately damaging neurons, glia, and endothelial cells[23].
4.2.4 Neuroinflammation
The neuroinflammation is a critical pathophysiological process of stroke that is present during the acute and chronic stages. It is a response to brain injury, necrosis and apoptosis, which causes damage-associated molecular patterns and reactive oxygen species to be released and activates nuclear factor κB pathways[24]. This results in the inflammation of resident immune cells, i.e., of microglia and astrocytes, and the entry of peripheral immune cells, i.e., of neutrophils, monocytes, and lymphocytes, into the brain parenchyma. These cells produce a cascade of pro-inflammatory cytokines (e.g., TNF- 0, IL-1 and IL-6), chemokines, and matrix metalloproteinases. This inflammatory process enhances brain damage which contributes to disruption of the blood-brain barrier, oxidative stress, cerebral oedema and cell death as well as affecting tissue repair and functional recovery[18].
4.2.5 Apoptosis and Cell Death Pathways
One of the most important pathophysiological processes in stroke, occurring especially in neurons in the ischemic penumbra, where recovery potential exists, is apoptosis, or one of the major forms of programmed cell death. This is a process that is characterized by specific morphological alterations, such as cell shrinkage, cytoplasmic condensation and DNA fragmenting, which is usually devoid of an inflammatory reaction[25]. Excessive calcium accumulation into the cell (which results in mitochondrial depolarization and dysfunction) is a critical event that causes apoptosis. This dysfunction leads to cytochrome C release which leads to caspase cascade activation, including caspase-3 that are key players in neuronal death. The balance of pro- and anti-apoptotic proteins of the Bcl-2 family is also involved in the regulation of mitochondrial apoptosis[26]. Excitotoxicity which is caused by over stimulation of glutamate and NMDAR also enhances these pathways of apoptosis by the production of free radicals and the impairment of mitochondria[27].

Figure 1 : Diagram illustrating classification and pathophysiology of stroke, divided into two sections: types of stroke and pathophysiological mechanisms. Section one details ischemic and hemorrhagic stroke with associated risk factors, while section two explains apoptosis, cerebral ischemia, oxidative stress, neuroinflammation, and excitotoxicity using labeled cellular components and biochemical pathways.
5. Mechanisms of Action of Anti-Stroke Agents
5.1 Thrombolytic Agents
Thrombolytic agents play a pivotal role in the treatment of acute ischemic stroke because they actively dissolve the clots of blood, hence, replenishing the blood supply to the ischemic brain tissue. The initial action is the activation of the plasminogen to form plasmin which is a powerful enzyme that breaks down fibrin which is the major building block of blood clots. A recombinant tissue plasminogen activator (rtPA) like alteplase is a major thrombolytic protein that shows a significant affinity towards fibrin and is able to directly activate plasminogen on the surface of the clot[28]. This fibrin specific effect reduces the chance of systemic bleeding when compared to non-fibrin specific agents. It takes place in two stages, where a slow stage is the first stage whereby the plasminogen on the surface of fibrin is activated by single-chain tPA and the rapid stage whereby partial degradation of fibrin reveals more binding sites, transforming single-chain tPA into its more active two-chain functional form and continuously generating plasmin. Similar fibrinolytic pathways are also involved in other agents like non-immunogenic staphylokinase and Tenecteplase[29].
5.2 Antiplatelet Agents
Antiplatelet agents are also important in the prevention and control of ischemic stroke because they inhibit platelet aggregation and the occurrence of thrombus. These are the drugs which mainly disrupt platelet activation and coagulation cascades. Aspirin is an antiplatelet agent that is commonly used, which irreversibly suppresses platelet cyclooxygenase inhibiting the production of thromboxane A2, a powerful platelet aggregate[30]. Clopidogrel is another type of drug which, like P2Y12 adenosine diphosphate receptor, attaches irreversibly to the platelet surface and hence ADP-induced platelet aggregation is inhibited. Ticagrelor acts in the same way but is a more reversible P2Y12 receptor inhibitor. In addition, tirofiban, eptifibatide, and abciximab are tirofiban, eptifibatide, and abciximab, which are glycoprotein IIb/IIIa receptor antagonists that inhibit an important platelet aggregation pathway. P2Y12- and TXA2-targeted novel compounds that inhibit aggregation triggered by an ADP and arachidonic acid have also been designed[31].
5.3 Anticoagulant Agents
Anticoagulants play an important role in the prevention and treatment of stroke through the prevention of the formation of blood clots, which may block blood circulation. These agents disrupt the coagulation cascade in a number of ways. Anticoagulants are generally divided into direct and indirect thrombin inhibitor and direct Factor Xa inhibitors. In this case, an example of such an inhibitor is argatroban, which is a direct selective inhibitor of thrombin, which is one of the enzymes involved in the formation of clots[32]. There is also the use of indirect thrombin inhibitors, which are unfractionated heparin and low molecular weight heparin, which inhibit the activity of thrombin and thus prevent clotting. Also, direct oral anticoagulants like rivaroxaban are specific and target Factor Xa, an upstream element in the coagulation cascade that is necessary in the formation of thrombin. These stages are met and therefore prevent and treat thromboembolic events in stroke by anticoagulants[33].
5.4 Neuroprotective Agents
Neuroprotective agents strive to protect the brain tissue against the multifocal damage caused by stroke, especially in the ischemic penumbra. They use various different mechanisms, including excitotoxicity, oxidative stress, inflammation, and apoptosis. These agents attempt to avert the neuronal cell death by diminishing the loss of ATP, eliminating glutamate-induced excitotoxicity, and opposing the production of free radical [34]. As an example, oxidative damage is directly counteracted by free radical scavengers, i.e. edaravone. There are also neuroprotective effects of minocycline that is inhibitory of microglial activity, glutamate toxicity and caspase 1-dependent apoptosis. Stroke can be enhanced by growth factors that decrease the damage by acting as anti-apoptotic and anti-inflammatory. Resveratrol also emphasizes neuroprotective measures because of its antioxidative, anti-inflammatory, and anti-apoptotic effects, which is frequently achieved by strengthening the endogenous cellular antioxidant mechanisms[35]. Since stroke is a complex pathology, one neuroprotective agent might not be sufficient, and one might consider that a combination of the agents will work together in a multifaceted approach to provide more extensive protection[36].
5.5 Anti-inflammatory and Antioxidant Agents
Anti-inflammatory and antioxidant agents play an important role in reversing the damages caused by the stroke by acting on critical pathological mechanisms. Anti-inflammatory drugs make neuroinflammation less prominent; it is a major cause of brain damage. As an example, olive polyphenols are reinforcing nuclear factor kappa B, pro-inflammatory cytokines, including IL-1b and TNF-a, inducible nitric oxide synthase (iNOS) and cyclooxygenase-2[37]. Shrimp lipid bioactive, adjust inflammatory signaling, diminish the metabolism of inflammatory mediators and decrease migration of macrophages and inflammatory gene expression. Antioxidants fight the harmful action of oxidative stress. Directly scavenging the free radicals are the herbal medicines and olive polyphenols which prevent oxidative damage[38]. The olive polyphenols also enhance the activities of antioxidant enzymes and chelate metals including iron that can increase inflammatory oxidative bursts. Astaxanthin, a compound derived by shrimps, inhibits superoxide anion and improves the action of glutathione peroxidase and, as a result, lowers the activity of lipid peroxidation and carbonylation of proteins. The combination of these actions helps save the brain tissue of severe damage after a stroke[39]
Table 1 : Classification of Anti-Stroke Agents
|
Class |
Examples |
Mechanism |
|
Thrombolytics |
Alteplase, Tenecteplase |
Clot dissolution |
|
Antiplatelets |
Aspirin, Clopidogrel, Ticagrelor |
Inhibit platelet aggregation |
|
Anticoagulants |
Heparin, Argatroban, Rivaroxaban |
Prevent thrombus formation |
|
Neuroprotective Agents |
Edaravone, Minocycline |
Reduce neuronal injury |
|
Anti-inflammatory Agents |
Olive polyphenols |
Suppress inflammation |
|
Antioxidants |
Resveratrol, Astaxanthin |
Scavenge free radicals |
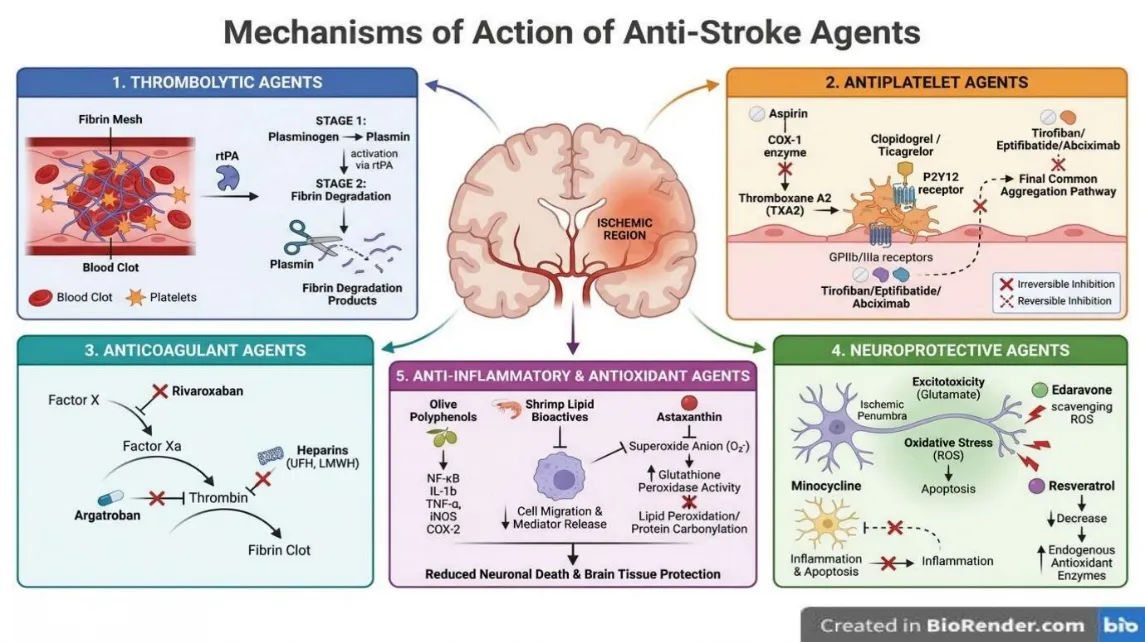
Figure 2 : Diagram illustrating mechanisms of action for five types of anti-stroke agents, including thrombolytic, antiplatelet, anticoagulant, neuroprotective, and anti-inflammatory & antioxidant agents. Each section uses color-coded boxes with labeled pathways, molecular targets, and effects such as clot degradation, platelet inhibition, reduced neuronal death, and decreased oxidative stress, highlighting key drugs and biochemical interactions involved in stroke treatment.
6. Clinical Applications of Anti-Stroke Agents
6.1 Acute Management of Ischemic Stroke
Thrombolytic agents are very important in the acute treatment of ischemic stroke as they are used to dissolve the blood clots and reestablish cerebral blood. The approved FDA thrombolytic agent is the recombinant tissue plasminogen activator (tPA), alteplase, which is currently under clinical use[9]. Its application is suggested intravenously in 4.5 h after the symptoms appear, with endovascular thrombectomy in combination in most cases being the most effective. The average dosage of alteplase is 0.9 mg/kg in which 10 percent is administered as a bolus and the rest 90 percent as an infusion over 60 minutes. Alteplase has a narrow therapeutic index despite being effective thus can only be used by a small proportion of eligible patients and harbours the risk of haemorrhage[40]. Tenecteplase is an up-and-coming alternative with similar safety and efficacy to alteplase, and the benefit of a single bolus, which is the easiest and fastest to administer [31]. The clinical treatment of the acute ischemic stroke mainly aims at quickly eliminating clots but the limitation of the therapeutic window is still an important issue[41].
6.2 Secondary Prevention of Stroke
To prevent stroke secondary prevention, anti-stroke agent clinical use is mainly aimed at addressing the underlying risk factors and the recurrence of events. Eprosartan and telmisartan are antihypertensive agents, which have critical roles in lowering blood pressure, a major determinant of stroke recurrence[42]. There is a high level of effectiveness of lipid-lowering drugs, especially statins, like atorvastatin. In SPARCL study, the risk of subsequent stroke was reduced significantly by 16% using atorvastatin within the sample of patients who had TIA or minor stroke. Antithrombotic treatments, such as antiplatelet treatment and anticoagulants, play an important role in the prevention of the formation of new clots. Another high-risk factor is diabetes, the management of which is done with hypoglycaemic drugs. The overall application of these agents will tackle the different physiological pathways that cause stroke, and thus, reduce the chance of a stroke recurring drastically [43].
6.3 Management of Hemorrhagic Stroke
According to the available information, no special FDA-approved drugs are particularly available as of now in the management of haemorrhagic stroke. Whereas the use of anti-stroke agents has become widespread when dealing with ischemic stroke, the treatment paradigms vary greatly when dealing with haemorrhagic stroke, where the brain is involved in bleeding and not developing a clot. Tissue plasminogen activators (tPA) such as alteplase, which are some of the agents used in ischemic stroke, may result in haemorrhage as one of their serious side effects, including symptomatic intracerebral haemorrhage[44]. The design of effective stroke therapeutic agents is an urgent requirement as numerous neuroprotective agents targeting multiple pathological cascades have not been subject to much success in clinical trials, and in many cases, these drugs are unable to be extrapolated to clinical efficacies[45].
6.4 Role in Stroke Rehabilitation and Recovery
Anti-stroke agents play a significant role in stroke rehabilitation and recovery, filling multiple neurological and functional brain deficits. Edaravone is a free radical scavenger, neuroprotective drug with proven beneficial effects in terms of reducing infarct volume and enhancing the outcome of rehabilitation processes, including motor functional gains and independence. Recovery can be facilitated by growth factors and minocycline since these two have neuroprotective benefits[46]. Along with neuroprotection, such regenerative solutions as stem cell-based therapies and cerebral organoids are also emerging. Isografting cerebral organoids, such as, has been shown to recreate the injured motor cortex, alleviate brain injury and improve motor functioning associated with the nervous system in experimental animals. This is done by more neurogenesis, synaptic regeneration, axonal regeneration and enhanced neuronal survival. Moreover, nanoparticle formulations comprising of agents like N-oleoyl ethanolamine have been demonstrated to enhance motor skills and cognitive abilities including spatial learning and memory, in addition to protecting the brain and reducing inflammation after a stroke[47].
7. Emerging Anti-Stroke Therapies and Novel Targets
7.1 Stem Cell-Based Therapies
Stem cell-based therapies are a relatively new and promising area of future in anti-stroke care, which should restore and regenerate the impaired brain tissue. These treatments use the available properties of many forms of stem cell including mesenchymal stem cells, induced pluripotent stem cells (iPSCs) and neural progenitor cells [48]. Their therapeutic actions are facilitated by various mechanisms: they have the ability to differentiate into new neurons and glial cells to substitute those that were lost during the stroke, release a wide range of bioactive molecules, including growth factors and cytokines (paracrine effect), and regulate immune and inflammatory responses. Another important new target is mitochondrial repair, in which MSCs are able to deliver healthy mitochondria to injured brain cells, restoring aerobic respiration as well as inhibiting apoptosis[49]. Moreover, researchers are looking at stem cell-generated conditioned media and secretum’s as potent to diminish the size of lesions, enhance motor performance, and neurovascular restructuring. Though many clinical trials are ongoing, mostly in phase I and II, there are still difficulties in finding the best type of cells, doses, delivery methods, and a stable graft survival and integration in the long run[50].
7.2 Gene and RNA-Based Therapies
Gene- and RNA-based treatments are arising as the new and promising ways of treating a stroke, mostly aimed at controlling gene expression to mitigate the injury and ensure recovery. The role of microRNAs (miRNAs), a type of short non-coding RNA, in the pathophysiology of strokes has received a lot of attention. Some miRNAs have an aberrant level that causes damage in ischemic stroke and therefore constitute a good therapeutic intervention in stroke. Indicatively, it has been demonstrated that inhibiting miR-141-3p, which is increased after stroke, has the potential to improve the recovery of the stroke. Developers are also looking into nanoparticle-based anti-miRs, including phosphorothioates and peptide nucleic acid-based anti-miRs, to be used to target certain microRNAs. These RNA-based medicines function by either cleaving of target messenger RNA (mRNA) or sterically blocking of mRNA-ribosome interactions, thus regulating expression of genes[51]. The development of these therapeutic modalities has a major challenge of efficient delivery of these agents across the blood-brain barrier. Nonetheless, nanoparticles can provide a pathophysiological benefit to disrupt blood-brain barrier in stroke and have their therapeutic effect[52].
7.3 Mitochondria-Targeted Therapeutics
The therapeutic approach of mitochondria is a new approach to stroke treatment that may help resolve the crucial role of mitochondrial dysfunction in cell damage and stroke death in neurons. Mitochondria are affected by ischemic stroke resulting in dysfunction, low ATP generation, elevated oxidative stress, calcium overload, and demonstration of apoptotic pathways[53]. Innovative treatment methods are meant to heal the mitochondria and preserve the brain cells. Naturally occurring compounds are being studied as having the potential to improve the functionality of the mitochondria, decrease the production of reactive oxygen species, and block mitochondrial apoptotic mechanisms. Such examples are Noto ginsenoside R1, which enhances mitochondrial morphology and ATP levels and oxyresveratrol, which suppress cytochrome c release and caspase-3 activation[54]. Additionally, there are more sophisticated drug delivery systems, including mitochondria-targeted nanocarriers (e.g., TPP-modified and ceria nanoparticles), which are being designed to deliver the antioxidants and other therapeutics agent directly to the mitochondria, effectively scavenging the ROS, and providing neuro-protection. Other uses of mitochondrial repair are found in stem cell-based therapies, which involve transfer of healthy mitochondria to a damaged cell to restore the functionality of the cell, and to induce neurological recovery[55].
7.4 Nanotechnology-Based Drug Delivery Systems
The drug delivery systems that have been developed using nanotechnology are changing the way stroke is treated by addressing the issue facing the other therapies including limited therapeutic effects, low half-lives, and ineffective delivery through the blood-brain barrier[56]. Nanoparticles provide efficient drug loading, regulated release, increased BBB permeability, and targeting diseased BBB tissues which are customizable [47]. These are nano warriors which enhance the stability of the drug and increase blood circulation and infiltration within the infarct area. They are developing various types of nanocarriers, which are polymer-based nanoparticles, lipid-based systems such as liposomes, and carbon-based nanomaterials. The techniques to improve brain targeting include cell membrane use or surface modification with particular molecules. Even the intranasal delivery is coming up as a non-invasive mode of getting through the BBB[57]. In this method, several therapeutic agents can be delivered concomitantly with the intent to achieve synergistic effects, but clinical translation issues, as well as sufficient safety assessments, are still a problem[58].
7.5 Neurorestorative and Neurodegenerative Agents
Neurorestorative and neurodegenerative agents are key emerging therapies that have a goal of repairing and supporting functional recovery of brain damage after a stroke. Neural repair, which is different to neuroprotection is concerned with restoring damaged tissue and several animal models have investigated how to induce the process of neurogenesis and neuronal repair[59]. The leading area is the stem cell therapies. Mesenchymal stem cells and multilineage differentiating stress-enduring cells have been demonstrated to be promising under different types of stem cells. These cells are able to engraft into injured tissue, differentiate to restore functionality, induce neurogenesis, reorganize neural networks and increase axonal growth and synaptogenesis. They have therapeutic advantages, in that, they provide tissue regeneration and repair by means of their capability of self-renewal and multilineage differentiation. Moreover, the Chinese traditional herbal medicines are also being studied as neurorestorative. As an example, neuroprotective and neurorestorative effects of some herbal compounds and extracts have been demonstrated in preclinical stroke models of MLC901. These agents tend to operate by the stimulation of pathways such as the HIF-1: VEGF signaling pathway that play a significant role in enhancing angiogenesis and brain improvement of neurological functions and cerebral microvasculature networks, thus contributing to the recovery of stroke[60].
Table 2 : Emerging Anti-Stroke Therapies
|
Therapy |
Mechanism |
Current Status |
|
Stem Cells |
Neuroregeneration |
Phase I–II trials |
|
Gene Therapy |
Gene regulation |
Preclinical |
|
miRNA Therapy |
RNA modulation |
Experimental |
|
Mitochondrial Therapy |
Restore ATP production |
Experimental |
|
Nanotechnology |
Targeted drug delivery |
Early clinical development |
|
Cerebral Organoids |
Brain tissue regeneration |
Preclinical |
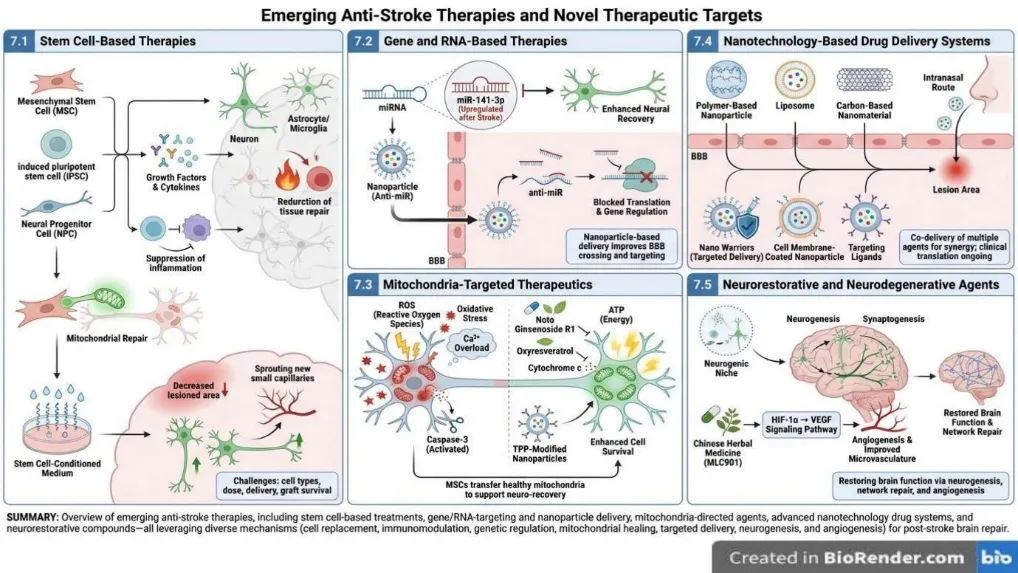
Figure 3: Diagram illustrating emerging anti-stroke therapies and novel therapeutic targets, divided into five sections: stem cell-based therapies, gene and RNA-based therapies, mitochondria-targeted therapeutics, nanotechnology-based drug delivery systems, and neurorestorative and neurodegenerative agents. Each section includes labeled illustrations of biological processes, therapeutic mechanisms, and delivery methods, highlighting key elements such as mitochondrial repair, miRNA regulation, nanoparticle carriers, and neurogenesis stimulation.
8. Challenges and Limitations in Current Anti-Stroke Therapy
The existing anti-stroke treatment options have a number of major challenges and drawbacks, which limit their efficacy and general use. In the case of acute ischemic stroke, the alteplase, the leading thrombolytic agent, has a limited therapeutic time, contraindications, and possible complication, and only a small percentage of patients undergo such therapy. Despite the combination of intravenous thrombolysis with endovascular thrombectomy, a good number of patients remain functionally dependent or disabled through delayed/incomplete recanalization, or microthrombin[61]. In addition, the endovascular thrombectomy may be unavailable in some areas. In new treatment interventions such as transplanting stem cells, the main issues involve determining the best cell type, dosage, and timing of various stroke subtypes, and the survival, integration, and differentiation of transplanted cells in the hostile microenvironment of the brain. The possibility of tumour formation, immune response, and formation of ectopic tissues also should be thoroughly evaluated[62]. The prospects of nanotechnology-based drug delivery systems have challenges in the quality control and mass production, as there is a complicated approach to engineering. Nanocarriers that should be made to have simplified structures are preferred in high stroke-targeting in order to address the problem that concerns reproducibility and cost-effectiveness. Also, most synthesized nanoparticles do not have comprehensive safety studies involving in-depth toxicity tests, biocompatibility, and long-term stability tests[63]. Moreover, the majority of intravenous nano therapies are likely to be deposited in non-target organs, and thus more effective brain-targeting technologies are necessary. In the case of natural compounds, although they have potential, most of the studies are preclinical and cannot be definitively confirmed of their effect and safety due to lack of large-scale randomized controlled clinical trials. The mechanisms, best administration routes, pharmacokinetics, bioavailability, which are long term effectiveness, possible drug interactions, and side effects are not well known. In general, new, safer, and more effective stroke treatment is urgently needed[7].
Table 3 : Challenges and Future Opportunities
|
Challenge |
Impact |
Future Solution |
|
Narrow thrombolytic window |
Low eligibility |
Extended-window therapies |
|
BBB penetration |
Poor drug delivery |
Nanocarriers |
|
Stem cell survival |
Reduced efficacy |
Biomaterial scaffolds |
|
Clinical translation |
Trial failures |
Better models |
|
Safety concerns |
Delayed approval |
Long-term monitoring |
The future of anti-stroke treatment requires researchers to develop new more effective more safe treatment because of the pressing need to overcome the drawbacks of the existing treatment. Much attention will be paid to enhancing the translation of promising preclinical results into the effective clinical application, which has been an obstacle in the past hindering progress. In higher-order treatment, such as stem cell therapy, the primary challenges have been to optimize the cell types, dosages and routes of delivery in addition to the long-term survival, integration and differentiation of transplanted cells in the complex brain microenvironment. Although nanoparticles have been found to be beneficial in drug loading, delivery, and the blood-brain barrier, in nanotechnology-based drug delivery, the next step to optimize brain-targeting methods and combat the challenges of quality control and mass production are necessary. In addition, a whole set of safety investigations, including detailed toxicity analyses, biocompatibility, and long-term stability assessments is necessary with newly developed nano therapies. In the case of natural compounds, a further crucial step to undertake is large-scale randomized controlled clinical trials to strictly test their effectiveness and safety, and to understand their mechanisms of action, pharmacokinetics, and possible drug-to-drug interactions.
CONCLUSION
Stroke is one of the acute health emergencies and one of the most critical in the world causing the severe and irreparable neurological damage. Ischemic and haemorrhagic strokes are both conditions which leave the brain tissue without the needed oxygen and glucose which leads to massive destruction of neurons. Although improved treatment methods, especially concerning ischemic stroke, have been made, there is still a pursuit of more efficient and safer anti-stroke medications. The pressing necessity is the constant research and the discovery of new neurotherapeutic agents and the most optimal treatment approaches to alleviate the serious effects of stroke.
REFERENCES










Himanshu Roy, Md Sayeed Anwar, Md. Musab Sufiyan, Sushil Raj, Khushi Gupta, Piyush Ranjan, Robin Singh, Sonu, Lakshyadeep Choudhary, Shyam lal Yadav, Anti-Stroke Agents: Current Therapeutic Strategies, Emerging Neuroprotective Approaches, and Future Perspectives in Stroke Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1932-1948, https://doi.org/10.5281/zenodo.20592311
 10.5281/zenodo.20592311
10.5281/zenodo.20592311