
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
S.C.S College of Pharmacy, Harapanahalli, Karnataka, India
Background: Surgical antibiotic prophylaxis (SAP) is an important strategy for preventing surgical site infections in orthopedic procedures. Appropriate antibiotic selection, timing and duration are essential for reducing postoperative infections while minimizing antimicrobial resistance. However, deviations from recommended prophylactic guidelines remain common in many healthcare settings. Objective: To evaluate surgical antibiotic prophylaxis practices, antibiotic utilization patterns and adherence to established prophylactic guidelines among patients undergoing orthopedic surgery in a tertiary care teaching hospital. Materials and Methods: We conducted a six-month observational study in the Orthopedics Department at Chigateri District Hospital in Davangere. We included 200 patients who received antibiotic prophylaxis. We collected and analyzed data on demographics, orthopedic conditions, surgical procedures, antibiotic use, route of administration, duration of therapy and compliance with guidelines using descriptive statistics. Results: Among the study population, 64.5% were male and 35.5% were female. Lower limb fractures were the most common orthopedic condition (52.45%), and ORIF was the most frequently performed surgical procedure (41.70%). The most commonly prescribed pre-operative antibiotic was Ceftriaxone (76%), while cephalosporins were the predominant class of antibiotic used (45.94%). Intravenous administration accounted for 90.41% of the prescriptions. Triple antibiotic therapy was prescribed in 45.5% of patients. Guideline adherence was observed in only 19% of cases, whereas 81% of the prescriptions were noncompliant. Conclusion: The study shows considerable variation from the recommended surgical antibiotic prophylaxis guidelines, particularly regarding antibiotic selection and prescribing patterns. The high rate of non-compliance highlights the need for antimicrobial stewardship initiatives, regular prescription audits and improved adherence to evidence-based guidelines to promote rational antibiotic use and orthopedic surgical practice.
Surgical wound infection is one of the most common healthcare-associated infections (HAIs). A World Health Organization (WHO) survey reported that the incidence of surgical wound infections worldwide ranges from 5% to 15% (World Health Organization, 2015). Several studies have identified many risk factors that cause surgical wound infections, such as diabetes, smoking habits, systemic use of steroids, obesity, old age, poor nutritional status, infections at poorly vascularized wound sites, or colonization. All orthopedic surgical procedures carry a risk of infection. Thus, preoperative and post-operative antibiotics are standard in implant installation procedures, implant removal procedures, and other major surgeries that require blood or are expected to involve significant blood loss. Providing appropriate antibiotics based on bacterial patterns or empirical research is important in reducing the risk of surgical wound infections. Therefore, the administration of antibiotics for surgical procedures should ideally follow guidelines for prophylactic antibiotics or local guidelines based on hospital bacterial patterns.1
Increased infection rates have been reported within certain high-risk groups: for example, the infection rate in patients with open fractures may exceed 30%, in comparison with 0.5-2% for equivalent closed fractures. Similarly, the infection rate for revision of failed prosthetic joints may be up to 40%, whereas the rate for primary joint replacement is approximately 1-4%.2
The primary purpose and benefit of SAP is to prevent SSIs and, subsequently, the impact thereof on the patient and healthcare system. The appropriate use of SAP is founded on evidence-based research describing the correct SAP indication, antibiotic choice, route of administration, antibiotic dosing and re-dosing, administration time and duration.
The efficacy of SAP is based on the ability of the antibiotic to inhibit bacterial growth at the surgical site, enabling the host’s immune mechanism to prevent infections. SAP in orthopedic procedures is indicated for clean-contaminated, contaminated and dirty surgical wounds as they have an increased risk of SSIs. Intravenous (IV) administration of SAP will ensure a rapid onset of action with adequate antibiotic blood and tissue concentrations.3
The current widespread use of cephalosporins in order to reduce the incidence of wound and soft tissue infections as well as infections around orthopedic implants following orthopedic operations was well established in many clinical trials that clearly demonstrated their effectiveness in reducing infections. The current recommendations are to administer intravenously a first or a second-generation cephalosporin enough time before surgery in order to achieve serum and tissue bactericidal levels when the incision is made. Cefazolin is the most frequently used agent, whereas allergic patients receive clindamycin or vancomycin.4
The present study was conducted to evaluate antibiotic prophylaxis practices among orthopedic surgical patients and assess adherence to standard prophylactic guidelines. The findings may provide valuable evidence for healthcare professionals and policymakers in developing strategies to promote rational antibiotic use, improve patient outcomes, reduce antimicrobial resistance, and minimize unnecessary healthcare expenditures.
OBJECTIVES
Primary Objective
Secondary Objectives
MATERIALS AND METHODS
Study Design
A hospital-based prospective observational study was conducted to evaluate Surgical antibiotic prophylaxis practices among patients admitted to the Orthopedics Department of a tertiary care teaching hospital.
Study Site
The study was carried out in the Department of Orthopedics at Chigateri District Hospital, Davangere, Karnataka, India.
Study Duration
The study was carried out over a period of six months.
Study Population
A total of 200 patients admitted to the Orthopedics Department who received antibiotic prophylaxis during the study period were included in the study.
Sample Size
A total of 200 patients were included in the study.
Inclusion Criteria
All hospital in-patients who received antibiotics in the orthopedic ward during the study period, irrespective of age or sex.
Exclusion Criteria
Data Collection
Patient data were collected using a structured data collection form from inpatient medical records. Data collected included patient demographic characteristics, diagnosis, co-morbidities, surgical procedures, antibiotic utilization patterns, route of administration, duration of therapy, and adherence to prophylactic antibiotic guidelines.
Statistical Analysis
The collected data were entered into Microsoft Excel and analyzed using descriptive statistical methods. Results were expressed as frequencies and percentages.
RESULTS
A total of 200 orthopedic patients receiving antibiotic therapy were included in the study.
1. Demographic Characteristics
Out of the 200 patients included, 129 (64.5%) patients were male and 71 (35.5%) were female. The largest proportion of patients belonged to the 61–70 years age group (20.5%), followed by the 51–60 years age group (19.5%). The lowest representation was observed in the 0–10 years age group (2.5%).
Table 1: Gender-wise distribution
|
GENDER |
FREQUENCY |
PERCENTAGE (%) |
|
MALE |
129 |
64.5 |
|
FEMALE |
71 |
35.5 |
|
TOTAL |
N=200 |
100 |
Table 2: Age-wise distribution
|
AGE GROUP (YEARS) |
FREQUENCY |
PERCENTAGE (%) |
|
0-10 |
5 |
2.5 |
|
11-20 |
10 |
5 |
|
21-30 |
28 |
14 |
|
31-40 |
31 |
15.5 |
|
41-50 |
25 |
12.5 |
|
51-60 |
39 |
19.5 |
|
61-70 |
41 |
20.5 |
|
71-80 |
14 |
7 |
|
81-90 |
7 |
3.5 |
|
TOTAL |
N=200 |
100 |
2. Co-Morbidities
Most of the patients had no documented co-morbid conditions. Among patients with co-morbidities, cardiovascular disorders were the most common (23.28%), followed by endocrine and metabolic disorders (11.21%) and respiratory disorders (7.33%).
Table 3: Presence of co-morbidity
|
TYPES OF CO-MORBIDITY |
FREQUENCY |
PERCENTAGE (%) |
|
CARDIOVASCULAR CONDITIONS |
54 |
23.275 |
|
ENDOCRINE AND METABOLIC CONDITIONS |
26 |
11.206 |
|
RESPIRATORY CONDITIONS |
17 |
7.327 |
|
RENAL AND URINARY CONDITIONS |
11 |
4.741 |
|
NEUROLOGICAL DISORDERS |
6 |
2.586 |
|
HEPATIC DISORDERS |
5 |
2.155 |
|
HAEMATOLOGICAL DISORDERS |
1 |
0.431 |
|
WITHOUT CO-MORBIDITIES |
112 |
28.225 |
|
TOTAL |
N=232 |
100 |
3. Fracture Pattern
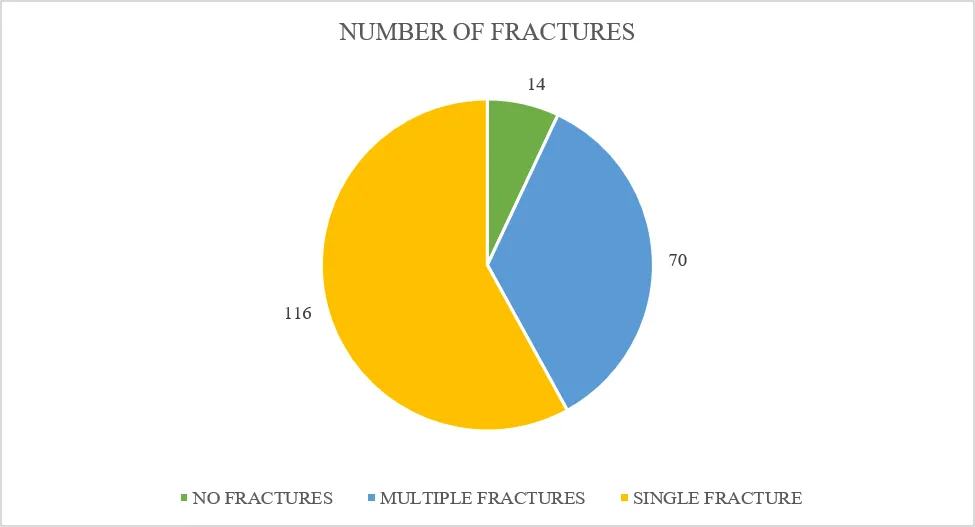
Lower limb fractures represented the most common orthopedic condition (52.45%), followed by upper limb fractures (32.87%). Single fractures were observed in 58% of patients, whereas multiple fractures were reported in 35% of patients.
Table 4: Types of fracture/ injury/ orthopedic condition
|
TYPES |
FREQUENCY |
PERCENTAGE |
|
UPPER LIMB FRACTURE |
94 |
32.867 |
|
LOWER LIMB FRACTURE |
150 |
52.447 |
|
OLD FRACTURES WITH IMPLANT IN-SITU |
12 |
4.195 |
|
INFECTED IMPLANTS |
9 |
3.146 |
|
LIGAMENT/ TENDON TEAR |
4 |
1.398 |
|
SPINE LISTHESIS/ COMPRESSION |
4 |
1.398 |
|
RIBS FRACTURE |
3 |
1.048 |
|
OSTEOARTHRITIS |
3 |
1.048 |
|
OSTEOMYELITIS |
3 |
1.048 |
|
OSTEOPOROSIS |
2 |
0.699 |
|
CTEV |
1 |
0.349 |
|
POLIOTIC LIMB |
1 |
0.349 |
|
TOTAL |
N=286 |
100 |
Table 5: Number of fractures
|
NUMBER OF FRACTURES |
FREQUENCY |
PERCENTAGE (%) |
|
NO FRACTURES |
14 |
7 |
|
MULTIPLE FRACTURES |
70 |
35 |
|
SINGLE FRACTURE |
116 |
58 |
|
TOTAL |
N=200 |
100 |
4. Surgical Procedures
Open Reduction and Internal Fixation (ORIF) was the most frequently performed surgical procedure (41.70%), followed by Closed Reduction and Internal Fixation (CRIF) (16.60%). Orthopedic implants and K-wires were used in 84% of patients.
Table 6: Type of surgery conducted
|
TYPE OF SURGERY |
FREQUENCY |
PERCENTAGE (%) |
|
ORIF |
98 |
41.702 |
|
CRIF |
39 |
16.595 |
|
OTHER PROCEDURES |
24 |
10.212 |
|
IMPLANT REMOVAL |
18 |
7.659 |
|
CRPF |
16 |
6.808 |
|
HIP HEMIARTHROPLASTY |
15 |
6.381 |
|
DEBRIDEMENT |
13 |
5.531 |
|
CREF |
11 |
4.680 |
|
ORPF |
1 |
0.425 |
|
TOTAL |
N=235 |
100 |
5. Antibiotic Utilization Pattern
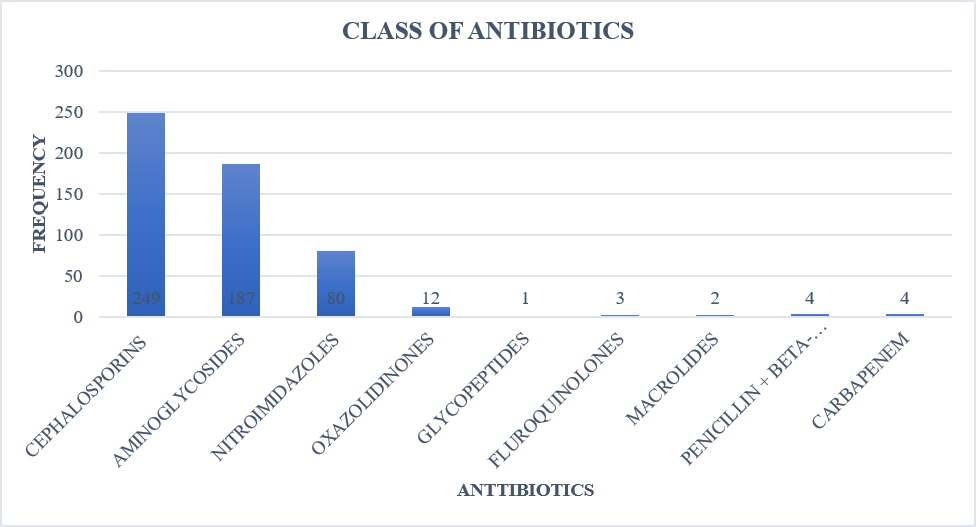
Ceftriaxone was the most frequently prescribed pre-operative antibiotic (76%), followed by piperacillin-tazobactam (13%). Intravenous administration was the predominant route of antibiotic delivery (90.41%). Overall, ceftriaxone (36.53%) was the most frequently utilized agent, followed by amikacin (33.21%) and metronidazole (14.76%). Cephalosporins represented the most commonly prescribed antibiotic class (45.94%), followed by aminoglycosides (34.50%) and nitroimidazoles (14.76%).
Table 7: Pre-operative antibiotic use
|
ANTIBIOTICS USED |
FREQUENCY |
PERCENTAGE (%) |
|
CEFTRIAXONE |
152 |
76 |
|
PIPZO |
26 |
13 |
|
CEFAZOLIN |
12 |
6 |
|
CEFUROXIME |
10 |
5 |
|
TOTAL |
N=200 |
100 |
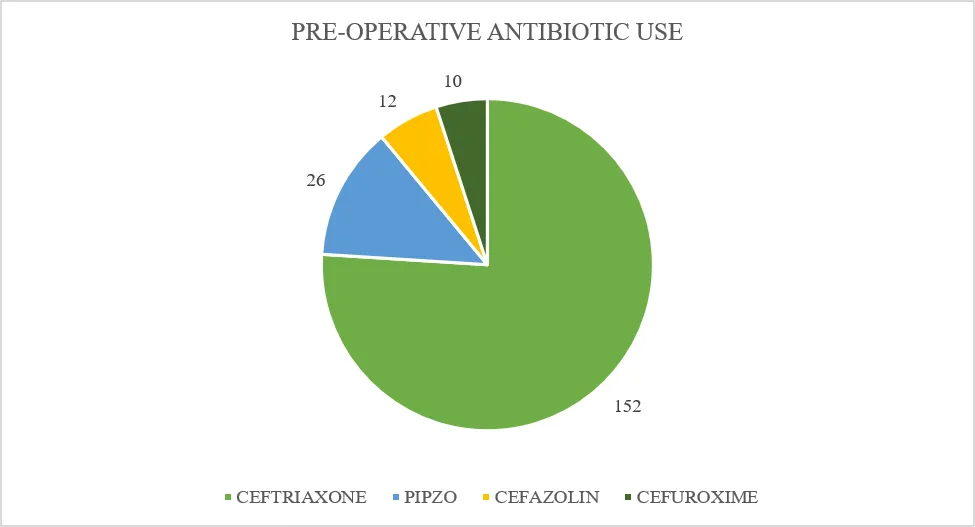
Table 8: Route of administration of antibiotics
|
ROUTE |
FREQUENCY |
PERCENTAGE (%) |
|
IV |
490 |
90.405 |
|
ORAL |
52 |
9.594 |
|
TOTAL |
N=542 |
100 |
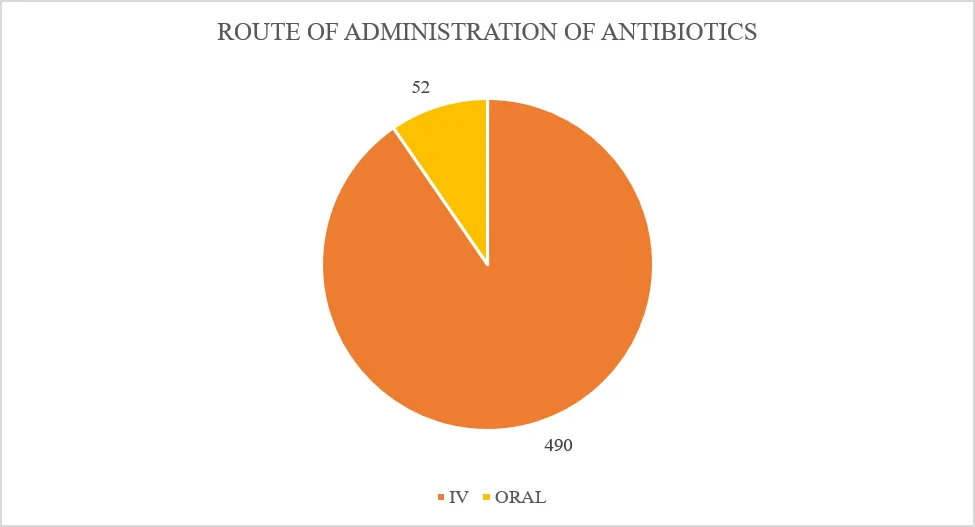
Table 9: Antibiotics used
|
ANTIBIOTICS USED |
FREQUENCY |
PERCENTAGE |
|
CEFTRIAXONE |
198 |
36.531 |
|
AMIKACIN |
180 |
33.210 |
|
METRONIDAZOLE |
80 |
14.760 |
|
CEFIXIME |
33 |
6.088 |
|
LINEZOLID |
12 |
2.214 |
|
GENTAMICIN |
7 |
1.291 |
|
CEFOTAXIME |
6 |
1.107 |
|
CEFAZOLIN |
5 |
0.922 |
|
CEFEPIME |
4 |
0.738 |
|
MEROPENEM |
4 |
0.738 |
|
CEFUROXIME |
3 |
0.553 |
|
CIPROFLOXACIN |
3 |
0.553 |
|
PIPERACILLIN + TAZOBACTAM |
3 |
0.553 |
|
AZITHROMYCIN |
2 |
0.369 |
|
AMOXICILLIN + CLAVULONIC ACID |
1 |
0.184 |
|
VANCOMYCIN |
1 |
0.184 |
|
TOTAL |
N=542 |
100 |
Table 10: Class of antibiotics used
|
CLASS OF ANTIBIOTICS |
FREQUENCY |
PERCENTAGE (%) |
|
CEPHALOSPORINS |
249 |
45.940 |
|
AMINOGLYCOSIDES |
187 |
34.501 |
|
NITROIMIDAZOLES |
80 |
14.760 |
|
OXAZOLIDINONES |
12 |
2.214 |
|
GLYCOPEPTIDES |
1 |
0.184 |
|
FLUOROQUINOLONES |
3 |
0.553 |
|
MACROLIDES |
2 |
0.369 |
|
PENICILLIN + BETA-LACTAMASE INHIBITOR |
4 |
0.738 |
|
CARBAPENEM |
4 |
0.738 |
|
TOTAL |
N=542 |
100 |
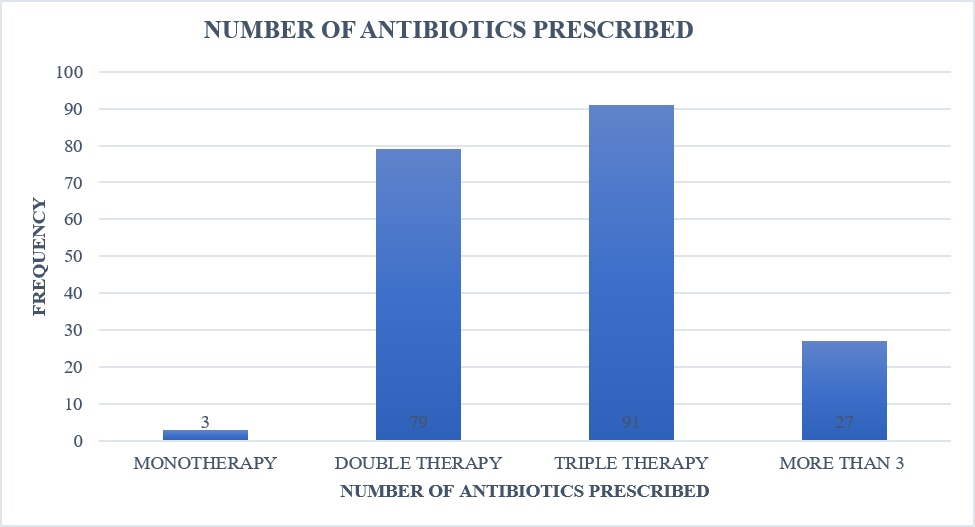
6. Number of Antibiotics Prescribed
Triple antibiotic therapy was prescribed in 45.5% of patients, while dual therapy was prescribed in 39.5% of patients. Monotherapy was observed in only 1.5% of cases.
Table 11: Number of antibiotics prescribed
|
NUMBER OF ANTIBIOTICS |
FREQUENCY |
PERCENTAGE (%) |
|
MONOTHERAPY |
3 |
1.5 |
|
DOUBLE THERAPY |
79 |
39.6 |
|
TRIPLE THERAPY |
91 |
45.5 |
|
MORE THAN 3 |
27 |
13.5 |
|
TOTAL |
N=200 |
100 |
7. Duration of Antibiotic Therapy
The majority of patients received antibiotics for 11–20 days (67.5%), followed by 0–10 days (29%). Only a small proportion of patients received therapy for more than 20 days.
Table 12: Duration of antibiotic therapy
|
DURATION (DAYS) |
FREQUENCY |
PERCENTAGE (%) |
|
0-10 |
58 |
29 |
|
11-20 |
135 |
67.5 |
|
21-30 |
4 |
2 |
|
31-40 |
3 |
1.5 |
|
TOTAL |
N=200 |
100 |
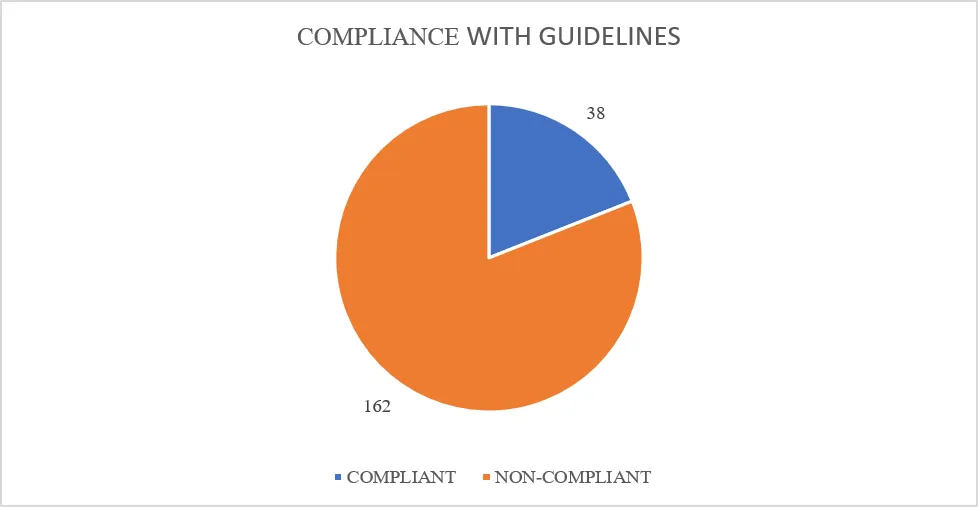
8. Compliance with Guidelines
Assessment of adherence to standard surgical antibiotic prophylaxis guidelines showed that only 38 prescriptions (19%) were compliant whereas 162 prescriptions (81%) were non-compliant.
Table 13: Compliance with guidelines
|
COMPLIANCE STATUS |
FREQUENCY |
PERCENTAGE (%) |
|
COMPLIANT |
38 |
19 |
|
NON-COMPLIANT |
162 |
81 |
|
TOTAL |
N=200 |
100 |
DISCUSSION
This study evaluated surgical antibiotic prophylaxis practices among orthopedic surgical patients in a tertiary care teaching hospital with particular emphasis on prescribing patterns and adherence to standard prophylactic guidelines. Although prophylactic antibiotics were routinely prescribed, compliance with guideline recommendations was low, indicating opportunities to improve antibiotic stewardship and promote evidence-based prescribing practices.
Male patients constituted nearly two-thirds of the study population. This may reflect the greater exposure of men to occupational injuries, road traffic accidents and other trauma-related events that frequently require orthopedic intervention This male predominance is consistent with findings reported by Argaw et al.,5 who observed that 72% of orthopedic surgical patients were male.
Most of the patients belonged to the older age groups particularly 61-70 years. Increasing age is associated with osteoporosis, reduced bone mineral density, impaired balance and a greater risk of fractures, which may explain the higher number of orthopedic procedures observed in this population. This finding is consistent with previous findings such as the study done by Radji et al.,6 who observed that 58.9% of cases took place among patients aged 26-65 years.
In terms of co-morbidities, it was seen that the most common co-morbidity associated with orthopedic inpatients was cardiovascular disorders, followed by endocrine and metabolic disorders and respiratory diseases. Co-morbid conditions seen commonly included hypertension and diabetes mellitus. These findings have also been shown previously by Masalma et al.,7 in their study, where they found hypertension, diabetes mellitus, and chronic heart disease as some of the prevalent co-morbid conditions among orthopedic inpatients.
Lower limb fractures were found to be the highest among orthopedic conditions (52.45%), followed by upper limb fractures (32.87%). These findings align with previous orthopedic epidemiological studies conducted by Setiawati et al.,8 which have reported lower limb fractures as the most common indication for surgical intervention. Single fractures were found in 58% of the subjects, whereas multiple fractures were identified in 35% of patients, implying an immense number of trauma-related injuries.
Open Reduction and Internal Fixation (ORIF) was found to be the most frequently performed surgical procedure (41.70%), followed by Closed Reduction and Internal Fixation (CRIF) (16.60%). The above results corroborate the previous studies of Gupta and Wadhwa,9 who reported ORIF as the most common orthopedic surgical procedure. The reason for this may be the high number of fracture cases, where internal fixation is needed.
A large percentage of the surgeries (84%) involved the use of implants and K-wires. Most patients received intravenous ceftriaxone as pre-operative prophylaxis. Hasler et al.,10 reported that 40% of patients undergoing implant-related procedures received intravenous cefuroxime before surgery. These findings mark the importance of appropriate perioperative antibiotic prophylaxis which helps reduce the risk of surgical site infections associated with orthopedic implants.
Ceftriaxone (76%) was the most frequently used pre-operative antibiotic in the present study, followed by piperacillin-tazobactam (13%) and cefazolin (6%). Post-operative antibiotic prophylaxis that was most commonly used involved ceftriaxone (36.531%), amikacin (33.210%), and metronidazole (14.760%). Cephalosporins and aminoglycosides were the predominant class of antibiotic prescribed. Similar results have been reported by Mistry et al.,11 who observed ceftriaxone (80.98%) as the preferred antibiotic for pre-operative prophylaxis, while ceftriaxone and amikacin were frequently utilized during post-operative management. Cephalosporins and aminoglycosides (89.93%) constituted the most commonly prescribed antibiotic classes in their study.
Ceftriaxone was the most frequently prescribed prophylactic antibiotic in the present study despite international guidelines commonly recommending cefazolin for clean orthopedic procedures. This prescribing pattern may reflect institutional protocols, local antimicrobial susceptibility patterns, drug availability, clinical preference or concerns regarding broader antimicrobial coverage. However, the routine use of broad-spectrum antibiotics when narrow-spectrum agents are appropriate may contribute to antimicrobial resistance and increased healthcare costs.
However, the study done by Mistry et al.,11 also showed that there was more use of intravenous antibiotics (96.40%) as part of their surgical prophylaxis while there was less use of oral antibiotics. This is similar to what was found in the current study since there was more use of intravenous antibiotics which was 90.405% compared to oral antibiotics, which were 9.594%. This reflects the preference for parenteral administration in perioperative management to achieve rapid and adequate tissue concentrations.
Nearly half of the patients received triple antibiotic therapy. While combination therapy may be justified in selected high risk or contaminated surgical procedures, its routine use in prophylaxis is generally not recommended by established guidelines. Excessive use of multiple antibiotics increases treatment cost, exposes patients to unnecessary adverse effects and may accelerate the emergence of antimicrobial resistance. Triple antibiotic therapy accounted for 45.5% of prescriptions, followed by dual antibiotic therapy in 39.5% of patients. Similar findings were reported by Gans et al.,12 who observed the use of multiple-dose antibiotic regimens in 59% of patients, whereas only 39% received single-dose therapy.
The rational use of antimicrobials was assessed using WHO and ICMR guidelines. The most important observation made in this study was the low rate of compliance with standard surgical antibiotic prophylaxis guidelines. Only 19% of the prescriptions fulfilled the requirements stipulated by the guideline. This means that there is a deviation between the current practice and the recommended evidence-based practice. This might be due to a number of reasons including lack of institutional policies, lack of consistent knowledge of the existing guidelines, limited antimicrobial stewardship and variation in the prescriber’s practice. All these aspects could be solved by performing prescription audits and education programs. Similar findings were reported by Anand et al.,13 who observed that 73.07% of antibiotic prescriptions failed to comply with established guidelines.
The prevalence of noncompliance noted in this current study underscores the need for the urgent implementation of an antimicrobial stewardship program in orthopedic departments. Prescription audits, prophylaxis protocol development for each institution, continuous education programs, and a multidisciplinary approach to antimicrobial stewardship can be very helpful in promoting rational antibiotic use and prescribing practices.
In general, the results of the current study highlight the significance of improving the practice of antibiotic prophylaxis in orthopedics. It can be seen from the results obtained that even though antibiotic prophylaxis is used on a routine basis, much still needs to be done to achieve the optimum. Strengthening antimicrobials stewardship programs and promoting evidence based prescribing practices are essential to improve patient outcomes while minimizing the development of antimicrobial resistance. Appropriate antibiotic selection, timing, route of administration, and duration of therapy are essential to maximize patient benefit while minimizing the risks associated with antimicrobial overuse.
CONCLUSION
This prospective observational study evaluated surgical antibiotic prophylaxis practices among orthopedic surgical patients in a tertiary care teaching hospital. Cephalosporins, particularly ceftriaxone was the most frequently prescribed prophylactic antibiotic and intravenous administration was the predominant route. Lower limb fractures were the most common orthopedic condition while ORIF was the most frequently performed surgical procedure. Combination antibiotic therapy especially triple drug therapy was commonly prescribed.
A key finding of this study was the low level of adherence to standard surgical antibiotic prophylaxis guidelines with only 19% of the prescriptions being compliant. This highlights considerable variation between the current prescribing practices and the evidence-based recommendations.
The results highlighted the significance of enhancing the effectiveness of antibiotic stewardship by way of conducting audits on prescriptions, having specific policies for antibiotics within hospitals, and educating health care practitioners. Adherence to established guidelines on surgical antibiotic prophylaxis may contribute to rational use of antibiotics and prevent the occurrence of antimicrobial resistance.
LIMITATIONS
ETHICAL APPROVAL
The study protocol was approved by the Institutional Ethics Committee of S.C.S College of Pharmacy, Harapanahalli, Karnataka, India, on 19 March 2024 prior to commencement of the study.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest related to this study.
FUNDING
The authors declare that no external funding was received for conducting this study.
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to the Department of Orthopedics, Chigateri District Hospital, Davangere, Karnataka, for providing permission and support to conduct the study. The authors also sincerely thank the principal and the Department of Pharmacy Practice, S.C.S College of Pharmacy, Harapanahalli, Karnataka, for their guidance, encouragement, and academic support throughout the study period.
The authors are grateful to all healthcare professionals, hospital staff, and patients whose cooperation contributed significantly to the successful completion of this study.
REFERENCES

J. S. Venkatesh, Adithi G, Aksa George, Amina Ameer, Anakha Shibu, Antibiotic Prophylaxis Practices in Orthopedic Surgery: A Prospective Observational Study from a Tertiary Care Teaching Hospital, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2600-2613. https://doi.org/10.5281/zenodo.21339985
 10.5281/zenodo.21339985
10.5281/zenodo.21339985