
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School Of Pharmacy, Desh Bhagat University, Mandi Gobindgarh, Punjab
Antibiotic resistance is a global health challenge. Antibiotics, disinfectants and bacteria resistant to them have been detected in environmental compartments such as waste water, surface water, ground water, sediments and soils. Antibiotics are released into the environment after their use in medicine, veterinary medicine and their employment as growth promoters in animal husbandry, fish farming and other fields. There is increasing concern about the growing resistance of pathogenic bacteria in the environment, and their ecotoxic effects. Increasingly, antibiotic resistance is seen as an ecological problem. This includes both the ecology of resistance genes and that of the resistant bacteria themselves. Little is known about the effects of subinhibitory concentrations of antibiotics and disinfectants on environmental bacteria, especially with respect to resistance. According to the present state of our knowledge, the impact on the frequency of resistance transfer by antibacterials present in the environment is questionable. The input of resistant bacteria into the environment seems to be an important source of resistance in the environment. The possible impact of resistant bacteria on the environment is not yet known. Antibiotic resistance is the biggest challenge to the medical profession in the treatment of infectious diseases. The wide range of occurrence of antibiotic resistance suggests that, in principle, any organism could develop resistance to any antibiotic. The phenomenon of horizontal gene transfer compounds the problem by facilitating rapid spread of antibiotic resistance. Unfortunately, the discovery and development of newer antibiotics have not kept pace with the emergence of antibiotic resistance.
Antibiotics are used extensively to prevent or to treat microbial infections in human and veterinary medicine. Apart from their use in aquaculture, they are also employed to promote more rapid growth of livestock. Most of the compounds used in medicine are only partially metabolized by patients and are then discharged into the hospital sewage system or directly into municipal waste water if used at home (1).
Along with excreta, they flow with municipal waste water to the sewage treatment plant (STP). They may pass through the sewage system and end up in the environment, mainly in the water compartment. Antibacterial substances used for livestock enter the environment when manure is applied to fields (2). These antibiotics may either end up in soil or sediment or in ground water. Antimicrobial agents are also used to treat infections in intensive fish farming where they are added directly to the water, resulting in high local concentrations in the water compartment and adjoining sediments (3). Some antibiotics such as streptomycins are used in fruit growing, others in bee-keeping. Disinfectants are widely used in the food and glue industries, medicine and livestock rearing. In addition to antimicrobials and disinfectants, resistant bacteria themselves are excreted by humans and animals and are emitted into sewage or manure and other environmental compartments (4). The use of antibiotics will inevitably eradicate bacterial infections in human and in some animals when administered correctly. Antibiotics serve as growth promoter additives in animal feed (5). Many antibiotics can be excreted via urine and faeces as unchanged and active species (6). The use of antibiotics in modern medicine has played a significant role in decreasing the spread of diseases, however, over prescription of the drug in the recent years has caused most strains to become resistance to treatment. An accelerated use of known antimicrobials for human, animals, and agriculture benefit revealed that regular and repeated use of antibiotics have negative implication to the environment and natural ecosystem (7).
Antimicrobial resistance (AMR) poses a serious global threat of growing concern to human, animal, and environment health. This is due to the emergence, spread, and persistence of multidrug-resistant (MDR) bacteria or “superbugs” (8).
The unwanted effects of microbial growth have long been controlled through use of antimicrobials. It has also long been recognized that susceptibility to such chemicals varies markedly between different groups of organisms and within these groups. The different mechanisms of action and the methods used to evaluate susceptibility are crucial for the results of susceptibility testing and the evaluation of resistance (9). A revolution in the health care sector was brought by the discovery of antibiotics that could treat microbial infections, thus saving lives worldwide; however, the community use of antibiotics far exceeds their nosocomial usage. For example, only 10% of the total antibiotic consumption in Europe was accounted for use in hospitals (10).
In the Asian region, China and India are significant contributors to the burden of antibiotics, and moreover, minimal guidelines are present in these countries for the use of antibiotics as growth promoters. These countries do not need a medical prescription for antibiotic application to be used as food for the animals (11). Once in the environment, antibiotic residues can have negative effects on biota at different trophic levels, and on human health – by consumption of contaminated food and water, by the contribution to increasing the resistant bacterial population and maintaining selective pressure that causes the development and/or dissemination of resistance in different compartments of the environment (12,13).
Besides the risk of favoring microbial antibiotic resistance, antibiotic residues can be absorbed by plants, interfering with physiological processes and causing potential ecotoxicological effects. In order to highlight the negative effects, numerous chronic and acute toxicity tests have been performed, which revealed the impact of antibiotics on photosynthesis (chloroplasts gene expression, and cell proliferation) and mitochondria (oxidative stress response in plants), probably explained by the bacterial origins of chloroplasts and mitochondria (14). Also, the concentrations of antibiotics which are found in agricultural soils could delay germination or reduce biomass, and consequently may negatively affect yield in farmland fertilized with contaminated manure (15). Moreover, antibiotic residues can alter the human microbiome and cause health disturbances, such as allergic reactions, chronic toxic effects after prolonged exposure, and disruption of digestive system functions (16).
Global antibiotic resistance shows no signs of decline, though it may perhaps shift direction. The etiology of antibiotic resistance is multifaceted, and its consequences pose an impact across the globe. Numerous attempts have been made to delineate the diverse aspects of antibiotic resistance and possible solutions required to deal with this global challenge have been tried. However, a principally coordinated campaign is lacking, particularly at the political level worldwide (17)
Although antibiotics have been applied in large quantities for some decades, until recently the existence of these substances in the environment was accorded very little attention. Studies conducted in various countries have detected a number of antibiotics in the low microgram per litre or the nanogram per litre (Table 1) range in different environmental compartments, i.e. hospital effluent, municipal waste water, effluent from sewage treatment plants, surface water and in some cases ground water (4). The compounds detected are from different important antibiotic classes such as macrolides, tetracyclines, sulphonamides, quinolones and others as far as analytical methods are available. b-Lactams have not been detected yet despite the fact that b-lactams are used in the highest amounts (18). Obviously, most of the antibiotics are not fully eliminated during the sewage purification process. The results of investigations using test systems indicate that a number of antibiotics and disinfectants are not biodegradable in the aquatic environment (19,20). In soil, tetracycline concentrations in the range of several hundred micrograms per kilogram have been detected some months after manure application (21,22). The antibiotic discharges from the pharmaceutical industry release higher concentrations in specific locations at certain times than other pollution sources and can pose a significant ecological and public health concern. These situations are particular, because there is no metabolism phase involved, which leads to higher levels of antibiotics in the wastewater systems (23,24). Moreover, the environmental risk assessment required in the registration procedure for new pharmaceuticals in Europe and USA does not take into account emissions from manufacturing (25). Voluntarily, several pharmaceutical companies have committed themselves to reducing effluent concentrations from their factories waste waters. Towards this purpose, several leading pharmaceutical companies signed an antimicrobial-resistance roadmap having the environmental management of antibiotic-related production as a central objective theme (26).
Table 1. Concentrations (ng/L) of antibiotics and disinfectants measured in the aqueous environment (1-4)
|
Class |
Compound |
Hospital effluent |
Sewage water |
Surface water |
Ground water |
|
Penicillin |
ampicillin |
up to 80 |
|
|
|
|
Tetracyclines a |
|
1 |
|
|
|
|
Macrolides |
erythromycin–H2O (metabolite) |
|
up to 6.0 |
0.1–1.7 |
0.05 |
|
|
clarithromycin and roxithromycin |
|
<1.0 |
0.1–0.6 |
0.03 |
|
Quinolones |
ciprofloxacin |
|
up to 124.5 |
0.4 |
0.1 |
|
Sulphonamides a |
sulfamethoxazole |
|
up to 1.0 |
0.1–0.2 |
0.4 |
|
|
trimethoprim and others |
|
<0.2 |
up to 0.03 |
|
|
Disinfectants |
quaternary ammonium compounds |
up to 5000 |
|
|
|
Apart from the issue of resistance, it has to be kept in mind that bacteria form one of the most important groups of organisms in soil and in other environmental compartments as well as in natural or technical sewage treatment (27). Without bacteria, water would not be clarified. Bacteria are essential for the closing of nutrient and geochemical cycles such as the carbon, nitrogen, sulphur and phosphorous cycle. Without bacteria, soil would not be fertile and organic matter such as straw or leaves would accumulate within a short time (28). In soil, naturally occurring antibiotics from bacteria and fungi amongst others control the dynamics of bacterial populations (29). In contrast to these, most of the compounds used nowadays are semi-synthetic or synthetic. They are often much more stable and are not biodegradable by bacteria. They may therefore persist in the environment. Furthermore, they often have a different, e.g. broader, activity spectrum. (29,30)
2.2) Antimicrobial resistance in the environment
Quantitative analyses of ARGs, resistant bacteria and selective agents in environmental samples differ in terms of how informative data are for assessing risks for evolution or transmission, or as a reflection of the regional clinical resistance situation. These distinct objectives are also best informed by analyses of different environmental matrices, as outlined recently (31). Most bacterial species do not cause disease and are not associated with clinical breakpoint concentrations. Accordingly, environmental microbiologists most often define ‘resistance’ as a decreased susceptibility to an antibiotic compared with other strains of the same species. As most species of environmental bacteria are difficult to culture with standard methods (32), environmental microbiologists, more often so than clinical microbiologists, also tend to study ARGs rather than resistant bacteria. It is important to appreciate the differences, particularly because the genetic context and host of the detected ARGs in most instances remain unknown.
According to Murray, the transfer as well as the emergence of new combinations of resistance genes will happen most frequently in compartments with high bacterial density, i.e. biofilms. Such biofilms are not only found in a medical context. Bacterial density is very high both in aerobic and anaerobic septic tanks of sewage treatment works, and in biofilms, e.g. in drinking water pipes, in sediments, and soils. Biofilms are no taxonomic barrier to this horizontal genetic transfer. Bacteria are either resistant by nature or they may have become resistant by the use of antibiotics as well as in the environment by uptake of genetic material encoding resistance (e.g. in hospital effluent or manure) before they reach a sewage treatment plant or the soil (33). The culture-independent techniques allow functional and structural characterization of microbial communities and enhance understanding of evolutionary pathways of ARGs spread in the environment (34). The ARGs are “easy to get, hard to lose” pollutants as they prevail in antibiotic-free environments or when even the selective pressure has been removed (35).
3) Identification of resistance and resistant bacteria in the environment
It has been known for quite some time that cultivable bacteria represent only a small portion of the vast number of bacteria present in the environment and that the number that can be enumerated is higher than can be cultivated. The known and cultivable environmental bacteria add up to only 5–10% of the total number assumed to be present in waste water and waste water treatment plants (36).
Environmental analyses of antibiotics advanced greatly in the past few decades; however, it can be challenging to accurately identify and quantify antibiotics that often occur at nanogram per litre levels in complex matrices (37,38). The concentrations of antibiotics and other pharmaceuticals in sewage are usually reasonably stable over time, but can show diurnal patterns (39). Emissions from production are often much more erratic and considerably more difficult to predict. This irregular discharge pattern was used in a recent study to attribute a large portion of various drugs found in a Swiss river to industrial emissions (40).
4) Sources of antibiotics and resistance in the environment
4.1) Municipal sewage and hospital waste
The antibiotics are discharged from the human body via routes of urinary and/or biliary system in faeces and urine in the form of antibiotic metabolites, glucuronic and sulfuric acid conjugates, or as parent compounds (41, 42, 43). Approximately 70–80% of antibiotic molecules present in sewage are in consistent forms (44). Hospital waste is also channelled into the municipal sewage system because most hospitals do not have on-site WWTP (45). In European countries, 75% of antibiotics in municipal sewage are contributed by households, and only 5–20% is contributed by hospitals (46). Municipal wastewater is reported to contain from around 100–1000 ng/L of antibiotics (47). Sulfamethoxazole, trimethoprim, ciprofloxacin, and ofloxacin are dominantly present in municipal wastewater (48, 49). On the contrary, βlactams, macrolides, fluoroquinolones, sulphonamides, trimethoprim, and lincomycin are frequently detected in effluents of the hospital with the rate of detection up to 35,500 ng/L (50). The unused/expired drugs are directly disposed of in the sewage system or landfills (51).
The prevalence of bacteria with reduced susceptibility to benzalkonium chloride was elevated in the effluent of a municipal STP (52). A strong selecting effect of benzalkonium chloride was found in biodegradability testing (53,54). In such tests, the benzalkonium chloride concentration was at least 100-fold higher than in hospital effluents or municipal sewage. Benzalkonium chloride and other quaternary ammonium compounds are sorbed by sewage sludge whereas pyridinium salts are not (55).
4.2) Input of resistant bacteria into municipal sewage
The input into and the elimination of resistant bacteria in three different sewage treatment plants (a municipal one and two located in the countryside) were monitored. It is often assumed that hospitals are the most important source for the input of resistant bacteria into municipal waste water. The numbers of resistant bacteria found in the effluent of an intensive care unit (ICU) of a hospital with maximum medical service spectrum were in the same range as those found for the influent of municipal STPs. The numbers and types of resistant bacteria found in the effluent of the ICU of the hospital offering maximum medical service showed that the number in the ICU effluent and in the influent of the STP are in the same range (56). Taking into consideration that the dilution of hospital effluent by municipal sewage is normally more than 100-fold, (57) and that in municipal sewage without hospital effluent resistant bacteria are also present (56) because of the use of antibiotics at home, the conclusion is that it is probably the general community which is responsible for the main input of resistant bacteria into STPs. Another point is that in Germany for example only one-quarter of the total consumption of antibiotics can be attributed to hospitals (57).
It is assumed that multi-resistant bacteria are selected mainly in hospitals and passed into waste water (58) The number of multi-resistant bacteria in sewage correlated with the size and the number of hospitals connected to an STP.
4.3) Surface water
Concentrations of antibiotics in surface waters, i.e. in rivers and lakes, are in the low microgram per litre range for most compounds (see in Table 1). In a study using ciprofloxacin and ceftazidime, it was concluded that the average concentrations of these compounds actually found in surface water will be clearly below concentrations able to change bacterial populations (59). This was monitored by classical microbiological methods such as Gram-staining, aminopeptidase and catalase test as well as metabolic fingerprints using the Bio log system. However, some restrictions imposed by the methodology have to be taken into account in this study.
Bacteria resistant to antibiotics are present in surface water. Goni-Urizza et al. found a correlation between resistant bacteria in rivers and urban water input. Schwartz et al. were able to amplify AmpC β-lactamase gene sequences by PCR in surface water. Genetic transformations have for instance been reported for E. coli. (60,62) Antimicrobial resistance was also found in marine bacteria and bacteria living in estuaries. Gentamicin resistance genes were found in Acinetobacter, Pseudomonas, Enterobacteriaceae, and in phylogenetically distant bacteria such as members of alpha and beta proteobacteria in coastal water polluted with sewage water (63,65).
4.4) Ground water
Antibiotics are rarely found in ground water and if they do occur, they are far below the microgram per litre range (Table 1). Leaching from fields fertilized with animal slurry or passing through sediments into the ground water might be a source of antibiotics in ground water. However, the volume load of antibacterial agents in ground water in rural areas with high concentrations of livestock has proved to be small (66). Antibiotic-resistant E. coli have been found with a surprisingly high incidence in rural ground water (64). The authors do not speculate much on the origin of this resistance but manure runoff from farms or leakage from septic tanks are clear possibilities for the input of resistant bacteria into ground water as well as broken sewage pipes.
4.5) Drinking water
Antibiotic-resistant bacteria were detected in drinking water as early as the 1980s and later in the 1990s. These authors found that resistant bacteria identified using classical microbiological methods, i.e. standard plate counting, occurred within the distribution network of drinking water supply systems. They concluded that the treatment of raw water and its subsequent distribution selects for antibiotic-resistant bacteria. In agreement with these data, increased phenotypic resistance rates were also detected at the drinking water sampling points in the study by (60,66). These are also found vanA and ampC genes in heterotrophic bacteria in drinking water biofilms.
4.6) Sediments
Resistant bacteria may be present because of the application of antibiotics in fish or because of selection by the antibiotics present in sediments. High antibiotic load in sediments in concentrations sufficiently potent to inhibit the growth of bacteria were reported for aquaculture. The fact that the exposure is highly locally concentrated has to be considered critical. The substances used in fish farming can enter sediments directly from the water without undergoing any kind of purification process. Some investigations have demonstrated the presence and persistence of antibiotics applied extensively in fish farming in sediments beneath fish farms (67–72).
Quinolones, sulphonamides and tetracyclines are sorbed by organic matter. Therefore, they can accumulate. It is not yet known to what degree and under what circumstances the compounds are effective after sorption or whether they are released and may contribute to resistance. Antimicrobials may have qualitative and quantitative effects upon the resident microbial community of the sediments (73).
4.7) Soil
Antibiotics used for veterinary purposes or as growth promoters are excreted by the animals and end up in manure as well as in disinfectants used in livestock. The manure is applied to agricultural land as a fertilizer. If antibiotics are used in animal husbandry, they pass from manure into the soil. Tetracyclines have been detected in soil in concentrations up to 0.3 mg/kg (74). Sulfachloropyridazine is not sorbed very much. Compounds from different antibiotic groups such as virginiamycin, sarafloxacin, tetracycline, oxytetracycline, chlortetracycline and cyclosporine A were only slowly biodegraded in soils (75,76). Tylosin disappeared soon after the application of manure (77). The spread of resistant bacteria and resistance genes by manure and sewage sludge used as fertilizer in agriculture or for land amendment has not been sufficiently investigated so far. Furthermore, antibiotics occur naturally in soils. Resistance against these antibiotics plays an important role in the population dynamics in soils. Antibiotics are a natural mechanism used by microbes in their natural ecology. The dynamics of soil microbiology and antibiotics has played out for millions of years. The abundance of natural antibiotics seems to be low on average and to be restricted to the nearest surroundings, i.e. the microenvironment of the bacteria. Tetracycline, for example, is produced by bacteria occurring naturally in soils. To the author’s best knowledge, there are no findings of tetracycline in soils which had not been fertilized with manure containing tetracycline. In soils used as control when studying the input and fate of tetracycline in soils, tetracycline concentration was always below the detection limit (74). At European level, but also globally, in regards to soil, underground waters and wastewaters contamination, there is an absence of strict regulations on how to monitor the antibiotic concentration in the environment, to investigate the environmental fate of these compounds and the transmission of monitoring data (data transmission network) and to assess the environmental risk of antibiotics. This legislative permissiveness and inexistence of specific regulations could be partially explained by the lack of consensus on safe environmental concentrations of antibiotic residues in terms of development of resistance and the lack of clear and robust scientific evidence on environmental pollution with drug residues (78,79).
In the solid soil phase, the antibiotics undergo reversible processes of equilibrium, sorption-desorption, and sequestration. Antibiotic’s polarity and water solubility control these processes. They are also a function of soil characteristics such as pH and pore size (80,81). The bio-accessibility and bioavailability of the antibiotics are negatively correlated with their exposure time in soil. This is because micro and nano-pores in the soil are very small for the diffusion of enzymes and microorganisms (82,83). Antibiotics in the soil can also form non-extractable residues that result from the enzymatically catalyzed formation of covalent bonds and physical diffusion into voids (84). Figure 1 depicts the sources and pathways for the flow of antibiotics in the environment (85).
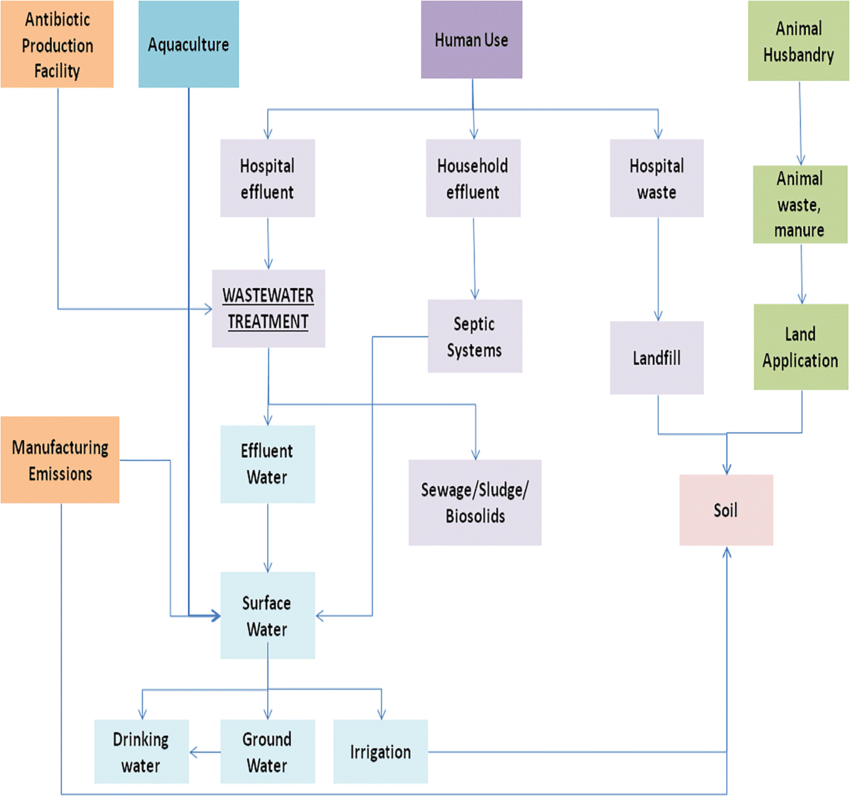
Fig. 1 Antibiotic flow in the environment. The antibiotic in human consumption, animal food industry, aquaculture, and manufacturing are represented by purple, green, blue, and orange boxes, respectively (85).
5) Mechanisms involved in antibiotic resistance
There are several genetic mechanisms by which resistance to antibiotics can develop in bacteria. These mechanisms give rise to resistance because they result in biochemical modifications that alter certain bacterial cell properties that normally render the cell sensitive to an antibiotic. Misuse, underuse, and overuse of antibiotics lead to their exposure to microbes at low levels for a prolonged period (86). It is the rationale for the emergence and dissemination of new cases of microbial resistance, which will eventually become a component of normal bacterial metabolism. Thus, resistance genes will be active even under low concentration or in the absence (control settings) (87). Resistance towards antibiotics can get propagated globally through horizontal gene transfer (HGT) events. The antibiotic resistance tends to raise the minimum inhibitory concentration (MIC) value of antibiotics for the microbes (88). The proliferation in antibiotic resistance is found to be positively associated with an increase in temperature and latitude coordinates. (89) found that an increase of 10°C increase in temperature leads to 4.2, 2.2, and 3.2% increase in the propagation of antibiotic resistance in Escherichia coli, Klebsiella pneumonia, and Staphylococcus aureus, respectively. There are multiple mechanisms by which bacteria can develop resistance to antibiotics. Examples include the activation of drug efflux pumps that actively remove a drug from the cell, the inactivation of a drug by bacterial enzymes, the alteration of bacterial cell drug targets, and the inhibition of drug uptake into the cell (90) (figure 2).
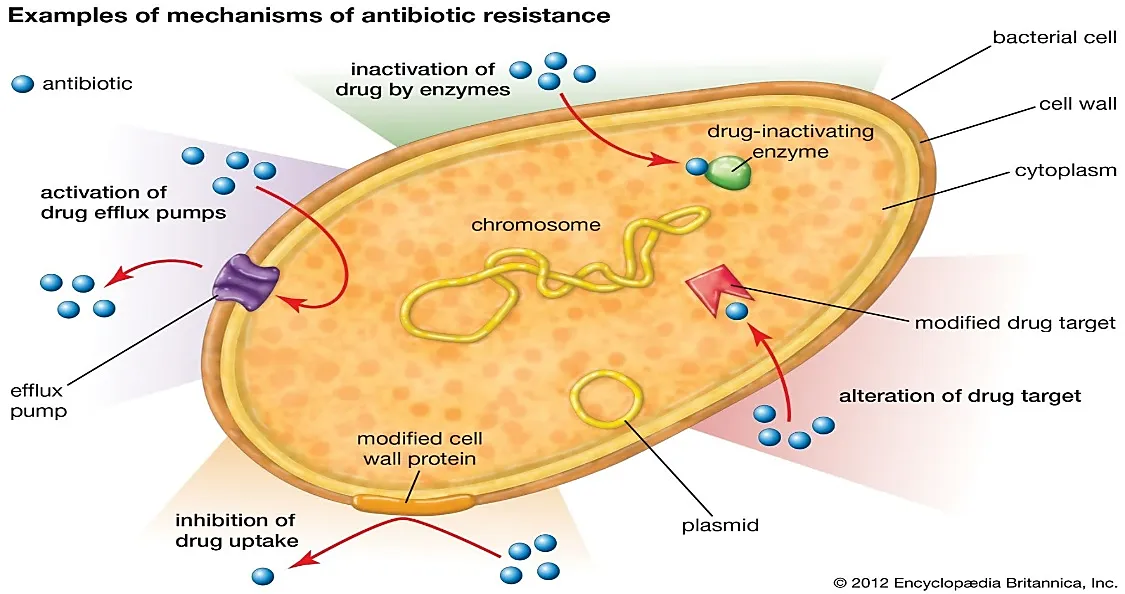
(Figure 2; Examples of mechanism of antibiotic resistance (90)).
6) Challenges in addressing antibiotic resistance
Tackling the emergence of antibiotic resistance presents complex challenges with no facile resolutions. Efforts to reduce humanity’s vast utilization of antibiotics are obstructed by their widespread integration into medical care and food animal production economics (91). Lacking rapid point-of-care diagnostics, physicians often depend on empiric antibiotic prescribing to safeguard against bacterial infections, while modern farming systems predicate the regular administration of antibiotics to livestock for infection prevention and growth promotion. Implementation of antimicrobial stewardship programs in healthcare and updated animal husbandry policies lag considerably despite awareness of resistance risks associated with antibiotic overuse. Compounding these issues, the antibiotic drug development pipeline cannot keep pace with the continuous evolution of MDR pathogens. Pharmaceutical companies increasingly abandon costly antimicrobial research with limited profit incentives. And while policy expansions financing antibiotic development mark progress, near-term solutions seem unlikely considering phase trial durations.
Further frustrating containment efforts, international coordination on antibiotic resistance surveillance and stewardship guidelines remains piecemeal despite organizations like the WHO, CDC, and UN recognizing its border less risks. Variable access to quality diagnostics and antibiotic oversight across countries enables local emergence and global spread of novel resistance factors. Patches of weak stewardship may continually undermine and negate localized progress. Ultimately, the unique ‘tragedy of the commons’ nature of antibiotic resistance demands equitable, cooperative global action and shared responsibility. However, geopolitical complexities continue obstructing consensus on binding international policies and funding channels needed to strengthen antimicrobial stewardship and innovation worldwide (92). Antibiotic resistance transcends geographical boundaries and has a global impact on populations. In recent times, formerly manageable infections have evolved into significant health concerns. The absence of efficacious antimicrobial agents renders routine medical procedures, such as surgeries, chemotherapy, and organ transplants, more precarious. In addition to the adverse impact on human health, antibiotic resistance also presents substantial economic challenges for healthcare systems, governments, and societies as a whole (93,94). The financial burden associated with managing resistant infections is significantly elevated as a result of extended hospitalizations, escalated healthcare consultations, and the necessity for costly medications as a last line of defense.
7) Future developments
The volume of waste water will drop in future as water-saving measures are introduced and the growing quantity of antibiotics used will probably increase antibiotic concentration in urban waste water. This will depend on demographic developments and changes in standards of living. According to the present level of our knowledge, concentrations necessary to favour the spread of resistance will not be reached. We have to understand this issue much better, not only with regard to resistance but also in relation to the functions and services which bacteria in the environment offer us. Frequently, it is unknown whether resistance is natural or acquired, because of the lack of identification methods regarding environmental bacteria and a lack of investigation of environmental samples from areas where no antibiotics are present due to human use. The future outlook is not optimistic, as evidenced by research commissioned by the government in the United Kingdom. This study projected that by the year 2050, there might be approximately 10 million deaths annually attributed to illnesses that are resistant to antibiotics (95). Uncomplicated infections and minor injuries could once again become life-threatening, while major procedures like organ transplants, chemotherapy, or hip replacements may become overwhelmingly risky. The economic losses associated with AMR will reach $100 trillion USD by 2050 (95). Low- and middle-income countries are expected to witness the most tremendous burden as bacterial resistance growth outpaces the development of new antimicrobial options. At the same time, resource constraints obstruct access to existing premium-priced therapies. Global coordination is critically lacking, with piecemeal containment efforts unable to match the evolutionary capacity of pathogenic bacteria continually exposed to humanity’s extensive antimicrobial use across healthcare, agriculture, and the environment.
Compounding direct mortality and economic impacts, the increasing inefficacy of antimicrobials could profoundly handicap modern medicine while enabling the resurgence of bacterial infections that had become historically rare thanks to antibiotic therapies. Cancer patients, the immunocompromised, and those requiring surgical interventions constitute populations especially vulnerable to emerging extensively- or pan-drug-resistant bacterial strains (96). Additionally, the collective burden of common infectious diseases like pneumonia, tuberculosis, and gastrointestinal illnesses may swell considerably in a post-antibiotic era. Ultimately, the rapid depletion of effective antimicrobial options jeopardizes decades of medical progress while portending reconvergence with humanity’s past, where bacterial infections constituted dominant environ-medical threats.
The history of antibiotics is ancient, long predating humans, and is a story of ongoing molecular innovations and resistance responses. While combination therapies promise to expand the antibiotic toolset for medicine, resistance development is inevitable as bacterial pathogens continue to evolve and escape the grasp of our therapeutic arsenal. Thus, rapid and adaptable discovery pipelines for a wide range of therapeutic strategies, including combination treatments, are crucial to keep the rate of discovery ahead of pathogen resistance and maintain the benefits of modern medical practice for patients.
8) CONCLUSIONS AND WORK TO BE DONE
There are enough gaps in the existing body of scientific evidence to make it a risky response to increasing public concern to deny that there is a problem with respect to resistance in the environment. On the basis of our present knowledge, an increased direct impact of antibiotics on bacteria in the aquatic environment and in soils is questionable. The input of bacteria already resistant following the use of antibiotics in human and veterinary medicine seems to be the more important source of resistant bacteria in STPs and the environment. What has been learned so far is that it is critical to prevent the selection of resistant strains in the first place both in human and veterinary medicine. The opportunities and routes whereby this may be achieved are different in both fields. According to present knowledge, the prudent use of antibiotics in all areas seems to be the key to coping successfully with resistance in the environment. Therefore, the proper use of antibiotics and disinfectants in human medicine and livestock farming will significantly reduce the risk for the general public and for the environment. This not only includes limiting the duration of the selective pressure by reducing the treatment period and the continuous use of subtherapeutic concentrations. It also includes controlling the dissemination of antibiotics being used. The use of antibiotics as growth promoters in fattening animals will diminish in Europe because of the complete ban on use of these substances by 2005.The use of antibiotics and disinfectants in veterinary medicine for prophylactic and therapeutic reasons must be monitored to make sure that there are no excessive compensatory effects. Using proper hygienic procedures and housing for animals can successfully compensate for the abandonment of growth promoters as shown by examples from Sweden and Denmark. Experience gained in Norway shows that the use of vaccines can significantly reduce the use of antimicrobials in fish farming. It is also important to use the possibilities to reduce properly the consumption in medicine. (97,98) Among other things, this will result in reducing the input of both resistant bacteria and antibiotics into the environment. These measures will also reduce costs. Therefore, the issue of resistance as a whole should be incorporated into the curricula of doctors and pharmacists. Public awareness has to be raised.
Knowledge about how antibiotic resistance arises, how resistant strains and resistance genes spread in nature and the significance of this for humans and nature is far from complete. There are not enough data available to draw a final conclusion especially with respect to the input of already resistant bacteria into the environment. This topic needs further consideration and investigation. An assessment of the different pathways also has to take into consideration the ingestion of resistant bacteria with food (e.g. poultry, pork). The importance of the different sources of resistance found in the environment, i.e. the presence of antibiotics in the environment and the importance of resistant bacteria resulting from the use of antibiotics in the various fields has to be measured. For this purpose, it is important to make a more detailed assessment of the significance of culture-dependent and laboratory-based methods in relation to conditions found in the environment. This also applies to the concentrations of antibiotics applied in the identification of resistant bacteria in laboratory testing compared to the concentrations of antibiotics in the environment. Thresholds favouring selection and transfer of resistance genes between different species under environmental conditions should be established. For this purpose, the significance of the availability and activity of the antibiotics in the environment, i.e. the extent and importance of their sorption to sludge, particles in surface water, sediment, and soil should be determined. The significance of the semi-synthetic and synthetic compounds used compared to naturally occurring compounds needs to be known for a final risk assessment. The conditions and time scales under which antibiotics and resistance are lost in the environment are also of importance in relation to the input of antibiotics and resistant bacteria. Antibiotic resistance remains an internationally worrisome problem that requires urgent intervention. The idea of antibiotic potentiation by molecules or approaches that block key metabolic pathways is a viable alternative to the “one compound, one target” model that has dominated antibiotic drug development. Although employing this combinatorial technique to build and improve antibiotics presents obstacles in terms of clinical trials and regulatory hurdles. The development of agents with the dual activity of inhibiting bacteria while also enhancing the immune system appears to be a promising strategy. Furthermore, antibiotic‐induced suppression of bacteria's downstream repair processes could be the ultimate haymaker for tackling bacterial pathogens. The benefits and need for the use of antibiotics cannot be ignored, but the effects of antibiotics in the environment must be taken into account, given their potential to maintain, cause and disseminate resistance, and also to exert a number of negative effects on the entire ecosystem. To improve knowledge regarding the impact of antibiotic residues on the environment, there is a need to take protective, timely measures to avoid latter irreversible consequences.
REFERENCES


Basit Akber Para*, Amandeep Kaur, Antibiotic Resistance, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2941-2958. https://doi.org/10.5281/zenodo.21363836
 10.5281/zenodo.21363836
10.5281/zenodo.21363836