
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1. Department of Pharmaceutical Science, Faculty of Pharmacy, Madhyanchal Professional University, Bhopal (M.P.)
Background: Diabetes mellitus is a chronic metabolic disorder characterized by persistent hyperglycemia, dyslipidemia, oxidative stress, and progressive damage to vital organs. The limitations associated with long-term use of conventional antidiabetic drugs have encouraged the exploration of plant-derived therapeutic agents. Saraca asoca (Roxb.) de Wilde is a medicinal plant rich in bioactive phytoconstituents with potential antioxidant and antidiabetic properties. Objective: The present study was undertaken to evaluate the antihyperglycemic, antihyperlipidemic, antioxidant, and organ-protective effects of ethanolic extract of Saraca asoca bark (SAB) in alloxan-induced diabetic rats. Methods: Experimental diabetes was induced in Wistar rats using alloxan monohydrate (150 mg/kg, i.p.). Diabetic animals were treated orally with SAB at doses of 250 and 500 mg/kg for 21 days. Fasting blood glucose levels were monitored periodically. Serum lipid profile parameters, antioxidant markers including superoxide dismutase (SOD), catalase (CAT), reduced glutathione (GSH), and malondialdehyde (MDA), as well as histopathological alterations in pancreatic, hepatic, and renal tissues were evaluated. Results: SAB treatment significantly reduced fasting blood glucose levels in a dose-dependent manner. The higher dose (500 mg/kg) reduced blood glucose levels to 107.10 ± 3.10 mg/dL, comparable to glibenclamide-treated animals. The extract significantly improved serum lipid profile by reducing triglycerides, total cholesterol, LDL, and VLDL levels while increasing HDL concentrations. Furthermore, SAB restored antioxidant enzyme activities and markedly reduced lipid peroxidation. Histopathological examination revealed substantial protection of pancreatic islets, liver architecture, and renal structures against alloxan-induced damage, with the higher dose exhibiting effects comparable to the standard drug. Conclusion: Ethanolic extract of Saraca asoca bark possesses significant antihyperglycemic, antihyperlipidemic, antioxidant, and organ-protective activities. These findings support its potential as a promising natural therapeutic agent for the management of diabetes mellitus and its associated complications.
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from impaired insulin secretion, insulin action, or both. The disease has emerged as a major global health concern due to its rapidly increasing prevalence and association with severe microvascular and macrovascular complications, including nephropathy, neuropathy, retinopathy, cardiovascular diseases, and hepatic dysfunction. According to the International Diabetes Federation, more than 537 million adults worldwide are currently living with diabetes, and this number is projected to rise substantially in the coming decades.¹ The increasing burden of diabetes poses significant challenges to healthcare systems, particularly in developing countries such as India, where the prevalence of type 2 diabetes continues to increase at an alarming rate.²
Chronic hyperglycemia is associated with profound disturbances in carbohydrate, lipid, and protein metabolism. Persistent elevation of blood glucose levels promotes excessive production of reactive oxygen species (ROS), resulting in oxidative stress and subsequent cellular damage.³ Oxidative stress plays a pivotal role in the pathogenesis and progression of diabetes and its complications by inducing lipid peroxidation, protein oxidation, DNA damage, and impairment of endogenous antioxidant defense mechanisms.⁴ Furthermore, diabetes-induced oxidative stress contributes to structural and functional alterations in vital organs, particularly the pancreas, liver, and kidneys.⁵
Experimental diabetes induced by alloxan monohydrate is a well-established animal model for investigating antidiabetic agents and their mechanisms of action. Alloxan selectively accumulates in pancreatic β-cells through the GLUT2 transporter and generates reactive oxygen species, leading to β-cell destruction, insulin deficiency, and persistent hyperglycemia.⁶ In addition to pancreatic damage, alloxan-induced diabetes is frequently associated with dyslipidemia, oxidative stress, and histopathological alterations in multiple organs, closely resembling the pathological manifestations observed in human diabetes mellitus.⁷
Although several synthetic antidiabetic drugs are currently available for the management of diabetes, long-term treatment is often associated with limitations such as adverse effects, reduced efficacy, high cost, and poor patient compliance.⁸ Consequently, there is growing interest in the exploration of medicinal plants as alternative or complementary therapeutic agents for diabetes management. Natural products are considered valuable sources of bioactive compounds with antihyperglycemic, antioxidant, antihyperlipidemic, and organ-protective properties.⁹
Saraca asoca (Roxb.) de Wilde, commonly known as Ashoka, is an important medicinal plant belonging to the family Fabaceae. The plant has been extensively utilized in traditional systems of medicine for the treatment of various disorders, including inflammation, gynecological conditions, ulcers, microbial infections, and metabolic abnormalities.¹⁰ Phytochemical investigations have revealed the presence of numerous biologically active constituents, including flavonoids, tannins, glycosides, phenolic compounds, saponins, and steroids.¹¹ These phytoconstituents are recognized for their antioxidant and free radical scavenging activities, suggesting potential therapeutic utility against oxidative stress-mediated diseases such as diabetes mellitus.¹²
Previous studies have demonstrated several pharmacological activities of Saraca asoca, including antioxidant, anti-inflammatory, antimicrobial, hepatoprotective, and cytoprotective effects.¹³˒¹⁴ However, scientific evidence regarding the antihyperglycemic efficacy of the bark extract and its influence on diabetes-associated oxidative stress, dyslipidemia, and organ damage remains limited. Furthermore, the potential protective effects of Saraca asoca bark against alloxan-induced pancreatic, hepatic, and renal injury have not been comprehensively investigated.
Therefore, the present study was undertaken to evaluate the antihyperglycemic, antihyperlipidemic, antioxidant, and organ-protective effects of ethanolic extract of Saraca asoca bark in alloxan-induced diabetic rats. The study aimed to assess its ability to regulate blood glucose levels, improve serum lipid profile, restore endogenous antioxidant defenses, and attenuate histopathological alterations in the pancreas, liver, and kidneys. The findings of this investigation may provide scientific evidence supporting the potential use of Saraca asoca bark as a natural therapeutic agent for the management of diabetes mellitus and its associated complications.
2. MATERIALS AND METHODS
2.1 Plant Material and Preparation of Extract
The bark of Saraca asoca (Roxb.) de Wilde was collected from authenticated sources and identified by a qualified taxonomist. The collected bark was washed thoroughly, shade-dried at room temperature, and pulverized into coarse powder using a mechanical grinder. The powdered material was stored in airtight containers until further use. Ethanolic extraction was performed by maceration, and the solvent was removed under reduced pressure to obtain a concentrated extract. The dried extract was preserved in a desiccator until pharmacological evaluation.¹⁵
2.2 Experimental Animals
Healthy adult Wistar albino rats of either sex weighing 150–200 g were procured from a registered animal breeding facility. Animals were housed under standard laboratory conditions (temperature 22 ± 2°C, relative humidity 55 ± 5%, and 12 h light/dark cycle) with free access to standard pellet diet and water ad libitum. The animals were acclimatized for one week prior to experimentation. All experimental procedures were conducted in accordance with the guidelines of the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA), Government of India, and were approved by the Institutional Animal Ethics Committee (IAEC).¹⁶
2.3 Acute Oral Toxicity Study
Acute oral toxicity of the ethanolic extract of Saraca asoca bark was evaluated according to the Organisation for Economic Co-operation and Development (OECD) guideline 423. Animals were administered the extract orally at a limit dose of 2000 mg/kg body weight and observed continuously for the first 4 h and periodically for 14 days for signs of toxicity, behavioral abnormalities, morbidity, or mortality. No mortality or significant toxic manifestations were observed during the study period, indicating the safety of the extract. Based on these findings, doses of 250 mg/kg and 500 mg/kg body weight were selected for pharmacological evaluation.¹⁷
2.4 Induction of Experimental Diabetes
Experimental diabetes was induced by a single intraperitoneal injection of freshly prepared alloxan monohydrate dissolved in normal saline at a dose of 150 mg/kg body weight. Following alloxan administration, animals were provided with 5% glucose solution for 24 h to prevent drug-induced hypoglycemic shock. After 72 h, fasting blood glucose levels were measured using a glucometer, and animals exhibiting fasting blood glucose levels greater than 200 mg/dL were considered diabetic and included in the study.⁶˒⁷
2.5 Experimental Design
Animals were randomly divided into five groups containing six rats each (n = 6):
Group I (NC): Normal control rats receiving vehicle only.
Group II (DC): Diabetic control rats receiving vehicle only.
Group III (SD): Diabetic rats treated with glibenclamide (10 mg/kg, p.o.).
Group IV (T1): Diabetic rats treated with ethanolic extract of Saraca asoca bark (250 mg/kg, p.o.).
Group V (T2): Diabetic rats treated with ethanolic extract of Saraca asoca bark (500 mg/kg, p.o.).
The treatment was continued once daily for 21 consecutive days. Body weight and fasting blood glucose levels were monitored periodically throughout the experimental period.¹⁸
2.6 Estimation of Fasting Blood Glucose
Fasting blood glucose levels were determined on days 0, 7, 14, and 21 using blood samples collected from the tail vein. Glucose concentration was measured using a validated glucometer and expressed as mg/dL.¹⁹
2.7 Biochemical Analysis
At the end of the experimental period, animals were anesthetized and blood samples were collected by retro-orbital puncture. Serum was separated by centrifugation at 3000 rpm for 15 min and used for biochemical analysis.
Serum triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and very-low-density lipoprotein cholesterol (VLDL-C) were estimated using commercially available diagnostic kits according to the manufacturer’s instructions.²⁰
2.8 Assessment of Antioxidant Parameters
Liver tissue homogenates were prepared in ice-cold phosphate buffer and used for the estimation of antioxidant biomarkers. Superoxide dismutase (SOD) activity was determined by inhibition of nitroblue tetrazolium reduction, while catalase (CAT) activity was measured based on the decomposition of hydrogen peroxide. Reduced glutathione (GSH) levels were estimated using Ellman’s reagent, and lipid peroxidation was assessed by measuring malondialdehyde (MDA) levels through thiobarbituric acid reactive substances (TBARS) formation.²¹–²⁴
2.9 Histopathological Examination
At the completion of the study, animals were sacrificed and the pancreas, liver, and kidneys were excised immediately. The tissues were washed with normal saline and fixed in 10% neutral buffered formalin. Following fixation, tissues were processed through graded alcohols, embedded in paraffin wax, sectioned at approximately 5 µm thickness, and stained with hematoxylin and eosin (H&E). Histopathological alterations were examined under a light microscope and photographed for documentation.²⁵
2.10 Statistical Analysis
All experimental data were expressed as Mean ± Standard Deviation (SD) for six animals per group. Statistical analysis was performed using one-way analysis of variance (ANOVA). Differences were considered statistically significant at p < 0.05.²⁶
3.1 Acute Oral Toxicity Study
The ethanolic extract of Saraca asoca bark did not produce any mortality, behavioral abnormalities, or signs of toxicity in rats up to an oral dose of 2000 mg/kg body weight. Therefore, the extract was considered safe, and doses of 250 mg/kg and 500 mg/kg body weight were selected for subsequent pharmacological studies.
3.2 Effect of Ethanolic Extract of Saraca asoca Bark on Fasting Blood Glucose Levels
The effect of ethanolic extract of Saraca asoca bark (SAB) on fasting blood glucose levels in alloxan-induced diabetic rats is presented in Table 1 and Figure 1. The diabetic control group maintained significantly elevated blood glucose levels throughout the experimental period, confirming persistent hyperglycemia following alloxan administration.
Treatment with glibenclamide and SAB resulted in a progressive reduction in fasting blood glucose levels. The antihyperglycemic effect of SAB was dose-dependent, with the 500 mg/kg dose producing a greater reduction than the 250 mg/kg dose. By day 21, blood glucose levels in the T2 group were comparable to those observed in the standard drug-treated group and approached normal physiological values. Statistical analysis revealed a significant reduction in fasting blood glucose levels in all treatment groups compared with the diabetic control group (p < 0.001).
Table 1. Effect of ethanolic extract of Saraca asoca bark on fasting blood glucose levels in alloxan-induced diabetic rats
|
Group |
Day 0 (mg/dL) |
Day 7 (mg/dL) |
Day 14 (mg/dL) |
Day 21 (mg/dL) |
|
NC |
95.20 ± 2.65 |
94.40 ± 1.58 |
96.80 ± 2.30 |
100.10 ± 4.90 |
|
DC |
281.90 ± 20.75 |
272.40 ± 20.60 |
236.10 ± 52.80 |
229.70 ± 16.90 |
|
SD |
256.80 ± 29.40 |
236.90 ± 19.80 |
219.60 ± 10.90 |
108.20 ± 3.40*** |
|
T1 |
256.50 ± 22.80 |
220.10 ± 39.60 |
204.80 ± 38.20 |
129.40 ± 9.20*** |
|
T2 |
190.10 ± 40.20 |
176.30 ± 32.90 |
147.20 ± 20.90 |
107.10 ± 3.10*** |
Data expressed as Mean ± SD (n = 6). ***p < 0.001 compared with DC.
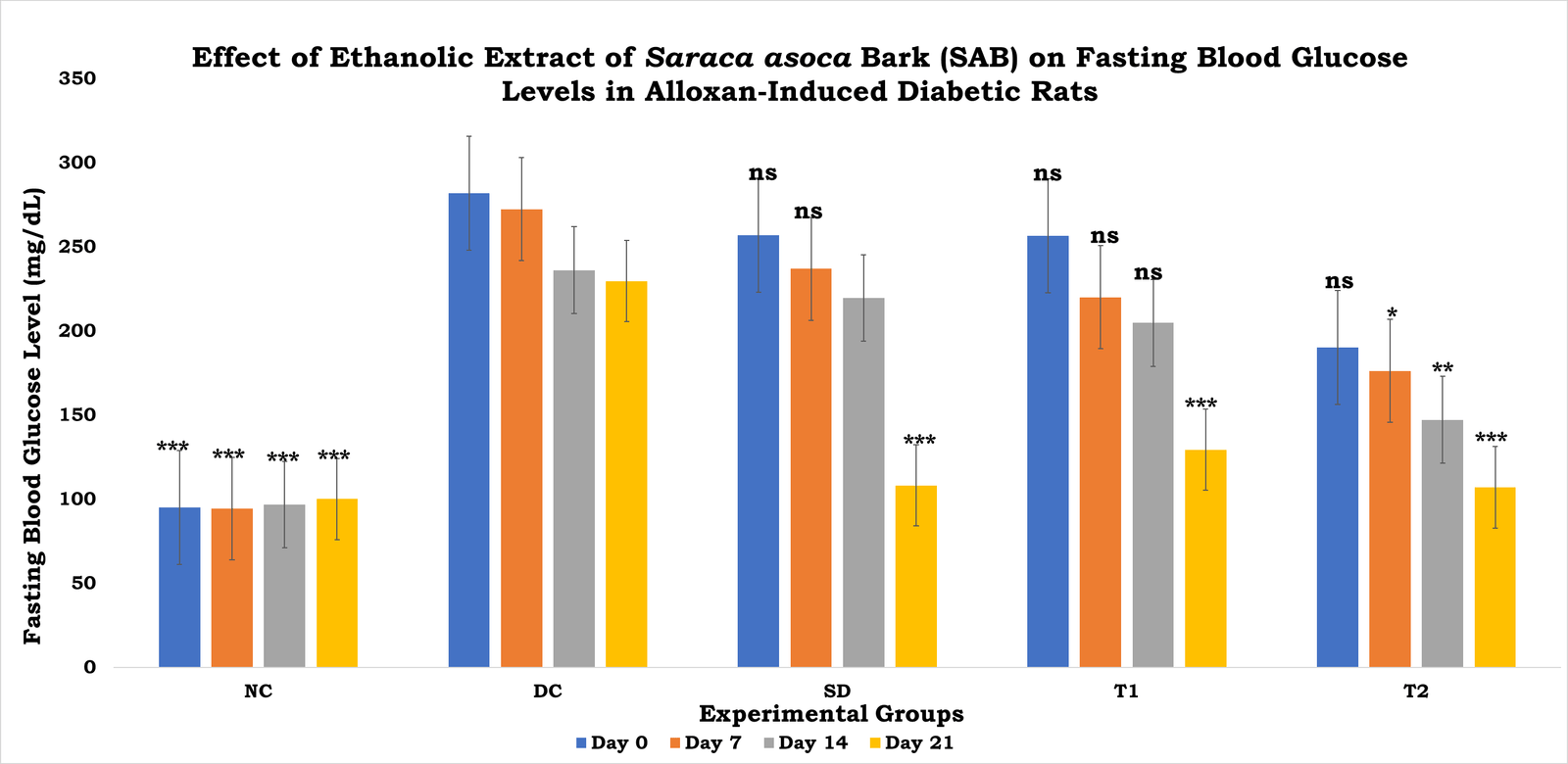
Figure 1. Effect of ethanolic extract of Saraca asoca bark (SAB) on fasting blood glucose levels in alloxan-induced diabetic rats during a 21-day treatment period.
Data are expressed as Mean ± SD (n = 6). Treatment with SD, T1, and T2 significantly reduced fasting blood glucose levels compared with the DC group in a dose-dependent manner. Statistical analysis was performed using one-way ANOVA. NC: Normal Control; DC: Diabetic Control; SD: Standard Drug (Glibenclamide, 10 mg/kg); T1: SAB (250 mg/kg); T2: SAB (500 mg/kg). *p < 0.001 compared with DC.
3.3 Effect of Ethanolic Extract of Saraca asoca Bark on Serum Lipid Profile
The effect of SAB on serum lipid profile parameters is shown in Table 2 and Figure 2. The diabetic control group exhibited significant dyslipidemia characterized by elevated triglycerides, total cholesterol, LDL, and VLDL levels accompanied by reduced HDL levels.
Treatment with SAB significantly improved the altered lipid profile in diabetic animals. The higher dose (500 mg/kg) demonstrated greater efficacy than the lower dose and markedly restored HDL levels while reducing triglycerides, total cholesterol, LDL, and VLDL concentrations. The lipid profile observed in the T2 group was comparable to that of the glibenclamide-treated group.
Table 2. Effect of ethanolic extract of Saraca asoca bark on serum lipid profile in alloxan-induced diabetic rats
|
Group |
TG (mg/dL) |
TC (mg/dL) |
HDL (mg/dL) |
LDL (mg/dL) |
VLDL (mg/dL) |
|
NC |
70.20 ± 1.30 |
105.60 ± 1.35 |
40.10 ± 1.65 |
36.40 ± 1.70 |
21.80 ± 2.10 |
|
DC |
183.40 ± 2.55 |
178.20 ± 1.80 |
25.90 ± 0.75 |
88.10 ± 1.60 |
31.40 ± 0.70 |
|
SD |
131.80 ± 1.85*** |
123.40 ± 1.90*** |
35.60 ± 0.90*** |
49.80 ± 1.55*** |
22.10 ± 1.30*** |
|
T1 |
160.50 ± 2.45** |
166.10 ± 3.10** |
28.60 ± 1.10* |
70.40 ± 0.95** |
28.90 ± 0.95* |
|
T2 |
143.20 ± 1.80*** |
113.10 ± 1.65*** |
39.10 ± 1.15*** |
58.40 ± 0.85*** |
26.10 ± 1.20** |
Data expressed as Mean ± SD (n = 6). *p < 0.05, **p < 0.01, ***p < 0.001 compared with DC.
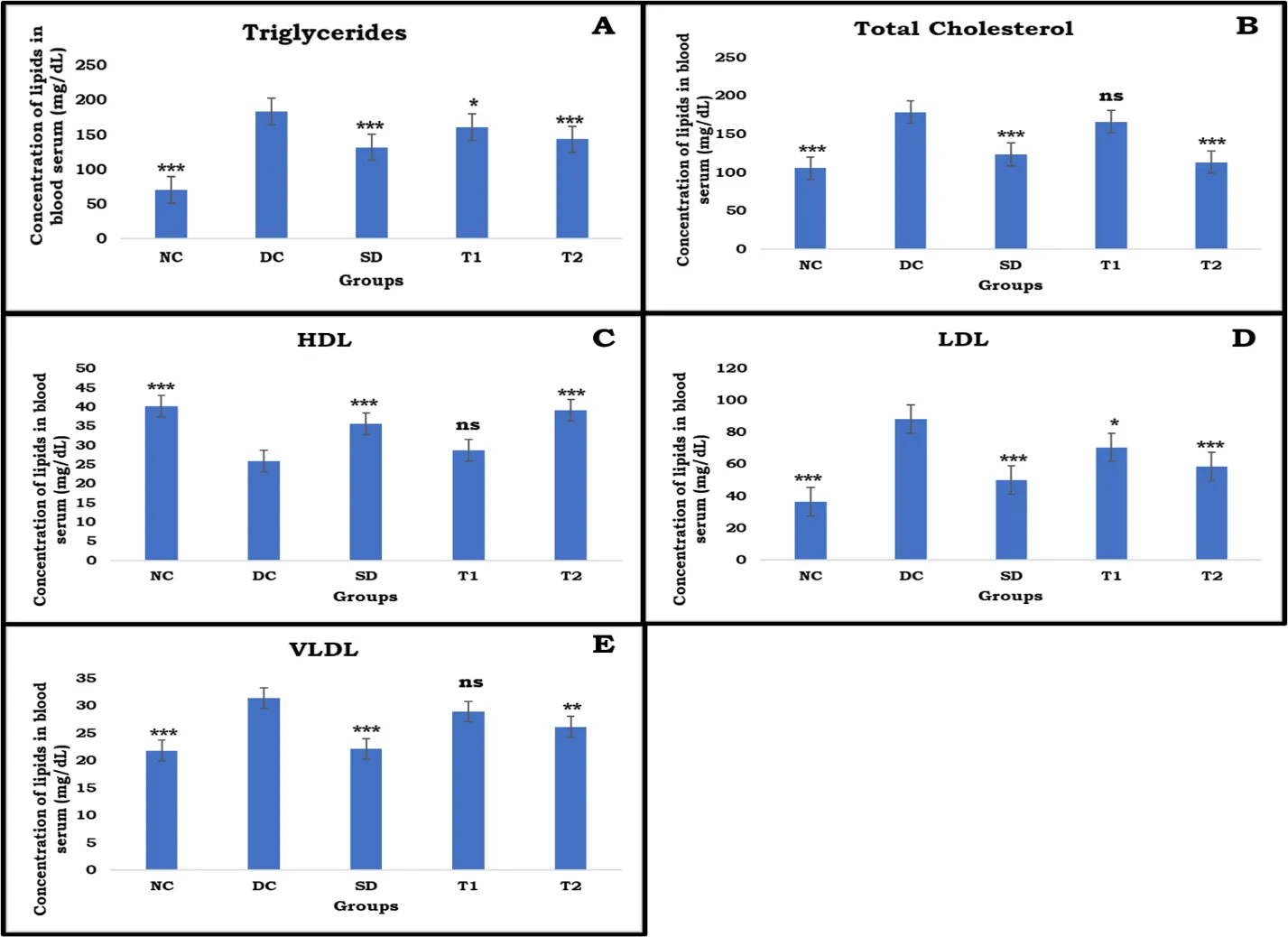
Figure 7.6. Effect of ethanolic extract of Saraca asoca bark (SAB) on serum lipid profile parameters in alloxan-induced diabetic rats after 21 days of treatment.
(A) Triglycerides, (B) Total Cholesterol, (C) HDL, (D) LDL, and (E) VLDL levels. Data are expressed as Mean ± SD (n = 6). Treatment with SD, T1, and T2 improved the altered lipid profile in diabetic rats, with T2 showing greater efficacy than T1. Statistical analysis was performed using one-way ANOVA followed by Tukey's multiple comparison test. NC: Normal Control; DC: Diabetic Control; SD: Standard Drug (Glibenclamide, 10 mg/kg); T1: SAB (250 mg/kg); T2: SAB (500 mg/kg). p < 0.05, p < 0.01, p < 0.001 compared with DC.
3.4 Effect of Ethanolic Extract of Saraca asoca Bark on Antioxidant Parameters
The antioxidant status of experimental animals is presented in Table 3 and Figure 3. Diabetes induction resulted in a marked reduction in endogenous antioxidant defenses, as evidenced by decreased SOD, CAT, and GSH levels together with a significant increase in MDA concentration.
Administration of SAB significantly restored antioxidant enzyme activities and reduced lipid peroxidation in a dose-dependent manner. The higher dose (500 mg/kg) exhibited antioxidant activity comparable to glibenclamide, resulting in substantial restoration of SOD, CAT, and GSH levels and marked suppression of MDA production.
Table 3. Effect of ethanolic extract of Saraca asoca bark on antioxidant parameters in alloxan-induced diabetic rats
|
Group |
SOD (U/mg protein) |
CAT (µmol H₂O₂ decomposed/min/mg protein) |
GSH (mg/g tissue) |
MDA (nmol/mg protein) |
|
NC |
8.45 ± 0.32 |
52.80 ± 2.15 |
6.90 ± 0.28 |
1.85 ± 0.12 |
|
DC |
4.10 ± 0.25 |
24.60 ± 1.90 |
3.15 ± 0.22 |
4.90 ± 0.30 |
|
SD |
7.60 ± 0.30*** |
47.90 ± 2.05*** |
6.10 ± 0.26*** |
2.10 ± 0.18*** |
|
T1 |
6.20 ± 0.28** |
38.40 ± 1.85** |
4.85 ± 0.24** |
2.95 ± 0.22** |
|
T2 |
7.85 ± 0.35*** |
49.30 ± 2.10*** |
6.35 ± 0.30*** |
2.05 ± 0.15*** |
Data expressed as Mean ± SD (n = 6). **p < 0.01, ***p < 0.001 compared with DC.

Figure 7.7. Effect of ethanolic extract of Saraca asoca bark (SAB) on antioxidant parameters in alloxan-induced diabetic rats after 21 days of treatment.
(A) SOD, (B) CAT, (C) Reduced GSH, and (D) MDA. Data are expressed as Mean ± SD (n = 6). Treatment with SD, T1, and T2 significantly improved antioxidant enzyme activities and reduced lipid peroxidation compared with the DC group. Statistical analysis was performed using one-way ANOVA followed by Tukey's multiple comparison test. NC: Normal Control; DC: Diabetic Control; SD: Standard Drug (Glibenclamide, 10 mg/kg); T1: SAB (250 mg/kg); T2: SAB (500 mg/kg). **p < 0.01, *p < 0.001 compared with DC.
3.5 Histopathological Evaluation
Histopathological examination of kidney, liver, and pancreatic tissues was performed to assess the protective effects of ethanolic extract of Saraca asoca bark (SAB) against alloxan-induced tissue injury (Figures 4–6).
3.5.1 Kidney Histopathology
Kidney sections from the normal control group exhibited normal renal architecture with intact glomeruli, Bowman's capsules, and well-organized renal tubules. In contrast, diabetic control animals showed marked renal damage characterized by glomerular degeneration, widening of Bowman's space, tubular epithelial degeneration, congestion, and inflammatory cell infiltration. Treatment with glibenclamide significantly restored normal renal histology. SAB treatment produced dose-dependent nephroprotection, with the 500 mg/kg group showing near-normal glomerular and tubular architecture and minimal inflammatory changes.
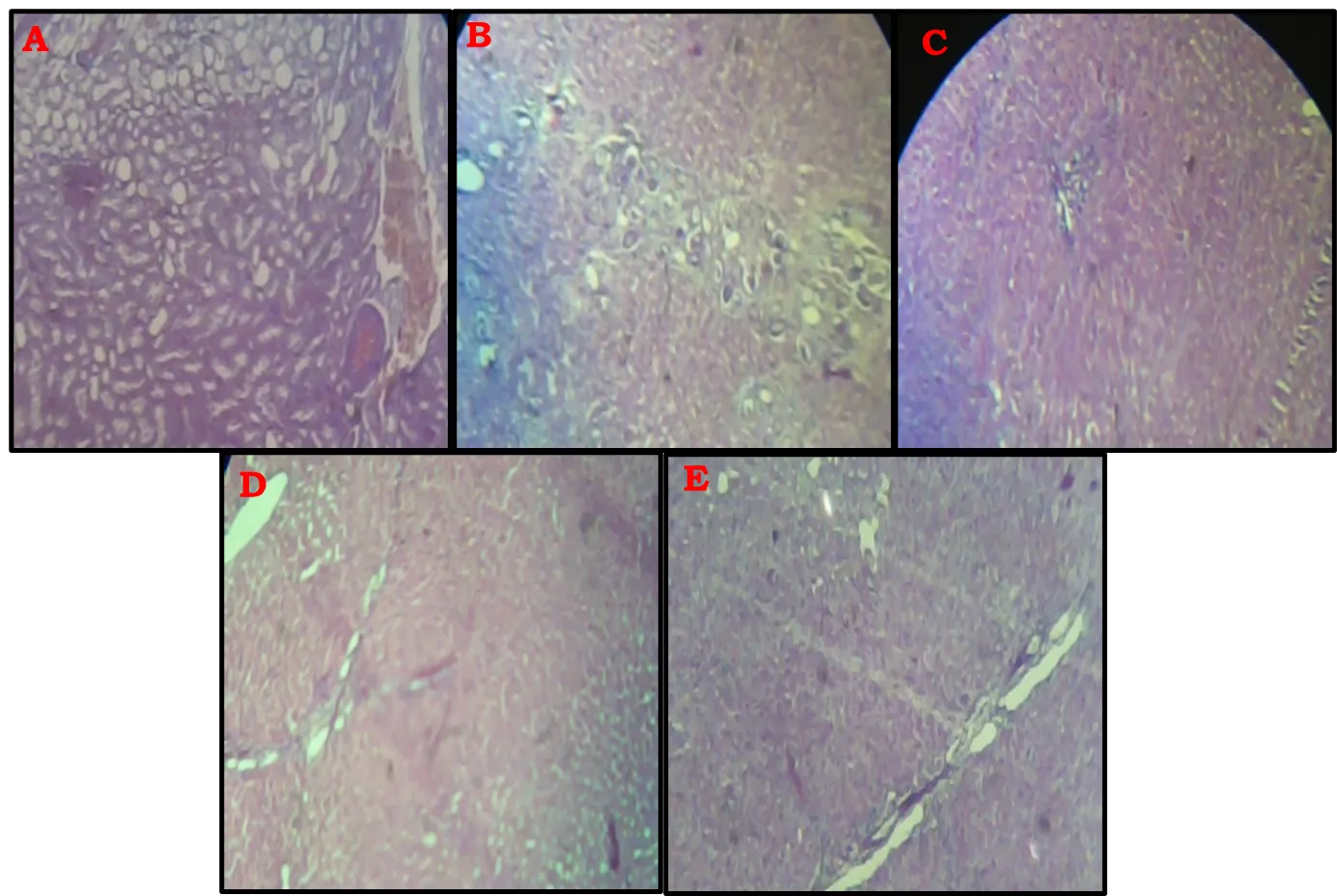
Figure 7.8. Histopathological examination of kidney tissue sections (Hematoxylin and Eosin staining, 100×).
(A) NC showing normal renal architecture with intact glomeruli and renal tubules; (B) DC showing severe glomerular and tubular degeneration, widening of Bowman's space, congestion, and inflammatory cell infiltration; (C) SD showing marked restoration of normal renal histology with reduced tissue damage; (D) T1 showing partial recovery of glomerular and tubular structures with mild residual degeneration; and (E) T2 showing near-normal renal architecture with well-preserved glomeruli and tubules. NC: Normal Control; DC: Diabetic Control; SD: Standard Drug (Glibenclamide, 10 mg/kg); T1: SAB (250 mg/kg); T2: SAB (500 mg/kg).
3.5.2 Liver Histopathology
Normal control animals displayed preserved hepatic architecture with intact hepatocytes, normal sinusoidal spaces, and organized hepatic cords. Diabetic control rats exhibited severe hepatocellular degeneration, cytoplasmic vacuolization, fatty changes, sinusoidal dilation, and inflammatory infiltration. Treatment with glibenclamide markedly improved hepatic morphology. SAB administration attenuated diabetes-induced hepatic injury in a dose-dependent manner, with the higher dose demonstrating substantial restoration of hepatocyte organization and reduction of degenerative changes.
Figure 7.9. Histopathological examination of liver tissue sections (Hematoxylin and Eosin staining, 100×).
(A) NC showing normal hepatic architecture with intact hepatocyte cords, normal sinusoidal spaces, and preserved lobular organization; (B) DC showing severe hepatocellular degeneration, cytoplasmic vacuolization, fatty changes, sinusoidal dilation, and inflammatory cell infiltration; (C) SD showing marked restoration of hepatic architecture with reduced degeneration and improved cellular organization; (D) T1 showing partial recovery of hepatic tissue with moderate restoration of hepatocyte arrangement and reduced fatty changes; and (E) T2 showing near-normal hepatic architecture with well-preserved hepatocytes, restored sinusoidal spaces, and minimal pathological alterations. NC: Normal Control; DC: Diabetic Control; SD: Standard Drug (Glibenclamide, 10 mg/kg); T1: SAB (250 mg/kg); T2: SAB (500 mg/kg).
3.5.3 Pancreatic Histopathology
Pancreatic sections from normal control animals showed intact islets of Langerhans and normal acinar tissue organization. Diabetic control rats exhibited marked islet shrinkage, reduced cellularity, β-cell degeneration, and inflammatory infiltration. Treatment with glibenclamide restored islet architecture and preserved β-cell integrity. Similarly, SAB treatment significantly improved pancreatic histology, with the 500 mg/kg dose producing near-normal islet morphology, increased cellularity, and minimal degenerative changes.
Overall, histopathological findings demonstrated that ethanolic extract of Saraca asoca bark effectively protected pancreatic, hepatic, and renal tissues against alloxan-induced damage. The protective effects were more pronounced at the higher dose and correlated with improvements in glycemic control, lipid profile, and antioxidant status.
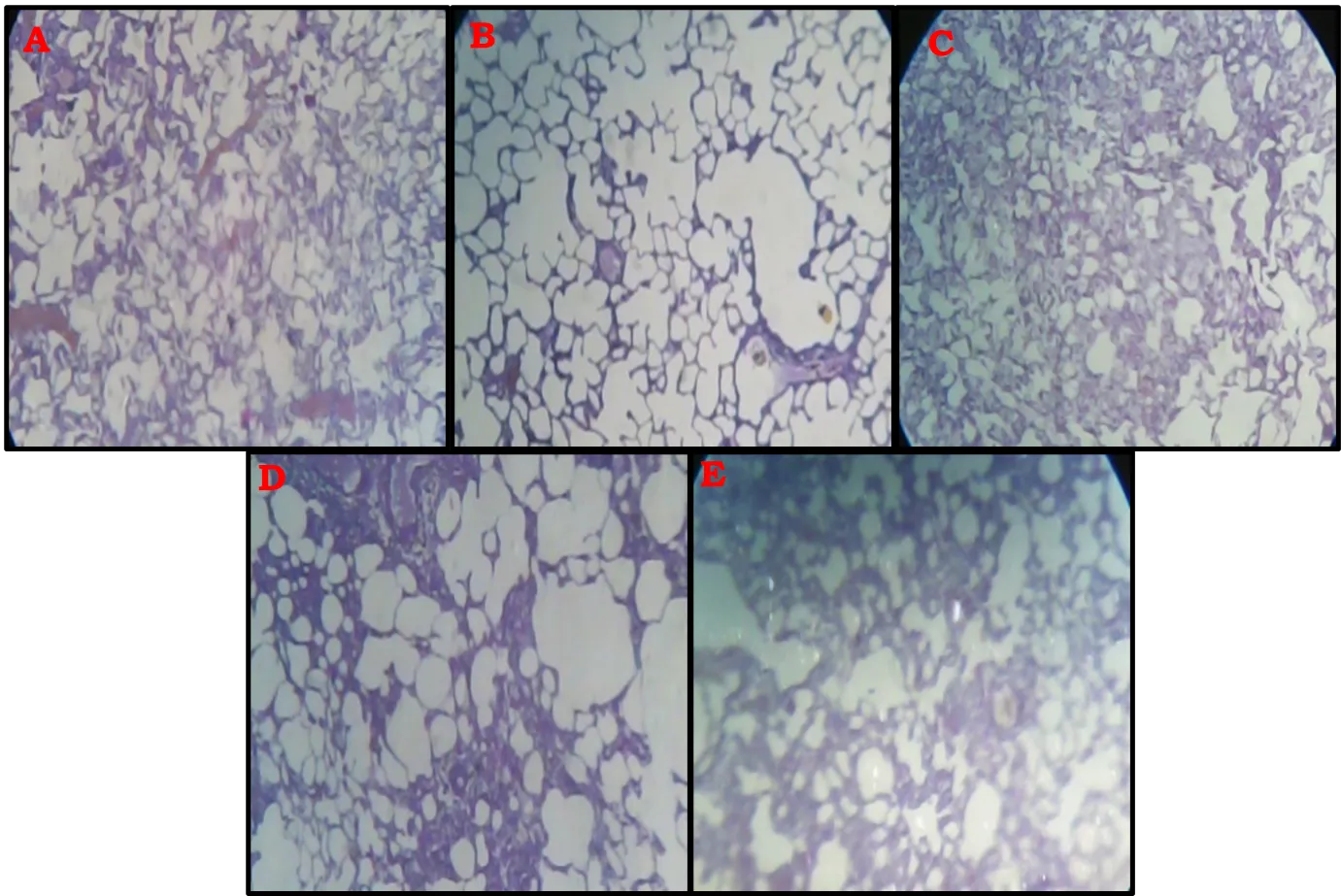
Figure 7.10. Histopathological examination of pancreatic tissue sections
(Hematoxylin and Eosin staining, 100×).
(A) NC showing normal pancreatic architecture with intact islets of Langerhans and normal acinar cells; (B) DC showing severe islet degeneration, β-cell destruction, reduced islet cellularity, and inflammatory infiltration; (C) SD showing marked restoration of islet architecture with preservation of β-cell integrity; (D) T1 showing partial recovery of islet structure with moderate improvement in cellular organization; and (E) T2 showing near-normal pancreatic architecture with increased islet cellularity, preserved β-cells, and minimal degenerative changes. NC: Normal Control; DC: Diabetic Control; SD: Standard Drug (Glibenclamide, 10 mg/kg); T1: SAB (250 mg/kg); T2: SAB (500 mg/kg).
Diabetes mellitus is a multifactorial metabolic disorder characterized by chronic hyperglycemia, impaired carbohydrate and lipid metabolism, oxidative stress, and progressive damage to various organs. Persistent elevation of blood glucose levels promotes excessive generation of reactive oxygen species (ROS), which contributes significantly to the development of diabetic complications, including nephropathy, hepatopathy, and pancreatic β-cell dysfunction.³⁻⁵ Therefore, agents capable of controlling hyperglycemia while simultaneously reducing oxidative stress and protecting vital organs are considered valuable therapeutic candidates.
In the present study, alloxan administration successfully induced experimental diabetes, as evidenced by marked elevation of fasting blood glucose levels in diabetic control animals. Alloxan selectively accumulates in pancreatic β-cells through the GLUT2 transporter and generates reactive oxygen species, resulting in oxidative destruction of insulin-producing cells and subsequent insulin deficiency.⁶˒⁷ The diabetic control group maintained significantly elevated glucose concentrations throughout the study period, confirming successful establishment of diabetes.
Treatment with ethanolic extract of Saraca asoca bark produced a significant and dose-dependent reduction in fasting blood glucose levels. The higher dose (500 mg/kg) demonstrated antihyperglycemic activity comparable to that of glibenclamide and restored blood glucose levels close to normal values. The observed glucose-lowering effect may be attributed to the presence of flavonoids, tannins, phenolic compounds, and glycosides reported in S. asoca. These phytoconstituents have been shown to enhance insulin secretion, improve peripheral glucose utilization, inhibit intestinal glucose absorption, and protect pancreatic β-cells from oxidative damage.¹¹˒¹² Similar antihyperglycemic effects have been reported for several phenolic-rich medicinal plants, where restoration of pancreatic function and improvement of insulin sensitivity contributed to glycemic control.²⁷˒²⁸
Hyperglycemia is frequently accompanied by profound disturbances in lipid metabolism, resulting in elevated serum triglycerides, total cholesterol, LDL, and VLDL levels along with decreased HDL concentrations. Such abnormalities are recognized as major risk factors for cardiovascular complications associated with diabetes.⁴˒²⁹ In the present investigation, diabetic control animals exhibited marked dyslipidemia, confirming the metabolic consequences of insulin deficiency. Reduced insulin activity enhances lipolysis and mobilization of free fatty acids from adipose tissues, leading to increased hepatic synthesis of triglycerides and cholesterol.³⁰
Administration of S. asoca bark extract significantly improved the altered lipid profile in diabetic rats. The higher dose produced substantial reductions in triglycerides, total cholesterol, LDL, and VLDL levels while simultaneously increasing HDL concentrations. These findings suggest that the extract effectively restores lipid homeostasis under diabetic conditions. The hypolipidemic activity may be related to improved insulin action, reduced hepatic cholesterol synthesis, enhanced lipid catabolism, and inhibition of lipid peroxidation. Flavonoids and polyphenolic compounds are known to regulate key enzymes involved in lipid metabolism and improve plasma lipoprotein profiles.³¹˒³² The observed restoration of HDL levels further supports the cardioprotective potential of the extract.
Oxidative stress is considered one of the central mechanisms responsible for diabetes-associated tissue injury. Excessive production of ROS causes oxidation of cellular macromolecules and depletion of endogenous antioxidant defenses, leading to progressive organ damage.³˒⁴ In agreement with previous reports, diabetic control animals exhibited significantly reduced activities of superoxide dismutase (SOD), catalase (CAT), and reduced glutathione (GSH), accompanied by elevated malondialdehyde (MDA) levels. These findings indicate severe oxidative stress and enhanced lipid peroxidation resulting from alloxan administration.²¹⁻²⁴
Treatment with S. asoca bark extract significantly restored antioxidant enzyme activities and reduced MDA levels in a dose-dependent manner. The antioxidant effect of the higher dose was comparable to that of glibenclamide, suggesting strong free radical scavenging activity. SOD and CAT constitute the primary enzymatic defense system against superoxide radicals and hydrogen peroxide, while GSH plays a crucial role in detoxification of reactive intermediates and maintenance of cellular redox balance.³³˒³⁴ Restoration of these antioxidant parameters indicates that the extract effectively strengthens endogenous antioxidant defenses and reduces oxidative injury. The reduction in MDA levels further demonstrates inhibition of lipid peroxidation and stabilization of cellular membranes. Such antioxidant activity is likely mediated by the phenolic and flavonoid constituents present in the bark extract, which possess well-documented radical-scavenging properties.¹²˒³⁵
Histopathological examination provided additional evidence supporting the biochemical findings. The pancreas is the primary target organ affected by alloxan toxicity, and severe damage to β-cells is responsible for insulin deficiency and hyperglycemia.⁶ In the present study, pancreatic sections from diabetic control animals showed marked degeneration of islets of Langerhans, reduced cellularity, β-cell destruction, and inflammatory infiltration. These observations are consistent with previous reports describing alloxan-induced pancreatic injury.³⁶
Treatment with S. asoca bark extract markedly improved pancreatic histology, particularly at the higher dose. Restoration of islet architecture, increased cellular density, and preservation of β-cell morphology were evident in treated animals. The histological recovery observed in pancreatic tissue correlates closely with the reduction in blood glucose levels and suggests that the extract may protect residual β-cells from oxidative damage or promote regeneration of damaged pancreatic tissue. Similar β-cell protective effects have been reported for polyphenol-rich medicinal plants possessing antioxidant and antidiabetic properties.³⁷˒³⁸
The liver plays a critical role in maintaining glucose and lipid homeostasis and is highly susceptible to oxidative stress during diabetes. Persistent hyperglycemia promotes hepatic lipid accumulation, inflammation, and cellular degeneration.³⁹ In the present study, liver sections from diabetic control animals exhibited hepatocellular degeneration, cytoplasmic vacuolization, fatty changes, sinusoidal dilation, and inflammatory infiltration. These pathological alterations indicate severe hepatic injury resulting from uncontrolled diabetes and oxidative stress.
Administration of S. asoca bark extract significantly attenuated hepatic damage and restored normal liver architecture. Treated animals showed improved hepatocyte organization, reduced fatty degeneration, and minimal inflammatory infiltration. The hepatoprotective effect may be attributed to improved glycemic control, inhibition of oxidative stress, and stabilization of cellular membranes. Previous studies have demonstrated that flavonoids and phenolic compounds protect hepatocytes by suppressing oxidative damage and inflammatory responses.¹³˒⁴⁰
Diabetic nephropathy is among the most common complications of diabetes and is strongly associated with oxidative stress and chronic hyperglycemia.⁴¹ In the present study, diabetic control rats exhibited pronounced renal damage characterized by glomerular degeneration, widening of Bowman's space, tubular epithelial injury, congestion, and inflammatory infiltration. These findings are consistent with the pathological manifestations of diabetic nephropathy reported in experimental models.⁴²
Treatment with S. asoca bark extract markedly improved renal histology and preserved glomerular and tubular integrity. The higher dose produced near-normal renal architecture and significantly reduced inflammatory changes. The nephroprotective effect may result from suppression of oxidative stress, improvement of glycemic control, and prevention of lipid peroxidation-induced cellular injury. Similar renoprotective effects have been reported for antioxidant-rich plant extracts capable of reducing ROS-mediated damage in diabetic kidneys.⁴³˒⁴⁴
Collectively, the present findings demonstrate that ethanolic extract of Saraca asoca bark exerts significant antihyperglycemic, antihyperlipidemic, antioxidant, and organ-protective activities in alloxan-induced diabetic rats. The observed therapeutic effects are likely mediated through the synergistic action of multiple phytoconstituents, particularly flavonoids, tannins, and phenolic compounds. By improving glycemic control, restoring antioxidant defenses, correcting dyslipidemia, and protecting vital organs from oxidative injury, S. asoca bark shows considerable promise as a natural therapeutic candidate for the management of diabetes mellitus and its associated complications.
The present study demonstrated that the ethanolic extract of Saraca asoca bark possesses significant antihyperglycemic, antihyperlipidemic, antioxidant, and organ-protective activities in alloxan-induced diabetic rats. Administration of the extract produced a marked and dose-dependent reduction in fasting blood glucose levels, indicating effective glycemic control under diabetic conditions. The higher dose (500 mg/kg) exhibited efficacy comparable to the standard antidiabetic drug glibenclamide.
In addition to its antihyperglycemic effect, the extract significantly improved diabetes-associated dyslipidemia by reducing serum triglycerides, total cholesterol, LDL, and VLDL levels while increasing HDL concentrations. These findings suggest a beneficial role of S. asoca bark in restoring lipid homeostasis and reducing the risk of metabolic complications associated with diabetes mellitus.
The extract also effectively attenuated oxidative stress, as evidenced by significant restoration of endogenous antioxidant enzymes including superoxide dismutase, catalase, and reduced glutathione, along with a marked reduction in malondialdehyde levels. The antioxidant activity observed in the present study indicates that the extract can counteract reactive oxygen species-mediated cellular damage and lipid peroxidation.
Histopathological examination further confirmed the protective effects of the extract on pancreatic, hepatic, and renal tissues. Treatment with S. asoca bark markedly restored normal tissue architecture, reduced inflammatory and degenerative changes, and preserved cellular integrity in diabetic animals. These observations strongly support the biochemical findings and indicate that the extract exerts substantial protection against diabetes-induced organ damage.
Overall, the results suggest that the therapeutic effects of Saraca asoca bark may be attributed to the synergistic action of its bioactive phytoconstituents, particularly flavonoids, tannins, and phenolic compounds. The findings provide scientific evidence supporting the traditional use of S. asoca and highlight its potential as a promising natural therapeutic agent for the management of diabetes mellitus and its associated complications. Further studies focusing on isolation of active constituents, molecular mechanisms, and long-term safety evaluation are warranted to facilitate its development as a phytopharmaceutical intervention.
DECLARATIONS
Ethics Approval and Consent to Participate
All animal experimental procedures were performed in accordance with the guidelines of the CPCSEA, Government of India, and were approved by the IAEC Approval No. 1698/PO/Re/S/13/CPCSEA.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare that there are no conflicts of interest regarding the publication of this manuscript.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
Vikash Chandra Saroj conceived and designed the study, performed the experimental work, analyzed and interpreted the data, and prepared the manuscript. Dharmendra Singh Rajput contributed to study supervision, experimental design validation, data interpretation, and critical revision of the manuscript. Naveen Gupta, Ganesh Prasad Patel, and Brajmohan Kaushal assisted in experimental execution, data collection, and manuscript review. Shaily Chaudhary supervised the overall research work, contributed to scientific interpretation of the results, and approved the final version of the manuscript.
All authors have read and approved the final manuscript.
Acknowledgements
The authors are grateful to the Department of Pharmaceutical Sciences, Faculty of Pharmacy, Madhyanchal Professional University, Bhopal, India, for providing the necessary laboratory facilities and support to carry out this research work.
REFERENCES

Vikash Saroj, Dharmendra Rajput, Naveen Gupta, Ganesh Patel, Brajmohan Kaushal, Shaily Chaudhary*, Antihyperglycemic, Antihyperlipidemic and Antioxidant Effects of Ethanolic Extract of Saraca asoca Bark in Alloxan-Induced Diabetic Rats, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 199-215. https://doi.org/ 10.5281/zenodo.21127290
 10.5281/zenodo.21127290
10.5281/zenodo.21127290