
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dr. Rajendra Gode College of Pharmacy, Amravati.
Clinical trials are essential to the safe, reliable, and effective development of medications. Artificial intelligence (AI) is being used in medical and healthcare organizations due to data-related limitations, labor-intensive manual labor, remote patient monitoring, and the complexity of traditional clinical patient research. For rapid and effective clinical trials, a tailored AI solution is the best use case. Through standardized, digitally driven, and structured components, artificial intelligence (AI) provides a variety of beneficial alternatives in medical research. Time-consuming elements of clinical research include patient enrollment, recruitment, ongoing monitoring, and medical adherence and retention. All of the patient's medical history information can be generated and managed automatically for the trial lifespan by an AI-powered, patient-focused platform. This article explains how new methods for data collecting, bio simulation, and early disease diagnosis for clinical trials have been revolutionized by artificial intelligence (AI). Additionally, it precisely overcomes the challenges by reducing expenses and time, boosting productivity, and improving drug development research with less rework requirements. AI has the potential to speed up clinical trials in the future, which is crucial for medical research because it produces results fast and has a wide range of uses. important for research in medicine. Artificial intelligence (AI) methods that improve decision-making, lower human error, and increase trial outcome accuracy include big data analytics, machine learning, and natural language processing.AI also facilitates faster identification of suitable candidates, enhances risk assessment, and boosts patient participation throughout the trial. It also effectively tackles challenges by reducing expenses and time, boosting productivity, and improving drug development research with less rework requirements. AI's potential to speed up clinical trials and enhance healthcare innovation in the future is critical for medical research and pharmaceutical development because of its numerous applications and quick discoveries.
The purpose of a clinical trial is to determine if a new medical treatment or a novel approach to use an existing medication will be more effective in preventing, diagnosing, or treating a disease. All new drugs must pass preclinical tests before they can be used in clinical trials. In vitro (i.e., test-tube or laboratory) research and trials on animal populations are a part of preclinical investigations. To gather initial data on pharmacokinetics, toxicity, and efficacy, a wide range of dosages of the research drug are administered to animal subjects or to an in vitro substrate.
PHASES OF CLINICAL TRIALS:
Pharmaceutical companies carry out thorough pre-clinical research on a medicine before beginning clinical trials. Studies conducted before clinical trials pre-clinical research includes investigations and trials on animal populations that are conducted in vitro, or in a test tube or laboratory. Animal participants or an in-vitro substrate are administered a wide range of dosages of the study medicine to gather preliminary data on pharmacokinetics, toxicity, and efficacy. This helps pharmaceutical companies determine if it is worthwhile to proceed with additional testing.
Phase 0: According to the U.S. Food and Drug Administration's (FDA) 2006 Guidance on Exploratory Investigational New Drug (IND) Studies, exploratory, first-in-human studies are now referred to as phase 0. By determining early on whether a prospective medication or imaging agent behaves in humans as predicted by preclinical research, phase 0 trials are intended to expedite the development of such products. A small group of 10 to 15 people will get a one-time, low (non-therapeutic) dose of the study drug to help us get an early idea of how it moves through the body. (How the body processes the drug) and pharmacodynamics (how the drug works in the body) is one of the distinctive characteristics of Phase 0 trials.
Phase I: Phase I trials are the initial phase of human subjects testing. Typically, a small (20–80) group of volunteers in good health will be chosen. Trials intended to evaluate a drug's pharmacokinetics, pharmacodynamics, tolerability, and safety (pharmacovigilance) are included in this phase. Full-time staff members can watch the person during these studies, which are frequently carried out in an inpatient clinic. After the medicine is administered, the patient is typically monitored for a number of drug half-lives. To determine the right dose for therapeutic usage, phase I trials often incorporate dose-ranging, also known as dose escalation, investigations. In animal testing, the range of dosages that are evaluated is often a small portion of the level that is harmful. The majority of phase I studies involve healthy participants. In certain situations, though, such as when a patient has end-stage illness and no other alternatives for therapy, actual people are employed. The most common exceptions to this rule are seen in HIV medication trials and oncology (cancer). In exchange for their time in the volunteer center, volunteers get an inconvenience fee. Pay varies based on duration of involvement, from a modest sum for a brief stay to a bigger sum of up to almost £4,000.
Phase II: After Phase I studies have established the study drug's initial safety, Phase II trials are conducted on larger groups (20–300) to evaluate the drug's effectiveness and to repeat Phase I safety evaluations in a larger patient and volunteer population. Failure to create a novel medicine frequently happens during Phase II trials when the drug is shown to have harmful effects or not operate as intended. Sometimes, Phase II trials are broken down into two parts: IIA and IIB. Phase IIB is especially intended to investigate effectiveness, whereas Phase IIA is specifically intended to evaluate dosage needs (the amount of medication that should be administered). (How well the medicine functions at the recommended dosage or dosages).
Phase III: Phase III studies are large tests done at different hospitals or clinics to see how well a new drug works compared to the best treatment currently available. They usually include 300 to 3,000 or more patients, depending on the illness being studied. These trials take a lot of time, money, and effort especially for diseases that last a long time because they are big and take a long time to complete. While the regulatory proposal is being processed by the relevant regulatory body, it is customary for some Phase III trials to proceed. A minimum of two successful Phase III trials proving a drug's safety and effectiveness are usually expected in order to receive approval from the relevant regulatory bodies (FDA (USA), TGA (Australia), EMEA (European Union), etc.), though this is not always the case. Following successful Phase III trials, the results of the trials are typically compiled into a lengthy document that includes a thorough explanation of the techniques and findings of both human and animal research, manufacturing processes, formulation specifics, and shelf life. The regulatory submission that is submitted for evaluation to the relevant regulatory bodies in various nations is composed of this compilation of data. The majority of medications during Phase III clinical studies can be sold in accordance with FDA regulations, provided that appropriate advice and instructions are followed. However, if any negative side effects are discovered anywhere, the medications must be taken off the market right once. It is not uncommon to find numerous medications undergoing Phase III clinical trials on the market, even though the majority of pharmaceutical corporations avoid this approach.
Phase IV: The Post Marketing Surveillance Trial is another name for a phase IV trial. Phase IV trials involve ongoing technical assistance and pharmacovigilance, or safety monitoring, following a medication's approval for sale. The sponsoring company may conduct phase IV studies for competitive (finding a new market for the drug) or other reasons (e.g., the drug may not have been tested for interactions with other drugs or on certain population groups like pregnant women, who are unlikely to subject themselves to trials) reasons, or regulatory authorities may require them. The purpose of safety surveillance is to identify any uncommon or chronic side effects across a longer time span and a far bigger patient population than was feasible during Phase I–III clinical trials. A medication may be discontinued from sale or limited to specific applications if Phase IV trials reveal harmful effects: Recent instances include troglitazone (Rezulin), rofecoxib, and cerivastatin (brand names Baycol and Lipobay).
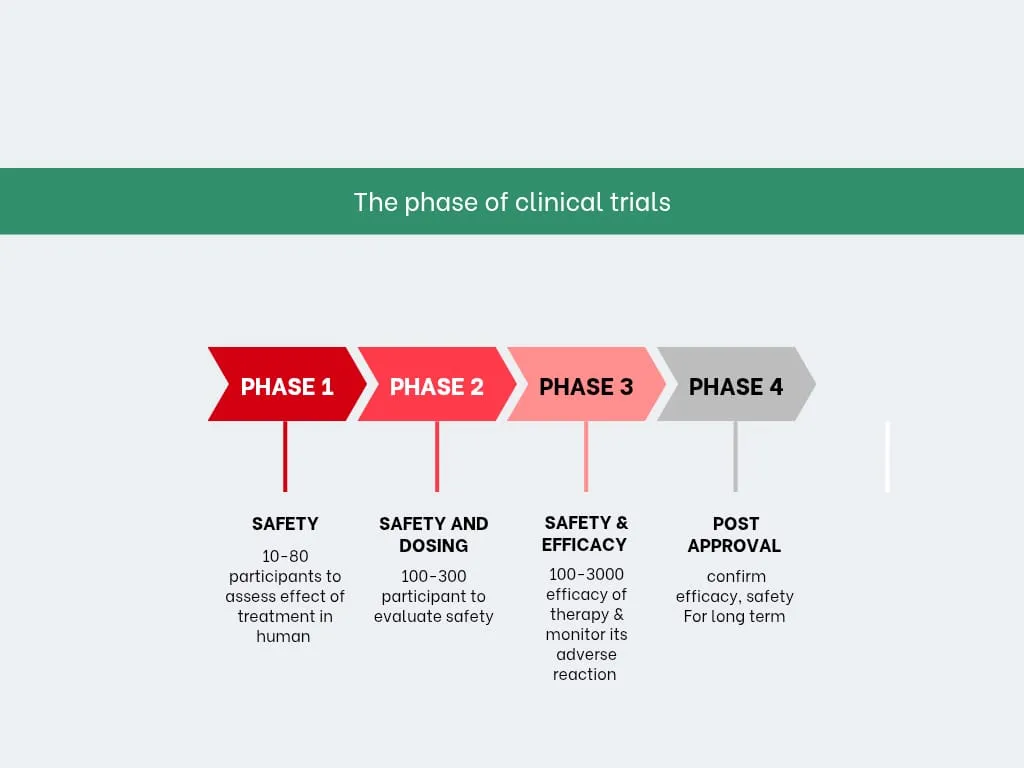
Figure no1: Phases of clinical trails
Importance: -
One of the pillars of contemporary evidence-based medicine is the evidence derived from clinical trials, in conjunction with clinical judgment and patient values and preferences[1]. Clinical trials are typically carried out to assess an intervention's cost-effectiveness, safety, or efficacy with a reasonable margin of error. The fundamental objective remains unchanged: enhancing patient care. Currently regarded as the most trustworthy source of data in medical practice, randomized controlled trials (RCTs) are commonly referred to as the gold standard of hypothesis testing. For patients, researchers, and the healthcare system as a whole, RCTs are time and effort-consuming. Additionally, as their findings are based on an intervention experiment carried out in a particular patient cohort under strict guidelines and well-defined conditions, their clinical application is not simple. When deciding whether or not to apply an intervention to a specific patient, doctors may consider all of these factors differently than those found in clinical practice. It is true that clinicians may find it challenging to evaluate results, and many research issues are typically ethically prohibitive from being investigated in clinical trials. Clinicians must contend with differences in the quality of study methodology and supporting data in addition to generalizability issues. When the quality and strength of the body of data supporting a clinical question are standardized, some of these obstacles can be removed. This is the goal of the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) technique, which is used in clinical practice guidelines. It combines subject expert knowledge with clinical trial evidence to produce recommendations [2]. Despite the widespread recognition of the value of clinical trials in enhancing healthcare, it is noteworthy that there is still a dearth of research assessing their effectiveness in relation to alternative sources of information. Researchers have created stricter, more detailed guidelines and standards to be used in order to safeguard recruited individuals, lessen biases and uncertainty, and strengthen the quality of the evidence generated by clinical trials since their use first increased in the late 1960s and early 1970s. These elements have been studied, improved, and applied to create a new scientific field called clinical trial methodology [3]. Based on their experience with academically started non-commercial trials, Farrell and Kenyon [4]. Making sure every part of a clinical trial is closely managed is very important, according to the Guide to Efficient Trial Management. Doctors need to be confident and well-trained to recruit participants, which can be done through one-on-one training, group sessions, or online tools like videos and calls. The trial team should also hold meetings to remind everyone why the trial is important. Maintaining personal contact with doctors, whether a few or many, is one of the most challenging but essential tasks for the trial team. It helps make the trial more connected and effective. However, clinical trials are not risk-free, and many drugs fail before reaching the market. Despite more spending on research and development, the failure rates of trials have increased over time. Between 1990 and 2004, failure rates raise from 30% to 50% in Phase 1, 40% to 70% in Phase 2, and 20% to over 50% in Phase 3[5,6]. Regulatory bodies only approve less than 10% of medications that initially go through clinical trials. Clinical trials represent only a small part of the overall drug development process. Before reaching human trials, new drugs must first be discovered, purified, and tested in laboratories using cells and animals. Only a few of these early candidates show enough promise to move forward. Drug development begins once a potential compound is identified and involves pre-clinical testing, regulatory approval to begin human trials, and eventually applying to market the drug. For example, about 250 of the 5,000 cancer compounds that are investigated in the lab move on to pre-clinical testing, less than 10 advance to clinical trials, Usually, only one is approved for use. Overall, the process from initial research to an approved treatment takes about 10 to 13 years [7]. The development of novel therapies as well as improved methods for illness detection and prevention depends on clinical trials. They assist scientists in determining what works and what doesn't in people, which is not possible with laboratory or animal research. Trials also assist physicians in balancing a treatment's potential advantages against any negative consequences. Determining whether to participate can be challenging because the trial's outcome is uncertain beforehand. Many have profited because others volunteered in trials that resulted in better therapies, even though some patients may suffer harm. Whether or not to participate in a trial depends on your circumstances [8].
The Evolution of AI:
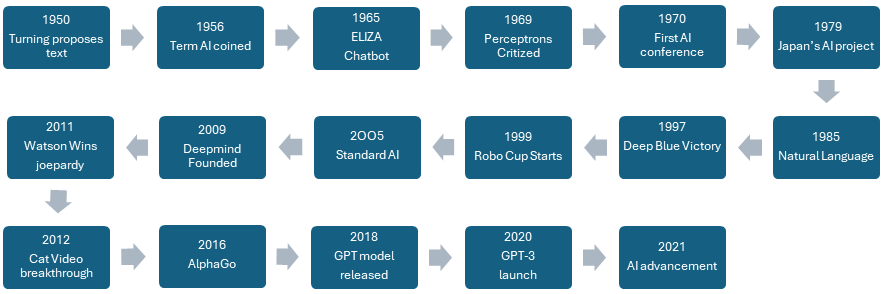
Figure no 2: -The Evolution of AI
The use of AI in medicine began in the early 1970s with the development of expert systems like MYCIN to improve diagnostic decision-making [9]. To educate computers to encode clinical information as logic rules for particular clinical circumstances, early medical AI systems, however, placed a significant reliance on medical domain specialists. These systems were limited by the fact that they required a lot of work and time to build, and that once they were in place, they were hard to update [10]. Until the 1990s and 2000s, the medical field did not adopt more advanced machine learning systems that can learn these rules by identifying and weighing relevant features from data such as unstructured text, medical images, and electronic health records (EHRs). The absence of publicly accessible data and the necessity of rigorous feature-engineering efforts involving significant commitments from medical domain experts were the key causes of this [11]. Two causes have caused a significant change in this scenario in recent years. First, thanks to hardware advancements and massive training datasets, the field of artificial intelligence (AI) saw revolutionary breakthroughs, especially in deep learning and associated machine learning techniques [12,13].Second, new public policy initiatives like the Electronic Records Meaningful Use Programs in the USA and technological advancements have made medical data more widely available in digital form. The use of AI in medicine has increased recently, and there have been early proof-of-concept results as well, beginning with medical imaging to identify diabetic retinopathy. [14]. and skin cancer [15], to utilizing EHR data to forecast critical clinical metrics, such as mortality and illness start [16].This explosion in artificial intelligence (AI) techniques has also helped the biomedical profession on several levels, from advanced natural language processing (NLP) searches of the biomedical literature [17],to employ DL for cancer sub-phenotyping [18], to predictions of gene targets of microRNAs [19], drug–target interactions, and drug repositioning hypotheses [20].
Different Methods Used in AI: -
Artificial Intelligence (AI): emulation of human intellectual processes by machines, such as self-correction, learning, and reasoning. Building computers that have human-like perceptions of the world and decision-making abilities is the ultimate objective of artificial intelligence.
Association rule mining: ML algorithms that find intriguing relationships between variables in big databases can assist a computer in simulating the human brain's ability to identify and abstract associations from fresh, unclassified material.
Brain–machine interface (BMI): A direct line of communication between an external device and an augmented or connected brain. Other terms that are used include mind-machine interface (MMI), brain-computer interface (BCI), and direct neural interface (DNI).
Deep learning (DL): a class of machine learning techniques based on artificial neural networks that employ numerous layers to gradually extract higher level characteristics from raw input by drawing inspiration from information processing and distributed communication nodes in biological systems. The term deep in deep learning describes how many layers are used to change the data.
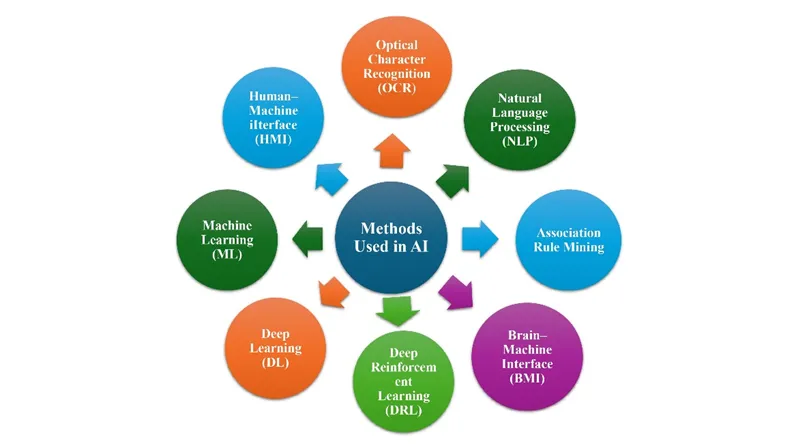
Fig no 3: - Different Methods Used in AI
Deep reinforcement learning (DRL): ML's reinforcement learning (RL) field focuses on creating software agents that can operate in a given environment in a way that maximizes a concept known as cumulative reward. In order to develop effective algorithms for this purpose, DRL integrates DL and RL concepts.
Human–machine interface (HMI): a channel of direct communication between a person and a gadget. An example of a human–machine interface is an artificial system that can automatically comprehend and react to human language, whether it be written or spoken.
Machine learning (ML): Algorithmic algorithms that, without being explicitly coded to do so, generate a mathematical model of sample data in order to make decisions or predictions. A common misconception about AI is that it includes machine learning.
Natural language processing (NLP): A branch of artificial intelligence that focuses on how computers interact with human (natural) languages, specifically on how to teach computers to handle and analyze vast volumes of natural language data. Numerous fields, such as computer science and computational linguistics, are included within NLP.
Optical character recognition (OCR): Computer vision, pattern recognition, and artificial intelligence researchers are studying the electronic conversion of images of typed, handwritten, or printed text into machine-encoded text (whether from scanned documents, document photos, scene photos, or subtitle text superimposed over an image).
AI and clinical trials:
It may be the people in charge of a clinical study's first stages who decide its future. Finding participants can increase the trial's likelihood for efficacy, but choosing and recruiting patients can take a lot of time and money. A study's failure may be due to ineffective or delayed recruitment efforts. In the early phases of clinical trials, this financial risk should be seen as a motivator to use AI technology. By categorizing data, AI can identify patient populations that might profit from clinical study. The recruitment effort might be more targeted by analysing social media content to find illness or condition hotspots. By analyzing hospital medical data and informing physicians and patients about clinical trial options, AI can speed up the process of finding appropriate volunteers. Previously complex admissions standards can be simplified by technology, increasing their accessibility for eligible candidates. Large volumes of medical data can be searched by AI to find possible clinical study patients. To classify people with type 2 diabetes into three groups, for example, researchers at Mount Sinai Medical Centre in New York employed topological data analysis (TDA) to examine genetic data and electronic health records (EHRs) [21]. The TDA's patterns of clinical characteristics and medical comorbidities provided insights on how certain individuals will respond to a medication or clinical trial. AI-powered patient identification is at the forefront of fields like social media data analysis. AI is capable of sorting through online chats from patient support groups to determine whether any sickness clusters exist in a certain location. This technique could help with the quick identification of cohorts, which would help companies design clinical trials more effectively. AI could help with hiring when a target population has been identified. AI might expedite recruiting and reduce unnecessary inspections.
Applications:
Compiling information for distributed testing
In decentralized clinical trials, handling the enormous volumes of data that need to be gathered and examined is one of the difficulties [22, 23]. Patients are not present throughout the trial, thus they must regularly and freely supply their own participation data. Informational errors and issues with patient compliance might result from this. AI can help medical research organizations and contract research organizations (CROs) overcome these obstacles in a variety of ways. In this case, regular patient compliance is the desired outcome, which might be accomplished by creating algorithms that evaluate patient data and make decisions. AI programs have the ability to assess the quality of patient data before it is accepted, which may greatly benefit patients. For example, a photograph may be analyzed by an AI system to see if it fits the requirements for clinical research [24]. After that, it can offer suggestions to the patient on how to enhance the quality of the shot they took, including modifying the lighting or the perspective. As a result, fewer submissions are incomplete or badly written, which lowers the amount of errors made while processing the data snapshot, such as how to change the lighting or the angle at which they took it. This lowers the quantity of badly written or incomplete submissions, which lowers the quantity of errors that occur during data processing.
Biosimulation:
One of the most important aspects of clinical research is testing for drug safety and effectiveness. Biosimulation can be used by researchers to conduct digital human tests and assess the drug's effects before it is ever tested on humans [20]. The process of simulating biological systems and processes is known as biosimulation. Researchers may utilize the predictions the simulation makes based on data and models utilizing AI and machine learning to learn more about the effects of the medicine. Biosimulation models use AI algorithms to examine drug-patient-demographic-trial parameter interactions and spot trends in clinical trials. With the use of these models, scientists may investigate issues such as population-level effectiveness, drug interactions, and ideal dosage. One example is the BIOiSIM platform from VeriSIM Life, which simulates the impact of chemicals on specific organs and whole-body systems using AI and ML [25].
Imperfect databases:
The intrinsic bias in research datasets is one of the primary issues facing AI. In medical research and genetic databases, patients of European and Caucasian heritage are overrepresented [26, 27]. Medical research is severely lacking in diversity because it frequently sees white, able-bodied people as the "default." An AI trained on these datasets is therefore inadequately knowledgeable about these groups, given that they constitute a substantial portion of the population yet have traditionally been underrepresented. This results in biased conclusions that might not be applicable to patient pools that do not contain those categories or to those groups themselves. Despite its promise to transform clinical trials, artificial intelligence currently confronts a number of challenges. Many clinical studies still often request patient data by fax, and hospitals frequently reply with PDFs or images (even images of handwritten notes) [28].Unstructured data can also be produced using various communication methods. For example, most of the original structure of a spreadsheet is lost when it is faxed or transformed to a read-only document (such as a PDF). With the present manual technique, researchers conducting clinical trials find it difficult to gather the precise information needed to determine a patient's eligibility [29, 30].
Patient recruiting using data mining:
Recruitment is a critical stage in clinical trials and medication development. Clinical trials fail if research groups are unable to find enough participants in a timely manner or if their recruitment efforts are unsuccessful. AI can help identify the kinds of people who could benefit most from taking part in clinical research by using demographic data.[31]. Additionally, an AI software may assist in selecting the most effective patient recruitment locations by analyzing the data and identifying the countries or regions where the sickness is most prevalent. It may also search medical records in preparation for future studies. Finally, in order to ascertain the qualifying criteria, AI systems may assess the current knowledge about the illness and compare it with the characteristics of the clinical research. These prerequisites can be simplified and made accessible to prospective study subjects.
Cost-effectiveness and ease of access:
The introduction of new technology is frequently accompanied with price tags. Supply may be scarce in the early phases of adopting new technology, which might raise the price of purchase or rental. Once it is on the equipment market, it could also be costly to make in large quantities. Furthermore, it's possible that many CROs and hospitals lack access to this technology. AI technology may only be produced and distributed by a small number of companies.
Automate Document Review
AI can rapidly examine and remove particular from huge capacity of clinical trial documents (eg. Trial protocols, medical records, consent forms).
Optimize Protocol Design
AI encourage in designing improved clinical trial protocols by: -
Patient Recruitment
Enlisting the right patients is many times the hardest part of a trial. AI upgrade this by: -
Real-time Safety Monitoring:
AI systems can constantly monitor participant data from wearable devices and another digital health technologies to observe unfavorable events or safety issues instantly.
Digital Twin Models
The term "digital twin" refers to a computer-made copy of a person or machine. In clinical trials: -
Treatment Response Prediction
AI can analyze patterns in patient data (genomics, biomarkers, clinical history) to predict: -
Difficulties with AI:
The introduction of new technologies will undoubtedly be fraught with difficulties and issues. This is especially true when it comes to a complex technology like artificial intelligence that is always developing and getting better. Even though AI technology has been shown to be beneficial in population selection and enrollment, integrating it into clinical trials remains challenging. The range of formats and quality levels of medical record data make it difficult to effectively use AI to generate new data sets. A unified global approach to data collection and use would be fantastic. Creating a framework for data organization and storage is essential to the development of AI. Technology will progress and digital health solutions will be strengthened as a result. The inherent bias in the data AI utilizes is another issue it must address. An algorithm that is trained on such datasets runs the risk of leaving out sizable portions of the population who have historically been underrepresented.
Recent collaborations of industry with AI and clinical trials:
Takeda: To develop novel medications, Takeda has also collaborated with AI firms. Prome the US Biosciences partnered with Takeda to conduct research and provide novel IBD medicines [32]. Using their respective firms' distinct bioinformatics discovery platforms and state-of-the-art machine learning techniques, Takeda and Prometheus Biosciences have partnered to develop up to three targeted treatments and companion diagnostics. Furthermore, a successful partnership with Recursion was formed in January 2020. In less than 18 months, its collaboration with Takeda in the rare disease sector has resulted in the analysis of preclinical and clinical molecules in over 60 different indications and the discovery of new therapy options for several conditions. In May 2020, Recursion was granted a license to use TAK-733 (REC-4881), a MEK inhibitor that is now undergoing clinical development for the treatment of inherited cancer syndrome and related oncological disorders [the discovery of new therapy alternatives for several illnesses in less than 18 months. In May 2020, Recursion received a license for TAK-733 (REC-4881), a MEK inhibitor that is being developed clinically to treat inherited cancer syndrome and related cancer disorders [33].
BMS or Bristol-Myers Squibb: Beginning in July 2020, BMS and ReviveMed collaborated to use their AI platform to study how immunotherapies affect cancer patients and how resistance to them develops [34]. In October 2020, insitro became a partner. insitro is a business that uses machine learning to speed up drug finding and development. [35]. The five-year agreement aims to develop and discover novel medications to treat frontotemporal diseases and amyotrophic lateral sclerosis. In the same year, Sensyne Health and BMS partnered to apply machine learning (ML) to investigate the emergence of myeloproliferative neoplasms, a class of rare blood disorders [36].
Saama: Saama, a company that offers AI and ML-based solutions that speed up clinical research and commercialization, has expanded its offering of bespoke solutions and services by introducing its unified platform of SaaS-based products. Sponsors of clinical studies. When using Saama's state-of-the-art technologies, CROs can save up to 90 minutes per query-on-query identification and generation, as well as up to 50 minutes on data transformation, 35 minutes on data input to analysis, and more. Using its proven AI and ML-enhanced solutions, Saama's new platform streamlines crucial clinical research phases and offers a comprehensive overview of trial operations and patient status updates. The high expense of developing new therapeutics, the time and resource restrictions needed to launch further therapies, the quickly increasing amount and velocity of patient data, and the talent gap that impedes the development of potentially life-saving treatments are just a few of the many challenges facing clinical research and development today. Saama's platform uses AI and big data analysis to automate resource-intensive clinical development procedures, enabling life science organizations to boost productivity and gain a deeper understanding of patient behaviours and reactions in real time. Through the use of AI and big data analysis, Saama's platform automates resource-intensive clinical development procedures, enabling life science organizations to boost productivity and gain a deeper understanding of patient behavior and reactions in real time. Years and a vast amount of data are needed to train AI models accurately. Having worked on more than 300 million data points and developed more than 90 models tailored to the life sciences, Saama has over ten years of expertise in AI development. Since these models are built directly into Saama, it will be simple to release updates to the platform and its offerings as it expands and changes to satisfy user needs [37].
Other companies: The utilization of linked devices in real-time research may enhance medication compliance. A mobile app that provides doctors with patient-reported data, dosage monitoring, educational materials, and reminders was published by Health (previously Pillsy) [38]. In August 2020, the firm, which has repositioned as a platform for remote patient monitoring, raised $15 million in a Series A funding round.
Certain approaches focus on gathering biometric data. The AliveCor wearable EKG device may detect abnormal heart rhythms like atrial fibrillation (AF) by applying machine learning (ML) to real-time data [39]. In order to enable remote clinical trials in cardiology, the company started collaborating with Medable in April 2020. AliveCor concluded a $65 million Series E fundraising round in November.
ADVANTAGES:
Protocol design: AI's ability to analyze large datasets has the potential to completely transform protocol design. These datasets may originate from prior clinical trials, medical records, and empirical data.
Participant recruitment: AI might use electronic medical records to find qualified patients. Patients could then be matched with study criteria.
Data generation: In order to model and simulate trial scenarios, artificial intelligence creates synthetic data. Additionally, algorithms can be trained without jeopardizing patient privacy.
Imaging: Medical picture analysis in clinical trials is improved by AI.
Risk and safety: In clinical trials, AI may make proactive risk monitoring and safety management possible.
Supply chain: AI helps figure out future demand, so supplies can be delivered better. Additionally, it may oversee inventory and guarantee the prompt delivery of vital trial supplies.
Optimized Protocol Development: AI creates effective methods by analyzing trial data from the past.
Improved Patient Recruitment: makes it possible for regimens to be flexible and adapt to patient responses in real time.
Adaptive Trial Design: makes it possible for regimens to be flexible and adapt to patient responses in real time.
Patient Recruitment and Retention
Data Management and Analysis
Cost and Time Efficiency
Patient Safety and Outcome Prediction
Regulatory and Compliance Support
DISADVANTAGES:
Recently, there has been a lot of talk about using AI to clinical trials and healthcare. Even while AI has the potential to completely transform many aspects of clinical research, it is crucial to understand its limitations and challenges be recognized. The following explains the main AI limitations in clinical studies. Artificial intelligence (AI) systems can sort through masses of data and make predictions about what might happen next without human judgment. They are unable to account for human abilities such as medical expertise, common sense, and intuition, though. Decision-making in clinical trials usually requires taking into account a number of factors, such as patient history, comorbidities, and potential confounding variables. AI models run the danger of overlooking important contextual nuances and elements that could influence a study's outcome. The accuracy and reliability of AI models are significantly impacted by the quality and variety of training data., or otherwise unrepresentative training data may compromise the AI model's predictions and generalizability. Furthermore, the effectiveness of AI models in clinical trial settings may be hampered by the absence of data on rare diseases or conditions. When AI is employed in clinical research, regulatory framework ambiguities and complexity are increased. The FDA and other regulatory bodies are still developing rules and guidelines for AI-driven healthcare solutions. Validating and comprehending AI model findings in a way that meets regulatory standards can be challenging because doing so typically calls for thorough testing, validation, and justification of the underlying algorithms. Concerns about data security, privacy, and informed consent persist in the context of clinical research powered by AI. Integrating AI into clinical research raises significant ethical concerns that need to be taken into account. Patients may not fully understand how the AI model operates or how their data will be utilized, making it challenging to obtain their informed consent when AI algorithms are implemented. AI models must be clear and simple to use in order to gain patients' trust and uphold a high standard of moral behavior. Integrating AI technology with current clinical trial processes and systems could be challenging and time-consuming. Clinical trials are important to a wide range of stakeholders, including government organizations, physicians, patients, and scientists. AI adoption necessitates significant changes to processes, systems, and staff training. There is frequently a steep learning curve involved in adopting and maintaining AI systems, and those who are sceptical about or uninformed about AI may be resistant to the integration process. Deep learning neural networks are among the many AI systems that are referred to as "black box" models since it is challenging to comprehend and describe how they operate within. This lack of interpretability could impede widespread adoption because it is frequently difficult to understand how an AI model came to a certain conclusion or recommendation. The ability to justify and defend decisions taken during clinical trials is essential for patient safety, regulatory compliance, and technology trust. The ability of AI models trained on specific datasets to generalize and adjust to new data or populations has drawn criticism. Due to the wide range of participants in clinical trials, AI models created and trained on one patient or institution may not function as effectively when applied to different populations or circumstances. Although AI has demonstrated potential in clinical trials, its application and scalability may be limited by its lack of generalizability and transferability. In summary, clinical trials could be significantly enhanced by AI, but its drawbacks must be considered. In order to overcome these obstacles, researchers must collaborate and thoroughly consider the moral, legal. Advantages and disadvantages of AI is given in the following table 1.
Advantages and Disadvantages of using Artificial Intelligence (AI) in Clinical Trials: -
|
Table 1: Advantages and Disadvantages of Artificial Intelligence (AI) in Clinical Trials |
|
|
Advantages |
Disadvantages |
|
|
|
|
|
|
|
|
|
|
FUTURE GOAL:
Clinical trials are changing in almost every way because to AI. AI has a significant and wide-ranging impact on everything from improving patient monitoring and data analysis to creating smarter studies. AI is having a major impact on a number of important fields, including: -
Trial Planning and Enhancement, Safety monitoring and adverse event management, Regulatory compliance and documentation, Data management and analysis, Improvements in patient recruitment and retention. The combination of AI with cutting-edge technologies like blockchain to improve data security and transparency is one fascinating area of research. Researchers, participants, and regulators may all have more faith in tamperproof trial records produced by this combination. Advances in multi-omics and genomes data will enable AI to plan clinical trials with previously unheard-of accuracy. With AI, more individualized and efficient treatments will be provided by customizing therapies to each patient's unique genetic profile. Some analysts predict that clinical trials will eventually become completely independent. With little assistance from humans, AI systems will manage all aspect of this vision, from planning the experiment and finding volunteers tracking developments, evaluating data, and producing reports [40]. The three areas of optimization, facilitation, and simulation were the subject of discussions and viewpoints about how artificial intelligence (AI) might affect the planning and execution of clinical trials. The delegates envisioned how the historical data on clinical trials may be optimized. This data will be utilized to cut down on the amount of time now spent preparing protocols, eliminate errors and the need for revisions, and assist clinical teams in choosing the best biomarkers, measures, milestones, and endpoints [41]. Clinical trials will be established by combining future AI with improved advances in computer simulation and tailored healthcare [42]. Virtual trials use the power of contemporary digital technology to lower expenses, delays, and challenges for patients. This would speed up clinical development and improve patient retention, potentially supporting up to 50% of all studies through virtual trials. Artificial intelligence will save human labour, time, and money. Big pharmaceutical firms are now beginning to make AI investments. The application of artificial intelligence in research projects could possibly expand, though. Research using AI is conducted more rapidly, securely, and economically.[43].
RESULTS
1. Patient Recruitment and Retention
AI can analyze electronic health records (EHRs), demographic data, and genetic profiles to identify eligible participants more efficiently. AI-based recruitment improves enrollment speed, diversity, and participant retention.
2. Protocol Optimization
AI helps design effective clinical trial protocols by analyzing previous trial data, predicting dropout rates, and optimizing inclusion and exclusion criteria.
3. Biosimulation
AI-powered biosimulation models predict drug behavior and interactions before human testing, reducing risks and improving drug development efficiency.
4. Data Management and Analysis
AI automates data collection, detects missing or inconsistent entries, and enables real-time monitoring of clinical outcomes and adverse events.
5. Decentralized Clinical Trials
AI supports remote patient monitoring through wearable devices and mobile applications, improving accessibility and reducing trial costs.
6. Treatment Response Prediction
AI analyzes biomarkers, genomics, and patient history to predict treatment responses and support personalized medicine.
7. Safety Monitoring
AI systems continuously monitor patient data and rapidly identify adverse events, improving patient safety and regulatory compliance.
8. Industry Collaborations
Several pharmaceutical companies such as Takeda, Bristol Myers Squibb, and Saama have collaborated with AI firms to accelerate drug discovery and clinical trial processes.
DISCUSSION
AI has significantly transformed clinical trial management by improving efficiency, reducing operational costs, and enabling faster drug development. Traditional clinical trials often face challenges such as delayed patient recruitment, high dropout rates, protocol deviations, and massive data handling requirements. AI technologies help address these issues by automating repetitive tasks and enabling data-driven decision-making. Machine learning algorithms can process large datasets and identify hidden patterns that may not be visible through conventional analysis methods. AI-driven patient recruitment systems improve trial enrollment by identifying suitable candidates from EHRs and genomic databases. This reduces delays and increases the probability of successful trials. Another important advancement is the use of decentralized clinical trials, where patients can participate remotely using digital devices and wearable technologies. AI helps monitor patient compliance and health status in real-time, reducing the need for frequent hospital visits. Despite these advantages, AI implementation in clinical trials faces several limitations. Data privacy, informed consent, algorithm bias, lack of transparency, and regulatory uncertainties remain major concerns. AI systems trained on biased datasets may produce inaccurate or unfair outcomes for underrepresented populations. Furthermore, integrating AI into existing healthcare systems requires substantial infrastructure investment and skilled personnel. The future of AI in clinical trials appears highly promising. Integration with blockchain technology, digital twins, and personalized medicine may further improve transparency, security, and treatment accuracy. As regulatory frameworks become more standardized, AI is expected to play a central role in future drug development and healthcare research.
CONCLUSION
Clinical trials could be made more effective, more affordable, and of higher quality with the help of artificial intelligence (AI) and machine learning (ML). By enhancing recruitment, participant retention, compliance, and data analysis, these technologies can accelerate trial timelines and improve patient outcomes. AI also enables automation and access to previously unavailable insights, positioning it as a transformative tool in the drug development value chain. Despite this potential, several critical challenges remain. These include ethical concerns like bias, informed consent, and data privacy, as well as technical issues such as data quality and standardization. Regulatory bodies like the FDA and other international agencies must provide clearer guidelines to ensure transparency, oversight, and safety in AI/ML-driven clinical processes. Until such frameworks are in place, the interest in applying ML in clinical trials is likely to outpace its actual implementation. Looking forward, as AI capabilities mature and regulatory standards evolve, more sophisticated methods will become available to streamline drug development. These advancements can allow companies to access broader participant pools, reduce costs, reuse data more efficiently, and improve overall trial success rates. AI’s integration into personalized medicine also presents immense promise, offering targeted treatments based on individual patient data. However, broad adoption requires addressing lingering challenges related to data governance, ethical considerations, and industry skepticism. In summary, while AI/ML can revolutionize clinical trial management and drug development, realizing their full potential will depend on resolving key technical, ethical, and regulatory hurdles.
REFERENCES





Ganesh Waghmare, Kanishka Shamatkar, Falguni Thakare, Abhijit Raut, Suraj Yadav, Artificial Intelligence in Clinical Trials: Current Applications, Challenges, and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 6811-6829, https://doi.org/10.5281/zenodo.20928780
 10.5281/zenodo.20928780
10.5281/zenodo.20928780