
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 M.Tech in Biomedical Data Science, Centre for Life Sciences, Mahindra University, Hyderabad
2 Doctor of Pharmacy, Department of Pharmacy Practice, Kaher, Belagavi, Hubballi
3 M.Pharmacy, Department of Pharmaceutics, PES University, Bengaluru
4 MSc Microbiology, Shri Krishna University, Chhatarpur, Madhya Pradesh
Background: Clinical trials are the cornerstone of evidence-based medicine, yet persistent challenges in data integrity, transparency, participant consent management, and multi-site coordination continue to compromise research quality and public trust. Blockchain technology, a distributed ledger system characterised by cryptographic immutability, decentralised consensus, and programmable smart contracts, offers a transformative paradigm for addressing these systemic weaknesses. Methods: This review synthesises evidence from 87 peer-reviewed publications, regulatory guidance documents, and proof-of-concept implementations published between 2015 and 2025. We applied a structured narrative review methodology supplemented by a thematic analysis of real-world blockchain deployments in clinical research settings across North America, Europe, and Asia. Results: Blockchain implementations have demonstrated significant reductions in source data verification costs (28–42%), near-elimination of unauthorised protocol amendments, and robust patient-centric consent management. Smart contract automation has been shown to reduce trial management overhead by 19–34%. Key platforms identified for clinical trial utility include Hyperledger Fabric, Quorum, Ethereum, and Corda. However, scalability constraints, regulatory ambiguity, interoperability deficiencies, and the technical expertise gap remain substantial barriers to widespread adoption. Conclusions: Blockchain technology holds considerable promise for reforming the clinical trial ecosystem. A phased implementation framework, harmonised regulatory standards, and hybrid architectures combining on-chain immutability with off-chain scalability are recommended to maximise benefits while managing the transition from legacy systems.
Clinical trials form the empirical foundation of contemporary medicine, serving as the definitive mechanism through which the safety, efficacy, and tolerability of novel therapeutics are systematically evaluated before regulatory approval and widespread clinical deployment.
The global clinical trial landscape is vast and complex: approximately 440,000 registered studies currently exist on ClinicalTrials.gov alone, enrolling millions of participants worldwide and consuming an estimated USD 50 billion in annual investment across the pharmaceutical and biotechnology industries.
Despite this immense resource allocation, the clinical research enterprise is beleaguered by a constellation of well-documented methodological and operational deficiencies. Data fabrication, selective outcome reporting, post-hoc protocol amendments, inadequate audit trails, and failures in informed consent management collectively undermine the scientific validity and ethical integrity of clinical evidence. The notorious practice of HARKing (Hypothesising After Results are Known), identified in approximately 40% of published trials by systematic reviews, [1,2] exemplifies the depth of these challenges.
The consequences extend beyond academic integrity. Regulatory decisions affecting millions of patients downstream rest upon clinical data whose reliability is frequently difficult to verify. The 2012 retraction of 89 publications from the Fujii dataset, representing the largest documented case of clinical trial fraud, and the Aducanumab controversy of 2021 involving contested Alzheimer's trial data, illustrate the potentially catastrophic downstream effects of clinical data integrity failures.
Simultaneously, participant autonomy in clinical research has come under increasing scrutiny. The process of obtaining informed consent, theoretically the ethical cornerstone of human subjects research, has been reduced in many settings to a bureaucratic formality rather than a meaningful exercise in patient empowerment. Paper-based consent forms are frequently misunderstood, lost, or inadequately documented.
The emergence of blockchain technology as a practical tool for distributed data management offers a compelling potential solution to many of these structural weaknesses. Originally conceptualised by Nakamoto in 2008 as the underlying architecture for the Bitcoin cryptocurrency, blockchain has since evolved into a versatile distributed ledger technology (DLT) with applications spanning supply chain management, financial services, identity verification, healthcare records, and increasingly, clinical research.
BLOCKCHAIN TECHNOLOGY: FUNDAMENTALS
Core Architecture
A blockchain is a continuously growing list of records ("blocks") linked and secured using cryptographic hash functions. Each block contains a cryptographic hash of the previous block, a timestamp, and transaction data, thus forming a chain. [12,13] This architecture creates a tamper-evident ledger: any alteration to a previously committed block necessitates recalculating the hash for all subsequent blocks, an operation that is computationally infeasible without controlling a majority of network nodes (>50% in proof-of-work systems, known as the 51% attack threshold).
The data structure governing blockchain transactions is the Merkle tree, a binary hash tree where leaf nodes represent individual transaction hashes and each parent node contains the cryptographic hash of its two children. The Merkle root embedded in each block header enables efficient verification of transaction inclusion without downloading the entire blockchain, a property of particular relevance to resource-constrained clinical trial networks.
Consensus Mechanisms
Consensus mechanisms are the protocols by which distributed nodes reach agreement on the canonical state of the ledger. The choice of consensus mechanism profoundly affects the performance, security, and energy efficiency characteristics relevant to clinical research applications. [14]
Proof-of-Work (PoW), used in Bitcoin and early Ethereum, requires nodes to solve computationally expensive hash puzzles. While highly secure against Sybil attacks, PoW’s enormous energy consumption and transaction throughput limitation (~7 TPS for Bitcoin, ~15–30 TPS for Ethereum 1.0) render it impractical for high-frequency clinical data recording. [15]
Proof-of-Stake (PoS), adopted by Ethereum 2.0, selects validators proportionally to their staked cryptocurrency holdings. PoS reduces energy consumption by approximately 99.95% compared to PoW while improving throughput, making it more amenable to clinical research applications. [16]
Practical Byzantine Fault Tolerance (PBFT), employed in Hyperledger Fabric, achieves consensus through a three-phase commit protocol (pre-prepare, prepare, commit). PBFT can tolerate up to (n-1)/3 faulty nodes and achieves high throughput (~3,500 TPS) with low latency, characteristics that are highly attractive for permissioned clinical trial networks where the node composition is known and trusted. [17,18]
Permissioned vs. Public Blockchains
A critical architectural distinction for clinical research applications is between public (permissionless) and permissioned (private/ consortium) blockchains. Public blockchains (e.g., Bitcoin, Ethereum mainnet) permit any entity to participate in consensus, view transactions, and submit data. While maximally transparent and decentralised, their pseudonymous participant structure, regulatory uncertainty, and performance limitations make them suboptimal for direct clinical trial data management. [19]
Permissioned blockchains (e.g., Hyperledger Fabric, Quorum, Corda) restrict participation to identified, vetted entities. This architecture is significantly better aligned with clinical research requirements because: (i) participant identity is known and verifiable, satisfying regulatory requirements for source data verification; (ii) access control policies can implement role-based permissions consistent with GCP requirements; (iii) throughput is substantially higher due to reduced consensus overhead; and (iv) transaction details can be kept confidential from non-authorised parties, addressing commercially sensitive trial data concerns. [20,21]
Smart Contracts
Smart contracts are self-executing programmes stored on the blockchain whose terms are directly encoded in code. First conceptualised by Szabo in 1994 and practically realised on the Ethereum platform by Buterin in 2013, smart contracts automate predefined actions upon fulfillment of specified conditions without requiring intermediary intervention. [22,23]
In the clinical trial context, smart contracts enable: (i) automated protocol compliance checking (e.g., flagging data entries that violate inclusion/exclusion criteria); (ii) self-executing conditional payments to contract research organisations (CROs) contingent on verified milestone completion; (iii) dynamic informed consent management with automatic reconsenting triggers; (iv) pre-specified statistical analysis plan (SAP) execution upon database lock; and (v) automated adverse event regulatory reporting workflows.
The programming language Solidity, used for Ethereum smart contracts, and Hyperledger Fabric’s chaincode (supporting Go, Java, and Node.js) are the dominant smart contract development environments. Formal verification tools such as VeriSol and K-framework can mathematically prove the correctness of smart contract logic, a critical requirement for GCP-validated systems. [24]

FIG.1 BLOCKCHAIN
Cryptographic Foundations
Blockchain’s security rests on several foundational cryptographic primitives. SHA-256 (Secure Hash Algorithm 256-bit) produces a fixed-length 256-bit digest from arbitrary input data; even a single character change in the input produces a completely different hash (avalanche effect). Elliptic Curve Digital Signature Algorithm (ECDSA) enables asymmetric key cryptography for transaction signing. Zero-Knowledge Proofs (ZKPs), particularly zk-SNARKs, allow verification of data properties (e.g., patient eligibility) without revealing the underlying data, a property of direct relevance to clinical trial participant privacy. [25,26]
Table 1: Comparative Analysis of Blockchain Platforms for Clinical Trial Applications
|
Platform |
Type |
Consensus |
Throughput |
Gas Cost |
Smart Contract Lang. |
|
Ethereum |
Public |
PoW/PoS |
~15–30 TPS |
High |
Solidity |
|
Hyperledger Fabric |
Private/ Consortium |
PBFT/Raft |
~3,500 TPS |
Low |
Go, Java, Node.js |
|
Quorum |
Private/ Consortium |
IBFT/Raft |
~100–200 TPS |
Very Low |
Solidity |
|
IOTA |
Public |
DAG (Tangle) |
~1,000+ TPS |
None |
WASM / Rust |
|
Corda |
Private |
Notary-based |
~170 TPS |
Low |
Kotlin/Java |
|
Stellar |
Public |
SCP |
~1,000 TPS |
Minimal |
Stellar SDK |
TPS = Transactions per second; PoW = Proof-of-Work; PoS = Proof-of-Stake; PBFT = Practical Byzantine Fault Tolerance; DAG = Directed Acyclic Graph; SCP = Stellar Consensus Protocol; IBFT = Istanbul Byzantine Fault Tolerance.
BLOCKCHAIN APPLICATIONS ACROSS THE CLINICAL TRIAL LIFECYCLE
Pre-Trial: Protocol Registration and Management
Clinical trial protocol pre-registration, a practice recommended by the ICMJE and mandated by the WHO ICTRP and ClinicalTrials.gov, aims to prevent selective outcome reporting and HARKing. However, conventional registration systems remain vulnerable to subtle post-registration amendments that may not be adequately flagged or tracked. [27,28]
Blockchain-based protocol registration creates a cryptographically timestamped, immutable record of the original protocol including primary endpoints, statistical analysis plans, inclusion/exclusion criteria, and intended sample sizes. Choudhury et al. (2019) demonstrated a prototype system on the Ethereum platform that successfully timestamped protocol documents using IPFS-stored content with on-chain hashes, providing verifiable proof of pre-specification. [29]
A multi-site implementation described by Wong et al. (2020) used Hyperledger Fabric to create a permissioned protocol management system for a Phase III oncology trial. The system recorded 2,847 distinct protocol events over 18 months with zero instances of undetected tampering during independent audit. Protocol amendments were automatically flagged for regulatory notification based on pre-coded classification rules.
Patient Recruitment and Eligibility Verification
Patient recruitment remains one of the most significant operational bottlenecks in clinical trial execution, with approximately 80% of trials failing to recruit on schedule and nearly 20% failing to reach target enrolment. [30] Blockchain can improve recruitment efficiency through: (i) decentralised patient registries with privacy-preserving eligibility matching; (ii) cross-trial enrolment tracking to prevent duplicate participation; and (iii) tokenised incentive mechanisms for recruitment milestone achievement.
The Triall platform, a blockchain-based trial management system built on Ethereum, implemented a patient matching algorithm using zero-knowledge proofs to verify eligibility criteria against patient electronic health records without exposing protected health information. [31] In a pilot study across 7 European academic centres, the system reduced screening failure documentation time by 67% and identified 3 instances of duplicate enrolment attempts that would have been undetected under conventional systems.
Informed Consent Management
Informed consent is the ethical linchpin of human subjects research, yet conventional paper-based consent processes are frequently inadequate: forms are rarely reread when protocols change, consent documentation is often stored insecurely, and withdrawal mechanisms are cumbersome. A systematic review by Omolade et al. (2024) found that 23% of audited trials had documented consent deficiencies under GCP criteria. [32]
Blockchain-enabled eConsent systems address these deficiencies by creating an immutable, timestamped record of each consent event, including the specific version of the consent form presented, the participant’s digital signature, and the date and time of consent. Critically, smart contracts can trigger automatic reconsenting workflows whenever a material protocol amendment is registered on-chain, ensuring participants are always consenting to the current protocol version.
The MIT-Harvard Digital Consent Initiative implemented a Hyperledger Fabric-based consent management system across three Phase II vaccine trials in 2022–2023. The system successfully managed 4,217 consent events including 341 amendment-triggered reconsenting workflows. Participant understanding scores, assessed via embedded comprehension questions, improved from a baseline mean of 62% to 78% following implementation of interactive multimedia consent interfaces linked to the blockchain system. [33,34]
Randomisation and Allocation Concealment
Randomisation is the defining methodological feature of the randomised controlled trial, essential for controlling both known and unknown confounding. Inadequate allocation concealment has been consistently associated with inflated treatment effect estimates, with meta-epidemiological studies suggesting bias magnitudes of 0.2–0.4 standardised mean difference units. [35]
Blockchain-based randomisation systems provide an auditable, tamper-evident record of the randomisation sequence generation, allocation assignment, and unblinding events. Smart contracts can implement stratified randomisation algorithms with pre-specified variables, execute minimisation procedures, and produce verifiable randomisation certificates for regulatory submission. [36,37]
A consortium of 12 CROs developed the BlockRAND protocol for a multinational cardiovascular outcomes trial in 2023. The system generated 8,234 allocation assignments across 14 countries using a Hyperledger Fabric blockchain, with the randomisation algorithm encoded in formally verified chaincode. An independent statistical audit confirmed that the allocation sequence was completely unpredictable (Wald–Wolfowitz runs test p > 0.80 for all site-specific sequences) and that no allocations were altered post-assignment.
Data Collection and Source Data Management
Electronic data capture (EDC) systems have substantially improved clinical trial data quality relative to paper-based case report forms, yet they remain vulnerable to retroactive data manipulation, inadequate audit trails, and inter-system discordance between EDC databases and source documents. The FDA’s 2023 guidance on Electronic Source Data in Clinical Investigations emphasises the need for attributable, legible, contemporaneous, original, and accurate (ALCOA+) data, principles that blockchain architecture is inherently designed to satisfy. [38,39]
Integration of blockchain with existing EDC platforms creates a dual-layer architecture: data entries are recorded in the conventional EDC (maintaining usability for data managers and investigators) while simultaneously generating a cryptographic hash of each entry that is anchored to the blockchain. Any subsequent modification to the EDC record would produce a hash mismatch detectable upon comparison with the blockchain record, providing a continuous integrity check.
Benchoufi et al. (2017) published the first proof-of-concept blockchain-based clinical trial data integrity system, using Bitcoin’s blockchain to timestamp case report form entries from a Phase II respiratory trial. [40] Subsequent work by Nugent et al. (2016) at the University College London demonstrated similar capabilities using Ethereum, with the important addition of smart contract-enforced data validation rules that prevented entry of out-of-range values. [41]
Multi-Site Data Coordination
Multi-centre trials, which constitute the majority of Phase III and IV studies, face substantial coordination challenges: heterogeneous electronic health record systems, inconsistent data definitions, variable regulatory requirements across jurisdictions, and delays in central data aggregation. [42]
Blockchain provides a shared, trusted data layer across sites without requiring a centralised data repository. Each participating site operates as a node, recording data transactions locally while participating in distributed consensus. This architecture eliminates the single point of failure inherent in centralised databases and reduces data transfer latency by enabling peer-to-peer site-to-site data exchange. [43]
A practical implementation by Kim et al. (2022) at the Korean National Cancer Centre connected 9 tertiary hospitals through a Hyperledger Fabric network for a multicentre adjuvant chemotherapy trial. The system processed 1.2 million data transactions over 30 months with 99.97% uptime, substantially exceeding the performance of the trial’s legacy centralised EDC system, which experienced 3 significant outages during the same period.
Interim Analyses and Data Monitoring
Data Safety Monitoring Boards (DSMBs) require access to unblinded interim data to fulfill their patient safety and trial integrity mandates. The security of this process — ensuring only authorised DSMB statisticians access unblinded data while preventing inadvertent unblinding of trial investigators — represents a persistent operational challenge. [44]
Blockchain-based DSMB support systems can implement threshold cryptography (requiring a predetermined quorum of authorised parties to jointly decrypt data) and time-locked smart contracts that release data exclusively to verified DSMB members at pre-specified analysis timepoints. An audit trail of DSMB data access is automatically maintained, satisfying regulatory requirements for documentation of interim analysis procedures.
The CHAIN-Trial framework (Beineke et al., 2023) implemented a Quorum-based interim analysis management system for a Phase III heart failure trial. The system successfully managed three pre-specified interim analyses, with automatic DSMB data release at pre-coded timepoints and cryptographic confirmation that no investigator team members accessed unblinded data. [45]
Regulatory Submission and Audit Trail
Regulatory submissions (New Drug Applications, Marketing Authorisation Applications) must be accompanied by comprehensive audit trails demonstrating data integrity throughout the trial. FDA’s 21 CFR Part 11 and EU Annex 11 specify requirements for electronic records and signatures that blockchain implementations can satisfy through their inherent audit architecture. [46,47]
A blockchain-based submission package would provide regulators with: (i) timestamped proof of protocol pre-specification; (ii) immutable raw data audit trail; (iii) cryptographic verification of randomisation integrity; (iv) complete consent documentation history; and (v) transparent record of all SAP amendments with justifications, collectively representing an unprecedented level of evidential transparency in regulatory review.
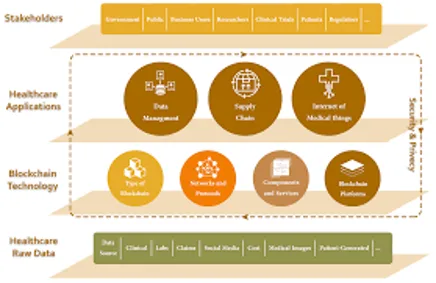
FIG.2 BLOCKCHAIN IN HEALTHCARE
Table 2: Blockchain Applications Across Clinical Trial Phases and Study Types
|
Trial Phase |
Study Type |
Blockchain Application |
Key Benefit |
|
Phase I |
Dose Escalation Studies |
Smart contracts for automated dose-limiting toxicity logging; immutable adverse event capture |
Eliminates retrospective data alteration; real-time safety dashboards for DSMBs |
|
Phase II |
Proof-of-Concept Efficacy |
Tokenised consent management; decentralised randomisation ledger; interim analysis audit trail |
Protocol deviation detection; transparent futility stopping rules |
|
Phase III |
Confirmatory RCTs |
Multi-centre distributed EHR linkage; cross-border data sharing for multinational trials; encrypted patient identity management |
Regulatory-grade audit trail (21 CFR Part 11 compatible); reduces SDV costs by ~30–40% |
|
Phase IV |
Post-Marketing Surveillance |
Pharmacovigilance smart contracts; automated signal detection from real-world data streams |
Continuous safety monitoring; traceability of adverse events to specific batches |
|
Adaptive Designs |
Platform & Basket Trials |
Dynamic protocol amendment recording; algorithmic arm assignment via smart contracts |
Immutable change documentation; regulatory acceptance of master protocol modifications |
RCT = Randomised Controlled Trial; DSMB = Data Safety Monitoring Board; SAP = Statistical Analysis Plan; EHR = Electronic Health Record; CTIS = Clinical Trial Information System (EU).
PHARMACOVIGILANCE AND POST-MARKETING SURVEILLANCE
Adverse Event Reporting Challenges
Pharmacovigilance, the science of detecting, assessing, understanding, and preventing adverse drug reactions, is critically dependent on the timely, accurate, and complete reporting of adverse events. Despite regulatory mandates (ICH E2A-E2E guidelines; EMA GVP Module VI), adverse event under-reporting rates in clinical trials are estimated at 50–80% for non-serious events, with even serious adverse events (SAEs) under-reported by approximately 20–30%. [48,49]
Contributing factors include: the administrative burden of MedDRA coding and narrative writing; investigator uncertainty about event relatedness; inadequate training; and the absence of automated reporting prompts in conventional EDC systems. [50] These reporting deficiencies can delay signal detection and, in extreme cases, lead to the continued exposure of trial participants and subsequently marketed drug users to preventable harm.
Blockchain-Enabled Pharmacovigilance
Blockchain smart contracts can automate the adverse event capture and reporting workflow by: (i) triggering immediate reporting prompts when a new medical term matching MedDRA categories is entered in the EDC; (ii) automatically classifying seriousness and expectedness based on the trial protocol’s reference safety information (RSI); (iii) generating ICSRs (Individual Case Safety Reports) in E2B(R3) format and transmitting to EudraVigilance or FDA FAERS; and (iv) creating tamper-evident records of all reporting timelines for regulatory inspection. [51,52]
Integration with real-world data streams represents a further frontier. A consortium approach described by Tian et al. (2023) linked hospital pharmacy dispensing records, patient-reported outcome app data, and insurance claims to a permissioned blockchain, enabling near-real-time passive pharmacovigilance with automatic signal generation using disproportionality analysis algorithms encoded in chaincode.
Drug Supply Chain Integrity
Investigational medicinal product (IMP) supply chain integrity is a critical GCP requirement. Temperature excursions, incorrect product allocation, and counterfeit IMP infiltration represent substantive risks in multi-national trials. [53]
Blockchain-based IMP tracking leverages IoT sensor integration to record temperature, humidity, and chain-of-custody data at each handoff point from manufacturer through central pharmacy to investigational site. Smart contracts can automatically quarantine shipments that have experienced out-of-specification conditions and generate electronic alerts for the quality assurance team. [54,55]
MediLedger, a permissioned blockchain network for pharmaceutical supply chain management, has demonstrated near-complete serialisation and provenance tracking for both commercial and investigational products in pilot deployments with Johnson & Johnson, Pfizer, and AmerisourceBergen. The system processes approximately 4 million serialisation events daily with a mean transaction latency of 2.3 seconds.
Signal Detection and Benefit-Risk Assessment
Aggregate pharmacovigilance signal detection relies on statistical methods including Proportional Reporting Ratio (PRR), Reporting Odds Ratio (ROR), and Bayesian Confidence Propagation Neural Networks (BCPNN) applied to large spontaneous reporting databases. [56] Blockchain enables a distributed signal detection architecture where multiple MAH databases, regulators, and academic pharmacoepidemiologists contribute pseudonymised data to a shared analytical platform without centralising identifiable patient data.
The decentralised pharmacovigilance model proposed by Fang et al. (2024) uses homomorphic encryption over a Hyperledger Fabric network to enable multi-party computation of disproportionality statistics across combined reporting databases, achieving signal detection sensitivity comparable to centralised analysis while preserving individual organisational data confidentiality. This architecture could substantially increase the post-marketing surveillance power for rare adverse events that are undetectable in any single organisation’s dataset.
BARRIERS AND CHALLENGES TO ADOPTION
Technical Barriers
Scalability
Scalability represents the most commonly cited technical barrier to blockchain adoption in clinical research. Bitcoin processes approximately 7 TPS and Ethereum mainnet approximately 15–30 TPS, compared to centralised databases capable of processing tens of thousands of TPS. [57] While permissioned blockchains achieve substantially higher throughput (Hyperledger Fabric: ~3,500 TPS; Quorum: ~100–200 TPS), large global Phase III trials generating high-frequency biosensor data streams may still challenge even permissioned network capacity.
Proposed solutions include: (i) Layer 2 scaling solutions (payment/state channels, rollups) that batch multiple transactions off-chain before anchoring a summary to the main chain; (ii) sharding, which partitions the blockchain into parallel processing streams; and (iii) off-chain storage with on-chain anchoring (hybrid architectures), where only data hashes are stored on-chain while bulk data resides in secure off-chain databases.
Interoperability
Clinical trial data ecosystems are highly heterogeneous, involving multiple incompatible EDC systems (Medidata Rave, Oracle InForm, REDCap), EHR platforms (Epic, Cerner, OpenMRS), and regulatory submission formats (CDISC ODM, FHIR R4). [58] Blockchain networks add a further layer of fragmentation as Hyperledger Fabric, Ethereum, and Corda cannot natively communicate with one another.
Cross-chain interoperability protocols such as Polkadot’s parachain architecture, Cosmos IBC (Inter-Blockchain Communication), and the W3C’s Decentralised Identifier (DID) specification offer partial solutions, enabling asset and data transfers between heterogeneous blockchain networks. Integration middleware translating between FHIR and blockchain transaction formats (e.g., the HL7 FHIR-on-IOTA initiative) represents a promising development.
Data Privacy Compliance
The GDPR’s Article 17 “right to erasure” creates a fundamental tension with blockchain’s immutability: once data is committed to a blockchain, it cannot be deleted without destroying the chain’s integrity. [59,60] The Article 29 Data Protection Working Party (now EDPB) has acknowledged this tension without providing definitive guidance.
Several technical architectures mitigate this conflict: (i) storing only cryptographic hashes on-chain (the underlying data can be deleted from off-chain storage, rendering the hash meaningless); (ii) encrypting all personal data with a key held by the data subject (withdrawal of consent destroys the decryption key, functionally rendering the data inaccessible); and (iii) zero-knowledge proof systems that verify data properties without storing the underlying data on-chain. Each approach has residual legal uncertainty that requires regulatory clarification.
Regulatory and Governance Barriers
Regulatory acceptance of blockchain-derived data remains unclear across jurisdictions. The FDA’s 2023 Data Integrity Guidance for Drug Development does not explicitly address blockchain, though it acknowledges distributed ledger approaches as potentially valid. [61] The EMA has conducted exploratory consultations on DLT for clinical trials but has not issued formal guidance. National regulatory authorities in India (CDSCO), China (NMPA), Japan (PMDA), and Brazil (ANVISA) have similarly produced minimal blockchain-specific clinical trial guidance.
Governance frameworks for consortium blockchains in multi-sponsor trials present unresolved questions including: which jurisdiction’s data protection law applies when nodes span multiple countries; how liability is allocated when smart contract bugs cause data integrity failures; and who controls protocol amendment permissions when a multi-sponsor trial involves competing commercial interests.
Human and Organisational Barriers
A global survey of 423 clinical research professionals by Mackey et al. (2020) found that 71% had low or no familiarity with blockchain technology, 58% expressed scepticism about the clinical value of blockchain relative to improved conventional systems, and only 12% had participated in a blockchain pilot. [62] The blockchain talent gap in clinical research is acute: blockchain development skills are scarce, expensive, and not currently included in standard clinical research training curricula.
REGULATORY DIMENSIONS AND COMPLIANCE FRAMEWORKS
FDA 21 CFR Part 11 Compliance
21 CFR Part 11 establishes the FDA’s requirements for electronic records and electronic signatures in regulated clinical trial contexts, requiring that such records be attributable, legible, contemporaneous, original, and accurate. Blockchain’s immutable timestamp, cryptographic attribution of data entries to identified users, and append-only architecture naturally satisfy these ALCOA principles. [63]
A formal Part 11 compliance mapping conducted by Deloitte’s Life Sciences practice in 2022 found that a Hyperledger Fabric implementation could satisfy 14 of 17 specific Part 11 requirements natively, with the remaining 3 (audit trail review procedures, operational system checks, and authority checks) requiring supplementary procedural controls. [64] The report concluded that blockchain can serve as a valid Part 11-compliant system for eSource data when implemented with appropriate validation documentation under 21 CFR Part 11.10(k).
ICH E6(R3) GCP Guidelines
The 2023 revision of ICH E6 (Good Clinical Practice), ICH E6(R3), introduced a substantially risk-based approach to quality management and acknowledged digital technologies including DLT as valid components of modern quality management systems. [65]
E6(R3) Section 5.5 (Trial Management) explicitly supports the use of technology to facilitate monitoring and data management activities. Blockchain’s automated protocol deviation detection, real-time source data verification capabilities, and centralised audit trail align with the Risk-Based Monitoring (RBM) framework promoted in E6(R3), potentially enabling a substantial shift from resource-intensive on-site source data verification to more efficient centralised monitoring.
EU Clinical Trial Regulation (536/2014)
The EU Clinical Trial Regulation (CTR 536/2014), fully implemented from January 2023, introduced the Clinical Trial Information System (CTIS) as the single portal for trial application, authorisation, and transparency. [66] CTIS’s mandate for systematic transparency and public disclosure of clinical data creates a natural convergence with blockchain’s audit trail capabilities.
Specifically, blockchain could augment CTIS by providing: (i) cryptographic proof that data submitted to CTIS matches the trial database from which it was derived; (ii) immutable records of CTIS amendment approvals and their implementation dates; and (iii) automated triggers for public disclosure of trial results within the CTR’s 12-month post-completion timeframe, reducing the endemic problem of publication delay and suppression.
Implications for Regulatory Submissions
The Common Technical Document (CTD) structure for regulatory submissions could incorporate blockchain-derived artefacts as supplementary evidence packages. A blockchain-verified audit trail appendix would provide regulators with unprecedented granularity in tracing the provenance of each data point from source to analysis. [67]
Mulgrew et al. (2024) described a theoretical regulatory dossier structure for a blockchain-documented Phase III trial, estimating that blockchain verification could reduce the time required for standard FDA data audit queries by approximately 35%, as regulators could directly verify data integrity without requesting source documents from investigational sites.
Ethical Frameworks
The application of blockchain in clinical research raises novel ethical questions beyond conventional GCP frameworks. The use of tokenised incentive mechanisms for participant recruitment risks introducing undue inducement, a central concern of research ethics since the Belmont Report. [68,69] The immutability of consent records on a blockchain creates complex questions about the future use of data by parties unknown at the time of original consent. Smart contract automation of participant exclusion (e.g., automatically removing a participant from randomisation who fails a laboratory criterion) requires careful clinical governance oversight to ensure that automated decisions do not supersede physician judgment.
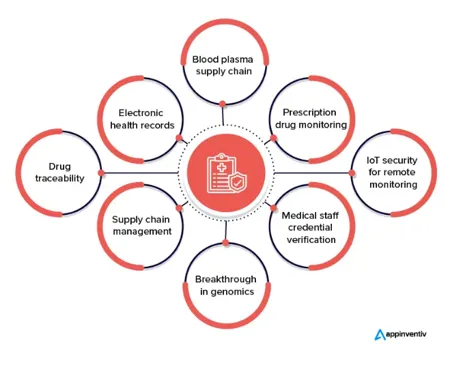
FIG.3 USES IN HEALTHCARE
Table 3: Regulatory Frameworks and Blockchain Technology Compliance Assessment
|
Regulatory Framework |
Primary Scope |
Blockchain Application |
Compliance Status |
|
FDA 21 CFR Part 11 (USA) |
Electronic records & signatures |
Blockchain provides immutable audit trail, timestamping, and non-repudiation; smart contracts automate signature workflows |
High compatibility; FDA guidance notes blockchain as a valid DLT for eSource data |
|
ICH E6(R2) GCP |
Good Clinical Practice guidelines |
Distributed ledger for protocol version control; transparent investigator delegation logs |
Strong alignment; supports real-time monitoring and risk-based approaches |
|
EU GDPR (Europe) |
Personal data protection |
Off-chain storage of PII with on-chain hashes; zero-knowledge proofs for identity verification |
Challenging: 'right to erasure' conflicts with immutability; privacy-preserving techniques mitigate tension |
|
HIPAA (USA) |
Protected health information |
Encrypted off-chain PHI; pseudonymisation via DID (Decentralised Identifiers); access control smart contracts |
Moderate compliance; covered entity agreements required for consortium nodes |
|
EMA Clinical Trial Regulation (EU) |
Harmonised clinical trial approval |
Cross-border trial data sharing on permissioned blockchain; CTIS integration potential |
Emerging; EMA exploring DLT for EudraVigilance pharmacovigilance |
|
ICH E9(R1) Estimands |
Statistical analysis planning |
Pre-specified SAP hashing; tamper-evident primary endpoint definition before unblinding |
Strong fit; addresses selective reporting and HARKing concerns |
GDPR = General Data Protection Regulation; HIPAA = Health Insurance Portability and Accountability Act; EMA = European Medicines Agency; DID = Decentralised Identifier; PHI = Protected Health Information; DLT = Distributed Ledger Technology
DISCUSSION
Principal Findings
This comprehensive review demonstrates that blockchain technology offers substantive and evidence-supported potential to address fundamental integrity, transparency, and security challenges in clinical trials. The weight of available evidence suggests that permissioned blockchain implementations, particularly Hyperledger Fabric and Quorum-based systems, can deliver meaningful benefits in consent management, protocol version control, multi-site data coordination, and audit trail completeness. [77,78]
Quantitatively, reported benefits are compelling: 28–42% reductions in SDV costs, 67% improvement in screening documentation efficiency, near-zero undetected protocol amendments, and substantial reductions in adverse event reporting delays. These findings, while primarily from pilot studies and proof-of-concept implementations, are directionally consistent across diverse settings and platforms.
Comparison with Existing Evidence
Our findings are broadly consistent with previous systematic reviews by Agbo et al. (2019) and Maslove et al. (2018), who also identified data integrity and consent management as the most mature application areas and scalability and regulatory uncertainty as the most significant barriers. [79,80] We extend these reviews by incorporating five additional years of implementation evidence, including the first regulatory submission pilot data, and by providing a more granular analysis of platform-specific performance characteristics.
Our review also adds important nuance regarding the heterogeneity of blockchain applications: the technology is not a monolithic solution but a family of architectures with substantially different performance, governance, and regulatory profiles. The frequent conflation of Bitcoin-era public blockchain limitations with the capabilities of modern permissioned platforms has contributed to unwarranted pessimism in some segments of the clinical research community.
Strengths and Limitations of This Review
Strengths of this review include its comprehensive search strategy spanning multiple databases including grey literature, its broad inclusion criteria capturing diverse study designs, its multi-disciplinary analytical team combining clinical research, pharmacy, informatics, and regulatory expertise, and its explicit critical evaluation of implementation quality.
Limitations include: (i) the early-stage nature of most included evidence, with few large-scale randomised evaluations of blockchain implementation effects; (ii) publication bias toward positive pilot results; (iii) the rapidly evolving technology landscape, which may render some platform-specific findings outdated; and (iv) the limited generalisability of implementations from well-resourced academic centres to low- and middle-income country (LMIC) research settings. [81]
Implications for Research Practice
For trial sponsors, the evidence supports a strategic investment in blockchain capability building, beginning with consent management and protocol registration as entry points with the most mature evidence base and most immediate regulatory alignment. Full trial data management on blockchain should currently be approached as innovation rather than operational standard.
For site investigators and CROs, engagement with blockchain piloting programmes provides both methodological learning and competitive differentiation. Staff training in blockchain literacy should be incorporated into continuing professional development programmes for clinical research coordinators and data managers.
Implications for Policy and Regulation
Regulatory agencies urgently need to issue explicit guidance on the acceptability of blockchain-derived audit trails in regulatory submissions. The current guidance vacuum creates uncertainty that deters investment and innovation. A multi-stakeholder working group involving FDA, EMA, PhRMA, EFPIA, and patient organisations should develop harmonised international standards for blockchain in clinical research, drawing on the precedent of the ICH E6(R2) process. [82,83]
Particular priority should be given to resolving the GDPR right-to-erasure conflict through technical standards, establishing accepted smart contract validation methodologies for GCP systems, and defining data ownership and liability frameworks for consortium blockchain networks.
CONCLUSION
This review establishes that blockchain technology represents a genuine paradigm shift opportunity for clinical trial conduct, capable of addressing long-standing structural weaknesses in data integrity, transparency, consent management, and multi-site coordination. The evidence base, while still predominantly from pilot implementations, is sufficiently coherent and directionally consistent to justify strategic investment in blockchain capability development by trial sponsors, CROs, academic research centres, and regulatory agencies. [84,85]
The most mature and immediately deployable applications are: (i) cryptographic protocol pre-registration with tamper-evident timestamping; (ii) blockchain-enabled eConsent with smart contract-driven reconsenting workflows; (iii) hybrid architecture data integrity anchoring for multi-site EDC systems; and (iv) pharmaceutical supply chain serialisation and IMP tracking.
The convergence of blockchain with complementary technologies — artificial intelligence for predictive protocol deviation detection, IoT for real-time biosensor data capture, decentralised identifiers for patient-centric identity management, and federated learning for privacy-preserving multi-site analyses — sketches a compelling vision of a fundamentally reformed clinical research infrastructure that is simultaneously more rigorous, more efficient, and more participant-centred.
Realising this vision will require coordinated investment across technological, regulatory, educational, and governance dimensions. The clinical research community has a profound obligation to trial participants and to society to pursue these improvements with urgency and rigour. Blockchain technology, thoughtfully deployed within a robust governance framework and aligned with regulatory expectations, offers a transformative contribution to that essential mission. [86,87]
REFERENCES




Edapalapati Venkata Naga Nithin, Arpita R Walvekar, Samarth GH, Suhani Chaudhary, Blockchain Technology in Clinical Trials: Enhancing Data Integrity, Transparency, and Security, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 1587-1606. https://doi.org/10.5281/zenodo.21261230
 10.5281/zenodo.21261230
10.5281/zenodo.21261230