
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shreeshakti Shaikshanik Sanstha, Divine college of Pharmacy, Nampur road, Satana, Nashik – 423301, Maharashtra, India.
Urolithiasis is a common and recurrent urinary tract disorder characterized by the formation of calculi due to urinary supersaturation, crystal nucleation, aggregation, oxidative stress, and renal epithelial injury. Despite advances in conventional therapies, including pharmacological and surgical interventions, recurrence rates remain high and treatment-associated adverse effects continue to be a concern. Consequently, there is growing interest in phytotherapeutic approaches for the prevention and management of urinary stone disease. This review critically examines traditional herbal therapies used in urolithiasis and evaluates their mechanisms of action, therapeutic benefits, and limitations. Particular emphasis is placed on the potential of herbal combination therapy as a multi-targeted treatment strategy. Among the various medicinal plants investigated, Bauhinia variegata and Zea mays corn silk emerge as promising candidates due to their complementary pharmacological activities. Bauhinia variegata possesses significant antioxidant, anti-inflammatory, and nephrotective properties, whereas Zea mays corn silk exhibits notable diuretic, antioxidant, and urinary tract protective effects. The combination of these plants may provide synergistic benefits by targeting multiple pathogenic mechanisms involved in stone formation, including oxidative stress, crystal retention, inflammation, and urinary supersaturation. Although existing evidence supports the therapeutic potential of both plants individually, systematic evaluation of their combined antiurolithiatic efficacy remains limited. Therefore, further experimental and clinical investigations are warranted to validate their effectiveness and establish their role as a novel phytotherapeutic intervention for urolithiasis
Urolithiasis, often known as kidney stone disease, is a multifactorial condition marked by the development of crystalline calculi in the urinary tract. It is one of the most common urological conditions in the world and puts a lot of strain on healthcare systems, both financially and clinically.[1] The disease is characterized by the excessive concentration of urine with stone-forming substances like calcium, oxalate, phosphate, and uric acid, resulting in the nucleation, growth, and aggregation of crystals that ultimately develop into calculi. Epidemiological studies show that urolithiasis affects between 5% and 15% of the world's population. It is more common in areas with hot climates, poor diets, and little physical activity. also, recurrence rates remain considerably high, with nearly 50% of affected individuals experiencing recurrent episodes within 5–10 years following initial stone formation. These factors together show how important it is to have good preventive and therapeutic strategies.[2]
The pathogenesis of urolithiasis is intricate, encompassing various physiological and biochemical processes such as urinary supersaturation, crystal nucleation, crystal growth, and aggregation. Calcium oxalate stones make up about 70–80% of all urinary calculi cases. Hypercalciuria, hyperoxaluria, hypocitraturia, and hyperuricosuria are some of the metabolic problems that are known to cause stones to form.[3] Recent evidence also shows that oxidative stress, damage to renal tubules, and inflammation all play a big part in making crystals stick to and stay in renal tissues.
These processes work together to help microscopic crystals grow into stones that are large enough to cause problems. As a result, therapeutic strategies focused on diminishing oxidative damage, preventing crystal aggregation, and improving urinary flow are regarded as promising methods for the treatment of urolithiasis.[4]
Standard treatment for urolithiasis mainly includes surgery and medication. Medications like thiazide diuretics, potassium citrate, and allopurinol are given based on the metabolic problems that cause stones to form. When stones are big or block the flow of urine, doctors often use surgery to remove them. Some examples of these surgeries are extracorporeal shock wave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy.[5] Even though these treatments work to get rid of stones that are already there, they don't completely get rid of the chance that they will come back. Additionally, pharmacological therapies may be linked to negative effects such as electrolyte imbalance, gastrointestinal discomfort, and long-term metabolic issues. On the other hand, surgery is often expensive and can cause problems like infection, bleeding, or damage to the kidneys. These limitations have led to a growing interest in alternative treatment methods that are both safe and effective.[6]
In recent years, medicinal plants have garnered significant interest as potential therapeutic agents for the treatment of urolithiasis. Phytotherapeutic interventions have been widely employed in traditional medical systems, such as Ayurveda and traditional Chinese medicine, for the management of urinary disorders. Many medicinal plants have been documented to possess antiurolithiatic properties via mechanisms including the inhibition of crystal nucleation and aggregation, the enhancement of urinary output, antioxidant activity, and the protection against renal epithelial damage.[7] Plants like Tribulus terrestris, Boerhavia diffusa, Crataeva nurvala, and Phyllanthus niruri have been studied a lot to see if they can stop or break up urinary stones. Despite encouraging results from experimental and clinical studies, the therapeutic efficacy of individual plant extracts is sometimes limited due to their restricted spectrum of pharmacological activity.[8]
An emerging strategy to enhance the therapeutic potential of phytotherapy involves the use of herbal combination therapies, which are designed to exploit the synergistic interactions among multiple bioactive constituents. Combination therapy can target multiple pathways involved in stone formation simultaneously, thereby improving overall efficacy. For instance, the integration of plants possessing antioxidant, diuretic, anti-inflammatory, and nephroprotective properties may provide a more comprehensive approach to the prevention and management of urolithiasis. In this context, the medicinal plants Bauhinia variegata and Zea mays (corn silk) have attracted growing scientific interest due to their diverse pharmacological activities.[9,10]
Bauhinia variegata, a member of the Fabaceae family, is traditionally used in various herbal formulations for the treatment of inflammatory and metabolic disorders. Phytochemical investigations have revealed the presence of flavonoids, tannins, saponins, and phenolic compounds that exhibit potent antioxidant and anti-inflammatory properties.[11] These bioactive constituents may contribute to renal protection and inhibition of oxidative processes associated with crystal formation. Similarly, the corn silk derived from Zea mays has been widely utilized in traditional medicine as a diuretic and urinary tract remedy. Corn silk contains a variety of biologically active compounds including flavonoids, alkaloids, polysaccharides, and potassium salts, which are known to promote diuresis, reduce urinary supersaturation, and exert protective effects on renal tissues.[12]
Considering the complementary pharmacological properties of these two medicinal plants, the combination of Bauhinia variegata and Zea mays corn silk may represent a promising phytotherapeutic strategy for the management of urolithiasis. Their combined antioxidant, diuretic, and nephroprotective actions could potentially inhibit multiple stages of stone formation, including crystal nucleation, aggregation, and retention within renal tissues. Therefore, a comprehensive evaluation of existing herbal combinations and the therapeutic potential of this plant combination is warranted. The present review aims to critically analyze traditional phytotherapeutic approaches used in the management of urolithiasis while highlighting the potential synergistic benefits of Bauhinia variegata and Zea mays corn silk as a novel herbal combination for the prevention and treatment of urinary stone disease.[13]
2. PATHOPHYSIOLOGY OF UROLITHIASIS
The development of Urolithiasis is a complex physicochemical and biological process involving the formation, growth, and retention of crystalline deposits within the urinary tract. Stone formation occurs when urine becomes supersaturated with lithogenic substances such as calcium, oxalate, phosphate, and uric acid. Under such conditions, these solutes exceed their solubility threshold, leading to the initiation of crystal nucleation, which represents the earliest step in the formation of urinary calculi. Subsequent crystal growth and aggregation result in the development of larger particles capable of forming clinically significant stones within the renal collecting system.[14]
Among the various types of urinary calculi, calcium oxalate stones are the most prevalent, accounting for nearly 70–80% of all cases. The formation of these stones is strongly influenced by metabolic abnormalities including hypercalciuria, hyperoxaluria, hypocitraturia, and hyperuricosuria. These metabolic disturbances alter urinary chemistry, increasing the concentration of stone-forming ions and reducing the presence of natural inhibitors of crystallization such as citrate, magnesium, and glycoproteins. In the absence of adequate inhibitory factors, crystals tend to aggregate and adhere to renal epithelial surfaces, promoting the progression of microscopic crystals into macroscopic stones.
In addition to physicochemical mechanisms, recent studies have emphasized the significant role of oxidative stress and renal tubular injury in the pathogenesis of urolithiasis. Excessive production of reactive oxygen species (ROS) can damage renal epithelial cells, thereby facilitating crystal attachment and retention within the renal tubules. Oxidative stress also stimulates inflammatory responses and lipid peroxidation, which further aggravate renal tissue injury and create favorable conditions for crystal deposition. Consequently, antioxidants capable of reducing oxidative damage have been suggested as potential therapeutic agents for preventing stone formation.[15]
Another important factor contributing to stone formation is reduced urinary flow or urinary stasis, which prolongs the contact time between crystals and renal epithelial cells. Adequate urine volume is therefore considered an essential protective factor against urolithiasis, as increased diuresis dilutes urinary solutes and facilitates the elimination of microscopic crystals before they aggregate into larger calculi. This explains why diuretic agents, including several medicinal plants, have traditionally been used to manage kidney stone disease.
Inflammatory processes also play a critical role in the progression of urolithiasis. The presence of crystals within renal tissues can trigger inflammatory signaling pathways, leading to the recruitment of immune cells and the release of pro-inflammatory mediators. These inflammatory responses may enhance crystal retention and contribute to renal tissue damage. Therefore, agents possessing anti-inflammatory properties may help mitigate these pathological processes and reduce the likelihood of recurrent stone formation.[16]
Taken together, the pathogenesis of urolithiasis involves a multifactorial interplay between urinary supersaturation, crystal nucleation and aggregation, oxidative stress, renal epithelial injury, and inflammatory responses. Effective therapeutic strategies should therefore target multiple stages of this pathological cascade, including inhibition of crystal formation, enhancement of urinary output, reduction of oxidative stress, and protection of renal tissues. In this context, phytotherapeutic agents possessing antioxidant, diuretic, and nephroprotective properties have attracted increasing scientific interest as potential alternatives or adjuncts to conventional treatments for urolithiasis.[17]
3. TRADITIONAL HERBAL THERAPIES OF UROLITHIASIS
The use of medicinal plants for the management of Urolithiasis has a long-standing history in various traditional systems of medicine, including Ayurveda, Unani, and Traditional Chinese Medicine. Herbal remedies have been widely employed due to their accessibility, perceived safety, and multifaceted pharmacological properties. Over the past few decades, numerous plant-based therapies have been scientifically investigated for their antiurolithiatic potential, demonstrating a range of mechanisms such as diuretic activity, inhibition of crystal nucleation and aggregation, antioxidant effects, and protection against renal epithelial injury.[18]
Among the extensively studied medicinal plants, Tribulus terrestris has been traditionally used for urinary disorders owing to its pronounced diuretic and lithotriptic properties. Experimental studies have indicated that extracts of this plant can enhance urinary output and reduce the supersaturation of stone-forming constituents, thereby facilitating the dissolution and expulsion of urinary calculi. Similarly, Boerhavia diffusa, commonly known as Punarnava, has been reported to possess significant diuretic, anti-inflammatory, and nephroprotective activities. Its ability to modulate urinary composition and reduce renal inflammation contributes to its therapeutic efficacy in the management of kidney stones.[19]
Another important medicinal plant is Crataeva nurvala, which has been widely utilized in traditional formulations for urolithiasis. The plant exhibits anti-inflammatory and anti-lithic properties, primarily through its ability to reduce urinary oxalate levels and inhibit stone formation. Additionally, Aerva lanata has gained attention for its potential to prevent crystal aggregation and promote the disintegration of preformed stones. The plant is also known to possess mild diuretic activity, which aids in flushing out stone-forming constituents from the urinary tract.[20]
Furthermore, Phyllanthus niruri, often referred to as the “stone breaker,” has been extensively investigated for its antiurolithiatic properties. Studies suggest that this plant can inhibit calcium oxalate crystal growth, reduce crystal adhesion to renal epithelial cells, and modulate urinary biochemistry. Its antioxidant and anti-inflammatory activities further contribute to its protective effects on renal tissues. Despite these promising findings, the efficacy of individual plant extracts may be limited by their inability to simultaneously target multiple pathways involved in stone formation.[21]
Dolichos biflorus (Kulthi) has long been used in traditional medicine for managing urinary stones, mainly due to its diuretic action and its ability to limit crystal formation and aid their removal. Likewise, Crataeva nurvala (Varuna) is valued for its stone-breaking and anti-inflammatory effects, which help improve urine flow and ease associated discomfort. When used together, these plants have shown enhanced effectiveness in experimental studies, including a noticeable reduction in stone formation and oxalate deposition, suggesting their promise as a combined herbal approach for urolithiasis.[22]
Dolichos biflorus (Kulthi) is traditionally valued for its diuretic effect and its ability to reduce the buildup of stone-forming crystals, aiding their elimination. Bergenia ligulata (Pashanbheda), on the other hand, is well known for its lithotriptic action, helping to break down existing calculi. Together, these plants may offer a complementary effect by both inhibiting crystal formation and promoting their dissolution, although available studies suggest that their combined efficacy may vary compared to individual use.[23]
Boerhavia diffusa (Punarnava) is known for its nephroprotective and anti-inflammatory effects, helping to reduce renal irritation and support kidney function. Aerva lanata (Pashanabheda) is widely used for its diuretic and antiurolithiatic properties, aiding in the flushing out of urinary crystals. When considered together, these plants may offer a complementary approach by protecting renal tissue while promoting the elimination of stone-forming substances, although direct studies on their combined use remain limited.[24]
Traditional herbal formulations often combine multiple plants to enhance therapeutic effects through synergistic actions. Combinations like Tribulus terrestris with Boerhavia diffusa and Crataeva nurvala with Aerva lanata are used to manage different aspects of urolithiasis. However, many lack strong scientific validation and mainly focus on limited effects such as diuresis or inflammation. This underscores the need for more rational combinations targeting multiple pathogenic pathways, including oxidative stress and crystal aggregation.
4. COMPARATIVE ANALYSIS OF COMMON HERBAL COMBINATIONS
Existing herbal combinations show good therapeutic potential but often fail to address all aspects of urolithiasis. Combining plants with complementary actions may improve outcomes by targeting oxidative stress, crystal formation, urinary supersaturation, and renal protection simultaneously. Such multi-mechanistic approaches are more promising than single-plant therapies. In this regard, Bauhinia variegata and Zea mays corn silk, with their antioxidant, diuretic, and nephroprotective properties, merit further investigation as a potential treatment strategy.
Table 1 Herbal combinations with their mechanism, reported activity & limitations
|
Sr.no. |
Herbal Combination |
Major Mechanism |
Reported Activity |
Limitations |
References |
|
1. |
Tribulus terrestris + Boerhavia diffusa |
Diuretic, anti-inflammatory |
Enhances urine output and reduces inflammation |
Limited antioxidant and anti-crystallization effects |
[19] |
|
2. |
Crataeva nurvala + Aerva lanata |
Anti-inflammatory, anti-lithic |
Reduces stone formation and urinary oxalate levels |
Insufficient evidence on oxidative stress modulation |
[20] |
|
3. |
Phyllanthus niruri (single/combined) |
Anti-crystallization, antioxidant |
Inhibits crystal growth and adhesion |
Variable efficacy in complex cases |
[21] |
|
4. |
Dolichos biflorus + Crataeva nurvala |
Diuretic, anti-lithic, anti-inflammatory |
Demonstrated reduction in calcium oxalate deposition and improved renal histopathology in experimental models |
Limited clinical studies |
[22] |
|
5. |
Dolichos biflorus + Bergenia ligulata |
Anti-crystallization, lithotriptic |
Inhibits calcium oxalate crystal formation and aggregation (in vitro studies) |
Combination not consistently superior to individual extracts |
[23] |
|
6. |
Boerhavia diffusa + Aerva lanata |
Nephroprotective, diuretic, anti-inflammatory |
Reduces renal damage and promotes elimination of crystals based on individual pharmacological activities |
Lack of direct combination-based experimental studies |
[24] |
|
7. |
Bauhinia variegata + Zea mays |
Antioxidant, diuretic, anti-crystallization, nephroprotective |
Potential multi-targeted therapeutic effect |
Requires systematic experimental validation |
|
5. PHARMACOLOGICAL PROFILE OF Bauhinia variegata

Figure 1Bauhinia variegata
Bauhinia variegata Linn., a member of the family Fabaceae, is a widely distributed medicinal plant extensively utilized in traditional systems of medicine for the treatment of various inflammatory, metabolic, and urinary disorders. Different parts of the plant, including the bark, leaves, flowers, and roots, have been employed in ethnomedicinal practices owing to their broad spectrum of pharmacological activities. In recent years, Bauhinia variegata has attracted considerable scientific interest due to the presence of diverse bioactive phytoconstituents that contribute to its therapeutic relevance in renal and urinary pathologies, including urolithiasis.
Phytochemical investigations have revealed the presence of several biologically active compounds, including flavonoids, tannins, saponins, glycosides, phenolic compounds, triterpenoids, and phytosterols. Among these, flavonoids such as quercetin and kaempferol, along with their glycosidic derivatives like rutin, are particularly significant due to their potent antioxidant properties.
Oxidative stress is recognized as a critical factor in the pathogenesis of urolithiasis, as it promotes renal epithelial injury, crystal adherence, and inflammatory responses within the urinary tract. Therefore, the antioxidant potential of these flavonoids plays a crucial role in attenuating oxidative renal damage and reducing the progression of crystal-induced tissue injury.[26]
In addition to antioxidant activity, Bauhinia variegata exhibits notable anti-inflammatory effects. This activity is largely attributed to triterpenoid constituents such as lupeol, which have been reported to suppress inflammatory mediators and alleviate tissue inflammation. This is particularly relevant in urolithiasis, where crystal deposition induces local inflammatory responses. Chronic inflammation within the renal epithelium may facilitate crystal retention and exacerbate tissue damage; hence, anti-inflammatory agents capable of mitigating these responses contribute to the prevention of stone progression and recurrence. The plant has also been associated with analgesic and cytoprotective properties, further supporting its role in the management of urinary tract disorders.[27]
Another important feature of Bauhinia variegata is its nephroprotective potential. Phytosterols such as β-sitosterol, along with phenolic compounds, are known to stabilize cellular membranes, reduce lipid peroxidation, and enhance endogenous antioxidant defense mechanisms. Such actions help preserve renal epithelial integrity and decrease the likelihood of crystal attachment, which is a crucial step in the formation of urinary calculi.[28]
Although direct evidence specifically investigating the antiurolithiatic activity of Bauhinia variegata remains relatively limited compared to some established lithotriptic plants, its pharmacological profile strongly supports its therapeutic potential. The plant exhibits a combination of antioxidant, anti-inflammatory, and nephroprotective effects that are highly relevant to the multifactorial pathogenesis of urolithiasis. Moreover, its rich phytochemical composition suggests that it may contribute synergistically when combined with other medicinal plants possessing complementary activities, particularly diuretic and anti-crystallization properties.
From a phytotherapeutic perspective, Bauhinia variegata may therefore be considered a promising candidate for combination-based antiurolithiatic interventions. Its ability to target renal oxidative stress and inflammatory injury provides a strong mechanistic rationale for its inclusion in herbal formulations intended for the prevention and management of urinary stone disease. Consequently, when combined with a medicinal agent such as Zea mays corn silk, which is traditionally recognized for its diuretic and urinary tract protective actions, Bauhinia variegata may contribute to a more comprehensive and mechanistically integrated therapeutic approach toward urolithiasis due to presence of Chemical constituents included in figure 3.
Table 2 Parameters of Bauhinia variegata
Figure 3 Chemical constituents of Bauhinia variegata
|
Parameter |
Details |
|
Botanical Name |
Bauhinia variegata L. |
|
Family |
Fabaceae |
|
Common Name |
Kachnar (Mountain Ebony) |
|
Part Used |
Bark, leaves, flowers |
|
Traditional Use |
Anti-inflammatory and used in urinary and metabolic disorders |
|
Phytoconstituents |
Flavonoids, tannins, saponins, phenolics, glycosides, alkaloids |
|
Pharmacological Actions |
Antioxidant, anti-inflammatory, nephroprotective |
|
MOA (Antiurolithiatic) |
Reduces oxidative stress, inflammation, and renal epithelial damage |
|
Role in Urolithiasis |
Prevents crystal adhesion and protects kidney tissue |
|
Combination Role |
Provides antioxidant support enhancing synergistic effect |
6. PHARMACOLOGICAL PROFILE OF Zea mays Corn Silk

Figure 2 Zea mays
Zea mays L., belonging to the family Poaceae, is one of the most extensively cultivated cereal crops worldwide. In addition to its nutritional significance, several parts of the plant have been employed in traditional medicine for the management of various ailments, particularly those affecting the urinary system. Corn silk, the elongated stigmatic threads of the female inflorescence, has long been recognized as a valuable ethnomedicinal material and has been traditionally used as a diuretic, anti-inflammatory, and soothing agent in urinary tract disorders. Its relevance in the management of urolithiasis is increasingly supported by pharmacological evidence demonstrating its beneficial effects on urinary flow, renal protection, and modulation of oxidative stress.
Phytochemical analyses of Zea mays corn silk have revealed a diverse array of bioactive constituents, including flavonoids, phenolic compounds, alkaloids, saponins, tannins, polysaccharides, phytosterols, and mineral salts, particularly potassium. Among these, flavonoids such as maysin and isoorientin, along with phenolic acids like ferulic acid and caffeic acid, are considered major contributors to its antioxidant activity. Additionally, phytosterols such as β-sitosterol contribute to membrane stabilization and cellular protection.
Potassium salts are primarily associated with the traditional diuretic effect of corn silk. The presence of these bioactive molecules supports the therapeutic versatility of corn silk and provides a scientific basis for its use in renal and urinary disorders.[29]
One of the most significant pharmacological properties of corn silk is its diuretic activity. Increased urinary output is a crucial therapeutic strategy in the prevention and management of urolithiasis, as it reduces urinary supersaturation of lithogenic substances and facilitates the elimination of microscopic crystals before they can aggregate into larger calculi. Corn silk has been traditionally administered to promote urination and relieve urinary irritation, and experimental studies have supported its ability to increase urine volume. This diuretic effect may contribute directly to reducing the risk of crystal retention within the renal tubules and urinary tract.
In addition to its diuretic action, Zea mays corn silk exhibits notable antioxidant and nephroprotective properties. The antioxidant activity is largely attributed to flavonoids such as maysin and isoorientin, along with phenolic acids like ferulic acid, which effectively scavenge reactive oxygen species and reduce lipid peroxidation.
Oxidative stress plays a central role in renal epithelial damage and crystal adhesion during stone formation. By mitigating oxidative injury, these constituents help protect renal tissues and preserve cellular integrity. Furthermore, nephroprotective effects reported in experimental models suggest that corn silk may help maintain renal architecture and function under conditions of metabolic stress and toxic insult. Such protective actions are highly relevant in urolithiasis, where recurrent crystal deposition may lead to epithelial disruption and impaired renal function.[30]
Corn silk has also been reported to possess mild anti-inflammatory and soothing effects on the urinary tract. Inflammatory responses associated with crystal deposition can exacerbate renal tissue injury and promote stone retention. Therefore, agents capable of attenuating inflammation may provide additional therapeutic benefit in reducing the progression and recurrence of urinary calculi. Although the anti-inflammatory activity of corn silk may be less pronounced than its diuretic effect, it nonetheless contributes to its overall utility as a supportive phytotherapeutic agent in urinary tract disorders.[31]
From a therapeutic standpoint, Zea mays corn silk represents a particularly valuable component in combination-based herbal strategies for urolithiasis. Its principal contribution lies in its ability to enhance urinary flow, reduce lithogenic concentration, and provide antioxidant and nephroprotective support. These attributes complement the pharmacological profile of Bauhinia variegata, which is characterized primarily by antioxidant and anti-inflammatory effects. Accordingly, the integration of Zea mays corn silk with Bauhinia variegata may result in a synergistic phytotherapeutic combination capable of targeting multiple pathogenic determinants of urolithiasis, thereby offering a more comprehensive and rational approach to disease management.
Figure 4 Chemical constituents of Zea mays
Table 3 Parameters of Zea mays
|
Parameter |
Details |
|
Botanical Name |
Zea mays L. |
|
Family |
Poaceae |
|
Common name |
Maize (corn) |
|
Part Used |
Corn silk (female stigmatic threads) |
|
Traditional Use |
Diuretic and urinary soothing agent |
|
Phytoconstituents |
Flavonoids, phenolics, saponins, tannins, β-sitosterol, potassium |
|
Key Activities |
Diuretic, antioxidant, nephroprotective |
|
MOA (Antiurolithiatic) |
Increases urine flow and reduces oxidative stress |
|
Role in Urolithiasis |
Prevents crystal formation and promotes elimination |
|
Combination Role |
Enhances diuresis and supports kidney protection |
7. SCIENTIFICRATIONAL FOR THE COMBINATION OF Bauhinia variegata & Zea mays CORN SILK
The development of an effective phytotherapeutic strategy for urolithiasis requires a multi-targeted approach capable of addressing the diverse mechanisms involved in stone formation and renal injury. Since the pathogenesis of urolithiasis encompasses urinary supersaturation, crystal nucleation and aggregation, oxidative stress, inflammatory responses, and epithelial damage, the use of a single therapeutic agent may not always provide comprehensive protection. In this context, combination-based herbal therapy has emerged as a rational and potentially superior strategy, particularly when the selected plants possess complementary pharmacological properties. The combination of Bauhinia variegata and Zea mays corn silk appears especially promising because their distinct yet overlapping bioactivities may collectively target several critical stages of urolithiasis pathogenesis.
Bauhinia variegata is characterized primarily by its potent antioxidant, anti-inflammatory, and nephroprotective activities. Its rich content of flavonoids, phenolic compounds, tannins, and saponins suggests a significant capacity to attenuate oxidative stress and reduce crystal-induced renal epithelial injury. Since oxidative damage and local inflammation facilitate crystal adhesion and retention within renal tissues, the pharmacological actions of Bauhinia variegata may help limit tissue injury and impede the progression of microscopic crystals into clinically significant calculi. Thus, the plant may play a protective role by targeting the cellular and biochemical disturbances that predispose to stone formation.[29]
In contrast, Zea mays corn silk contributes predominantly through its diuretic, antioxidant, and urinary tract protective effects. By increasing urine output, corn silk may reduce the urinary concentration of lithogenic substances such as calcium and oxalate, thereby decreasing supersaturation and facilitating the elimination of small crystals before they undergo aggregation. Its antioxidant constituents further support renal protection by reducing reactive oxygen species-mediated damage, while its mild anti-inflammatory properties may contribute to the alleviation of urinary tract irritation associated with crystal passage. Consequently, Zea mays corn silk offers a valuable functional dimension that complements the pharmacological profile of Bauhinia variegata.[30]
The scientific basis for combining these two medicinal plants lies in their potential to exert synergistic effects through mechanistic complementarity. Whereas Bauhinia variegata primarily addresses oxidative stress, inflammation, and epithelial protection, Zea mays corn silk enhances urinary flow and assists in the reduction of lithogenic burden. Together, these actions may result in a broader antiurolithiatic effect than either plant could provide individually. Such a combination may not only inhibit crystal formation and aggregation but also promote crystal expulsion and preserve renal tissue integrity.
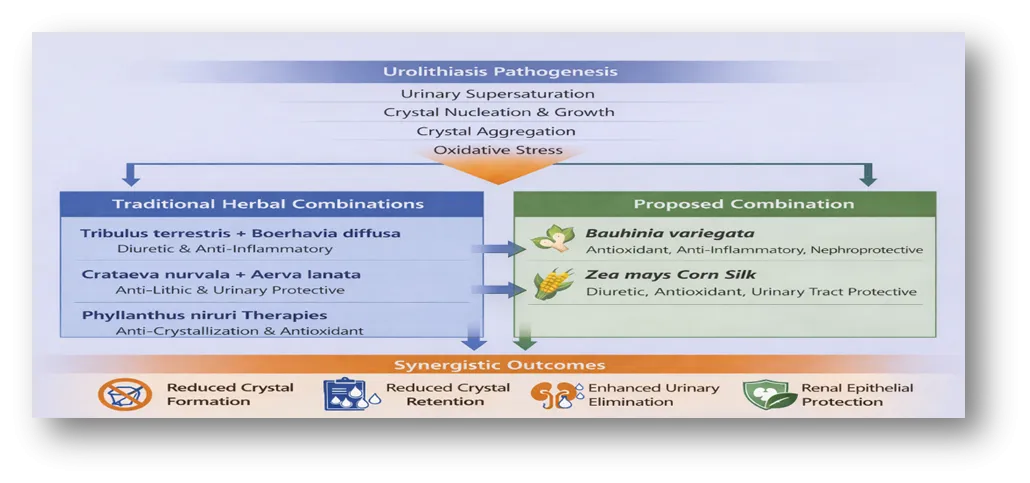
Figure 3 traditional herbal combination vs B.variegata and Zea mays combination
From a phytotherapeutic perspective, this combination represents a rational intervention designed to target multiple determinants of urolithiasis simultaneously. Its anticipated benefits include attenuation of oxidative renal injury, reduction of inflammatory responses, enhancement of diuresis, and minimization of crystal retention. Therefore, the combination of Bauhinia variegata and Zea mays corn silk may be considered a scientifically justified and potentially effective herbal approach for the management of urolithiasis, warranting further experimental and clinical investigation.
8. RESEARCH GAP
Despite considerable research on plant-based interventions for the management of Urolithiasis, existing literature is predominantly centered on single-plant extracts or empirically derived traditional formulations, with limited emphasis on systematic comparative evaluation.[31,32] Although several medicinal plants, including Tribulus terrestris, Boerhavia diffusa, and Crataeva nurvala, have demonstrated notable antiurolithiatic activity[33], their therapeutic scope is often restricted to specific mechanisms such as diuresis or inhibition of crystal formation. Consequently, the potential advantages of rationally designed phytotherapeutic combinations that can simultaneously target multiple pathogenic pathways remain insufficiently explored.[34]
In particular, the combined application of Bauhinia variegata and Zea mays corn silk has not been systematically investigated, despite compelling evidence supporting their individual antioxidant, diuretic, anti-inflammatory, and nephroprotective properties.[35,36] The absence of critical evaluation of such complementary combinations represents a significant gap in current phytotherapeutic research.[37] Therefore, a comprehensive and comparative review examining existing herbal formulations while elucidating the potential synergistic benefits of this combination is warranted to inform future experimental and clinical investigations.[38]
CONCLUSION
Urolithiasis remains a clinically significant disorder characterized by high prevalence, recurrence, and multifactorial pathogenesis involving urinary supersaturation, crystal aggregation, oxidative stress, and renal epithelial injury. Although conventional therapeutic strategies are effective in the removal of existing calculi, their limitations, including recurrence and potential adverse effects, necessitate the exploration of safer and more comprehensive treatment approaches. In this context, phytotherapy has emerged as a promising alternative, particularly through the use of herbal combinations that can simultaneously target multiple pathogenic mechanisms.
The present review critically evaluated traditional herbal therapies and highlighted their pharmacological contributions and limitations in the management of urolithiasis. While several medicinal plants demonstrate notable antiurolithiatic activity, many conventional combinations lack a holistic mechanistic approach. In contrast, the combination of Bauhinia variegata and Zea mays corn silk presents a rational phytotherapeutic strategy supported by complementary pharmacological actions, including antioxidant, anti-inflammatory, diuretic, and nephroprotective effects. These properties collectively suggest the potential of this combination to inhibit stone formation, promote crystal elimination, and protect renal tissues.
However, despite its promising therapeutic rationale, the efficacy of this combination requires further validation through well-designed experimental and clinical studies. Future research focusing on mechanistic evaluation, standardization, and clinical applicability may facilitate the development of an effective and evidence-based phytotherapeutic intervention for urolithiasis.
REFERENCES

Harshali Khairnar, Chandrashekhar Patil, Kajal Pansare, Jubershaha Fakir, Durgesh Pagar, Sunil Mahajan, Comparative Evaluation of Traditional Herbal Combinations in the Management of Urolithiasis with Special Reference to Bauhinia variegata and Zea mays, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 567-581, https://doi.org/10.5281/zenodo.21155649
 10.5281/zenodo.21155649
10.5281/zenodo.21155649