
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of pharmacognosy, Aditya Institute of Pharmacy, Chalisgaon, 424101
Diabetes mellitus is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from impaired insulin secretion, insulin action, or both. The increasing prevalence of Type I and Type II diabetes has led to growing dependence on both synthetic and herbal therapeutic approaches. Synthetic drugs remain the cornerstone of diabetes treatment; however, herbal remedies are increasingly preferred due to their affordability, availability, and lower perceived side effects. The present study aimed to compare the utilization pattern of herbal and synthetic drugs used in the management of Type I and Type II diabetes mellitus in selected areas of Chalisgaon, Maharashtra. A cross-sectional observational survey was conducted using dispensing trend data collected from selected medical stores located in Signal Point, Ghat Road, Captain Corner, College Point, and Bus Stand areas. Data were categorized into Type I and Type II diabetes and further divided into herbal and synthetic drug utilization groups. Results showed that in Type I diabetes, synthetic drug utilization (593 cases) was significantly higher than herbal drug utilization (430 cases). In Type II diabetes, synthetic drug utilization (550 cases) was also higher than herbal drug utilization (496 cases), although the difference was comparatively smaller. Overall, synthetic drugs showed greater utilization (1143 cases) compared to herbal drugs (926 cases). The findings suggest that synthetic therapy remains the dominant treatment option, especially in Type I diabetes, while herbal drug utilization is comparatively more common in Type II diabetes. The study indicates increasing acceptance of herbal therapies as supportive treatment options. Further clinical and population-based studies are recommended to evaluate efficacy, safety, and integrative treatment strategies.
Diabetes mellitus is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both1. It is one of the most significant non-communicable diseases affecting millions of people worldwide and poses a major burden on healthcare systems, particularly in developing countries like India2. The condition is associated with disturbances in carbohydrate, fat, and protein metabolism, which ultimately lead to various acute and chronic complications if not properly managed3. The global prevalence of diabetes has been increasing at an alarming rate over the past few decades4. Rapid urbanization, sedentary lifestyle, unhealthy dietary habits, obesity, and genetic predisposition are some of the key contributing factors5. According to international health reports, diabetes is expected to become one of the leading causes of morbidity and mortality in the near future6. In India, often referred to as the “diabetes capital of the world,” the burden of both Type I and Type II diabetes is continuously rising, affecting individuals across different age groups7. Diabetes mellitus is broadly classified into Type I Diabetes Mellitus (T1DM) and Type II Diabetes Mellitus (T2DM)8. Type I diabetes is primarily an autoimmune disorder characterized by the destruction of pancreatic β-cells, resulting in absolute insulin deficiency. Patients with Type I diabetes require lifelong insulin therapy for survival9. On the other hand, Type II diabetes is more common and is characterized by insulin resistance along with relative insulin deficiency. It is strongly associated with lifestyle factors such as physical inactivity, obesity, and poor dietary patterns10. The pathophysiology of diabetes involves multiple metabolic abnormalities. In Type II diabetes, decreased insulin sensitivity in peripheral tissues, increased hepatic glucose production, impaired insulin secretion, and reduced incretin effect contribute to elevated blood glucose levels11. Additionally, abnormalities in lipid metabolism and increased oxidative stress further complicate disease progression12. Long-term uncontrolled diabetes can lead to serious complications such as neuropathy, nephropathy, retinopathy, cardiovascular diseases, and diabetic foot ulcers, significantly affecting the quality of life13. The management of diabetes mellitus primarily focuses on maintaining blood glucose levels within the normal range and preventing complications14. Conventional treatment includes the use of synthetic (allopathic) drugs such as insulin, biguanides (metformin), sulfonylureas, DPP-4 inhibitors, SGLT2 inhibitors, thiazolidinediones, and GLP-1 receptor agonists15. These drugs act through various mechanisms, including increasing insulin secretion, improving insulin sensitivity, reducing hepatic glucose production, and enhancing glucose excretion16. Although synthetic drugs are highly effective in controlling blood glucose levels, they are often associated with certain limitations17. These include adverse effects such as hypoglycemia, gastrointestinal disturbances, weight gain, and, in some cases, cardiovascular risks. Additionally, the long-term use of these medications can be costly, which may limit accessibility for patients in low- and middle-income regions18. These challenges have led to increased interest in alternative and complementary treatment approaches19. In recent years, herbal medicines and natural products have gained significant attention in the management of diabetes mellitus. Traditional systems of medicine such as Ayurveda, Unani, and herbal therapy have been used for centuries to treat various ailments, including diabetes. Herbal drugs are considered relatively safe, cost-effective, and easily accessible, especially in rural and semi-urban areas20.
Several medicinal plants have been reported to possess antidiabetic properties. Plants such as Nigella sativa (black seed), Cinnamomum verum (cinnamon), Zingiber officinale (ginger), Coptis chinensis, Rosmarinus officinalis (rosemary), and Elettaria cardamomum (cardamom) contain bioactive compounds like alkaloids, flavonoids, phenolics, and terpenoids that exhibit hypoglycemic effects21. These compounds act through multiple mechanisms, including enhancing insulin sensitivity, stimulating insulin secretion, inhibiting carbohydrate-digesting enzymes, reducing oxidative stress, and improving glucose uptake in peripheral tissues22. One of the major advantages of herbal drugs is their multi-targeted mechanism of action, which allows them to act on various pathways involved in diabetes23. Additionally, they are associated with fewer side effects compared to synthetic drugs. However, limitations such as lack of standardization, variability in potency, and insufficient clinical evidence still exist, which restrict their widespread acceptance in modern medicine24. In developing regions such as Chalisgaon, Maharashtra, both herbal and synthetic drugs are commonly used for diabetes management. The choice of therapy is influenced by various factors, including cost, availability, patient awareness, cultural beliefs, and recommendations from healthcare professionals. While synthetic drugs are generally prescribed by physicians, herbal remedies are often used based on traditional knowledge or personal preference25. Despite the increasing use of both treatment modalities, there is limited regional data comparing the utilization patterns of herbal and synthetic drugs in diabetes management26. Understanding these patterns is essential for evaluating patient preferences, identifying gaps in treatment, and promoting rational drug use27. Therefore, the present study titled “Comparative Study of Herbal and Synthetic Drugs Used in the Management of Type I and Type II Diabetes Mellitus in Chalisgaon Area” was undertaken. The study aims to analyse and compare the utilization trends of herbal and synthetic antidiabetic drugs across different areas of Chalisgaon. By doing so, it seeks to provide valuable insights into current treatment practices and the growing role of herbal medicine in diabetes care. This study also highlights the potential for an integrated approach combining both herbal and synthetic therapies. Such an approach may offer improved glycemic control, reduced side effects, and better patient compliance. Ultimately, the findings of this study can contribute to the development of more effective and patient-centered strategies for diabetes management.
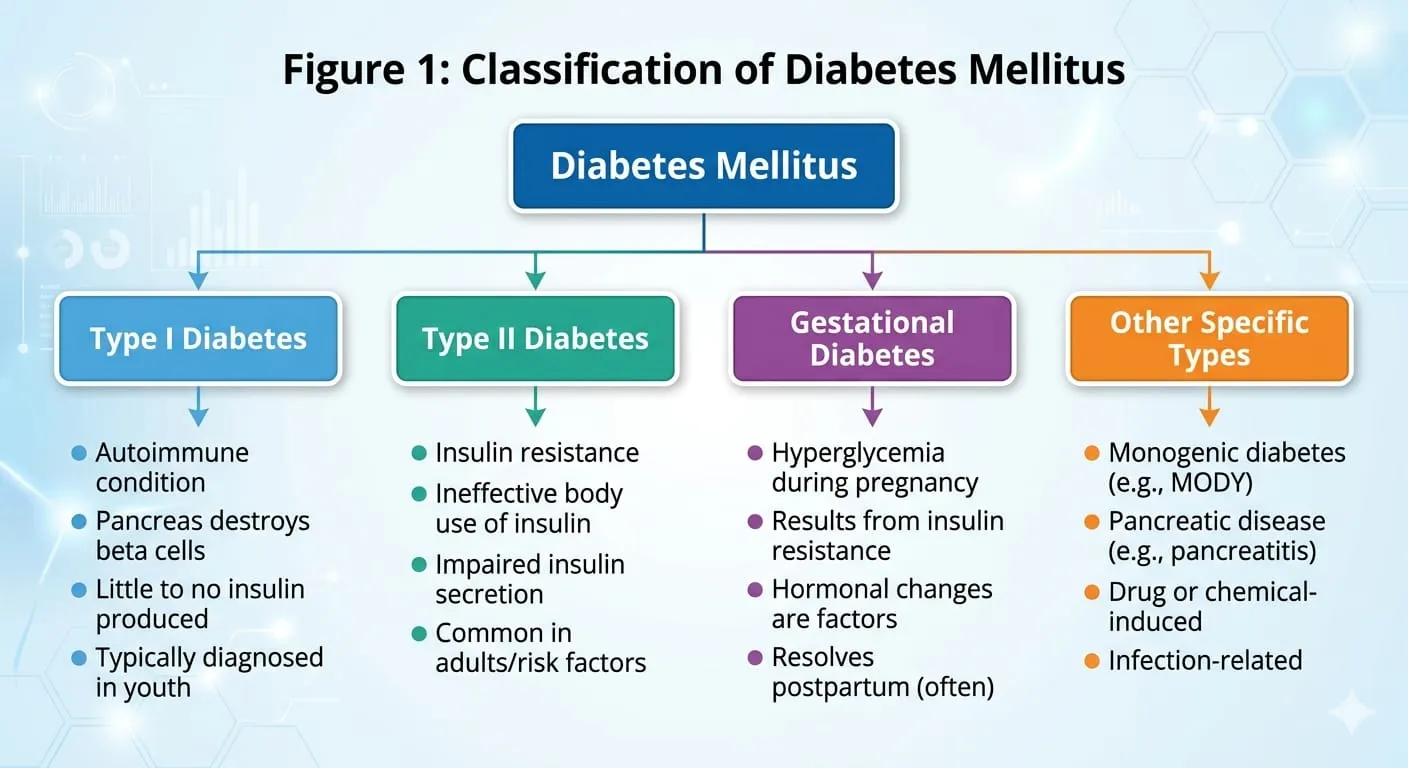
Dig.1.Classification of Diabetes Mellitus
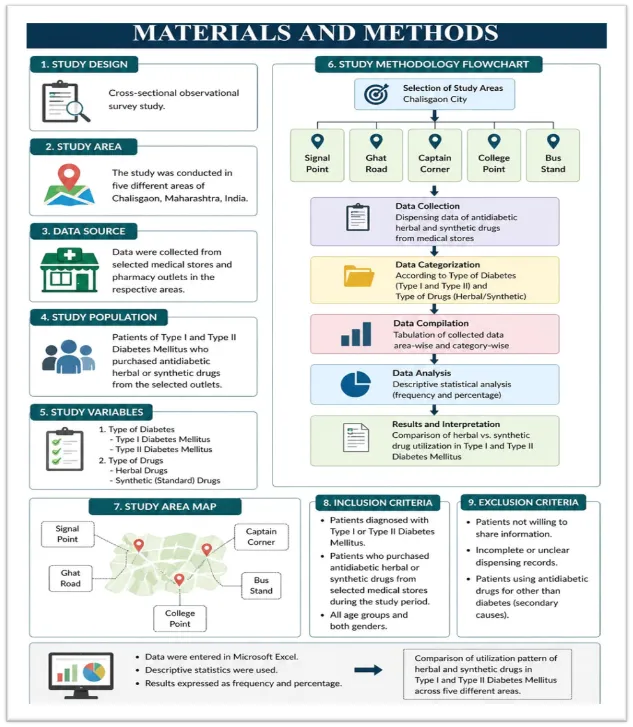
2. Materials & Methods
2.1 Study Design
Cross-sectional observational survey.
2.2 Study Area
Selected areas of Chalisgaon, Maharashtra:
2.3 Data Source
Utilization trend data were collected from selected medical stores/pharmacy outlets.
2.4 Study Variables
Data were categorized as:
2.5 Data Analysis
Data were compiled in tabular form and analysed using descriptive statistics such as totals, percentages, and comparative interpretation.
4. RESULT
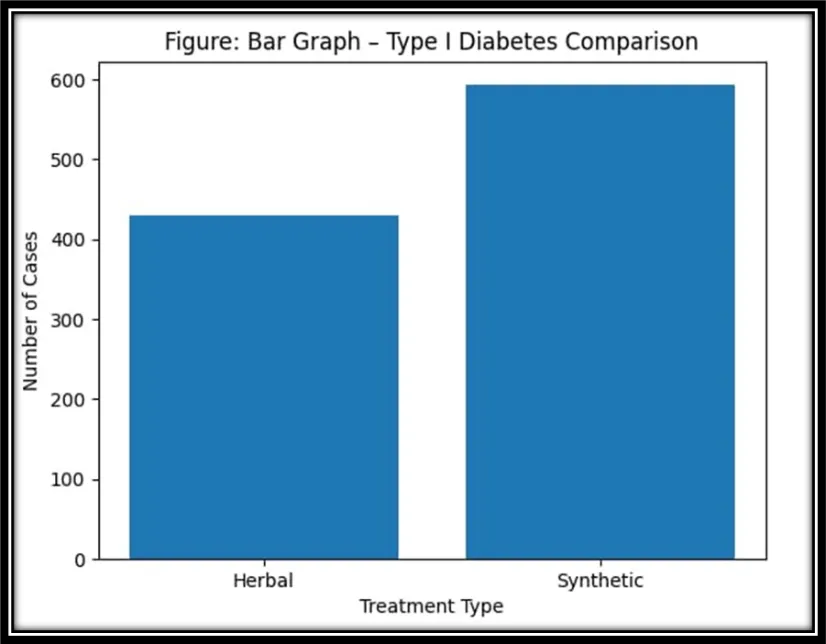
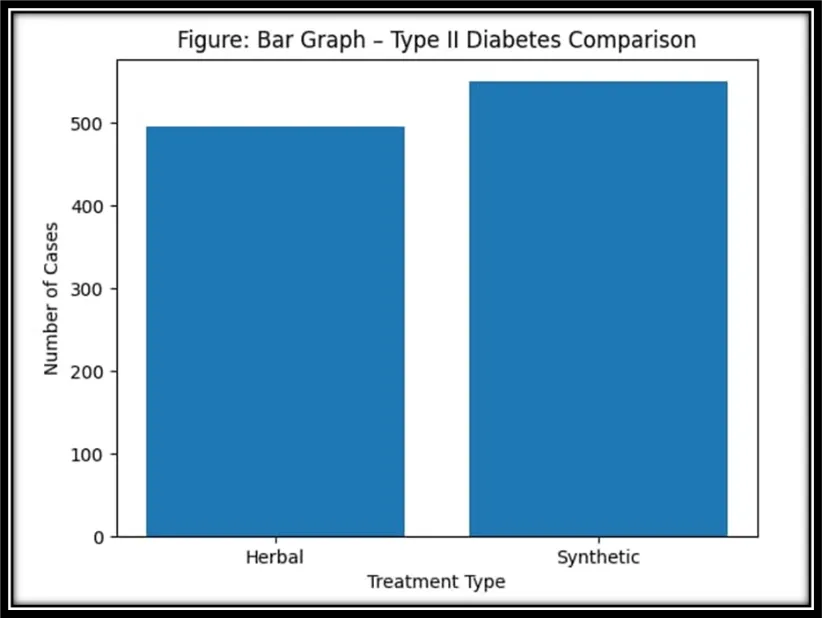
The result table presents the comparative utilization pattern of herbal and synthetic drugs used in the management of Type I and Type II Diabetes Mellitus across five selected areas of Chalisgaon, namely Signal Point, Ghat Road, Captain Corner, College Point, and Bus Stand. The findings indicate that in all study areas, the use of synthetic drugs was higher than herbal drugs for both Type I and Type II diabetes mellitus. In Type I diabetes, synthetic drug use ranged from 115 to 121 patients, whereas herbal drug use ranged from 82 to 90 patients. This suggests that synthetic therapy remains the preferred treatment option in Type I diabetes due to the clinical necessity of insulin and other standard medications. Among the selected areas, College Point recorded the highest use of synthetic drugs for Type I diabetes (121 patients), while Captain Corner showed the highest use of herbal drugs (90 patients). The lowest herbal utilization for Type I diabetes was observed at Signal Point (82 patients). In Type II diabetes mellitus, synthetic drug use varied from 108 to 112 patients, while herbal drug use ranged from 96 to 102 patients. Although synthetic drug utilization remained higher, the difference between herbal and synthetic drug use was smaller compared to Type I diabetes. This indicates an increased acceptance of herbal therapy among Type II diabetic patients. For Type II diabetes, Signal Point had the highest synthetic drug use (112 patients), while College Point showed the highest herbal drug use (102 patients). The lowest synthetic use was recorded at College Point (108 patients). The overall data suggest that synthetic drugs continue to dominate diabetes management because of their established efficacy and physician preference. However, the considerable use of herbal drugs, especially in Type II diabetes, reflects growing public awareness regarding natural therapies, lower cost, easy availability, and perceived safety. Thus, the result table clearly demonstrates a rising trend of herbal drug utilization alongside conventional synthetic treatment, particularly in the management of Type II diabetes mellitus.
Table 1. Area-wise Utilization Pattern
|
Area |
Type I (Herbal) |
TypeI (Synthetic) |
Type II (Herbal) |
Typr II (Synthetic) |
|
Signal Point |
82 |
118 |
96 |
112 |
|
Ghat Road |
88 |
120 |
101 |
109 |
|
Captain Corner |
90 |
115 |
98 |
110 |
|
College Point |
84 |
121 |
102 |
108 |
|
Bus Stand |
86 |
119 |
99 |
111 |
Table 2. Total Utilization
|
Category |
Herbal |
Synthetic |
|
Type I Diabetes |
430 |
593 |
|
Type II Diabetes |
496 |
550 |
|
Grand Total |
926 |
1143 |
Percentage Analysis
(A) Type I Diabetes
Herbal: 42.03%
Synthetic: 57.97%
(B) Type II Diabetes
Herbal: 47.42%
Synthetic: 52.58%
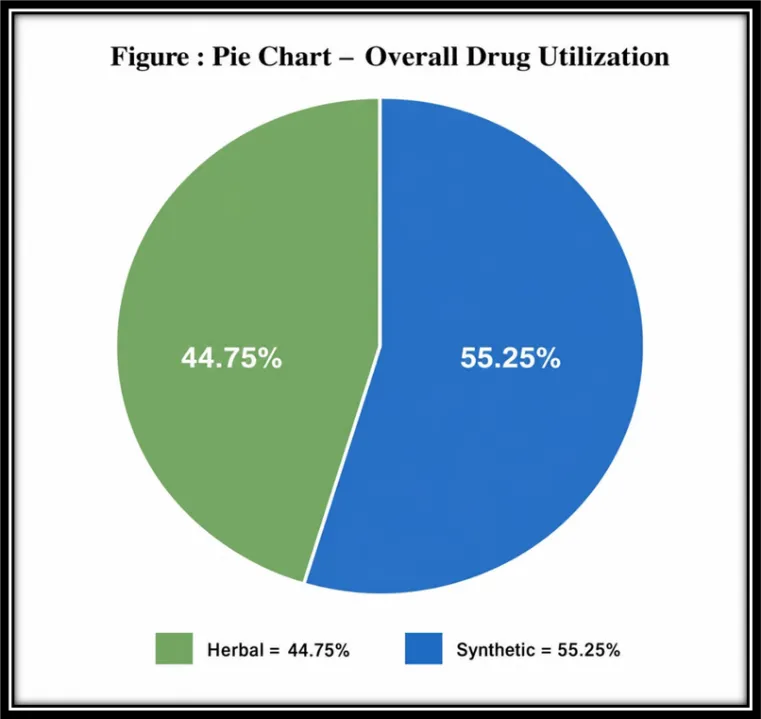
Overall
Herbal: 44.75%
Synthetic: 55.25%
5. DISCUSSION
The present study demonstrates that synthetic drugs remain the predominant therapeutic option in both Type I and Type II diabetes mellitus across selected areas of Chalisgaon. In Type I diabetes, synthetic utilization was markedly higher than herbal utilization. This trend is clinically justified because insulin and other standard therapies are essential in Type I diabetes due to absolute insulin deficiency. Herbal medicines may be used as supportive therapy but cannot replace insulin-based treatment28. In Type II diabetes, the difference between synthetic and herbal utilization was smaller, indicating relatively higher acceptance of herbal medicines among Type II patients. This may be due to the chronic nature of Type II diabetes, lifestyle-linked progression, and public perception that herbal medicines are safer for long-term use29. The use of herbal products may also be influenced by lower cost, local availability, cultural beliefs, and fewer reported side effects. Commonly used herbs such as cinnamon, ginger, fenugreek, black seed, and cardamom are frequently promoted for glycemic support30. Synthetic medicines still dominate because of stronger clinical evidence, physician prescribing habits, rapid glucose-lowering action, and standardized dosing31. The findings suggest a growing trend toward complementary therapy, especially in Type II diabetes. This creates opportunities for future evidence-based integrative management models31.
CONCLUSION
The study concludes that synthetic drugs are more commonly utilized than herbal drugs in the management of both Type I and Type II diabetes mellitus in selected areas of Chalisgaon. Synthetic therapy remains dominant, especially in Type I diabetes, where standard treatment is essential. Herbal drug utilization was comparatively higher in Type II diabetes, indicating increasing public interest in natural therapies for long-term disease management. Herbal medicines may serve as supportive or adjunctive treatment options when used rationally. An evidence-based combination of herbal and synthetic therapies may improve treatment outcomes, patient adherence, and quality of life. Further clinical studies are required to assess safety, efficacy, interactions, and long-term benefits of integrative diabetic care.
7. LIMITATIONS
8. FUTURE SCOPE
Development of integrative diabetic treatment models.
REFERENCES

M. M. Athar, Yash Shimpi*, Pavan Patil, Vishal Patil, Kirti Gadhari, Divyangana Tayade, Comparative Study of Herbal and Synthetic Drugs Used in the Management of Type I and Type II Diabetes Mellitus in Chalisgaon Area., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 8366-8374. https://doi.org/10.5281/zenodo.20478609
 10.5281/zenodo.20478609
10.5281/zenodo.20478609