
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Maharashtra Institute of Pharmacy, Betada, Bramhapuri, Chandrapur.
Diabetes mellitus is one of the most prevalent chronic metabolic disorders worldwide and continues to pose a significant challenge to global healthcare due to its increasing prevalence and associated complications. Conventional oral antidiabetic therapies often fail to provide optimal glycemic control because they do not account for circadian variations in glucose metabolism, particularly the early morning hyperglycemia known as the dawn phenomenon. Chronotherapeutic drug delivery has emerged as an effective strategy to synchronize drug release with the body's biological rhythms, thereby improving therapeutic outcomes. Among various chronotherapeutic approaches, pulsatile drug delivery systems have gained considerable attention because they provide a predetermined lag phase followed by rapid drug release at the desired time. Pellet-based formulations further enhance this approach by offering uniform gastrointestinal distribution, improved coating efficiency, reduced dose dumping, and flexible release characteristics. Teneligliptin, a potent and selective dipeptidyl peptidase-4 (DPP-4) inhibitor, possesses favorable pharmacokinetic and pharmacodynamic properties that make it an excellent candidate for pulsatile drug delivery. This review summarizes recent advances in chronotherapeutic drug delivery, pulsatile pellet technologies, pelletization techniques, formulation strategies, functional polymers, and the pharmacological profile of Teneligliptin. The article also discusses formulation optimization, evaluation methods, and recent research developments that support the potential of pulsatile pellet systems in diabetes management. Overall, pulsatile pellet-based delivery of Teneligliptin represents a promising strategy for improving glycemic control, enhancing patient compliance, and advancing personalized chronotherapeutic treatment of Type 2 diabetes mellitus.
Diabetes mellitus is one of the most prevalent chronic metabolic disorders worldwide and has become a major public health concern due to its rapidly increasing incidence and associated complications. The disease is characterized by persistent hyperglycemia resulting from impaired insulin secretion, insulin resistance, or a combination of both. Long-term uncontrolled diabetes can lead to serious microvascular and macrovascular complications, including nephropathy, retinopathy, neuropathy, and cardiovascular diseases, thereby significantly affecting the quality of life and increasing healthcare expenditure. Although several antidiabetic medications are available, conventional drug delivery systems often fail to provide optimal glycemic control because they do not consider the body's natural biological rhythms. Consequently, considerable attention has been directed toward chronotherapeutic drug delivery systems that synchronize drug release with circadian variations in disease activity. Among these approaches, pulsatile drug delivery systems have emerged as a promising strategy for improving therapeutic efficacy by delivering drugs at the most appropriate physiological time.[1]
1.1 Diabetes Mellitus: Global Burden
Diabetes mellitus is recognized as one of the fastest-growing non-communicable diseases worldwide. According to recent global estimates, the prevalence of diabetes continues to rise due to urbanization, sedentary lifestyles, obesity, population aging, and unhealthy dietary habits. Type 2 diabetes mellitus accounts for nearly 90–95% of all diabetes cases and represents a significant burden on healthcare systems. The increasing number of affected individuals has resulted in higher rates of disability, premature mortality, and economic costs. Effective disease management is therefore essential to reduce complications and improve long-term patient outcomes. [2]
Table 1. Global Burden of Diabetes Mellitus
|
Parameter |
Details |
|
Disease |
Diabetes Mellitus |
|
Major Type |
Type 2 Diabetes Mellitus (90–95%) |
|
Major Risk Factors |
Obesity, sedentary lifestyle, unhealthy diet, genetics |
|
Major Complications |
Nephropathy, neuropathy, retinopathy, cardiovascular disease |
|
Need |
Effective chronotherapeutic management |
1.2 Challenges in Conventional Antidiabetic Therapy
Despite the availability of numerous oral antidiabetic agents and insulin formulations, conventional therapy has several limitations. Immediate-release dosage forms often produce fluctuations in plasma drug concentration, resulting in periods of subtherapeutic or excessive drug exposure. These fluctuations may reduce treatment efficacy and increase the risk of adverse effects, including hypoglycemia. Furthermore, conventional dosage forms do not adequately address the circadian variation in glucose metabolism, particularly the early morning rise in blood glucose levels known as the dawn phenomenon. Frequent dosing and poor patient adherence further compromise therapeutic outcomes, highlighting the need for advanced drug delivery systems capable of providing time-specific drug release. [3]
1.3 Circadian Rhythm and Glucose Homeostasis
Circadian rhythms are endogenous biological cycles that regulate numerous physiological processes over approximately 24 hours. These rhythms are controlled by the central biological clock located in the suprachiasmatic nucleus of the hypothalamus and influence hormone secretion, metabolism, sleep–wake cycles, and glucose homeostasis. Blood glucose levels, insulin secretion, insulin sensitivity, and hepatic glucose production exhibit significant circadian variation throughout the day. Disruption of these biological rhythms has been associated with impaired glucose regulation and increased risk of metabolic disorders, including Type 2 diabetes mellitus. Therefore, aligning drug administration with circadian physiology offers an effective strategy for improving glycemic control. [4]
Table 2. Circadian Rhythm and Disease Activity
|
Disease |
Peak Symptom Time |
Chronotherapy Required |
|
Diabetes Mellitus |
Early morning |
Yes |
|
Hypertension |
Morning |
Yes |
|
Asthma |
Night/Early morning |
Yes |
|
Rheumatoid Arthritis |
Morning |
Yes |
1.4 Dawn Phenomenon and Chronotherapy
The dawn phenomenon refers to the spontaneous increase in blood glucose concentration during the early morning hours, typically occurring between 4:00 AM and 8:00 AM, without preceding nocturnal hypoglycemia. This physiological event is primarily caused by increased secretion of counter-regulatory hormones such as cortisol, growth hormone, glucagon, and catecholamines, which stimulate hepatic glucose production and reduce insulin sensitivity. In patients with Type 2 diabetes mellitus, this early morning hyperglycemia contributes to poor glycemic control and increases the risk of long-term diabetic complications. Chronotherapy aims to synchronize drug administration with the body's biological rhythms so that therapeutic drug concentrations are achieved precisely when they are most needed. This approach has shown considerable potential for improving treatment outcomes in patients experiencing the dawn phenomenon. [5]
1.5 Need for Pulsatile Drug Delivery
Pulsatile drug delivery systems have been developed to overcome the limitations of conventional sustained-release and immediate-release formulations. These systems are designed to provide a predetermined lag phase followed by rapid and complete drug release, thereby synchronizing drug availability with disease activity. In diabetes management, pulsatile formulations can be programmed to release antidiabetic drugs during the early morning hours when blood glucose levels rise due to the dawn phenomenon. Such time-controlled drug delivery minimizes unnecessary drug exposure during periods of low therapeutic requirement while enhancing efficacy during periods of maximum need. Consequently, pulsatile drug delivery systems represent a promising strategy for chronotherapeutic management of diabetes mellitus.
2. Chronotherapeutic Drug Delivery
Chronotherapeutic drug delivery is an advanced pharmaceutical approach that considers the influence of biological rhythms on disease progression and drug response. Instead of maintaining constant drug concentrations throughout the day, chronotherapeutic systems are designed to release medications at predetermined times corresponding to the body's circadian rhythms. This strategy enhances therapeutic efficacy while minimizing adverse effects by ensuring that drug availability coincides with periods of greatest disease activity. Chronotherapeutic drug delivery has gained considerable importance in the management of chronic disorders such as diabetes mellitus, hypertension, asthma, arthritis, and cardiovascular diseases. [6]
2.1 Concept of Chronotherapy
Chronotherapy refers to the administration of medications according to the body's biological clock to optimize therapeutic outcomes. Since many physiological functions and pathological conditions exhibit circadian variation, delivering drugs at the appropriate time can significantly improve efficacy and reduce toxicity. Chronotherapy integrates principles of chronobiology and pharmacotherapy to achieve maximum clinical benefit while minimizing adverse drug reactions. This concept has become increasingly important in the development of advanced drug delivery systems capable of programmed and time-dependent drug release. [7]
2.2 Circadian Rhythm in Drug Therapy
Circadian rhythms influence several pharmacokinetic and pharmacodynamic processes, including drug absorption, distribution, metabolism, excretion, receptor sensitivity, and enzyme activity. As a result, the therapeutic response to many medications varies depending on the time of administration. Drug delivery systems that account for these biological variations can provide improved disease management by ensuring that medications are released during periods of maximum therapeutic need. Incorporating circadian principles into pharmaceutical formulation has therefore become an important aspect of modern drug delivery research. [8]
2.3 Diseases Benefiting from Chronotherapy
Diabetes Mellitus
Chronotherapeutic drug delivery plays an important role in diabetes management by addressing circadian fluctuations in blood glucose levels, particularly the early morning hyperglycemia associated with the dawn phenomenon. Timed drug release improves glycemic control while reducing the risk of hypoglycemia and enhancing patient compliance.
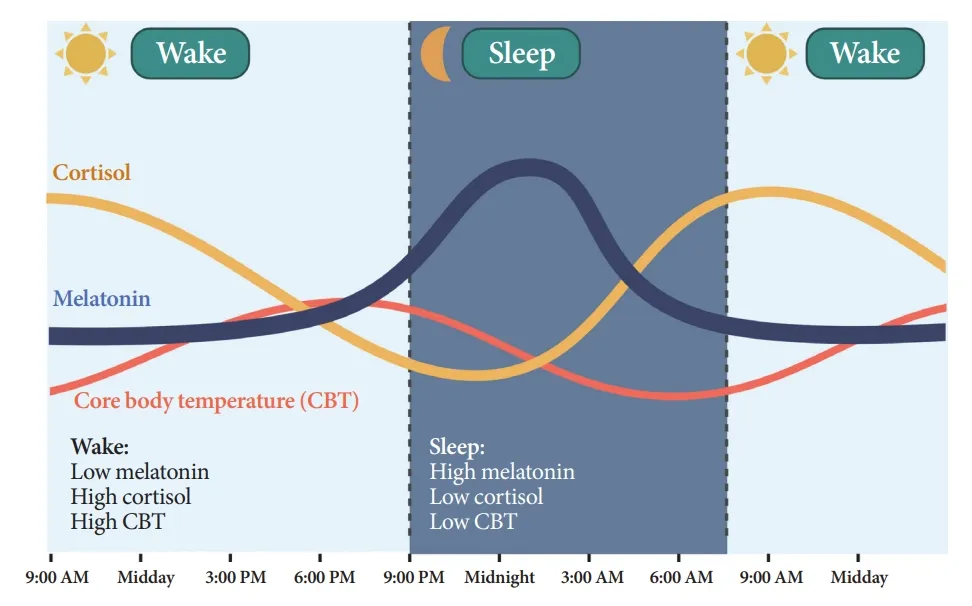
Figure 1: Circadian Rhythm of Blood Glucose Levels
Hypertension
Blood pressure exhibits marked circadian variation, with a significant rise during the early morning hours that increases the risk of myocardial infarction and stroke. Chronotherapy enables antihypertensive drugs to achieve peak plasma concentrations during this high-risk period, thereby improving cardiovascular protection. [9]
Asthma
Asthma symptoms typically worsen during the night and early morning because of circadian changes in airway inflammation and bronchial responsiveness. Chronotherapeutic formulations can deliver bronchodilators and anti-inflammatory agents when respiratory symptoms are most severe, resulting in better disease control and improved pulmonary function.
Arthritis
Patients with rheumatoid arthritis frequently experience severe joint pain, stiffness, and inflammation during the early morning hours due to circadian variation in inflammatory cytokine production. Chronotherapeutic drug delivery allows anti-inflammatory medications to be released before symptom onset, reducing morning stiffness and improving joint mobility and overall quality of life. [10]
3. Pulsatile Drug Delivery Systems
Pulsatile drug delivery systems (PDDS) are advanced pharmaceutical formulations specifically designed to release drugs after a predetermined lag period followed by rapid and complete drug release. Unlike conventional sustained- or controlled-release formulations that maintain relatively constant drug concentrations, pulsatile systems synchronize drug release with the body's biological rhythms or the onset of disease symptoms. This approach is particularly beneficial for disorders exhibiting circadian variation, such as diabetes mellitus, hypertension, asthma, and rheumatoid arthritis. By delivering the drug at the time when it is most therapeutically required, pulsatile drug delivery enhances treatment efficacy, minimizes adverse effects, and improves patient compliance. Owing to these advantages, PDDS has emerged as an important area of research in chronotherapeutic drug delivery. [11]
Table 2. Circadian Rhythm and Disease Activity
|
Disease |
Peak Symptom Time |
Chronotherapy Required |
|
Diabetes Mellitus |
Early morning |
Yes |
|
Hypertension |
Morning |
Yes |
|
Asthma |
Night/Early morning |
Yes |
|
Rheumatoid Arthritis |
Morning |
Yes |
3.1 Definition
A pulsatile drug delivery system is a modified-release dosage form that provides a programmed lag time before the rapid release of the active pharmaceutical ingredient. The system is designed to maintain minimal or no drug release during the lag phase and subsequently deliver the drug as a pulse at the desired time. This time-controlled release profile enables synchronization of drug availability with circadian rhythms and disease progression, thereby improving therapeutic effectiveness while reducing unnecessary drug exposure. [12]
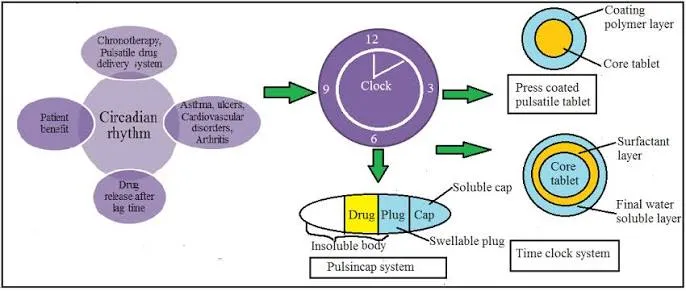
Figure 2: Pulsatile drug delivery system
3.2 Principle
The fundamental principle of pulsatile drug delivery is to release the drug only when it is required rather than maintaining continuous drug levels in the systemic circulation. A predetermined lag time is incorporated into the formulation using specialized polymers or release-controlling mechanisms. After completion of this lag phase, the formulation undergoes rapid disintegration, swelling, erosion, membrane rupture, osmotic pressure development, or enzymatic degradation, leading to immediate drug release. The duration of the lag time can be adjusted according to the pharmacological requirements of the drug and the circadian pattern of the target disease. This strategy allows maximum therapeutic benefit while minimizing systemic adverse effects. [13]
3.3 Advantages
Pulsatile drug delivery systems provide several therapeutic and pharmaceutical advantages over conventional dosage forms. The most important benefit is the synchronization of drug release with the body's biological rhythms, resulting in improved clinical efficacy. These systems effectively manage diseases characterized by circadian variation, particularly early morning hyperglycemia in diabetes mellitus. Pulsatile formulations reduce unnecessary drug exposure during periods of low therapeutic demand, thereby minimizing adverse effects and drug tolerance. They also improve patient compliance by decreasing dosing frequency and enabling predictable drug release. Furthermore, multiparticulate pulsatile systems reduce the risk of dose dumping, provide uniform gastrointestinal distribution, and exhibit lower inter-patient variability. Their flexibility in formulation design makes them suitable for a wide range of therapeutic agents requiring time-specific drug delivery. [14]
3.4 Limitations
Despite their numerous advantages, pulsatile drug delivery systems possess certain limitations that restrict their widespread clinical application. The formulation and manufacturing processes are relatively complex and require precise optimization of polymers, coating thickness, and lag time. Specialized equipment and sophisticated coating technologies increase production costs compared with conventional dosage forms. Variations in gastrointestinal pH, motility, and gastric emptying time may influence the performance of oral pulsatile formulations. Achieving reproducible lag time and uniform coating remains a major formulation challenge. In addition, large-scale manufacturing, quality control, and regulatory approval require extensive evaluation to ensure product consistency and therapeutic reliability. [15]
3.5 Mechanism of Pulsatile Drug Release
The drug release mechanism in pulsatile systems depends on the design of the formulation and the triggering stimulus. In swelling-controlled systems, hydrophilic polymers absorb gastrointestinal fluids and expand until the outer barrier ruptures, resulting in rapid drug release. Erosion-controlled systems utilize biodegradable polymers that gradually dissolve to expose the drug-containing core after a specific time interval. Osmotic systems generate internal pressure through water uptake, leading to membrane rupture and pulsatile drug release. In pH-dependent systems, enteric polymers dissolve only after exposure to specific gastrointestinal pH conditions, thereby providing site-specific release. Enzyme-triggered formulations employ biodegradable materials that are degraded by intestinal or colonic enzymes before releasing the drug. Rapture-controlled systems rely on increasing internal pressure to rupture the surrounding coating membrane and release the drug rapidly after the programmed lag period. These mechanisms enable accurate control of drug release timing and make pulsatile systems highly suitable for chronotherapeutic applications.
4. Classification of Pulsatile Drug Delivery Systems
Pulsatile drug delivery systems can be classified according to the mechanism responsible for triggering drug release. Different formulation strategies have been developed to achieve a specific lag time followed by rapid drug release. Selection of the appropriate system depends on the physicochemical properties of the drug, disease characteristics, site of drug absorption, and therapeutic objectives. The major classes of pulsatile drug delivery systems include time-controlled systems, stimuli-induced systems, pH-dependent systems, enzyme-triggered systems, osmotic systems, and rupturable systems. [16]
4.1 Time-Controlled Systems
Time-controlled pulsatile systems are designed to release the drug after a predetermined lag period irrespective of physiological conditions. The lag time is generally controlled by polymer coatings, hydrophilic barriers, or erodible layers. Following completion of the programmed delay, the formulation rapidly releases the drug. These systems are widely employed for chronotherapeutic management of diseases exhibiting predictable circadian rhythms and are particularly suitable for oral pulsatile formulations. [17]
4.2 Stimuli-Induced Systems
Stimuli-induced pulsatile drug delivery systems release the drug in response to specific internal or external stimuli. Internal triggers include changes in pH, enzyme concentration, glucose level, inflammatory mediators, and temperature, whereas external triggers may involve magnetic fields, ultrasound, electrical stimulation, or light. These intelligent drug delivery systems offer site-specific and patient-responsive therapy, making them attractive for future personalized medicine applications. [18]
4.3 pH-Dependent Systems
pH-dependent pulsatile systems utilize enteric polymers that remain intact in the acidic environment of the stomach but dissolve at higher pH values encountered in the intestine or colon. Commonly used polymers include Eudragit® L100, Eudragit® S100, cellulose acetate phthalate, and hydroxypropyl methylcellulose phthalate. These systems protect acid-sensitive drugs and permit site-specific as well as time-controlled drug release.
4.4 Enzyme-Triggered Systems
Enzyme-triggered drug delivery systems depend on the enzymatic activity of the gastrointestinal microflora to initiate drug release. Biodegradable polymers such as pectin, chitosan, guar gum, dextran, and amylose undergo degradation by bacterial enzymes in the colon, leading to rapid release of the incorporated drug. These formulations are particularly useful for colon-targeted chronotherapy and treatment of diseases requiring delayed drug release. [19]
4.5 Osmotic Systems
Osmotic pulsatile drug delivery systems operate through osmotic pressure generated after water enters the dosage form across a semipermeable membrane. As internal pressure gradually increases, the outer membrane ruptures or expels the drug through a delivery orifice, resulting in a pulsatile release profile. Osmotic systems provide highly reproducible lag times and are less influenced by physiological variables, making them reliable controlled-release formulations.
4.6 Rupturable Systems
Rupturable pulsatile systems consist of a drug-containing core surrounded by a polymeric coating that ruptures after a predetermined lag period. Water penetration into the formulation causes swelling of superdisintegrants or gas-generating agents, leading to increased internal pressure. Once the mechanical strength of the coating is exceeded, the membrane ruptures and the drug is released rapidly. Because of their simplicity, reproducibility, and ability to provide accurate lag times, rupturable systems are among the most extensively investigated approaches for chronotherapeutic drug delivery. [20]
Table 4. Classification of Pulsatile Drug Delivery Systems
|
System |
Principle |
Example |
|
Time-controlled |
Polymer erosion/swelling |
Coated pellets |
|
pH-dependent |
pH-sensitive polymers |
Eudragit L/S |
|
Osmotic |
Osmotic pressure |
OROS |
|
Enzyme-triggered |
Enzymatic degradation |
Colon-targeted systems |
|
Rupturable |
Membrane rupture |
Press-coated tablets |
|
Stimuli-induced |
Internal/External stimulus |
Smart drug delivery |
5. Pellet-Based Drug Delivery Systems
5.1 Introduction
Pellet-based drug delivery systems are multiparticulate dosage forms composed of small, free-flowing spherical particles, typically ranging from 500 to 1500 μm in diameter. These systems offer improved drug distribution within the gastrointestinal tract, enhanced bioavailability, and reduced variability in drug absorption. Their ability to provide immediate, controlled, delayed, or pulsatile drug release makes them highly suitable for chronotherapeutic applications. Owing to their excellent flow properties, uniform coating, and formulation flexibility, pellet-based systems have become an important platform for developing advanced oral drug delivery systems. [21]
5.2 Types of Pellets
Pellets are broadly classified into matrix pellets, reservoir pellets, drug-layered pellets, coated pellets, and multiparticulate pellet systems. Matrix pellets contain the drug uniformly dispersed throughout the formulation, whereas reservoir pellets consist of a drug core surrounded by a polymer coating that controls drug release. Drug-layered and coated pellets are commonly employed for modified-release formulations, while multiparticulate systems provide better gastrointestinal distribution and improved therapeutic performance. [22]
5.3 Advantages
Pellet-based drug delivery systems provide several advantages over conventional dosage forms. They exhibit excellent flowability, uniform drug distribution, and reduced risk of dose dumping. Their multiparticulate nature ensures consistent gastrointestinal transit and minimizes local irritation. Furthermore, pellets are easy to coat, allowing precise control of drug release and making them highly suitable for sustained, delayed, and pulsatile drug delivery applications. [23]
5.4 Pelletization Techniques
Various pelletization techniques are employed to produce pharmaceutical pellets with desired physical and release characteristics. Among these, extrusion–spheronization is the most widely used technique due to its ability to produce highly spherical and mechanically strong pellets. Drug layering involves depositing the drug onto inert cores using a binder solution, while powder layering builds successive layers of drug powder and binder onto starter pellets. Solution or suspension layering provides uniform drug coating through fluidized-bed processing. Spray drying rapidly converts drug solutions into spherical microparticles by solvent evaporation, whereas hot melt extrusion produces pellets by processing drug–polymer mixtures under controlled heat and pressure without the use of organic solvents. These techniques provide flexibility in designing pellet formulations with desired release profiles for chronotherapeutic drug delivery. [24]
Table 5. Pelletization Techniques
|
Technique |
Principle |
Advantages |
|
Extrusion–Spheronization |
Wet mass extrusion |
Uniform pellets |
|
Drug Layering |
Drug coated on cores |
Uniform drug loading |
|
Powder Layering |
Powder deposition |
High drug loading |
|
Solution/Suspension Layering |
Spray coating |
Uniform coating |
|
Spray Drying |
Rapid solvent evaporation |
Fine spherical particles |
|
Hot Melt Extrusion |
Melt processing |
Solvent-free process |
6. Polymers Used in Pulsatile Pellet Systems
Polymers are essential components in pulsatile pellet formulations because they regulate lag time, control drug release, improve mechanical strength, and enhance formulation stability. Appropriate selection and optimization of polymers enable synchronization of drug release with the body's circadian rhythm, thereby improving the therapeutic efficacy of chronotherapeutic drug delivery systems. [25]
6.1 Hydroxypropyl Methylcellulose (HPMC)
Hydroxypropyl methylcellulose (HPMC) is a hydrophilic polymer widely used as a release-controlling agent in modified-release formulations. It hydrates rapidly upon contact with gastrointestinal fluids, forming a gel layer that regulates water penetration and drug diffusion. Owing to its excellent swelling properties and biocompatibility, HPMC is extensively used in pulsatile drug delivery systems. [26]
6.2 Ethyl Cellulose
Ethyl cellulose is a water-insoluble polymer commonly employed as a sustained-release coating material. It forms a strong diffusion barrier around pellet cores, thereby delaying drug release and providing the desired lag time. Its excellent film-forming properties and chemical stability make it suitable for chronotherapeutic formulations. [27]
6.3 Eudragit RS
Eudragit RS is a water-insoluble but slightly permeable acrylic polymer used for controlled-release drug delivery. Its low permeability allows gradual penetration of gastrointestinal fluids, resulting in prolonged and controlled drug release. It is frequently combined with other polymers to optimize lag time in pulsatile systems.
6.4 Eudragit RL
Eudragit RL is an acrylic polymer with higher permeability than Eudragit RS due to a greater concentration of quaternary ammonium groups. It permits faster water uptake and drug diffusion while maintaining controlled-release characteristics. The combination of Eudragit RL and RS provides flexibility in designing desired release profiles. [28]
6.5 Eudragit L/S
Eudragit L and Eudragit S are pH-dependent enteric polymers that remain intact in acidic gastric conditions and dissolve at intestinal pH. These polymers protect acid-sensitive drugs and provide site-specific as well as delayed drug release. They are widely used in chronotherapeutic and colon-targeted drug delivery systems.
6.6 Polyvinylpyrrolidone (PVP)
Polyvinylpyrrolidone (PVP) is a water-soluble polymer primarily used as a binder during pellet preparation. It enhances particle cohesion, improves mechanical strength, and promotes uniform drug distribution within the pellet matrix. PVP also contributes to better processing characteristics during extrusion–spheronization. [29]
6.7 Microcrystalline Cellulose (MCC)
Microcrystalline cellulose (MCC) is one of the most widely used pelletization aids in pharmaceutical formulations. It possesses excellent binding and plasticity properties, facilitating the formation of spherical pellets with high mechanical strength. MCC also improves flowability, compressibility, and overall pellet quality, making it an indispensable excipient in extrusion–spheronization-based pellet formulations. [30]
Table 6. Polymers Used in Pulsatile Pellet Systems
|
Polymer |
Function |
Application |
|
HPMC |
Swelling polymer |
Controlled release |
|
Ethyl Cellulose |
Hydrophobic polymer |
Lag time control |
|
Eudragit RS |
Low permeability |
Sustained release |
|
Eudragit RL |
High permeability |
Controlled release |
|
Eudragit L/S |
Enteric polymer |
pH-dependent release |
|
PVP K-30 |
Binder |
Pellet formation |
|
MCC |
Pelletization aid |
Extrusion–spheronization |
7. Teneligliptin: Pharmacological Overview
7.1 Introduction
Teneligliptin is a potent and selective dipeptidyl peptidase-4 (DPP-4) inhibitor used for the treatment of Type 2 diabetes mellitus. It improves glycemic control by increasing endogenous incretin hormone levels, thereby enhancing glucose-dependent insulin secretion and suppressing glucagon release. Its favorable pharmacokinetic profile and prolonged duration of action make it a promising candidate for modified and pulsatile drug delivery systems. [31]
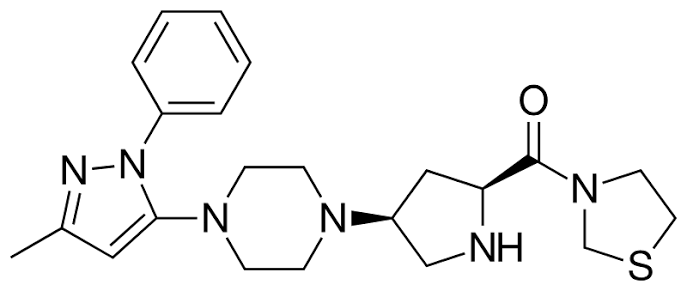
Figure 3: Teneligliptin chemical structure
7.2 Mechanism of Action
Teneligliptin inhibits the DPP-4 enzyme responsible for the degradation of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). Increased concentrations of these incretin hormones stimulate insulin secretion and reduce glucagon release in a glucose-dependent manner, leading to effective control of blood glucose levels with a low risk of hypoglycemia. [32]
7.3 Pharmacokinetics
Teneligliptin is rapidly absorbed following oral administration and reaches peak plasma concentration within approximately one to two hours. It has a relatively long elimination half-life, allowing once-daily dosing. The drug undergoes both hepatic metabolism and renal excretion, reducing the need for dose adjustment in many patients with renal impairment. [33]
7.4 Pharmacodynamics
The pharmacological activity of Teneligliptin is characterized by sustained inhibition of the DPP-4 enzyme, resulting in prolonged elevation of active incretin hormones. This enhances insulin secretion, suppresses hepatic glucose production, and improves both fasting and postprandial blood glucose levels, contributing to effective long-term glycemic control. [34]
7.5 Clinical Applications
Teneligliptin is indicated for the management of Type 2 diabetes mellitus as monotherapy or in combination with other oral antidiabetic agents or insulin. It is particularly useful in patients who require improved glycemic control with a low incidence of hypoglycemia and favorable tolerability.
7.6 Advantages over Other DPP-4 Inhibitors
Compared with several other DPP-4 inhibitors, Teneligliptin exhibits high binding affinity, prolonged enzyme inhibition, and an extended duration of action. It demonstrates effective glycemic control, good cardiovascular safety, and minimal risk of hypoglycemia. Its dual elimination pathway also offers therapeutic advantages in patients with mild to moderate renal dysfunction. [35]
7.7 Rationale for Pulsatile Delivery
The circadian variation in blood glucose levels, particularly the early morning hyperglycemia associated with the dawn phenomenon, provides a strong rationale for developing pulsatile formulations of Teneligliptin. A programmed lag time followed by rapid drug release can synchronize peak drug concentration with the period of greatest therapeutic need. This chronotherapeutic approach may improve glycemic control, reduce unnecessary drug exposure, and enhance overall treatment efficacy in patients with Type 2 diabetes mellitus.
Table 7. Pharmacological Profile of Teneligliptin
|
Parameter |
Description |
|
Drug Class |
DPP-4 Inhibitor |
|
Indication |
Type 2 Diabetes Mellitus |
|
Mechanism |
DPP-4 inhibition |
|
Half-life |
Approximately 24 h |
|
Dosing |
Once daily |
|
Major Advantage |
Low risk of hypoglycemia |
8. Formulation Strategies for Teneligliptin Pulsatile Pellets
The successful development of Teneligliptin pulsatile pellets requires careful selection of formulation components and process parameters to achieve the desired lag time followed by rapid drug release. The formulation strategy involves preparation of core pellets, application of functional polymer coatings, and optimization of release characteristics to synchronize drug delivery with the circadian rhythm associated with Type 2 diabetes mellitus. [36]
8.1 Core Pellet Formulation
Core pellets are prepared by blending Teneligliptin with suitable excipients such as microcrystalline cellulose, lactose, and polyvinylpyrrolidone. The powder mixture is converted into a wet mass and processed by extrusion–spheronization to obtain spherical pellets with good mechanical strength, uniform particle size, and satisfactory drug content. [37]
8.2 Coating Technologies
Polymer coating is a critical step in the development of pulsatile pellets. Functional polymers such as Ethyl Cellulose, Eudragit RS, and Eudragit RL are applied using fluidized-bed coating techniques to create a diffusion barrier around the core pellets. The coating thickness determines the lag time before drug release and plays an important role in achieving chronotherapeutic delivery. [38]
8.3 Polymer Optimization
Optimization of polymer type and concentration is essential to obtain the desired release profile. Hydrophobic polymers delay drug release, whereas more permeable polymers allow controlled penetration of dissolution medium. Appropriate combinations of polymers provide the required lag time while ensuring rapid drug release after the programmed delay. [39]
8.4 Lag Time Optimization
Lag time is optimized by modifying the coating composition and thickness. The objective is to delay drug release until the early morning hours, thereby matching the rise in blood glucose levels associated with the dawn phenomenon. An optimized lag time improves therapeutic efficacy and minimizes unnecessary drug exposure.
8.5 Drug Release Optimization
Drug release behavior is evaluated through dissolution studies, and formulation variables are adjusted to obtain rapid and complete drug release following the predetermined lag period. Optimization ensures reproducible release kinetics, improved bioavailability, and effective chronotherapeutic management of diabetes mellitus.
Table 8. Advantages of Pellet-Based Drug Delivery Systems
|
Advantage |
Benefit |
|
Uniform GI distribution |
Better absorption |
|
Reduced dose dumping |
Improved safety |
|
Better coating efficiency |
Controlled release |
|
Improved flowability |
Easy manufacturing |
|
High drug loading |
Better formulation flexibility |
|
Better patient compliance |
Reduced dosing frequency |
9. Evaluation Parameters [40]
Evaluation of pulsatile pellet formulations is essential to ensure their quality, performance, and therapeutic effectiveness. Various preformulation, physical, and in vitro studies are carried out to assess the characteristics of both core pellets and coated pellets.
9.1 Preformulation Studies
Preformulation studies provide information regarding the physicochemical properties of the drug and its compatibility with selected excipients. Parameters such as appearance, solubility, melting point, FTIR analysis, DSC analysis, and drug–excipient compatibility are evaluated to ensure formulation stability and suitability for pellet preparation.
9.2 Pellet Evaluation
Particle Size
Particle size distribution is determined using sieve analysis to ensure uniformity of pellet diameter. Uniform particle size contributes to consistent coating efficiency and reproducible drug release.
Flow Properties
The flowability of pellets is evaluated by determining the angle of repose, bulk density, tapped density, Carr's compressibility index, and Hausner ratio. Good flow characteristics facilitate uniform coating and capsule filling.
Friability
Friability testing assesses the mechanical strength of pellets during handling and processing. Pellets with low friability exhibit better resistance to abrasion and maintain their structural integrity throughout manufacturing.
Drug Content
Drug content analysis is performed using UV-visible spectrophotometry or HPLC to determine the amount of Teneligliptin present in the pellets. Uniform drug content confirms proper mixing and consistent formulation quality.
9.3 Coated Pellet Evaluation
Lag Time
Lag time is measured during dissolution studies to determine the delay before the initiation of drug release. This parameter is critical for achieving chronotherapeutic drug delivery.
Dissolution Study
In vitro dissolution studies are performed using USP dissolution apparatus under simulated gastrointestinal conditions. The release profile is evaluated to confirm the programmed lag phase followed by rapid drug release.
Release Kinetics
Drug release data are fitted to various kinetic models, including zero-order, first-order, Higuchi, Korsmeyer–Peppas, and Hixson–Crowell models, to understand the mechanism governing drug release.
Stability Study
Stability studies are conducted according to ICH guidelines under accelerated storage conditions to evaluate the physical appearance, drug content, dissolution behavior, and overall stability of the optimized formulation over the specified storage period. These studies confirm the formulation's ability to maintain its quality, safety, and therapeutic performance during storage.
Table 9. Evaluation Parameters
|
Evaluation |
Purpose |
|
FTIR |
Drug–excipient compatibility |
|
DSC |
Thermal behavior |
|
Particle Size |
Pellet uniformity |
|
Flow Properties |
Processability |
|
Friability |
Mechanical strength |
|
Drug Content |
Content uniformity |
|
Dissolution |
Drug release profile |
|
Release Kinetics |
Release mechanism |
|
Stability Study |
Shelf-life assessment |
DISCUSSION
The reviewed literature demonstrates that pulsatile pellet-based drug delivery systems offer an effective approach for chronotherapeutic management of Type 2 diabetes mellitus. Conventional oral dosage forms often fail to address the early morning rise in blood glucose levels associated with the dawn phenomenon. In contrast, pulsatile formulations provide a predetermined lag time followed by rapid drug release, ensuring drug availability at the most appropriate therapeutic period. Pellet-based systems further enhance treatment by providing uniform gastrointestinal distribution, improved bioavailability, reduced dose dumping, and reproducible drug release. Among DPP-4 inhibitors, Teneligliptin exhibits favorable pharmacokinetic and pharmacodynamic properties, making it a suitable candidate for pulsatile drug dAelivery. Appropriate selection of polymers such as HPMC, Ethyl Cellulose, and Eudragit grades enables precise modulation of lag time and release characteristics. Overall, the available evidence suggests that pulsatile pellet systems have significant potential to improve glycemic control, therapeutic efficacy, and patient compliance.
CONCLUSION
Pulsatile pellet-based drug delivery systems represent a promising strategy for the chronotherapeutic management of Type 2 diabetes mellitus. The integration of pellet technology with time-dependent polymer coatings enables synchronized drug release in accordance with circadian variations in blood glucose levels. Teneligliptin possesses suitable pharmacological characteristics for incorporation into pulsatile formulations due to its potent DPP-4 inhibition, prolonged duration of action, and favorable safety profile. Recent advances in formulation techniques and polymer technologies have further enhanced the development of efficient pulsatile pellet systems. Therefore, this approach offers considerable potential for improving therapeutic outcomes, minimizing adverse effects, and supporting the future development of personalized chronotherapeutic drug delivery systems.
REFERENCES



Supriya Gawade, Dr. Sachin Dudhe, Dr. Anup Barsagade, Design, Development and Evaluation of Pulsatile Pellet-Based Drug Delivery System of Teneligliptin for Chronotherapeutic Management of Diabetes Mellitus: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 3069-3085, https://doi.org/10.5281/zenodo.21376270
 10.5281/zenodo.21376270
10.5281/zenodo.21376270