
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology, Karnataka College of Pharmacy, Bengaluru, Karnataka, India.
Urolithiasis, often known as kidney stone disease, is a multifactorial condition that affects 10–15% of people worldwide and has a high recurrence rate. The complex relationships between biological phenomena, including oxidative stress, renal epithelial injury, and the role of urinary macromolecules like osteopontin, as well as physicochemical aspects like supersaturation, nucleation, and aggregation, are reviewed. The review also highlights the strong correlation between systemic metabolic diseases like diabetes, obesity, hyperparathyroidism, and renal disease, which are significantly related with urolithiasis. The clinical manifestation of the disease includes UTIs, hematuria, and renal colic. The review also includes the different treatment options, including pharmacological, surgical, as well as non-pharmacological, which are important in the management of urolithiasis. Finally, the review also discusses emerging treatment options that aim to provide more focused, efficient, and effective management of urolithiasis, including the modulation of the microbiome and the use of nanotechnology
The kidney stone disease or urolithiasis can be described as the multifactorial disease with the development of calculi in the urethra and is prevalent in close to 10-15% of the world population with high recurrence rates 1. The illness is a major burden on healthcare systems due to its rising incidence, particularly in emerging nations, and its association with metabolic, genetic, and environmental risk factors 2. Disease-related urolithiasis is frequently linked to the systemic conditions of diabetes mellitus, obesity, hyperparathyroidism, and renal tubular acidosis, which alters the composition of the urine and promotes the formation of stones 3.
In the end, this process is a complex interplay of physicochemical and biological phenomena at the molecular level, including the supersaturation of urine with components that form stones, nucleation, crystal formation, aggregation, and retention in renal tubules 4. These modulators include calcium, oxalate, uric acid and phosphate ions that are considered to play a major role in the formation of crystals and a shortage of natural inhibitors like citrate and magnesium compounds only adds to the process further 5.
Besides, oxidative stress and renal epithelial damage are also essential in crystal adhesion and retention mediated by reactive oxygen species and proinflammatory processes 6.
The relative roles of proteins, osteopontin, Tamm-Horsfall protein, and different cytokines in the pathophysiology of kidney stones have been highlighted by recent advances in molecular biology, indicating that urolithiasis is both a physicochemical phenomenon and a cell-mediated pathological process7. Moreover, individual predisposition has been demonstrated to be affected by genetic predisposition and epigenetic alteration 8.
Clinically, urolithiasis can cause severe flank pain (renal colic), haematuria, nausea, and urinary tract infections. It can also be asymptomatic and unintentionally discovered when using imaging techniques 9. Stone recurrence is a significant clinical issue and requires the use of long-term management plans that prevent the recurrence 10.
Several drugs affect urinary supersaturation like thiazide diuretics, potassium citrate and allopurinol, among others, depending on the type of stone 11. Further, novel treatments against oxidative stress, inflammation and adhesion of crystal are also getting some attention as potential means of prevention of stone formation and stone recurrence 12. Although the treatment process is enhanced, in-depth understanding of the processes surrounding the disease plays a very important role in designing improved and targeted treatment procedures.
2.1 Epidemiology
Age, gender, and race have been proven to be factors in the development of a person's first kidney stone. The risk of kidney stone formation has been calculated through the examination of clinical medical data or the use of a diagnostic code system 13. These determinants are dependent on the geographical location as well as the socioeconomic status. This is why urolithiasis does not have an equal rate throughout the world. According to studies conducted in other nations, 5–15% of people have urolithiasis 14. There were 106 million incident instances of urolithiasis in 2021, with men accounting for 67% of cases (71.1 million). Between 1990 and 2019, the incidence of urolithiasis increased by 48.57 percent, from 77.78 million cases in 1990 to 115.55 million cases in 2019 15. There were 106 million incident cases of urolithias in 2021. The incidence of kidney stones is two or three times higher in postmenopausal women than in premenopausal women, which suggests that hormonal status plays a role in kidney stone development 16. Post menopausal women may have a higher chronic kidney disease rate. The impact of sex hormones on stone illnesses has been studied. A lower risk of kidney stone disorders is linked to low testosterone. After controlling for other factors Researchers found comparable correlations between the recurrence of urolithiasis at 5 years and up to 80-90 years without preventative treatment (such as obesity, diabetes, dyslipidaemia, race/ethnicity, and age) 17. This increased rate of recurrence has significantly reduce the patients quality of life, as well as the high costs attributed to healthcare costs 18-19. Recent epidemiological studies have reported an increase in the incidence of kidney stone formation in children of pediatric age, which has been associated with dietary changes, obesity, low fluid intake, and enhanced diagnostic methods 20-22.
2.2 Clinical Significance
Clinical importance of disease related urolithiasis is that it is usually related to other systemic disorders like Diabetes Mellitus, Obesity, Hyperparathyroidism, and Chronic Kidney Disease that may interact with complicated molecular and metabolic pathways that can modify the formation of the stone 23. One of the worst kinds of discomfort is renal colic, which is typically caused by a stone obstructing the urinary tract 24. Haematuria is another common clinical sign that results from irritation and injury to the mucosa of the urinary system. The manifestation of recurring urinary tract infections and hydronephrosis in some cases may be predetermined by urinary obstruction 25. If left untreated, obstruction can lead to a persistent infection that can progressively harm the kidney and increase the patient's chance of developing chronic renal disease. In order to avoid problems and maintain renal activity, urolithiasis must be appropriately diagnosed and treated promptly 26. Kidney stones are associated with systemic conditions such as diabetes, high blood pressure, and dyslipidaemia, which are risk factors for cardiovascular disease 27. One risk factor for renal illness that might result in myocardial infarction is kidney stones. In the general population, decreased GFR and albuminuria are linked to coronary heart disease 28.
The urolithiasis with diseases can be classified based on the corresponding systemic diseases or metabolic disorders causing the development of stones. These diseases alter the urine makeup, enable the formation of crystals, or disorient the healthy work of the kidneys.
3.1. One-Breasted-Women-Urolithiasis
The presence of metabolic problems caused by changes in the components of the urine is one of the main factors that increases the risk of developing stones. The development of stones is caused by the correlation between increased levels of calcium, uric acid, and oxalate in the urine and conditions such diabetes mellitus, obesity, and metabolic syndrome 29.
3.2. Urolithiasis is an endocrinologic disease
There are also a few endocrine diseases that disrupt mineral metabolism and cause stones to form. The Hyperparathyroidism is also an example that increases the calcium level in the serum and urine and leads to the formation of calcium containing stones 30.
3.3. Renal Disease-induced urolithiasis
The kidney conditions may alter the manner in which kidneys process renal electrolytes and minerals rendering an individual more susceptible to stones. The patient may have Urolithiasis if the patient has kidney structural defects or Chronic Kidney Disease 31.
3.4. Infection-Related Urolithiasis
Patients with repeated urinary tract infections may develop struvite stones as a result of urease-producing bacteria. These stones are usually related to Urinary Tract Infection and can develop within a short period of time in case they are not treated 32.
3.5. Urolithiasis that is associated with Gastrointestinal Disease
In these gastrointestinal conditions, fat is malabsorbed or intestinal inflammation occurs and can augment intestinal oxalate absorption. This disorder is called enteric hyperoxaluria and it leads to excessive levels of oxalate in the urine and it predisposes one to calcium oxalate kidney stones 33. Oxalate becomes available for absorption when unabsorbed fatty acids bond to calcium in the colon of a disease like Crohn's disease or inflammatory bowel disease. The ingested oxalate is then excreted in the urine, which promotes the formation of calcium oxalate stones 34.
3.6. Urolithiasis of Genetic or Hereditary Diseases
Recurrent kidney stones are known to be caused by metabolic hereditary disorders. Alterations in the genetic defects may result in changes to the metabolism or renal clearance of certain substances like cystine or oxalate which causes excessive excretion of urine and formation of stones 35. An example of this is Cystinuria, an inherited disease of defective reabsorption of cystine and other dibasic amino acids by the renal tubules; the patients have elevated urinary concentrations of cystine and frequent cystine stones 36.
3.7. Drug-Induced Urolithiasis
Some drugs may cause precipitation in Urians and result in the formation of stones. Indinavir, triamterene and sulfonamides are some drugs that can be crystallized in the urinary tract or can change the urinary chemistry, causing the kidney stones formation due to drugs 37.
Urinary tract structural abnormalities can lead to the development of stones and urinary stasis. Medullary sponge kidney and ureteropelvic junction obstruction may increase the incidence of urolithiasis 38.
4. Molecular and Pathophysiological Mechanisms
Pathogenesis of the disease-related urolithiasis is a dynamic and multifactorial process that takes place due to complex physicochemical and biological interactions of the urinary system. It is no longer regarded only as a consequence of urinary oversaturation, but a consequence of complex mechanisms in molecules, cellular and environmental actions, which control crystal formation, growth and retention in the renal system 39.
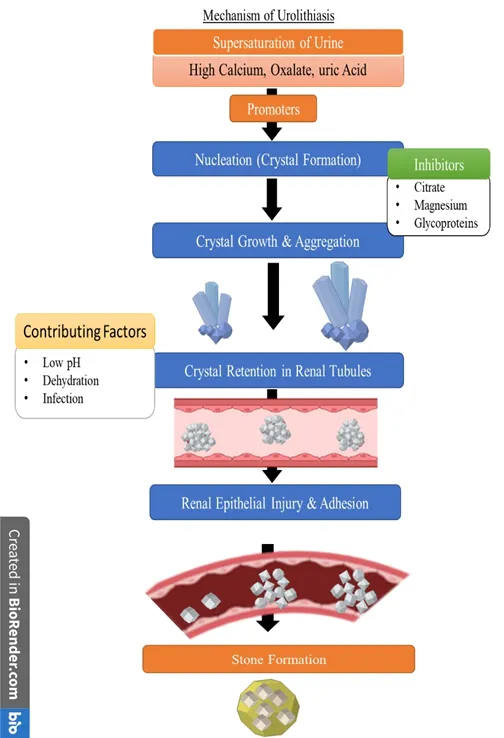
Fig. 1: Mechanism of renal stone formation
4.1. Nucleation and Urinary Supersaturation
The first step in the formation of stones is urinary supersaturation with lithogenic chemicals, such as calcium, oxalate, phosphate, and uric acid. As the solutes become high, compared to their solubility, the solutes are collected to form crystals in a phenomenon referred to as nucleation 40. Nucleation may be either homogeneous whereby crystals are generated spontaneously or heterogeneous where surfaces that are already present like cellular debris or urinary proteins serve as a nidus41. Low urine volumes, high levels of suture excretion, and altered urinary PH are some factors that cause supersaturation 42.
4.2. Crystal Growth, Aggregation and Retention
After nucleation, the crystals enlarge and unite to produce larger particles that may block. While aggregation is the clumping of individual crystals into big aggregates, crystal development occurs by binding ions of the supersaturated urine to the crystal surfaces already present 43. These crystals play a crucial role in the development of stones because they are retained in renal tubules. Small crystals are typically removed by the urine flow, but they can build up in situations when renal tubular dynamics or adherence to epithelial cells are compromised 44.
4.3. Role of Epithelial Injury of the Renal Tube
The destruction of the epithelial of the renal tubules is crucial in promoting the retention of the crystals and the formation of stones. Exposure to high amounts of oxalate or calcium oxalate crystals causes oxidative stress and cell injury in tubular epithelial cells 45. The injury causes expression of adhesion molecules and revealing of underlying matrix components which facilitates crystal attachment 46. Broken epithelial cells also discharge cellular debris, which will serve as a point of nucleation, further speeding up the formation of the stone 47.
4.4. Oxidative Stress Pathway and Inflammatory Pathways
One of the key processes in the pathophysiology of urolithiasis is oxidative stress. The reactive oxygen species (ROS) formation in reaction to crystal deposition causes lipid peroxidation, mitochondrial dysfunctions, and renal cell apoptosis 48. Numerous signalling pathways, including nuclear factor-kappa B (NF-k B), which stimulates the production of pro-inflammatory cytokines like interleukins and tumour necrosis factor-alpha, are also linked to ROS 49. This inflammatory reaction aggravates tissue damage and increases the retention of crystals, which are in a vicious cycle of destruction and stone development 50.
4.5. Involvement of Urinary Macromolecules
The urinary macromolecules like proteins and glycoproteins are also known to have a dual role in the development of the stones; to inhibit or to promote crystallization. By adhering to crystal surfaces and reducing the degree of supersaturation, citrate, magnesium, nephrocalcin, and Tamm-Horsfall protein inhibitors stop crystal growth and aggregation 51. On the other hand, some proteins such as osteopontin and uromodulin might cause crystals to be attached in pathological conditions 52. The disproportion of promoters and inhibitors plays a crucial role in the pathogenesis of stone formation.
4.6. Plaques and Interstitial Mechanisms of Randall
Randall has calcium phosphate deposits in the renal papillary interstitium, which are believed to be the precursors of calcium oxalate stones. These plaques begin in the loop of Henele's basement membrane and gradually spread to the papillary surface, where they serve as attachment sites for the crystal deposition 53. These plaques result in the development of calcium oxalate crystals when they come into contact with urine, which leads to the development of stones 54.
4.7. Influence of Urinary pH
The composition and development of stones are determined by the pH of the urine. In contrast to alkaline urine, which is more likely to produce calcium phosphate and struvite stones, acidic pee is more likely to produce uric acid and cystine stones 55. Urinary pH is significantly impacted by systemic conditions such as metabolic acidosis, renal tubular acidosis, and urease-producing bacteria infection, which also induce disease-specific urolithiasis 56.
4.8. Genetic and Epigenetic factors
In urolithiasis, genetic predisposition has great importance in disease-related urolithiasis. Genetic defects in oxalate metabolism, calcium transport, and cystine reabsorption have the capability to predispose an individual to the development of stones 57. For example, abnormalities in the renal tubular transport of cystine lead to its accumulation and crystallisation, which results in cystinuria. Moreover, DNA methylation and miRNA regulation are epigenetic alterations that have been reported to control the gene expression concerning the formation of crystals and kidney damage 58.
4.9. Contributions of Microbes and Biofilm Formation
Infection-related urolithiasis is linked to urease-producing bacteria, such as Proteus mirabilis, which converts urea to ammonia, elevating the pH of the urine and causes struvite stones to develop59. These bacteria are also able to create biofilms on the crystal surfaces, which increases the aggregation of crystals as well as shielding the microbes against host immune system flora as well as antibiotics 60. The development of biofilm is one of the determinants of recurrent and persistent infection related to stones.
4.10. Metabolic and Systemic Effects
The pathophysiology of urolithiasis is determined by major systemic disorders such as metabolic syndrome, diabetes mellitus, and obesity. All of these conditions alter the urine's composition, causing it to produce less citrate and more calcium oxalate and uric acid 61. Among the effects of insulin resistance, which is frequently observed in metabolic syndrome, is the decreased production of ammonium in the kidney, resulting in acidic urine and susceptibility to uric acid rocks 62.
Table 1: Molecular and Physicochemical Mechanisms of Lithogenesis
|
Stage |
Process Description |
Key Modulators/Factors |
|
Supersaturation |
Concentration of ions exceeds their solubility product. |
Calcium, Oxalate, Uric Acid, Phosphate. |
|
Nucleation |
Formation of the first solid crystal phase from a liquid. |
Homogeneous vs. Heterogeneous nucleation. |
|
Crystal Growth |
Increase in size of existing nuclei. |
Low levels of inhibitors (Citrate, Magnesium). |
|
Aggregation |
Clusters of crystals forming larger masses. |
Urinary macromolecules (Osteopontin). |
|
Retention |
Adhesion of crystals to the renal tubule wall. |
Oxidative Stress, ROS, Epithelial injury. |
|
Randall’s Plaques |
Sub-epithelial calcium phosphate deposiyion. |
Interstitial crystallization in papilla. |
This table outlines the progression from ionic saturation to stone retention 40,42,44,45,48.
Disease The disease is strongly influenced by underlying systemic and metabolic disease that modulates the composition of urine, urine physiology, and molecular signaling pathways. Various disease entities are characterized by distinctive pathways to cause stones by exhibiting diverse metabolic imbalance, epithelial damage and alteration of urinary micro environment 63.
5.1. Diabetes Mellitus and Insulin Resistance
Another a high risk factor for urolithiasis, and particularly ureic acid stones, is diabetes mellitus. The insulin resistance issue inhibits the renal ammoniagenesis that leads to low urinary PH that facilitates the uric acid crystallization 64. Also, hyperglycemia increases the adhesion of crystals and promotes oxidative stress and glycation end products, which damage renal tubules 65. Calcium and oxalate urine fixation is also greater in diabetic patients consequently exposing them to calcium based stones 66.
5.2. Obesity and Metabolic Syndrome
Metabolic syndrome and obesity are the risk factors in urolithiasis with association of several metabolic disorders. There is enhanced urinary calcium, uric acid, oxalate and sodium excretion with increased body mass index and all these enhance supersaturation 67. In addition, obesity causes systemic inflammation and oxidative stress, which change the renal tubular activity and enhance crystal retention 68. Low citrate concentration in the urine is a common symptom of metabolic syndrome, eliminates one of the possible inhibitors of the formation of stones, thus worsening the lithogenesis 69.
5.3. Hyperparathyroidism
Hypersecretion of parathyroid hormone (PTH), which causes hypercalcemia and hypercalciuria, is a disorder known as primary hyperparathyroidism. The calcium will increase the concentration of calcium in the urine and increase the risk of developing calcium phosphate and oxalate stones 70. Additionally, PTH promotes renal tubular calcium reabsorption and bone resorption, which both contribute to urine calcium excess 71. In case the disorder remains untreated due to the chronic nature of the disorder, then it could be described as recurrent stones.
5.4. Renal Tubular Acidosis (RTA)
Distal renal tubular acidosis is a condition which is characterized by the inadequate secretion of hydrogen ion resulting in alkaloid urine and acidic body. The high pH promotes the formation of calcium phosphate stones whereas acidosis in the system reduces the excretion of citrate and thus, the inhibitory effect of citrate on the crystal formation is eliminated 72. Moreover, permanent acidosis leads to bone demineralization which involves in the increasing concentration of calcium in the blood and urine 73.
5.5. Gout and Hyperuricemia
High serum uric acid levels associated with gout promote the formation of stones and increase uric acid excretion in the urine. The first initiation of uric acid stones takes place in the acidic urine, whereby uric acid is unable to dissolve effectively 74. Uric acid crystals can also act as a nidus in a calcium oxalate deposition, thus result in the mixed stones 75. Inflammatory conditions in gout may also result in renal epithelial damage and crystal retention.
5.6. Gastrointestinal Disorders and Enteric Hyperoxaluria
Enteric hyperoxaluria is caused by gastrointestinal disorders, such as Crohn's disease, inflammatory bowel disease, and complications of post-bariatric surgery. Inadequate absorption of the fats results in elevated amounts of free fatty acids in the intestine, which binds to calcium and leave little calcium available to bind oxalate. As a result, extraxyalate is absorbed, which causes hyperoxaluria 76. The augmented urinary oxalate promotes calcium oxalate crystals and deposition in tubules within the kidney 77.
5.7. Genetic Disorders: Cystinuria and Primary Hyperoxaluria
Hereditary conditions are very essential in certain types of urolithiasis. Cystinuria is a condition where the renal tubular reabsorption of cystine is impeded, leading to its accumulation and deposition in the urine due to its low solubility 78. Primary hyperoxaluria is a rare hereditary condition that is not communicable and is linked to an excess of endogenous oxalate formation due to a lack of enzymes involved in glyoxylate metabolism 79. These lead to serious hyperoxaluria, frequent stone formation, to chronic kidney damage.
5.8. Infection-Induced Urolithiasis
Struvite stones are the type of kidney stones which are formed as a result of urinary tract infections due to bacteria which produce urease like the Proteus, Klebsiella, and Pseudomonas. Urease decomposes urea to carbon dioxide and ammonia, raising urinary pH, and causing magnesium ammonium phosphate to precipitate 80. Crystallization and anti-bacterial resistance in the pathogens are also increased by bacterial biofilms, which cause chronic infections and stone recurrence 81.
5.9. Drug-Induced Urolithiasis
Some drugs may cause stones either directly or indirectly. Indinavir, triamterene, and sulfonamides are examples of drugs that crystallize in the urine because of low solubility resulting into drug induced stones 82. The other drugs, like corticosteroids and loop diuretics, also changes the calcium metabolism and increases in the urinary calcium excretion, which facilitates the formation of calcium-based stones 83. The risk itself is commonly dose-related and depends on whether one is hydrated or not.
5.10. Chronic Kidney Disease (CKD)
Urolithiasis results in and causes chronic kidney disease. The decreased renal functioning causes the poor excretion of the stone-forming solutes culminating into their accumulation and heightened chances of crystallization 84. Also, frequent blockage and infection through stones may hasten the CKD. Alteration in mineral metabolism further increases the incidence of calcium and phosphate stones in CKD patients 85.
Table 2: Systemic Diseases and Their Impact on Urinary Composition
This table summarizes the Clinical Manifestations and Systemic Illnesss 65,71,72,77,85,82.
|
Associated Disease |
Primary Urinary Alteration |
Common Stone Type |
|
Diabetes Mellitus |
Low urinary pH, hypercalciuria. |
Uric Acid, Calcium Oxalate. |
|
Obesity / MetS |
Increased acid excretion, hyperoxaluria. |
Calcium Oxalate. |
|
Hyperparathyroidism |
Significant hypercalcemia & hypercalciuria. |
Calcium Phosphate, Calcium Oxalate. |
|
GI Disorders |
Fat malabsorption (Enteric hyperoxaluria). |
Calcium Oxalate. |
|
UTI (Proteus/Klebsiella) |
High urinary pH (Ammonia production). |
Struvite (Infection stones). |
|
Renal Tubular Acidosis |
Low citrate, high pH. |
Calcium Phosphate. |
The disease-associated urolithiasis clinical manifestations are determined by the size and the location of the stones, as well as their composition with or without complications like obstruction or infection. Although some have no symptoms, most of them have acute or recurrent symptoms that greatly affect the quality of life 86.
6.1. Renal Colic
Renal colic is the characteristic manifestation of urolithiasis and usually it is because of acute obstruction of the ureters through the movement of stones. The pain is acute, sharp and colicky, and it begins in the flank and tends to spread to the groin or lower abdomen 87. It can be characterized as being among the most severe types of pains, and is linked with ureteral peristalsis and heightened intraluminal pressure 88. Due to pain severity, the patients are often restless and cannot stay in one position 89.
6.2. Hematuria
Haematuria is a common clinical manifestation that can be either gross or microscopic. It is a condition caused by irritation of the mucosa and injury to the urinary system caused by stones passing through or existing in the urinary tract 90. Even though hematuria is very common, it might be missing in certain instances especially when there is complete obstructions or stones that are non-motile 91.
6.3. Symptoms of Lower Urinary Tract
Lower urinary tract symptoms, such as urgency and frequency of urination, dysuria, and tenesmus are typically associated with stones in the distal ureter or surrounding the bladder 92. The symptoms can be similar to urinary tract infections and proper diagnosis is a must.
6.4. Gastrointestinal Symptoms
Renal colic is commonly accompanied by nausea and vomiting because of the overlapping of the sympathetic supply of the gastrointestinal and urinary systems 93. The symptoms may result in dehydration, which in turn may also increase urinary supersaturation and stones.
6.5. Urinary Tract Infection (UTI)
Urolithiasis is associated with the structure of urinary tract infections, particularly when there is obstruction. Fever, chills, dysuria, and cloudy or foul-smelling urine are the clinical signs 94. Infections of the urease producing organisms may also cause alkaline urine and development of struvite stones which in most cases cause recurring infections 95.
6.6. Obstructive Uropathy and Hydronephrosis
The presence of obstruction using stones may also result in hydronephrosis which is the dilation of renal pelvis and calyces as a result of obstructed urine flow 96. With prolonged obstruction, there could be decrease in the glomerular filtration rate, renal damage and kidney function loss 97. Patients can complain of flank pain, reduced urine production, or even acute kidney failure.
6.7. Asymptomatic (Silent) Stones
A good proportion of the stones are asymptomatic, and they are accidentally detected in imaging techniques like ultrasonography or computed tomography used to treat other conditions 98. These stones can expand with time though without any symptoms and they can later lead to complications.
6.8. Recurrent Stone Disease
A characteristic clinical presentation is recurrent urolithiasis particularly in individuals who have metabolic imbalances or general illnesses. Recurrence is high and most of the patients undergo recurring episodes with time 99. Similar symptoms are usually recurring such as renal colic and hematuria.
6.9. Disease-Specific and Systemic Manifestations
Urolithiasis caused by disease may have other systemic effects based on the underlying disease. As an example, the patients with metabolic syndrome can have such characteristics like obesity and insulin resistance, whereas patients with gout can have such features as a joint inflammation and uric acid stones 100. In the same way, hyperparathyroidism can be characterized by the signs of hypercalcemia, such as fatigue, bone pain, and gastrointestinal disturbances 101.
6.10. Complications
Urolithiasis may cause severe complications when left untreated since it may result in frequent urinary tract infections, nephropathy as an obstruction, and chronic kidney disease 102.Among the most dangerous complications is urosepsis which is a life-threatening disorder that is caused by infected blocked stones and needs acute care 103. The old stones can also result in structural damage of the urinary tract such as strictures and scarring.
Diagnostic evaluation of disease-related urolithiasis will aim at determining that disease-related urolithiasis is present, their size, location, and composition and underlying metabolic or systemic abnormalities. The patient requires a complicated treatment plan that includes clinical test, laboratory tests, and imaging to diagnose them and give them proper management 104.
7.1. Clinical Assessment
The physical examination and medical history is the beginning of the diagnostic process. Patients usually show symptoms like haematuria, renal colic, and discomfort when urinating. Routine stones, nutrition, consumption of liquids and other concomitant systemic illnesses such as diabetes or gout are useful clues to the etiology of urolithiasis 105. Physical examination may reveal the existence of flank tenderness, the findings may be unspecific.
7.2. Laboratory Investigations
The laboratory analysis is quite essential in identifying the metabolic defect and other complications. Urine analysis is also performed periodically to find out the presence of hematuria, urinary pH, crystalluria and the development of an infection such as bacteriuria or pyuria 106. In cases of suspected urinary stones, urine cultures are recommended in order to identify organisms causing the issue.
In serum, biochemical tests that can be performed to ascertain the functionality of the kidney and any systemic pathology include calcium, phosphate, uric acid, creatinine and electrolytes 107. In recurring or high-risk patients, a 24-hour analysis of the urine is critical in the determination of excretion of calcium, citrate, oxalate, sodium, uric acid and volume as an indicator of the metabolic etiology of stone formation 108.
7.3. Imaging Techniques
The diagnosis of urolithiasis is based on imaging. This is due to the fact that non-contrast computed tomography (NCCT) is the gold standard due to its exceptional sensitivity and specificity in identifying stones of all sizes and types 109. Additionally, it offers precise information on the locations of obstacles, stones, and structural anomalies.
One of the popular non invasive modalities with radiation free and ultrasonographic modality is ultrasonography that is useful in pregnant and the pediatric group of patients. Although it is less sensitive compared to CT to detect ureteral stones of smaller sizes, it is applicable in detecting renal stones and also hydronephrosis. The detection of radiopaque stones may be performed using plain abdominal radiography (KUB) with a low sensitivity 110.
7.4. Stone Analysis
The chemical composition of stones that have been passed or removed with the help of surgery is to be determined through analysis. IR spectroscopy and X-ray diffraction are some of these techniques which will give effective identification of stone constituents which is essential in informing preventive and pharmacological measures 111.
7.5. Assessment of Ultimate Causes
In urolithiasis associated with a disease, it is essential to find out underlying systemic conditions. Patients will be evaluated for metabolic syndrome, endocrine disorders, renal tubular acidosis, and gastrointestinal disorders that may contribute to the development of stones 112. Such detailed examination aids in customization of individualized treatment and avoidance of re-occurrence.
Treatment of urolithiasis associated with disease is conducted pharmacologically to treat acute symptoms, promote expulsion of stones, prevent recurrence and correct underlying metabolic defects. The decision of the therapy is made based on the kind of the stone, size, and composition, and other conditions and risk factors related to the system.
8.1. Management of Acute Renal Colic
The first urolithiasis treatment is focused on symptoms and pain management. Others of the first-line agents were the NSAIDS, such as ibuprofen and diclofenac, which can reduces the ureteral smooth muscle tone and inflammation caused by prostaglandin. The use of opioid analgesics is resorted to in the case of NSAIDs that should not be taken or do not work, but they have more side effects, such as sedation and nausea 113. Antiemetics are usually administered to manage the nausea and vomiting associated with renal colic include metoclopramide and ondansetron.
8.2. Medical Expulsive Therapy (MET)
Expulsive medical therapy which is routine used to facilitate dislocation of urinary stones, particularly stones having a diameter less than 10 mm. The reason is that tamsulosin and other alpha-adrenergic blockers relax the ureteral smooth muscle, reduce spasms and increase the speed of stone passage. Also, it is possible to treat it with calcium channel blocker like nifedipine however this is not widely used as compared to the alpha-blockers due to less effectiveness of the former when compared to the latter. MET has demonstrated speed in time to stone passage, reduced pain attacks and reduced the occurrence of surgery 114.
8.3. Therapeutic Intervention According to the Type of Stones
a. Calcium Stones
Calcium oxalate and calcium phosphate are the most common and frequent renal stones. Thiazide diuretics are also taken, including hydrochlorothiazide, inorder to decrease the concentration of calcium excreted in the urine by enhancing renal tubular calcium reabsorption 115. Potassium citrate is also commonly prescribed to raise the citrate levels in the urine, which prevents agglomeration of crystals, besides aiding in alkalinization of urine 116. Those therapies are especially effective in patients having hypocitraturia and hypercalciuria.
b. Uric Acid Stones
The primary treatment for uric acid stones involves alkalinising the urine with potassium citrate or sodium bicarbonate, which makes uric acid more soluble. Xanthine oxidase inhibitor used to treat hyperuricemia or hyperuricosuria is allopurinol, which reduces the production of uric acid 117. For those who cannot tolerate allopurinol, febuxostat may be considered an alternate 118.
c. Struvite Stones
The struvite stones are associated with urinary tract infections because of the urease-producing bacteria. Culture sensitive antibiotic aromatherapy is critical to eliminate infection and recurrence. Ammonia inhibitors like acetohydroxamic acid can also be utilized but their application is not very common due to side effects in certain situations 119.
d. Cystine Stones
Stones containing cystine are treated by increasing the volume of urine and alkalinizing it using potassium citrate. Penicillamine and tiopronin are thiol-binding agents that are employed to make more soluble cystine complexes and hence minimize the formation of stones 120. The agents are normally used in severe cases as they may have side effects.
8.4. Role of Antioxidants and New Therapies
Oxidative stress is primarily associated with the development of urolithiasis and antioxidant therapy has been considered as an adjunct therapy to urolithiasis. The experimental results have demonstrated that vitamin E, vitamin C, and phytochemicals are capable of reducing the renal epithelial injury and crystal adherence 121. Also, herbal preparations and plant extracts like the Phyllanthus niruri and Tribulus terrestris have been shown to be anti urolithiatic by interfering with crystal aggregation and by inducing diuresis 122.
The inhibitors of crystal adhesion, anti-inflammatory agents, and the modulators of urinary macromolecules are also the novel therapeutic targets of recent research 123.
8.5. Treatment of Systemic Underlying Conditions
It is important to treat the underlying systemic diseases that cause the formation of stones in the management of the disease. The example can be the insulin sensitizers used in the metabolic syndrome or parathyroidectomy in primary hyperparathyroidism. Alkali therapy is used to treat acidosis and avoid the formation of calcium phosphate stones in the renal tubular acidosis patients 124.
8.6. Preventive Pharmacotherapy
The prevention of recurrence is one of the main aspects of urolithiasis management. Thiazides, citrate supplements, and allopurinol are pharmacological interventions suggested, but only in case of individual metabolism assessment 125. Individual treatment based on 24-hour urine testing has proven to be very helpful in reducing the chances of recurrence.
9. Non-Pharmacological Management
The non-pharmacological management which concerns the lifestyle and dietary changes directed to reduce the urinary supersaturation and eliminate the metabolic imbalances are one of the fundamental factors in the prevention and recurrence control of the disease-related urolithiasis 126. These are just but some of the strategies that are important in light of the recurring and chronic nature of stone disease.
Adequate hydration is most of the preventive measures. The greater fluidity dilutes the lithogenic substances such as oxalate, calcium and uric acid hence minimizing crystal formation. Maintenance of two or more liters of urine per day is also quite effective in minimizing the recurrence rate 127. Dehydration should be avoided especially during a hot weather or in cases of intense activity.
Nutritional modification has a role to play in prevention of stone. The recommended calcium level in the diet is normal since it binds the oxalate in the intestines and reduces its absorption thus reducing the level of urinary oxalate 128. The consumption of high amount of sodium should be restricted as it increases the excretion of urinary calcium whilst excess consumption of animal protein increases acid load, hyperuricosuria and hypocitraturia all of which contributes to the development of stones 129. It is also prudent to have a limit on the amount of foods that contain oxalates such as nuts, spinach, and tea in calcium oxalate stone formers.
Additionally, maintaining a healthy weight and engaging in regular physical activity are lifestyle characteristics that are less likely to put an individual at risk. High urinary excretion of stone-forming substances and low urine pH that predisposes a person to urolithiasis is also associated with obesity 130.
10. Surgical Interventions in Urolithiasis
Surgery is recommended as the management of urolithiasis in patients who have large, symptomatic, obstructive, or renal stones in cases where the conservative or pharmacological therapy has failed. The selection of the intervention is conditioned by the size, location, composition, and individual aspects of the patient 131. The less invasive procedures have greatly supplanted the open surgery because they are less morbid and recover sooner.
ESWL a non-invasive technology which employs shock waves to break up stones, thus it is applicable in small to moderate-sized renal calculi; but this process might need several sessions since total clearance cannot be achieved 132. Image endoscopic visualization and laser fragmentation of the stones are performed in ureteroscopy (URS) and Retrograde Intrarenal Surgery (RIRS), which have great success rates, especially with ureteral and small renal stones 133.
In large stones (>20 mm), or other stones with complicated structure like staghorn stones, Percutaneous Nephrolithotomy (PCNL) is considered as the best option, with the possibility of direct access to stones through a percutaneous passage 134. Even in the selected cases laparoscopic or open surgery may be necessary especially in cases where anatomical abnormalities or failed minimally invasive surgeries exist 135.
11. Urolithiasis Prevention Strategies
Urolithiasis prevention mostly aims at the reduction of the recurrence rate, which is achieved through lifestyle alteration, dietary therapy, and the restoration of the metabolic defects. The basis of prevention is adequate hydration, which keeps the level of urine at least 2-2.5 L/day to dilute calcium, oxalate and uric acid, which make up stones, and inhibit supersaturation 136.
Food-based measures are very instrumental in reducing risk. It is advisable that one has a balanced intake of calcium because low calcium diets can have an opposite effect where the oxalate absorption and stone-forming increases 137. Dietary sodium and animal protein restriction are also recommended as large intake of sodium contributes to urinary calcium loss whereas excessive consumption of protein facilitates hyperuricosuria and acidify urine 138. Also, it is important to limit the consumption of foods rich in oxalates such as spinach, nuts and chocolate which contribute to the development of calcium oxalate stones 139.
Preventive factors are also weight management and physical activity because the risk of stones is closely linked with obesity and metabolic syndrome owing to the change in the urinary composition. In addition, underlying illnesses like hyperparathyroidism, urinary tract infection and renal tubular acidosis must be managed to avoid the recurrence 140.
Recurrent cases may also need pharmacological prophylaxis, such as thiazide diuretics in hypercalciuria, potassium citrate in hypocitraturia, and allopurinol in hyperuricemia; they depend on a metabolic assessment 136.
In general, a complex of personalized dietary, lifestyle, and medical interventions is necessary in the effective prevention of urolithiasis in the long run and lessening the recurrence rates.
12. Emerging Therapeutic Approaches
New treatment modalities in Urolithiasis are fast gaining momentum in terms of addressing the molecular pathways that underly stones, with the view of enhancing the efficacy and prevention of recurrence. The progress in the body of knowledge on crystal nucleation, growth and aggregation has seen the creation of new types of inhibitors capable of controlling these processes. Indicatively, natural inhibitor mimicking molecules like citrate and glycosaminoglycans are also in development to inhibit the aggregation and adhesion of calcium oxalate crystals on the renal epithelial cells 141.
The use of nanotechnology in drug delivery system has also been on the forefront in recent years. Nanoparticles would have the potential to improve the bioavailability and delivery of antiurolithiatic agents in the target areas and thus improve the treatment and reduce the systemic side effects. The systems find their application especially in the delivery of phytoconstituents and poorly soluble drugs themselves to the renal tissues 142.
Phytotherapy remains a significant field of study with some of the compounds extracted out of plants showing anti urolithiatic properties by way of antioxidant, anti-inflammatory and diuretic activity. Flavonoids, saponins, and polyphenols have been found to have potential in crystal formation inhibition and promotion of stone dissolution in experimental models 143.
Urinary microbiota modulation is another promising solution. Recent research indicates that some bacteria, including Oxalobacter formigenes, are involved in the degradation of oxalates in the gut, and thus, they inhibit urinary oxalate excretion. Therapy through probiotics to reestablish such healthy populations of microbes is under investigation as a prevention and treatment therapy 144.
There are also ongoing research efforts on gene and protein-targeted therapies on controlling protein expression that is related to crystal adhesion, which includes osteopontin and Tamm-Horsfall protein. The mode of action of these approaches is to disrupt important pathogenesis processes of stones at the molecular level 145.
13. FUTURE PERSPECTIVES
The future outlook in urolithiasis studies focuses on further development of precision medicine, early detection and mechanism-based treatment. As more is known about the molecular and genetic theory of stone formation, customized treatment plans on the basis of individual metabolic profiles, genetic predisposition and stone composition may be utilized to enhance clinical outcome. Combination of genomics, proteomics, and metabolomics might provide the opportunity to identify new biomarkers in the detection of early and risk stratification.It is also expected that artificial intelligence (AI) and machine learning will have a major role in predicting recurrence, treating more effectively, and diagnosing more through imaging. These technologies can help clinicians to make a data-driven decision, which can improve the management of patients and decrease the healthcare burden.Moreover, the study of the gut–kidney and urinary microbiome can potentially provide new avenues on preventive therapy, such as probiotic and microbiota-specific therapies. Another potential direction is the development of safer and more effective pharmacological agents, which selectively inhibit crystal nucleation, growth, and adhesion.
CONCLUSION
The process of the pathogenesis of disease-related urolithiasis has progressed from being a physicochemical process to a cell-mediated pathological process. Therefore, to effectively treat this illness, a multi-faceted approach that involves not only the treatment of the presenting symptoms of the illness but also the underlying systemic or genetic causes of lithogenesis is essential.Integrated Management: To effectively reduce the recurrence rates of this illness, an integrated approach that involves the use of pharmacological prophylaxis, coupled with significant changes to an individual’s lifestyle, such as increasing fluid intake, is essential.Systemic Focus: To effectively treat this illness, it is essential to address the underlying causes of lithogenesis, such as insulin resistance, hyperparathyroidism, and enteric hyperoxaluria.Future Directions: To effectively care for patients suffering from this illness, the future of treatment will be to use precision medicine techniques that will be informed by an individual’s genomic profile.Innovative Research: To effectively care for patients suffering from this illness, innovative research that involves the use of probiotics to treat this illness, as well as the use of artificial intelligence to reduce recurrence rates, will be essential.
REFERENCES


Ranjithkumar K, Kusu Susan Cyriac, Disease-Related Urolithiasis: Molecular Mechanisms, Clinical Manifestations and Pharmacological Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2684-2706, https://doi.org/10.5281/zenodo.20624359
 10.5281/zenodo.20624359
10.5281/zenodo.20624359