
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
*Department of Pharmacy, Faculty of Medical Paramedical and Allied Health Science, Jagannath University, Jaipur, Rajasthan, 303901, India
2 Faculty of Medical Paramedical and Allied Health Science, Jagannath University, Jaipur, Rajasthan, 303901, India
One of the most serious non-communicable disease crises of the twenty-first century is type 2 diabetes mellitus (T2DM). The International Diabetes Federation (IDF) Diabetes Atlas estimates that 589 million persons worldwide—roughly one in nine adults—currently have diabetes, and by 2050, this number is expected to rise to 853 million. Conventional treatments, such as insulin, metformin, sulfonylureas, and thiazolidinediones, are still essential, but it is becoming more widely acknowledged that they are inadequate to address the complex, multi-defect pathophysiology of type 2 diabetes, which includes ?-cell exhaustion, cardiovascular risk, and the progression of chronic kidney disease. Four main developing therapy categories-GLP-1 receptor agonists (GLP-1 RAs), SGLT2 inhibitors, dual GIP/GLP-1 receptor agonists (Tirzepatide), and oral insulin delivery systems-are rigorously assessed in this study based on their molecular underpinnings, clinical trial data, and relative efficacy. Additionally, a 2025 Lancet Diabetes & Endocrinology trial found that sotagliflozin, a new dual SGLT1/SGLT2 inhibitor, reduced composite cardiovascular risk by about 30%. A critical evaluation shows that dual agonists are quickly becoming the most effective medications for combination glycemic and weight management, even if GLP-1 RAs and SGLT2 inhibitors have already established a solid position in ADA and ESC 2025 guidelines. Despite ongoing research after Phase 3 disappointments, oral insulin treatment still has scientific potential thanks to delivery techniques based on nanoparticles. In addition to advocating for a paradigm change toward tailored, cardiometabolic, and organ-protective diabetes management, this review offers an organized gap analysis.
Type 2 diabetes mellitus (T2DM) is one of the most significant non-communicable disease crises of the twenty-first century. According to the International Diabetes Federation's (IDF) Diabetes Atlas, 589 million people worldwide—roughly one in nine adults—have diabetes at the moment, and by 2050, that figure is predicted to increase to 853 million.[1,2] The worldwide health problem is made worse by the startling percentage of cases that go undetected, especially in low- and middle-income nations.
Beyond just hyperglycemia, type 2 diabetes is linked to a number of potentially fatal side effects, such as neuropathy, retinopathy, chronic kidney disease (CKD), and cardiovascular disease. Over 95% of instances of diabetes are type 2 diabetes (T2DM), which is mostly caused by increased obesity, sedentary lifestyles, urbanization, and genetic vulnerability. The illness is one of the main causes of death worldwide, accounting for about 3.4 million fatalities every year.[1]
The pathophysiological underpinnings of type 2 diabetes go well beyond insulin insufficiency. T2DM was essentially reframed as a multisystem metabolic condition by DeFronzo's conception of the "Ominous Octet"—eight concurrent organ-level abnormalities.[3] This has spurred the creation of treatments that target obesity, cardiovascular risk, renal function, and patient adherence in addition to glycemic management.
Despite being clinically successful and reasonably priced, conventional medications like insulin, metformin, and sulfonylureas have several drawbacks, including weight gain, hypoglycemia risk, progressive loss of efficacy due to β-cell failure, and little organ-protective advantages.[4,5] Over the past ten years, these flaws have prompted the creation of new therapeutic classes, radically altering clinical practice recommendations.
GLP-1 receptor agonists, SGLT2 inhibitors, dual incretin receptor agonists (Tirzepatide), and oral insulin systems are among the emerging treatments for type 2 diabetes that are thoroughly and critically examined in this review. It includes updated clinical data from 2024–2025, a structured comparative analysis, and an identification of unmet research gaps. The objective is to offer a distinctively analytical and clinically applicable viewpoint to the quickly changing field of T2DM treatments.
1.Pathophysiology Framework
According to DeFronzo (2009), the current understanding of T2DM pathophysiology revolves around a complicated interplay of eight main abnormalities.[3] The 'Ominous Octet' model emphasizes how the pancreas, liver, muscle, adipose tissue, kidney, gut, and brain are all involved in maintaining hyperglycemia. To understand why new multi-target medicines, provide better results than previous single-pathway drugs, it is crucial to comprehend this framework
1.Core Defects
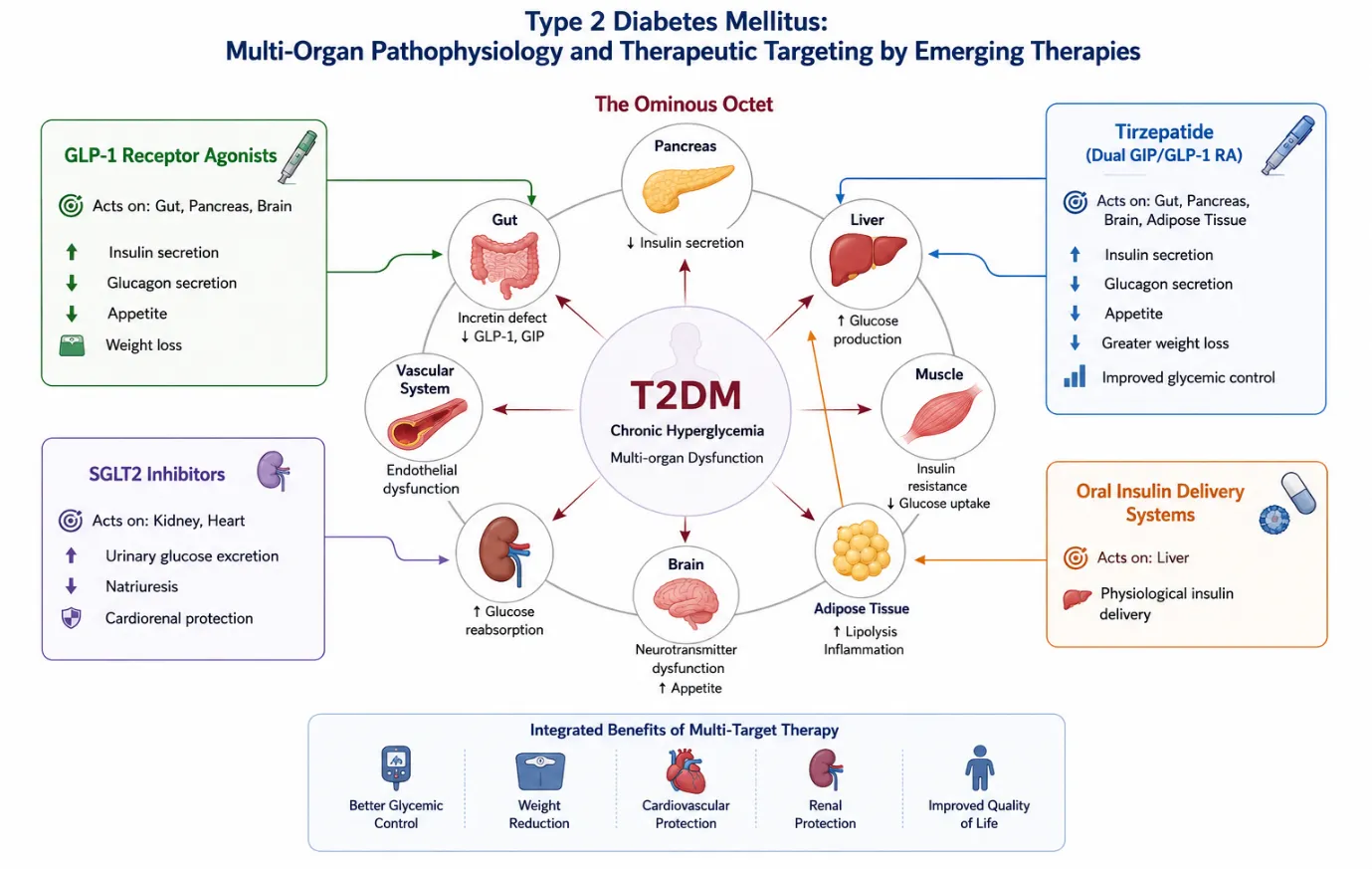
Figure 2.1: Integrated multi-organ pathophysiology of type 2 diabetes mellitus and therapeutic targeting by emerging antidiabetic therapies.
This multi-organ framework makes it abundantly evident why prolonged metabolic control is inherently difficult to achieve with traditional single-target medicines. New treatments are in a unique position to address several of this pathophysiological network's nodes at once.[3]
2.Pathophysiology Framework
According to DeFronzo (2009), the current understanding of T2DM pathophysiology revolves around a complicated interplay of eight main abnormalities.[3] The 'Ominous Octet' model emphasizes how the pancreas, liver, muscle, adipose tissue, kidney, gut, and brain are all involved in maintaining hyperglycemia. To understand why new multi-target medicines, provide better results than previous single-pathway drugs, it is crucial to comprehend this framework.
1.Core Defects


Arun Kumar Gulia, Rakesh Kumar Sharma, Emerging Therapies in Type 2 Diabetes Mellitus: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 392-403. https://doi.org/10.5281/zenodo.20493294
 10.5281/zenodo.20493294
10.5281/zenodo.20493294