
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
RJS College of Pharmacy, Kokamthan, Kopargaon.
Ethosomes are lipid-based vesicular carriers enhanced with ethanol that increase transdermal drug administration by increasing drug permeability through the skin. When used topically in traditional formulations, azithromycin, a broad-spectrum macrolide antibiotic, has poor skin penetration. Phospholipids, ethanol, and azithromycin were combined to create ethosomal vesicles in this study utilising the cold technique. These vesicles were then included into an appropriate gel base to create the ethosomal gel. The formulated ethosomal gel was evaluated for physicochemical parameters such as pH, viscosity, spreadability, and drug content. Vesicle size, entrapment efficiency were also determined to characterize the ethosomal suspension. In vitro drug release studies revealed a sustained release profile, and antimicrobial studies demonstrated enhanced antibacterial activity against Escherichia coli.
Bacterial infections continue to be a global health concern and frequently necessitate the long-term use of antibiotics. Variable bioavailability, decreased patient compliance, and systemic side effects might result from oral and parenteral delivery. Because they can localise drug activity, avoid first-pass metabolism, and maintain sustained therapeutic levels, transdermal and topical administration systems have become more important. Compared to traditional oral methods, transdermal and topical drug delivery systems have a number of benefits, such as avoiding first-pass metabolism, increasing drug bioavailability, maintaining drug release, and improving patient compliance. Specifically, vesicular carriers like liposomes, niosomes, and ethosomes have drawn interest due to their capacity to improve therapeutic agent penetration through the epidermal barrier. Topically applied ethosomes decrease systemic absorption and lengthen the drug molecule's residence period in the stratum corneum and epidermis. These characteristics make it easy for ethosomes to enter the deeper layers of skin and circulation. Deeper layers of the epidermis are disrupted by ethanol, which improves lipid fluidity and facilitates improved drug molecule penetration. Many bacterial infections, including folliculitis, impetigo, acne vulgaris, wound infections, and other superficial skin infections, are treated with azithromycin, a broad-spectrum macrolide antibiotic. By attaching to the 50S ribosomal subunit and preventing bacterial protein synthesis, it demonstrates exceptional antibacterial action against both Gram-positive and Gram-negative bacteria. Azithromycin's incorporation into ethosomal gel increases antibacterial efficacy, reduces systemic adverse effects, improves patient compliance, and offers targeted and prolonged drug administration at the site of infection. Azalides, a subclass of macrolide antibiotics, include azithromycin. It is generated from erythromycin and has a 15-membered lactone ring due to the incorporation of a methyl-substituted nitrogen atom.
Azithromycin's mode of action
Accumulating effectively in cells, particularly phagocytes, it is delivered in high concentrations to sites of infection, as reflected in rapid plasma clearance and extensive tissue distribution. Azithromycin is indicated for respiratory, urogenital, dermal and other bacterial infections, and exerts immunomodulatory effects in chronic inflammatory disorders, including diffuse pan bronchiolitis, post-transplant bronchiolitis and rosacea.
When it comes to the Gram-negative pathogen H. influenzae, azithromycin is much more effective than either erythromycin or clarithromycin. 201 Like other well-known macrolides, it is also very effective against M. catarrhalis, another Gram-negative pathogen of the upper respiratory tract, and C. trachomatis, an intracellular pathogen. Azithromycin is used in clinical settings to prevent MAC infections in AIDS patients and to treat respiratory tract infections, otitis media, pharyngitis, sinusitis, and trachoma eye infections. Azithromycin is an antibiotic drug used to treat various bacterial infections. It is marketed under the trade names Zithromax (for oral usage) and Azasite (for eye drops). This covers strep throat, pneumonia, middle ear infections, traveler's as well as certain other intestinal illnesses. It can also be used to treat malaria in conjunction with other drugs. It is given orally, intravenously, intraocularly.
The pharmaceutical company Pliva made the discovery of azithromycin in Yugoslavia (modern-day Croatia) in 1980, and it was authorised for use in medicine in 1988.
With more than 8 million prescriptions, it was the 78th most prescribed drug in the US. It is offered under numerous brand names and is accessible as a generic pharmaceutical.
Skin:
Skin layers make up the majority of the skin, while fine wrinkles, hairs, and skin surface lipids are found on the skin's outermost layer. Depending on how they are structured, these components have rather diverse optical behaviours.
Skin layers:
The skin is the most versatile and extensive channel for administering topical and systemic drugs. When applied topically, the stratum corneum, the skin's outermost layer, limits the bioavailability of medications by acting as the skin's most resilient barrier against drug penetration.
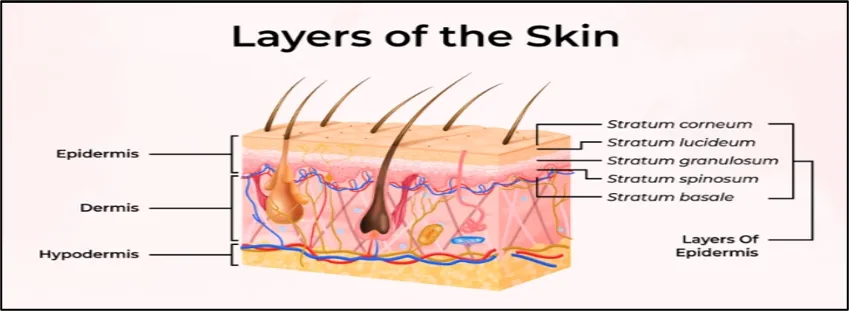
Figure No. 01: Layer of skin
Epidermis:
The epidermis and dermis are the two distinct layers that make up the skin layer. There is a distinct, wavy border between these two levels, as the illustration illustrates. Depending on a person's gender, age, body parts, etc., the skin layer's thickness varies significantly. Skin conditions like water retention can vary by location, age, and person. For example, because the NMF tends to decline with age, elderly people's skin layers are less able to retain water. Additionally, it has been shown that the stratum corneum, the outermost layer of the epidermis, becomes less transparent as its water content increases.
Stratum spinosum [prinkle cell layer]: Refers to the 10 to 20 layers that cover the basal cells. These layers are formed by turn-over, which causes the cells to become somewhat flatter [multi-sided]. These cells, which feature tiny spines on the exterior of their membrane, are known as prickle cells. Usually, these sublayers range in thickness from 50 to 150 µm.
Stratum granulosum [granular cell layer]: Consists of two to four layers of granular cells. The average thickness is 3 µm. Keratinisation of keratinocytes, a type of cornification, starts in this sublayer. Organelles like mitochondria and nuclei begin to resolve during this step. Compared to basal and prickle cell layers, cells have less moisture and are progressively packed with keratin fibres.
Stratum lucidum [clear layer]: can only be found in the palms and soles. This sublayer is extremely refractive. During turnover, its cells get flatter and more closely packed.
Stratum corneum [horny cell layer]: Is the epidermis' outermost layer. It is between 8 and 15 µm thick. This sublayer is made up of multiple layers of hard, flat, hexagon-shaped cells called corneocytes or horny cells. These are keratin-fiber-filled, dry, dead cells devoid of organelles.
Bacterial infection on skin:
When bacteria penetrate the skin through hair follicles or tiny skin breaks caused by scrapes, punctures, surgeries, burns, sunburns, animal or insect bites, wounds, and pre-existing skin conditions, they can cause bacterial skin infections. A number of activities, such as gardening in polluted soil or swimming in a contaminated pond, lake, or ocean, can cause bacterial skin infections in people.
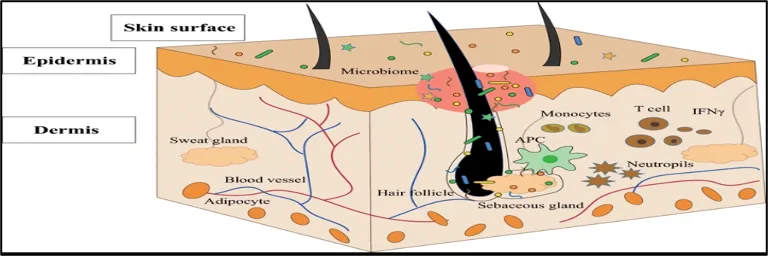
Figure No.02: Fungal infection on skin
Classification of Bacterial Infections:
Carbuncles: carbuncle is a cluster of boils that form a connected area of infection.
Ecthyma: Ecthyma is a skin infection. It is similar to imprtigo, but occurs deep inside the skin.
Folliculitis: Folliculitis is a common skin condition that happens when hair follicles become inflamed. It's often caused by an infection with bacteria.
Furuncles: Furuncles [boils] are skin abscesses caused by staphylococcal infection, which involve a hair follicle and surrounding tissue.
Impetigo: impetigo is a common bacterial skin infection that spreads easily. It causes itchy sores or blisters to form on exposed skin, commonly around the nose or mouth. Impetigo is seen most often in babies and young kids.
Ethosomes:
Ethosomes are lipid-elastic vesicles that have a high concentration of alcohol and phospholipids. Ethosomes are non-invasive delivery systems that deeply penetrate the epidermis. Ethosomes are pliable and flexible. Ethosomes are primarily utilised for medications with large molecular weight and poor solubility. Because of the combination of phospholipids and high ethanol concentrations in vesicular formulations, ethosomes have a synergistic effect that allows for deeper dispersion and penetration in the skin lipid bilayer. The size of ethosomes varies from nanometres to microns.
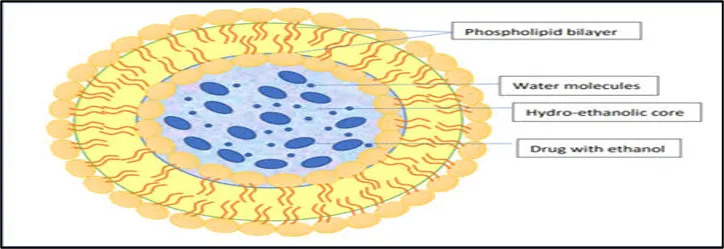
Figure No.3: Structure of Ethosome
Types of Ethosomal Systems:
1. Classical Ethosomes: Classical ethosomes are composed of phospholipids, water and high concentration of ethanol (40%). Drugs having molecular weight ranging from 130,077 Da to 24kDa can be entrapped in classical ethosomes.
2. Binary Ethosomes: Binary ethosomes can be prepared by adding another type of alcohol to the classical ethosomes. Propylene glycol (PG) and isopropyl alcohol (IPA) are most commonly used alcohols.
3. Transethosomes: It contains basic components from classical ethosomes and a penetration Enhancer (surfactant). Developed to combine the advantages of classical ethosomes and transferosomes to produce transethosomes. Transethosomes are advanced type of ethosomes as they have the advantages of both i.e classical ethosome and transferosomes.
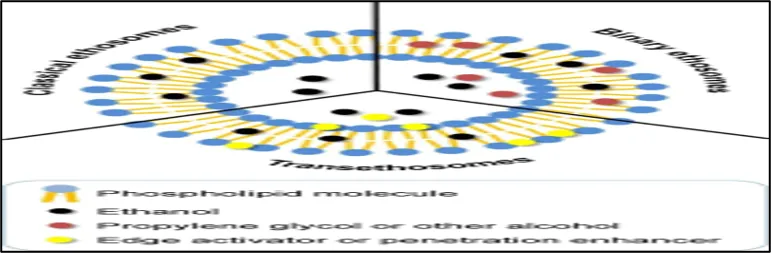
Figure No. 04: Types of Ethosome
How do ethosomes work?
Because ethosomes and skin lipids interact more effectively than liposomes, they enhance the distribution of active ingredients over liposomes. When ethanol interacts with the lipid molecules in the polar head group region, the transition temperature of the lipids in the stratum corneum is lowered, which results in the drug being delivered into the deep levels of the skin by reducing lipid multilayer density and boosting fluidity; also, ethanol gives vesicles flexibility and smoothness, allowing for deeper penetration into the epidermal layer.
METHOD:
Cold Method
Phospholipid, cholesterol, drug, ethanol, and PEG were mixed and heated to 40 °C. Distilled water was added slowly with continuous stirring at 700 rpm, and mixing was continued for 5 minutes. The dispersion was cooled for 30 minutes at room temperature. Finally, it was sonicated at 4 °C for five cycles (3 minutes each) using a probe sonicator.
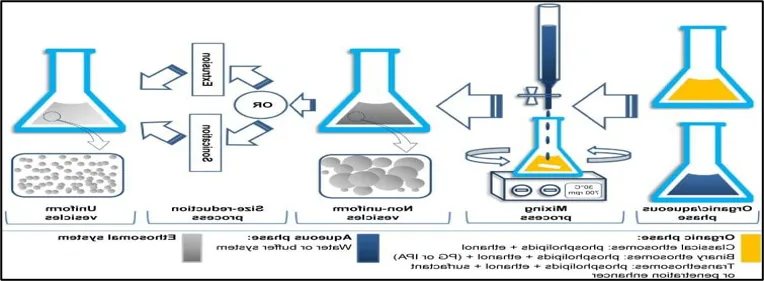
Figure No. 5: Cold Method
Hot Method:
Phospholipids are dispersed in water and heated at 40 °C to form a colloidal solution. In another vessel, ethanol and propylene glycol are mixed and heated to 40 °C. The organic phase is then added to the aqueous phase at the same temperature, and the drug is dissolved based on its solubility. Vesicle size is finally reduced using probe sonication or extrusion.
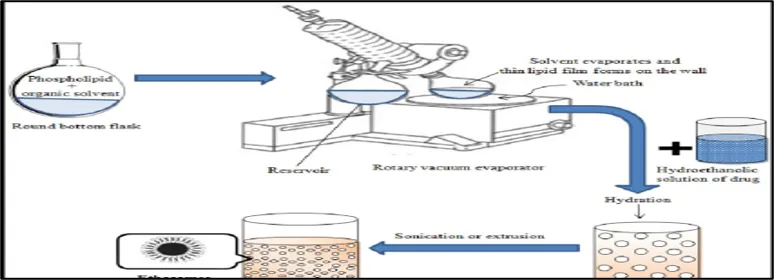
Figure No.6: Hot Method
Classic mechanical dispersion method:
The phospholipid and drug are dissolved in ethanol and heated to 30 °C. Distilled water is then added slowly to this mixture with continuous stirring at 700 rpm. The formed vesicle suspension is collected in a closed vessel. Finally, the dispersion is homogenized by passing it through a polycarbonate membrane using a hand extruder for three cycles.
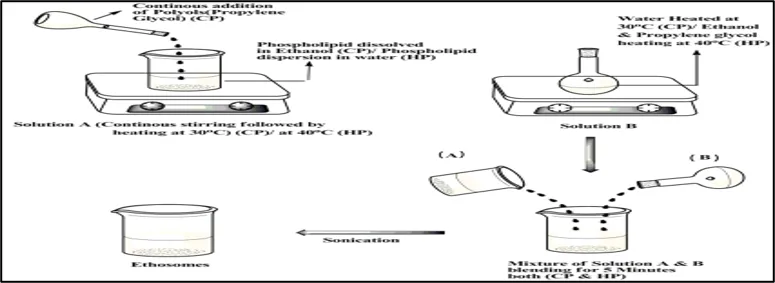
Figure No.7: Classic mechanical dispersion method
Classic Method:
Soya phosphatidylcholine is dissolved in a chloroform: methanol (3:1) mixture in a round-bottom flask. The solvents are evaporated using a rotary vacuum evaporator above the lipid transition temperature to form a thin lipid film. Remaining solvent traces are removed by keeping the flask under vacuum overnight. The dry lipid film is then hydrated with a hydroethanolic drug solution by rotating the flask at an appropriate temperature.
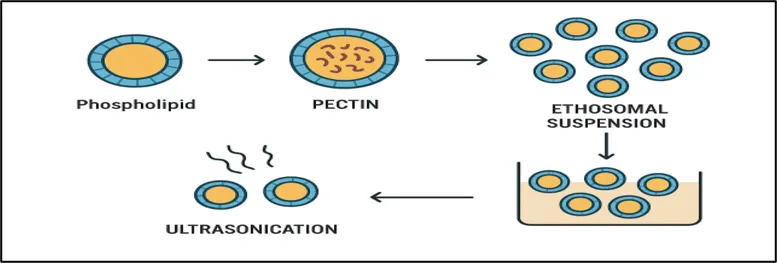
Figure No.8: Classic Method
MATERIAL AND METHOD
Material: Span 80, Polyethylene Glycol, Azithromycin , Soya lecithin ,Ethanol.
Method:
Cold Method
1. Weigh the required amount of Azithromycin and phospholipid.
2. Dissolved both in ethanol under magnetic stirring at 30-40 degree Celsius.
3. Add span 80 and polyethylene glycol. Heat the required amount of distilled water to the same temperature (30-40 degree Celsius).
5. Slowly add the aqueous phase into the ethanolic phase with continuous stirring to form ethosomes.
6. Stir the resulting dispersion for 30-40 minutes. Preparation was left to cool at room temperature for 30 min.
7. Then it was magnetic stirring 4 degree celcious for five cycles at 3 min, each with a min. rest between cycles using a magnetic stirrer.
Formula For Ethosomes Formulation
Table no. 1.Formula for Ethosomal Suspension
|
Sr. No |
Ingredient |
F1 |
F2 |
|
1 |
Azithromycin |
100mg |
100mg |
|
2 |
Soya lecithin (Phospholipid) |
250mg |
500mg |
|
3 |
Ethanol |
20ml |
25ml |
|
4 |
Span 80 |
100mg |
100mg |
|
5 |
Polyethylene Glycol |
10mg |
10mg |
|
6 |
Distilled Water |
10ml |
5ml |
EVALUATION PARAMETER OF ETHOSOME SUSPENSION
1. Particle shape analysis
The particle shape analyzed by using optical microscope.
2. pH-
The pH of the formulation was determined by using digital pH meter. The measurment of pH of theformulation was done in triplicate and average values are calculated.
3. Particle size & Zeta potential –
Particle size shows the average diameter of the ethosome vesicle. Zeta potential represents the surface charge of the vesicles, which helps to predict their stability. These parameters were measured using a Zetasizer instrument.
4. Entrapment efficiency - EE is defined as the ratio of drug molecules encapsulated into the ethosomal nanoparticles to the total used drug, and can be determined by the following equation.
EE= (Amount of trapped drug/Total amount of initially added-drug) × 100% after preparing ethosomal dispersion unentrapped drug is separated by dialysis, gel filtration and centrifugation.
Centrifugation
Centrifuge the sample at high speed (e.g., 15,000-20,000 rpm) for 60 minutes at 4°C. This separates the free (unentrapped) drug in the supernatant from the entrapped drug in the ethosomal pellet.
Separation: Carefully decant or pipette out the supernatant without disturbing the pellet.
Preperation of Carbopol gel
Table No. 02. Formula for Carbopol gel
|
Sr. No |
INGREDIENT |
QUANTITY |
ROLE |
|
1 |
Carbopol 934 |
0.350 gm |
Gelling agent |
|
2 |
Triethanolamine |
1-2 drops |
pH Adjuster |
|
3 |
Methyl Paraben |
0.03 gm |
Prservative |
|
4 |
Distilled Water |
q.s to 10 ml |
Vehicle |
Procedure
Take the required quantity of distilled water in a clean beaker. Slowly add Carbopol 934 into the distilled water with continuous stirring to avoid lump formation. Stir the mixture continuously for 30 minutes using a mechanical stirrer. Allow the dispersion to soak for 30 minutes. Add the required quantity of methyl paraben as a preservative and mix properly. Add triethanolamine dropwise with continuous stirring for neutralization. Continue stirring until a clear, smooth, and transparent gel base is obtained.
Preperation of ethosomal gel
Table No. 03. Formula for Ethosomal gel
|
Sr. No |
INGREDIENT |
QUANTITY |
ROLE |
|
1 |
Ethosomal Suspension |
20 ml |
Drug delivery system |
|
2 |
Carbopol 934 |
0.350gm |
Gelling agent |
|
3 |
Triethanolamine |
1-2 drops |
pH Adjuster |
|
4 |
Methyl Paraben |
0.03 |
Prevent microbial growth |
|
5 |
Distilled water |
q.s to 10 ml |
Vehicle |
The incorporation of the drug loaded ethosomes into gels was achieved by slow mechanical mixing at 25 rpm for 10 minutes.
Evaluation of ethosomal gel
1. Organoleptic properties
Colour
Odour
Washability
Transperency
2 . pH
The gels were initially diluted with distilled water at a dilution factor of 100 in order to assess the pH of the prepared gels. Triplicate and average value calculated .1 gm gel dissolve in 100 ml distilled water pH was measured.
3. Spreadability
1g of ethosomal gel was pressed between two slides and left for about 5 minutes where no more spreading was expected. Diameters of spreaded circles were measured in cm and were taken as comparative values for spreadability. The standardized weight tied on the upper slide was 500gm. The results obtained are average of three determinations.
4. Homogeneity and Grittines
A small quantity of ethosomal gel was pressed between thumb and the index finger. The consistency of ethosomal gel was noticed ( whether homogeneous or not ), if there is any coarse particle appeared on fingers .Also the homogeneity could be etected when a small quantity of ethosomal gel was rubbed on the skin of the back of the hand . The grittiness of prepared ethosomal gel was also observe in same manner.
5. Irritation test
Simply applying the gel to the skin and watching for any changes was how the irritation test was carried out.
6. Antibacterial Activity : Well diffusion method
1. The inoculum of the microorganism was prepared from the bacterial cultures.
2. 15 ml of nutrient agar (Hi media) medium was poured in clean sterilized Petri plates and allowed to cool and solidify.
3. 100 µl of broth of bacterial strain was pipette out and spread over the medium evenly with a spreading rod till it dried properly.
4. Wells of 6mm in diameter were bored using a sterile cork borer.
5. Solutions of the compounds (100µl/ml) were prepared in Water and 100µl of prepared test solutions (1mg/ml) and standard was added to the wells.
6. The petri plates incubated at 370C for 24 h.
7. Streptomycin (1mg/ml) was prepared as a positive control and DMSO was taken as negative control.
8. Antibacterial activity was evaluated by measuring the diameters of the zone of inhibitions (ZI).
RESULT & DISCUSSION
1. Particle Shape analysis-
The ethosomes prepared using fluconazole drug was studied under microscope to observe the formation of ethosomal vesicles. The shape of the ethosomes was obsereved spherical.
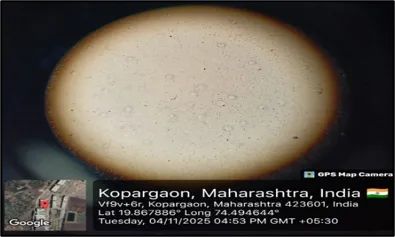
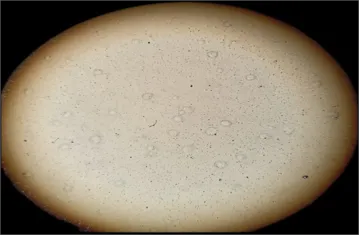
Figure no.9 Particle shape
2. pH-
The standard range of the pH of the ethosomal solution was 5-7 and the pH of the ethosomal solution was found to be 5.73 which is ideal pH.
Table No. 04. pH for Ethosomal Suspension
|
SR.NO |
SOLUTION |
pH |
Mean |
|
1. |
Ethosomal Suspension |
5.72 |
5.73 |
|
2. |
5.74 |
||
|
3. |
5.73 |
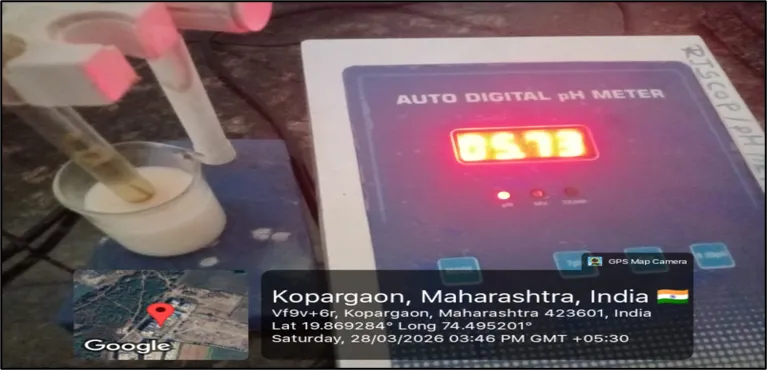
Figure no .10 Determination of pH
3. Particle size & Zeta potential-The prepare Azithromycin-loaded ethosomes show an average particle size of 398nm .The zeta potential was found to be -32mV, confirming good stability of ethosomal suspension.
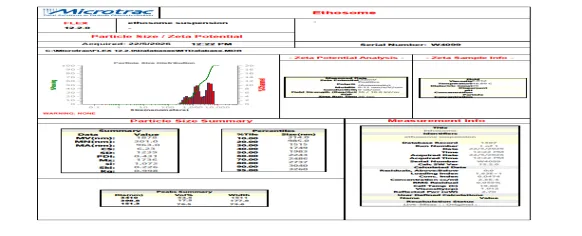
Figure No.11. Particle size & Zeta potential
4. Entrapment efficiency-
The entrapment efficiency of ethosome is of ethosome is 84.47%.
Ethosomal gel Evaluation
Table No. 05.Organoleptic Properties
|
Sr. No |
Parameter |
Result |
|
1 |
Colour |
Milky white |
|
2 |
Odour |
Charecteristics |
|
3 |
Washability |
Washable |
|
4 |
Transperency |
Translucent |
2. pH
Table No. 06. pH of Ethosomal gel
|
Sr. No |
Range of pH |
pH |
|
1 |
5.6-7.0 |
5.65 |
Figure No.12. pH of Ethosomal gel
3. Spreadability
Spreadability of ethosomal gel is 5.5gm.cm /sec.
Figure No.12. Spreadability of Ethosomal gel
4. Homogeneity and Grittines
Ethosomal gel was found to be homogeneous and no grittiness was noted.
5. Irritation test
The result of skin irritation study revealed no irritation from ethosomal gel.
6. Antibacterial Activity
Antibacterial activity of test compound against E. coli.
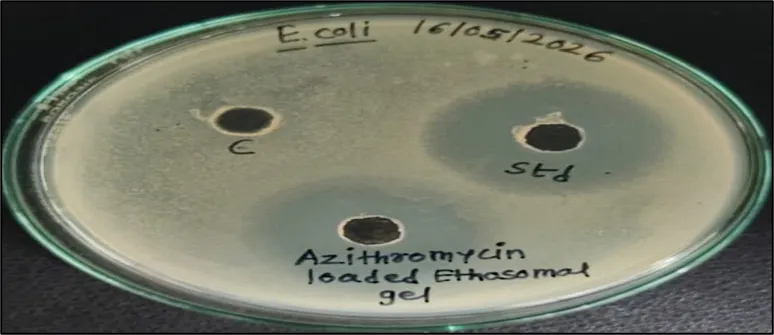
Figure No.13. Antibacterial activity
|
Table No. 07. Zone of inhibition of Antibacterial activity |
||
|
SR. NO |
SAMPLES |
ZONE IN DIAMETER (mm) |
|
1 |
Control |
00 |
|
2 |
Standard (Streptomycin) |
27 |
|
3 |
Azithromycin loaded Ethosomal gel |
23 |
Conclusion of the study:
The antibacterial pro?le of Azithromycin loaded Ethosomal gel was evaluated by measuring the zone of inhibition against E. coli( ATCC 25922) bacterial strains via well diffusion method. The compound Azithromycin loaded Ethosomal gel exhibited moderate antibacterial activity as compared to the standard streptomycin.
CONCLUSION
The study successfully prepared and evaluated fluconazole-loaded ethosomal suspension for topical drug delivery. Conventional formulations used for treating fungal infections often show limited therapeutic effect, poor stability, and lower safety. Many topical antifungal drugs fail to penetrate deeply into the skin because they cannot easily pass through the stratum corneum, which is the outermost protective layer of the skin. Due to this, the treatment becomes less effective and does not provide proper relief in fungal infections. These problems can be solved by using the ethosomal drug delivery system. Unlike liposomes and transfersomes that face difficulty crossing the stratum corneum, ethosomes have high flexibility and better penetration ability because of their high ethanol content. This allows the drug to reach deeper skin layers and improve therapeutic action.
REFERENCES

Suvarna Sangale, Kanchan Gursal, Formulation and Evaluation of Ethosomal Gel of Azithromycin for Bacterial Infection, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1766-1779. https://doi.org/10.5281/zenodo.20577579
 10.5281/zenodo.20577579
10.5281/zenodo.20577579