
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dr. Kolpe Institute of Pharmacy, Kolpewadi, Maharashtra, India.
Mouth ulcers, clinically known as ulcers or “Recurrent Aphthaous stomatitis “rank among the most prevalent oral mucosal conditions affecting approximately 10–20% of the global population. Defined by superficial sores, on non-keratinized oral tissue RAS significantly disrupts chewing, swallowing and overall quality of life. Present therapeutic choices, topical corticosteroids, anesthetics, antiseptics and systemic immunomodulators provide symptom relief; however their effectiveness is often limited by undesirable systemic side effects or inadequate local retention at the targeted area. Consequently there is increasing focus on creating safe, natural and “patient acceptable dosage forms”, like herbal lozenges. This research concentrates on the development, analysis and assessment of an Herbal lozenge created to deliver anti-inflammatory, Antimicrobial and mucosal-calming phytochemicals directly to the target area. Cinnamon (Cinnamomum verum) was chosen as the active compound due, to its rich concentration of cinnamaldehyde, known for its strong Antimicrobial, antioxidant and tissue-repairing effects (Ranasinghe et al., 2013). Extra botanical components, such as honey, Turmeric, Tulsi, ginger extract and menthol were incorporated to boost combined effects, in alleviating pain controlling microbes and promoting epithelial healing.
Mouth ulcers, medically termed Aphthaous ulcers or canker sores, are small, painful Lesions that develop on the mucous membranes inside the mouth. These ulcers can make eating, Drinking, and even speaking uncomfortable, impacting daily life significantly. While various Factors can contribute to their development, including stress, injury, or underlying health Conditions, finding effective treatments is crucial for managing symptoms and promoting healing [1]. The word “Aphthaous” originated from the Greek word “aphtha”, the meaning of which is ulcer. Aphthaous stomatitis is one of most common ulcerative disease associated mainly with the oral mucosa characterized by the extremely painful, recurring solitary, multiple ulcers in the upper throat and oral cavity. These types of ulcers are usually small, multiple, ovoid or round with circumscribed margins .which are having gray or yellow floors and are encompassed by erythematous halo [2, 3]. It was delineated in 400 B.C by Hippocrates; the disease is known by lay public and professionals by several other names such as cold sores, canker sores, “Recurrent Aphthaous stomatitis “(RAS), and recurrent Aphthaous ulcers (RAU). Нis is the most prevailing oral ulcerative disorder affecting up to 10-20% of our inhabitants and recurrence rate of 3 months in 50% of population [4]. These are quite painful that leads to difficulty in eating, speaking and swallowing that’s why it negatively affects the patient’s quality of life [5]. Aphthaous stomatitis is divided into three varieties: minor aphthae, major aphthae and herpetiform. Minor aphthae also called as Miculiz’s aphthae, is one of the most common variant that constitute 75-85% of all RAS cases. These types of ulcers have size usually less than 1 cm (10 mm) and heal without leaving scarring within 10 to 14 days. His type is commonly found in the non-keratinized mucosal surfaces like buccal mucosa, labial mucosa, and mouth floor. Major Aphthae also called as Sutton’s disease; usually exceeds 1 cm (10 mm) cause deeper ulceration thus leave scar. It constitutes only 10-15% of RAS cases. These ulcers may remain about 10-20 days and may take months also. Нe usual sites are throat, lips and soft palate. Нe Herpetiform is least common variant of RAS that constitutes only 07-10% of RAS cases. Ulcer size is very small measuring 2-3 mm in diameter; numerous in numbers (around 100 ulcers at once) can fuse together producing large irregular lesions that last for 7-10 days without leaving scars [6-7].
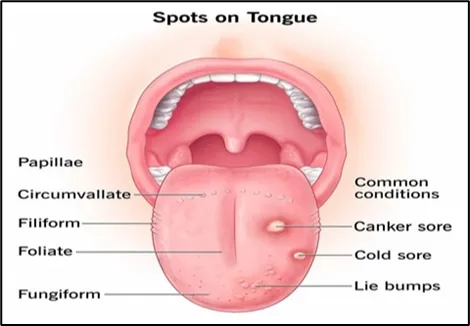
Figure 1: Mouth Ulcer
ANATOMY OF THE ORAL MUCOSA [8-12]
The oral cavity is lined by a mucous membrane (mucosa) that varies in thickness and keratinization depending on the location and function.
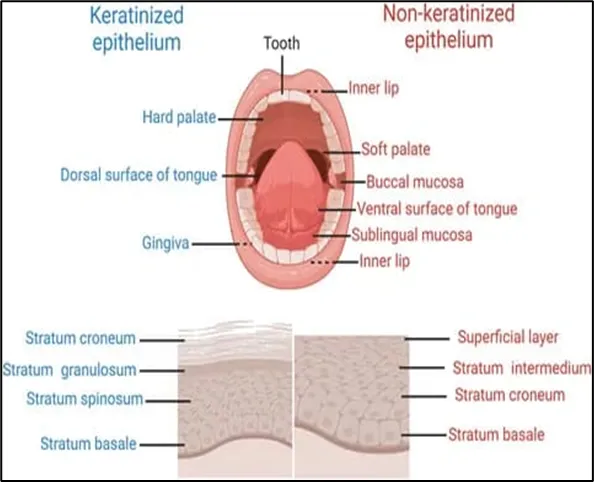
Figure 2: Anatomy of oral mucosa
PHYSIOLOGY
The process of ulcer formation and healing is broadly similar to skin wounds but with key differences, particularly less inflammation and the absence of scarring in most cases.
Pathophysiology of Oral Aphthaous Ulcer
The pathogenesis of recurrent aphthosis stomatitis (RAS) remains not completely understood. It likely involves a predominantly cell-mediated inflammation involving T-cells and TNF-α (tumor necrosis factor-alpha) production. Light and electron-microscope examination of oral Aphthaous ulcers showed a penetrating, early, lympho-monocyte infiltration of the epithelium. According to a study by Lehner [13], under light microscopy, oral ulcer epithelium showed considerable intercellular edema and degenerative changes. There was epithelial hyperplasia and only the basement membrane adjacent to the ulcer was affected, the rest of the basement membrane appeared intact. Mononuclear cells normally infiltrate the basal-cell and prickle-cell layers of the epidermis and they are most commonly lymphocytes and monocytes, but superficial to and immediately adjacent to the ulcer neutrophil polymorphs were also found. According to Lehner [13], the Intra-nuclear inclusion bodies were found in 3 out of the 25 biopsies examined by electron microscopy. The affected nuclei were slightly larger and the nucleoli were uneven in shape. Inclusion bodies were not seen in the cytoplasm. Herpetiform ulcers differ from recurrent Aphthaous ulcers in that they showed epithelial vesicles and intra-nuclear inclusion bodies, suggesting a virus etiology. The immuno-fluorescent studies showed predominantly IgG and IgM binding only in autologous tissues from patients with Aphthaous ulcers [14]. This reaction could indicate blood group antigens, trapped globulins due to the inflammatory reaction, non-immunological Physicochemical binding of the fluorescent conjugate, or normal immunoglobulin transport through the oral mucosa. An immunofluorescent examination couldn’t detect specific globulin binding to salivary gland tissue in the oral Aphthaous lesion. Major Aphthaous ulcers do not differ much from minor Aphthaous ulcers, but they have an increase in the degree of severity of the pathological changes. There were no vascular abnormalities and fibrinous necrosis noticed in recurrent oral ulcers. A three-fold rise in mast cells was found in recurrent oral Aphthaous, in contrast to a decreased count in non-specific ulcers. Mast cell count was present in all three groups of oral ulcers when it was compared with that in other oral lesions and normal tissue. Leukocytes have a normal chemotactic function in oral aphthosis but in Behcet’s disease, they showed hyperactive function [13]. There’s a chance that a few immunologically arbitrated mechanisms are playing an important role in the pathogenesis of oral aphthosis. It may be due to an unopposed or excessive production of IL (interleukin)-1 or IL-6, which is essential for its development, a concept that may explain why ulceration worsens after local injury, or cessation of smoking, or both [15].
Pathophysiological Mechanisms [8-12]
The exact cause of the most common type, “Recurrent Aphthaous stomatitis “(RAS), is often unknown but is considered multifactorial, involving a T-cell-mediated immune response.
TYPES OF MOUTH ULCER:
ETIOLOGY
CAUSE OF MOUTH ULCER:
SYMPTOMS OF MOUTH ULCER:
|
Topical antiseptic |
Chlorhexidine Gluconate, Triclosan |
|
Topical/ Systemic Anti-inflammatory/ Analgesic |
Benzydamine Hydrochloride, Diclofenac |
|
Topical Anesthetic |
Lidocaine, Benzocaine |
|
Topical antibiotic |
Chlortetracycline, Doxycycline |
|
Topical corticosteroids |
Hydrocortisone hemisuccinate, Triamcinolone acetonide, Betamethasone valerate, Beclometasone dipropionate, Budesonide, Clobetasol |
2) Second Line Therapy
|
Systemic Immunomodulator |
Levamisole, Colchicine, Hydrocortisone and Triamcinolone, Thalidomide, Dapsone, Pentoxphylline, 5-Amino salicylic acid, Azathioprine, Prostaglandin E2 |
|
Systemic Antibiotic |
Penicillin G Potassium |
|
Systemic Corticosteroids |
Prednisone |
CINNAMON BARK
Synonyms:-[21,22]
Dalchini, Ceylon Cinnamon, Cinnamon bark
Biological Source
Cinnamon is the dried inner bark of the coppiced shoots of Cinnamomum zeylanicum Nees., belonging to family Lauraceae.
Botanical Classification
Morphological characteristic
Chemical Constituent:
Volatile oil, tannins mucilage, calcium oxalate, starch, mannitol, Cinnamon oil
Geographical source: Sri lanka, Malabar Coast of India, Jamaica and Brazil

Fig 3.Cinnamon bark
Uses of cinnamon bark
Bark is used as-
Commercially used as:
In preparation of candy dentrifices and perfumes.
HONEY
Synonyms
Madhu, Madh, Mel, Purified Honey.
Biological Source
Honey is a viscid and sweet secretion stored in the honey comb by various species of bees, such as Apis mellifera, Apis dorsata, Apis florea, Apis indica and other species of Apis, belonging to family Apideae (Order: Hymenoptera).
Morphology of Honey
Chemical Constituents
Geographical Source
Africa, India, Jamaica, Australia, California, Chili, Great Britain and New Zealand.

Fig 4.Honey
Uses
HALDI (HINDI); CURCUMA;
Biological Source
Turmeric is the dried rhizome of Curcuma longa Linn. (syn. C.domestica Valeton)., belonging to family Zingiberaceae.
Chemical Constituents
Geographical Source
The plant is a native to southern Asia and is cultivated extensively in temperate regions. It is grown on a larger scale in India, China, East Indies, Pakistan, and Malaya.

Fig 5. Turmeric
Uses
TULSI
Synonyms
Sacred basil, Holy basil.
Biological Source
Tulsi consists of fresh and dried leaves of Ocimum sanctum Linn. belonging to family Labiatae.

Fig 6. Tulsi
Chemical Constituents
Geographical source
Uses
GINGER
Synonyms
Rhizoma zingiberis, Zingibere.
Biological Source
Ginger consists of the dried rhizomes of the Zingiber officinale Roscoe, belonging to family Zingiberaceae.
Chemical constituents
Geographical Source
It is mainly cultivated in West Indies, Nigeria, Jamaica, India, Japan, and Africa.
Uses
Antiemetic, positive inotropic, spasmolytic, aromatic stimulant, carminative, condiment, and flavouring agent.

Fig 7. Ginger
Lozenges are solid formulations that Include medications in a sweet and flavored base. They are meant to dissolve slowly in the mouth, like medicated candies.
Providing relief to the Irritated tissues in the throat. Lozenges are a commonly used type of medicine. The advantages of medicated lozenges include prolonging the time .The medicine stays in the mouth, improving its Absorption, reducing stomach irritation, and avoiding the initial metabolism in the liver.
TYPES OF LOZENGES:
Types of Lozenges:
Organization of Lozenges:
Rendering near Position of Act:
Giving to touch then arrangement:
Advantages and disadvantages of Lozenges [27, 28]
Rina G Maskare et al., 2022[1]
Mouth ulcers, or Aphthaous ulcers, are common oral lesions that cause significant discomfort and can interfere with daily activities such as eating and speaking. This research focuses on the development and evaluation of herbal lozenges incorporating Neem (Azadirachta indica) and Tulsi (Ocimum sanctum) as primary active ingredients for the treatment of mouth ulcers. Neem is renowned for its potent anti-inflammatory, Antimicrobial, and wound-healing properties, while Tulsi is valued for its analgesic and anti-inflammatory effects. The lozenges were formulated to dissolve slowly in the oral cavity, ensuring prolonged contact with ulcerated tissues, thereby maximizing therapeutic efficacy. Comprehensive evaluation included assessments of Physicochemical properties, taste, texture, and stability, alongside in vitro studies to determine Antimicrobial and healing potential. Results demonstrated that the synergistic combination of Neem and Tulsi in lozenge form provided effective pain relief, reduced inflammation, and promoted faster healing of mouth ulcers. The formulation was well-tolerated and exhibited favorable organoleptic properties. These findings suggest that herbal lozenges represent a promising, natural, and patient-friendly approach for the management of mouth ulcers, warranting further clinical investigation for widespread therapeutic use.
Pooja Yadav et al., 2018[29]
Lozenges are one of the widely used solid dosage forms. They contain medicament and are meant to be in mouth or pharynx. Lozenges have been in use since 20 th century and are still in commercial production. Lozenges provide a palatable means of dosage form administration and possess excellent advantages; though they suffer certain disadvantages too. Lozenges are adopted for both local and systemic administrations and a wide range of active ingredients can be incorporated in them. Lozenges currently available in market are: Caramel based soft lozenges, hard candy lozenges and compressed tablet lozenges. This present review covers researches performed till date, formulation and evaluation parameters, packaging and applications of lozenges.
Surbhi chaurasaya et al., 2018[30]
Lozenges are one of the very popular and better innovative dosage form and oral confectionary products. Lozenges have been in use since 20th century and are still in commercial production. Lozenges have bright future as a novel method of delivering drugs for local action and systemic effect in the oral cavity. The “lozenges are solid medicated, flavored and sweetened base dosage forms intended to be sucked and hold in the mouth/pharynx”. The benefits of the medicated lozenges is they increase the retention time of the dosage form in oral cavity which increases bioavailability, reduces gastric irritation and bypasses first pass metabolism. The acceptance for lozenges as a dosage form is high by adults and also more by children. Different types of lozenges available in market are compressed lozenges, hard lozenges & soft lozenges and their methods of preparation along with ingredients used in their preparation are discussed. The present review covers more or less all aspects associated with lozenges and also throws light on the applications of lozenges. It includes various researches performed till date, formulation and evaluation parameters, packaging and applications of lozenges.
Aim:
To formulate and evaluate herbal lozenges for effective treatment of mouth ulcers.
Objectives:
Need of the Study:
Ingredient Category Role
|
Ingredient |
Category |
Role |
Quantity |
|
Jaggery (Base) |
Sweetener/ Vehicle |
Provides the bulk and structure |
60 g |
|
Honey |
Demulcent/ Sweetener |
Soothes the throat. |
15 ml |
|
Turmeric & Ginger |
Active Ingredients |
Anti-inflammatory and Antimicrobial Properties. |
10 g |
|
Tulsi Extract |
Active Ingredient |
Immune support and respiratory relief. |
5 g |
|
Menthol & Cinnamon oil |
Flavouring/ Cooling |
Improves palatability and provides a cooling Sensation. |
2 ml |
|
Citric acid |
Preservatives |
Prevents microbial and fungal growth. |
1 g |
|
water |
solvent |
vehicle |
q.s |
PROCEDURE
Fig. Mold

Fig. Packaging
1. Physical Observation: The colour, odour, texture and taste of the lozenges were evaluated by direct observation.
|
Sr.No. |
Observation |
Batch 1 |
Batch 2 |
|
1 |
Colour |
Brown |
Brown |
|
2 |
Odour |
Slightly sweet |
Sweet |
|
3 |
Texture |
Hard |
Hard |
|
4 |
Taste |
Sweet |
Sweet |
Weight Variation= Average weight-Individual weight/Average weight*100
Average weight = 2.500 g
Weight variation
|
Sr. No. |
Weight of Individual Lozenges(gm) |
Percent Weight Variation (%) |
||
|
1 |
Batch 1 |
Batch 2 |
Batch 1 |
Batch 2 |
|
2 |
1.525 |
2.510 |
88 |
99 |
|
3 |
1.498 |
2.485 |
87 |
99 |
|
4 |
1.520 |
2.530 |
88 |
98 |
|
5 |
1.525 |
2.470 |
88 |
98 |
|
6 |
1.553 |
2.505 |
87 |
99 |
|
7 |
1.623 |
2.490 |
87 |
99 |
|
8 |
1.543 |
2.520 |
87 |
99 |
|
9 |
1.525 |
2.447 |
88 |
99 |
|
10 |
1.546 |
2.515 |
87 |
99 |
|
Sr.No. |
Observation |
Batch 1 |
Batch 2 |
Inference |
|
1 |
Average weight |
13.650gm |
2.500 gm |
Acceptable weight variation limit lies between 85%-115% |
|
2 |
Average weight variation |
84% |
90 % |
Initial weight= 25.010 for 10 g
Final weight= 24.890
% Friability= Initial weight- final weight *100 Initial weight
Friability test
|
Sr. No. |
Observation |
Batch 1 |
Batch 2 |
Inference |
|
1 |
Friability |
1.2 |
0.48 |
Limit of friability upto 1% |
Hardness testing
|
Sr. No. |
Observation |
Batch 1 |
Batch 2 |
Inference |
|
1 |
Hardness |
4.8 kg/cm2 |
5.9 kg/cm2 |
It should range from 4.4- 7.5 ± 0.5 kg/cm2 |
|
Sr. No. |
Observation |
Batch 1 |
Batch 2 |
Inference |
|
1 |
Thickness |
0.7 cm |
0.8 cm |
It should lie between 0.5-1cm |
|
2 |
Diameter |
1.7 |
1.8cm |
It should lie between 1-1.5cm |
Weight of empty dish+ sample before drying (W1) = 65.21gm
Weight of empty dish+ sample after drying (W2) =65.18 gm
Weight of sample= 1.690 gm
%Moisture content= W1- W2/W*100
|
Sr. No. |
Content |
Batch 1 |
Batch 2 |
Interference |
|
1 |
Moisture content |
1.9 % |
1.3% |
Moisture content should not be more than 1.5% |
Herbal lozenges containing cinnamon, tulsi, ginger, turmeric, showed promising therapeutic potential in the treatment of mouth ulcers due to there antimicrobial, anti-inflammatory, and analgesic properties. which can reduce pain, prevent secondary infections, and promote healing by remaining in the mouth for extended contact. The formulation provided prolonged contact time in the oral activity; which may help in reducing pain and promoting ulcer healing.
REFERENCES

Kolpe Rani, Aher Gayatri, Bhosale Siddharth, Bhosale Pravin, Nikhade Sujit, Bhamare Samiksha, Formulation and Evaluation of Herbal Lozenges for the Treatment of Mouth Ulcer, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 7965-7978. https://doi.org/10.5281/zenodo.20447629
 10.5281/zenodo.20447629
10.5281/zenodo.20447629