
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sage Institute of Technology Pharmacy Sanjeev Agarwal Global Educational University, Bhopal
Cardiovascular arrhythmias exhibit circadian variation, with episodes often peaking during early morning and late-night hours, highlighting the need for chronotherapy. Amiodarone, a class III antiarrhythmic agent, is effective but limited by adverse effects and variable bioavailability when administered conventionally. This study aimed to develop and evaluate a pulsatile drug delivery system (PDDS) of amiodarone to synchronize drug release with arrhythmic chronobiology. Hydrogel plugs prepared with HPMC K15M demonstrated desirable swelling behavior and mechanical integrity, while core tablets showed uniform hardness, acceptable friability, and complete drug release within 90 minutes. Cross linked gelatin capsules modified with formaldehyde vapors provided controlled release, minimizing drug release in gastric conditions and enabling sustained release in intestinal pH environments. In vitro dissolution confirmed a lag phase followed by rapid release, aligning with circadian rhythm requirements. The pulsincap system thus offers a promising chronotherapeutic approach to optimize efficacy, reduce toxicity, and improve patient compliance in arrhythmia management. Further in vivo studies are warranted to establish clinical utility.
Cardiovascular diseases remain the leading cause of morbidity and mortality worldwide, with arrhythmias representing a significant subset that requires precise therapeutic intervention. Amiodarone, a class III antiarrhythmic agent, is widely prescribed for the management of supraventricular and ventricular arrhythmias due to its broad-spectrum efficacy. However, its conventional administration is associated with challenges such as dose-dependent adverse effects, variable bioavailability, and the need for long-term therapy, which often compromise patient compliance and therapeutic outcomes [1]. The pathophysiology of arrhythmias exhibits a distinct chronobiological pattern, with the incidence of cardiac events such as atrial fibrillation and ventricular tachyarrhythmias showing circadian variation, often peaking during early morning hours and late at night [2]. This temporal fluctuation underscores the importance of chronotherapy, wherein drug administration is synchronized with the body’s biological rhythms to maximize efficacy and minimize toxicity. Traditional sustained-release formulations fail to address these circadian variations, leading to suboptimal therapeutic control [3].
Pulsatile drug delivery systems (PDDS) have emerged as an innovative approach to overcome these limitations. Unlike immediate or sustained-release systems, PDDS are designed to release drugs after a predetermined lag time, followed by rapid and complete drug release, thereby aligning drug availability with the circadian rhythm of disease manifestation [4]. Such systems are particularly advantageous for drugs like amiodarone, which require precise timing of release to counter arrhythmic episodes while reducing systemic exposure during periods of low risk [5]. Several technologies, including capsular systems (Pulsincap™), compression-coated tablets, and osmotic devices, have demonstrated the feasibility of pulsatile release in chronotherapy [6]. By tailoring the release profile of amiodarone to match arrhythmic chronobiology, a pulsatile delivery system can potentially enhance therapeutic efficacy, reduce adverse effects, and improve patient adherence. Furthermore, evaluation parameters such as in vitro dissolution, lag time determination, and pharmacokinetic profiling are critical to establish the clinical utility of such formulations [7].
Thus, the development and evaluation of a pulsatile delivery system of amiodarone for chronotherapy of arrhythmia represents a promising strategy to optimize treatment outcomes, reduce toxicity, and advance personalized medicine in cardiovascular therapeutics.
MATERIAL AND METHODS
Amiodarone (AMD) was generously gifted by Medreich Pharmaceuticals, Bengaluru, India; any other reagent, polymer or chemical was purchased from verified sources and used as procured.
Preformulation Studies
The procured AMD was studied for preformulation parameters like organoleptic features, melting point, solubility, loss on drying and partition coefficient [8]. The infrared spectrum was obtained by scanning the pure AMD from 400-4000 cm-1 using attenuated total reflectance type FTIR spectrophotometer (Bruker) [9]. The calibration curve of AMD was constructed by measuring the absorbance of using different concentrations of the drug using methanol, pH 6.8, pH 7.4 and pH 1.2 at 310.4 nm [10].
Preparation and evaluation of the hydrogel plug
The hydrogel plug was prepared by direct compression method. Accurately weighed quantity (Table 1) of Hydroxy propyl methyl cellulose, spray dried Lactose and polyvinyl pyrrolidone were mixed together in a mortar for 10 minutes. Magnesium stearate was added to this mixture and further blended for 5 minutes. The prepared formula blend was compressed using single punch tablet machine [11].
Table 1. Formula for preparation of hydrogel plug
|
Sr. No. |
Ingredient |
Role |
Quantity |
|
1 |
HPMC K15M |
Polymer to control lag time |
7.00 g |
|
2 |
Lactose |
Filler |
2.50 g |
|
3 |
PVP K30 |
Binder |
0.35 g |
|
4 |
Magnesium stearate |
Lubricant |
0.15 g |
Shape and appearance: Hydrogel plugs were examined under a lens for the shape of the tablet, colour was observed by keeping the tablets in light
Weight Uniformity: Ten plug tablets were weighed individually on electric balance from which the mean was calculated, and the percentage deviations were determined.
Thickness: The thicknesses of ten plug tablets were determined using a Vernier calliper and the mean of these readings was taken as the mean of the tablet thickness.
Friability: The friability of the plug tablets was determined using the Roche friabilator. Five tablets were weighed and put into the friabilator and set to rotate at 25 rounds per minute for about four minutes. The tablets were then removed and weighed again.
Swelling Index: The hydrogel plugs were kept immersed in three different pH conditions. Plugs were taken out carefully at 2,4,6,8,10,12 hours and their weights were determined accurately. The swelling index for the hydrogel plug was calculated using formula:
% swelling = Wet weight-Dry weight*100/Wet weight
Preparation and evaluation of Amiodarone core tablet
Accurately weighed quantity of amiodarone and lactose were mixed together in a mortar. To this was added the super-disintegrants cross-carmellose sodium and ac-di-sol in required quantity as per Table 2 and mixed. The dry binder was added to the mixture and isopropyl alcohol if required to provide binding was added as required. Purified talc and magnesium stearate were finally added and the blend was mixed properly in a sealed polybag using tumbler action. The blends were punched into tablets by direct compression using single punch tablet press [12].
Table 2. Formula for obtaining optimum the core tablet
|
Sr. No. |
Ingredient |
AC1 (mg) |
AC2 (mg) |
AC3 (mg) |
AC4 (mg) |
AC5 (mg) |
|
1 |
Amiodarone |
100 |
100 |
100 |
100 |
100 |
|
2 |
Cross-carmellose sodium |
10 |
15 |
20 |
25 |
30 |
|
3 |
Ac-di-sol |
16 |
16 |
16 |
16 |
16 |
|
4 |
Lactose |
65 |
60 |
55 |
50 |
45 |
|
5 |
PVP K30 |
5 |
5 |
5 |
5 |
5 |
|
6 |
Isopropyl Alcohol |
q.s |
q.s |
q.s |
q.s |
q.s |
|
7 |
Magnesium stearate |
2 |
2 |
2 |
2 |
2 |
|
9 |
Purified Talc |
2 |
2 |
2 |
2 |
2 |
|
|
TOTAL |
200 |
200 |
200 |
200 |
200 |
The core tablet blends were evaluated for precompression parameters like bulk and tapped density, angle of repose, Carr’s index and Hausner’s ratio. The prepared tablets were evaluated for hardness, thickness, weight variation, friability, drug content and in vitro release.
Drug content
Five tablets from each formulation were weighed to determine the average weight. These tablets were crushed in a mortar then the amount of powder equivalent to 20 mg of drug was transferred in 20 mL of methanol. 10ml from this stock solution was withdrawn and diluted up to 100 mL with methanol. 0.6 mL from this stock solution was pipetted out and diluted to 10 mL. Absorbance of the resulting solution was measured at 310 nm using UV spectrophotometer and the drug content was calculated using calibration curve [13].
In vitro release profile
The USP type II paddle apparatus with a paddle speed of 50 rpm was used for dissolution testing for the formulated core tablets. The dissolution media used consisted of 900 mL of 0.1 N HCl and distilled water. 5 mL of samples were collected at time points and the media was replenished with the same volume of fresh media. The free drug concentration was estimated using a UV spectrophotometer at a wavelength of 310 nm [13].
Preparation of cross-linked gelatin capsules
The “0” sized hard gelatin capsules about 100 in number were taken. The body of the capsules was placed on a wire mesh. 25ml of 15%v/v formaldehyde was taken into a desiccator and potassium permanganate was added to it to generate formalin vapors. The wire mesh along with the body was kept in the desiccator. The reaction was carried out for 12 hours, after which the body were removed and dried at 50ºC for 30 minutes to ensure completion of reaction between gelatin and formaldehyde vapor. They were dried at room temperature to facilitate removal of residual formaldehyde [14].
Physicochemical characterization of treated empty gelatin capsules
Length of the capsule, external diameter of the capsule, thickness of the capsule was determined.
Qualitative test for free formaldehyde
Standard used is formaldehyde solution and sample solution is formaldehyde treated bodies (about 25 capsules), cut into small pieces and taken into a beaker containing distilled water. This was stirred for 1 h with a magnetic stirrer, to solubilize the free formaldehyde. The solution was then filtered into a 50 ml volumetric flask, washed with distilled water and volume was made up to 50 ml with the washings [15].
Solubility study of treated capsules
The capsule bodies were exposed to 15% formaldehyde solution in varying time intervals. Then exposed capsule bodies were dried in hot air oven. The solubility of bodies was tested in 0.1N HCL. The time at which the capsule dissolves or forms a soft fluffy mass was noted [16,17].
Preparation of pulsincap
The pulsincap was similar in appearance to a hard gelatin capsule, but the body was water insoluble. Core tablet of amiodarone was and placed into the bottom of formaldehyde treated body. The capsules were then plugged with prepared hydrogel plug and capsule cap was placed over the body [12].
In vitro release study of the puslincap formulation
Dissolution studies were carried out using USP dissolution test apparatus (paddle method). Capsule was tied to paddle with a cotton thread so that the capsule was immersed completely in dissolution media but not float. In order to simulate the pH changes along the GI tract, three dissolution media with pH 1.2, 7.4 and 6.8 were sequentially used (sequential pH change method). The pH 1.2 was first used for 2 h then removed and the fresh phosphate buffer pH 7.4 was added. After 3 h the medium was removed and colonic fluid phosphate buffer pH 6.8 was added for subsequent study. 900 mL of the dissolution medium was used at each time. Rotation speed was 100 rpm and temperature was maintained at 37±0.5°C; 10 mL of dissolution medium was withdrawn at predetermined time intervals and fresh dissolution media was replaced. The withdrawn samples were analysed at 310 nm, by UV absorption spectroscopy and the cumulative percentage release was calculated [18].
RESULTS AND DISCUSSION
Preformulation Studies
The preformulation studies were done to assess the suitability of utilizing the drug and the formulations for the formulation. AMD was found white, crystalline powder with no odor and a bitter taste. Its melting point was obtained to be 156-158°C. It was found to be soluble in DMSO, chloroform, and methanol and slightly soluble in water and presented a LOD of 0.3%w/w and Log P value of 6.70.
The absorption maximum of AMD was obtained to be 310 nm and its calibration curve was prepared at the above wavelength using UV spectrophotometer (Figure 1).
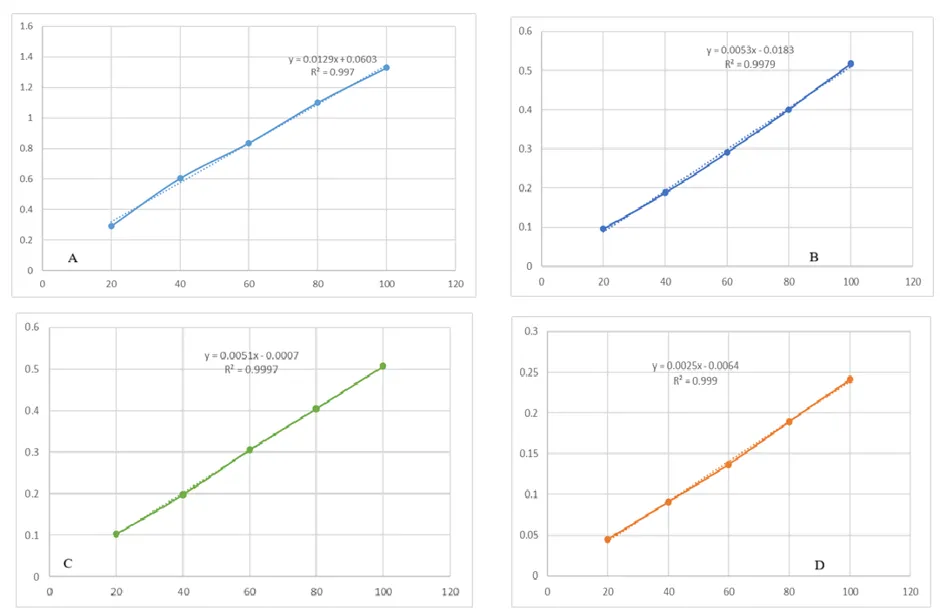
Figure 1. Calibration curve of AMD in (A) methanol (B) pH 6.8 (C) pH7.4 (D) pH 1.2
The FTIR spectra of AMD (Figure 2) reveals broad O–H/N–H stretching at 3333 cm-1, C-H stretching between 2919–2853 cm⁻¹, aromatic C=C stretch at 1638 & 1603 cm⁻¹, and strong C-O stretch between 1217–1044 cm⁻¹. The FTIR spectra of physical mixture -reveals stretching vibrations of 2941–2849 cm⁻¹ (C–H stretching), 2535 cm⁻¹ (O–H stretch, hydrogen-bonded), 1828 cm⁻¹ (C=O stretching), 1638 cm⁻¹ (C=C, aromatic), 1434 & 1383 cm⁻¹ (CH₂/CH₃ bending), 1222 & 1168 cm⁻¹ (C–O stretching). The occurrence of all peaks of drug in the physical mixture of AMD, cross-carmellose sodium and PVP K30 was evident of the compatibility of the drug and the polymers.
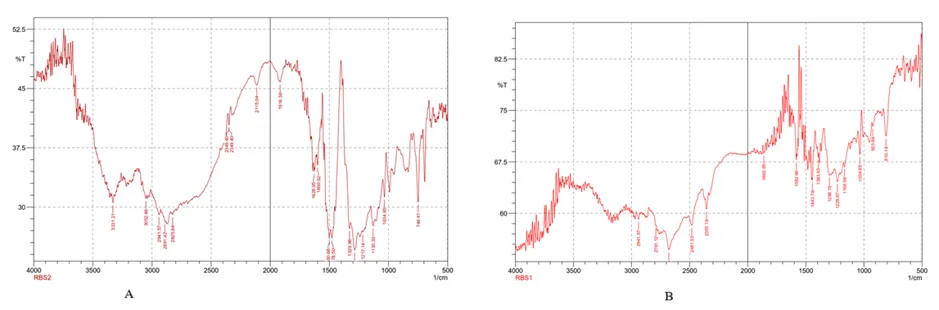
Figure 2. FTIR spectra of (A) AMD (B) Mixture of AMD and excipients
Evaluation of the hydrogel plug
The hydrogel plugs were prepared by direct compression of HPMC K15M and lactose using PVP K30 as the dry binder. The plug (tablets) was evaluated for weight variation, friability, thickness, shape and color. The swelling index of the hydrogel plug was also observed to confirm the integrity of the plug (Table 3). The plug was white in color, circular in shape with a thickness of 4.51 ± 0.013 mm, friability of 0.6-4% w/w and weight uniformity within ±10% w/w.
Table 3. Swelling property of hydrogel plug
|
pH |
Time (h) |
Initial wt |
Final wt |
% Swelling index |
|
1.2 |
2 |
0.202 |
0.287 |
29.62 |
|
4 |
0.202 |
0.411 |
50.85 |
|
|
6 |
0.202 |
0.485 |
58.35 |
|
|
8 |
0.202 |
0.601 |
66.39 |
|
|
10 |
0.202 |
0.697 |
71.02 |
|
|
12 |
0.202 |
0.804 |
74.88 |
|
|
7.4 |
2 |
0.203 |
0.291 |
30.24 |
|
4 |
0.203 |
0.423 |
52.01 |
|
|
6 |
0.203 |
0.501 |
59.48 |
|
|
8 |
0.203 |
0.618 |
67.15 |
|
|
10 |
0.203 |
0.713 |
71.53 |
|
|
12 |
0.203 |
0.822 |
75.30 |
|
|
6.8 |
2 |
0.202 |
0.285 |
29.12 |
|
4 |
0.202 |
0.406 |
50.25 |
|
|
6 |
0.202 |
0.481 |
58.00 |
|
|
8 |
0.202 |
0.591 |
65.82 |
|
|
10 |
0.202 |
0.704 |
71.31 |
|
|
12 |
0.202 |
0.794 |
74.56 |
The hydrogel plug was able to exhibit integrity for over 12 h of the swelling study along with sufficient swelling capacity.
Evaluation of amiodarone core tablets
The results of precompression studies make it evident that all the blends possessed the capability to flow freely and may present no hindrance in compression or tableting process. The values of Hausner’s ratio and Carr’s Index are found to be within the specifications of good flow property of powders (Table 4).
Table 4. Precompression parameters of core tablets
|
Formulation Code |
Bulk density (g/cm3) |
Tap density (g/cm3) |
Angle of repose (°) |
Carr's Index (%) |
Hausner's Ratio |
|
AC1 |
0.381 |
0.405 |
27°51' |
5.93 |
1.06 |
|
AC2 |
0.374 |
0.418 |
29°24' |
10.53 |
1.12 |
|
AC3 |
0.387 |
0.423 |
30°05' |
8.51 |
1.09 |
|
AC4 |
0.366 |
0.431 |
30°17' |
15.08 |
1.18 |
|
AC5 |
0.369 |
0.419 |
29°46' |
11.93 |
1.14 |
The tablets formulated after compression were evaluated for various quality control tests of solid dosage forms (tablets) in order to ensure that all the products meet the requirements of mouth dissolving tablets (Table 5).
Table 5. Post compression parameters of core tablets
|
Formulation Code |
Hardness (Kg/cm2) |
Thickness (mm) |
Average Weight variation (%) |
Friability (%) |
Drug content (%) |
|
AC1 |
3.8 |
4.56 |
4.6 |
0.61 |
96.75 |
|
AC2 |
4 |
4.57 |
5.3 |
0.56 |
97.30 |
|
AC3 |
3.9 |
4.53 |
3.8 |
0.53 |
98.10 |
|
AC4 |
3.8 |
4.55 |
4.1 |
0.50 |
97.80 |
|
AC5 |
3.9 |
4.52 |
2.7 |
0.55 |
98.10 |
The release of amiodarone from the core tablets was studied and it was found that 100% amiodarone was released in 90 min from the core (Figure 3).
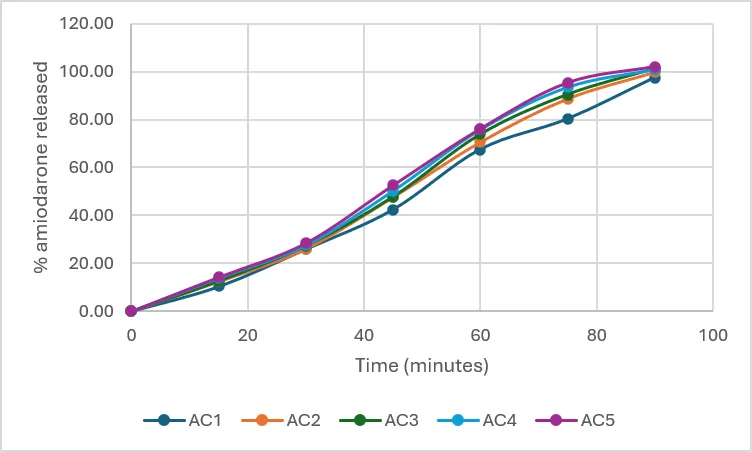
Figure 3. Cumulative release graph of amiodarone from core tablets
Evaluation of pulsincap
The release of amiodarone in various pH conditions according to the transit of the pulsincap was studied for a duration of 24h. It was found that in the acidic conditions of the stomach, about 60% of amiodarone was released in 2h whereas at pH7.4 none was released in 3h. At pH6.8 (colon), about 41% of the remaining drug was released in 19h of study (Figure 4) [18].
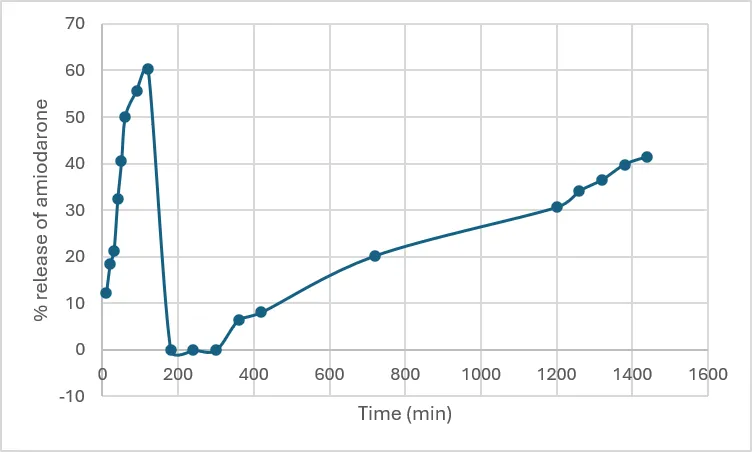
Figure 4. Release plot of amiodarone from pulsincap
The drug shows a burst release, reaching ~60% quickly. This suggests that a fraction of amiodarone is loosely bound or surface-associated with the carrier, dissolving rapidly in the medium. This was followed by drop in release to almost to baseline. This could indicate precipitation, recrystallization, or re-adsorption of the drug. Over time, the curve rises again, reaching ~40% by the end. This slow phase reflects controlled release from the matrix—likely diffusion through polysaccharide/nanoparticle networks or gradual erosion of the carrier.
CONCLUSION
The present work successfully demonstrated the formulation and evaluation of a pulsatile drug delivery system of amiodarone designed for chronotherapy of arrhythmia. Preformulation studies confirmed the physicochemical suitability of amiodarone and its compatibility with selected excipients. Hydrogel plugs prepared with HPMC K15M exhibited desirable swelling behavior and mechanical integrity, while core tablets showed excellent flow properties, uniform hardness, acceptable friability, and consistent drug content. The in vitro release profile confirmed complete drug release from the core within 90 minutes, ensuring rapid availability once the lag phase was overcome. Crosslinked gelatin capsules modified with formaldehyde vapors provided controlled release characteristics, with minimal drug release in acidic conditions and sustained release in intestinal pH environments. This design effectively mimics the circadian rhythm of arrhythmia, offering a promising chronotherapeutic approach. Overall, the pulsatile delivery system developed in this study demonstrates potential for improving therapeutic outcomes in arrhythmia management by synchronizing drug release with the body’s biological rhythms. Further in vivo studies and clinical evaluation are warranted to establish its efficacy and patient compliance.
REFERENCES

Azad Singh, Praveen Tahilani, Jitendra Banweer, Formulation and Evaluation of Pulsatile Delivery System of Amiodarone for Chronotherapy of Arrhythmia, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 944-952. https://doi.org/10.5281/zenodo.20532058
 10.5281/zenodo.20532058
10.5281/zenodo.20532058