
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Konkan Gyaanpeeth Rahul Dharkar College of Pharmacy And Research Institute
The advancement of oral drug delivery systems has been significantly influenced by modern scientific and technological developments, with the oral route remaining the most preferred due to its convenience and patient compliance. Among various oral dosage forms, medicated chewing gum has emerged as a promising and innovative drug delivery system. It offers both local and systemic drug delivery through the oral cavity while eliminating the need for water and enabling easy administration in diverse settings. Medicated chewing gums consist of an insoluble gum base composed of elastomers, emulsifiers, fillers, waxes, antioxidants, softeners, sweeteners, colouring, and flavouring agents, along with active pharmaceutical ingredients. Unlike conventional chewable tablets, these formulations are not intended to be swallowed and can be removed after use, providing controlled and sustained drug release through continuous mastication. Additionally, specially designed in vitro apparatuses have been developed to evaluate drug release from such systems. Their portability, non-invasive nature, and ability to deliver drugs without gastrointestinal degradation make them an attractive alternative to traditional dosage forms.Antifungal agents incorporated into chewing gum formulations belong to the Biopharmaceutics Classification System (BCS) Class II category, characterized by high permeability but poor aqueous solubility, which significantly limits their bioavailability and therapeutic efficacy. Conventional solubility enhancement techniques, including salt formation, particle size reduction, and encapsulation, have shown limited success due to their physicochemical limitations and pH-dependent solubility behaviour. Incorporating antifungal agents into medicated chewing gum formulations presents a novel approach to overcoming these challenges by facilitating drug release and absorption through the buccal mucosa. This review explores the formulation strategies, advantages, challenges, and potential of antifungal-loaded medicated chewing gums as an effective and patient-friendly drug delivery system.
Oral candidiasis is a common opportunistic fungal infection of the oral cavity caused predominantly by Candida albicans, a dimorphic yeast that normally exists as part of the healthy oral microflora. The condition was first described in 1838 by paediatrician François Veilleux. Under normal physiological conditions, Candida species coexist harmlessly within the oral environment; however, when the host’s immune defences are compromised or when the microbial balance is disturbed, the organism can transform from a commensal to a pathogenic state, leading to infection. [1, 2, 3]
The development of oral candidiasis is closely associated with immunosuppression, which may be either systemic or local in nature. Systemic predisposing factors include extremes of age, with neonates and elderly individuals being particularly susceptible due to immature or weakened immune systems. Immunocompromised conditions such as HIV/AIDS, diabetes mellitus, malignancies, and patients undergoing chemotherapy also exhibit a higher incidence of infection. In addition, prolonged use of systemic corticosteroids, broad-spectrum antibiotics, and immunosuppressive therapies significantly increases the risk of candidal overgrowth. Local immunosuppression is commonly seen in patients using inhaled corticosteroids for the management of asthma and chronic obstructive pulmonary disease, where deposition of the drug in the oral cavity alters local immunity and promotes fungal proliferation. [4]
Clinically, oral candidiasis presents in several forms, with acute pseudomembranous candidiasis (thrush) being the most frequently encountered type. However, multiple other clinical variants exist, reflecting the diverse pathogenic behaviour of Candida species. Lesions may appear as white or red plaques depending on the depth and nature of infection. White lesions include acute pseudomembranous candidiasis and chronic hyperplastic candidiasis, whereas erythematous or red lesions include acute and chronic erythematous candidiasis, angular cheilitis, median rhomboid glossitis, and generalized gingival erythema. In addition, less common forms such as cheilocandidiasis, chronic mucocutaneous candidiasis, and chronic multifocal candidiasis may also be observed, particularly in severely immunocompromised patients. [5]
The etiological spectrum of oral candidiasis is not limited to Candida albicans, although it remains the most predominant species responsible for more than 80% of cases. Other non-albicans species such as Candida glabrata, Candida tropicalis, Candida krusei, Candida parapsilosis, and Candida dubliniensis have also been increasingly reported, especially in patients with recurrent or resistant infections. These species often show varying degrees of resistance to conventional antifungal therapy, making treatment more challenging. [6]
Diagnosis of oral candidiasis is primarily clinical and is based on patient history, risk factor assessment, and characteristic clinical appearance of oral lesions. In most cases, a definitive diagnosis can be made through clinical examination alone. However, in atypical, recurrent, or treatment-resistant cases, additional investigations such as microbiological culture, smear examination, or biopsy may be required. Cultures are particularly useful when there is poor response to empirical antifungal therapy or when non-albicans species are suspected. [7]
The management of oral candidiasis depends on the severity and extent of infection. Mild cases are generally managed with topical antifungal agents such as nystatin, clotrimazole, miconazole, and amphotericin B lozenges, along with improved oral hygiene practices and elimination of predisposing factors. These agents act locally within the oral cavity and are effective in reducing fungal load without significant systemic absorption. In contrast, systemic antifungal therapy is reserved for moderate to severe infections, recurrent cases, or immunocompromised patients at high risk of dissemination. Common systemic agents include fluconazole, itraconazole alternatives such as voriconazole, posaconazole, and amphotericin B, which act by inhibiting ergosterol synthesis or disrupting fungal cell membrane integrity. [8]
Despite the availability of effective antifungal agents, treatment challenges persist due to drug resistance, poor patient compliance, and limited drug retention time in the oral cavity. These limitations highlight the need for novel drug delivery approaches that can enhance local drug concentration, improve residence time, and ensure sustained therapeutic action.
Medicated chewing gum has emerged as an innovative and patient-friendly oral drug delivery system. It offers several advantages, including ease of administration without water, enhanced local drug delivery through the oral mucosa, and improved patient compliance. Incorporation of antifungal agents into chewing gum systems allows for prolonged contact with the oral cavity, thereby improving therapeutic outcomes in oral candidiasis.[9]
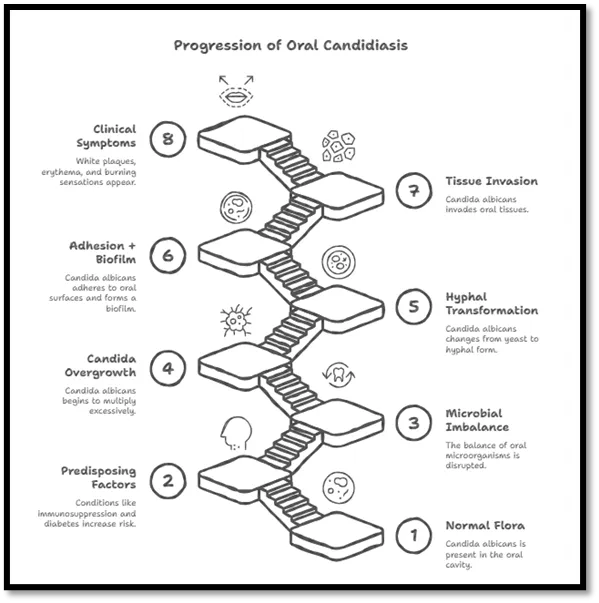
Figure 1: Pathogenesis of oral candidiasis
Etiology
Oral candidiasis is primarily caused by Candida species, with Candida albicans being the most frequently isolated organism, responsible for more than 80% of clinical cases. Candida albicans is a dimorphic fungus that exhibits both yeast and hyphal forms depending on environmental conditions. This morphological plasticity plays a key role in its pathogenicity, as the yeast form is associated with colonization, while the hyphal form is associated with tissue invasion and disease progression.
In addition to Candida albicans, several non-albicans species have also been implicated in oral candidiasis, particularly in recurrent or resistant infections. These include Candida glabrata, Candida tropicalis, Candida krusei, Candida guilliermondii, Candida lusitaniae, Candida parapsilosis, Candida pseudotropicalis, and Candida stellatoidea. Among these, non-albicans species are increasingly recognized in elderly patients and immunocompromised individuals, often showing reduced susceptibility to conventional antifungal agents, which complicates treatment outcomes. [10]
Candida species are considered normal commensals of the oral cavity in healthy individuals and are part of the resident oral microflora. Studies indicate that approximately 30–60% of healthy adults and 45–65% of infants may carry Candida species in the oral cavity without showing any signs of infection. In such cases, the organism exists in a balanced state with the host immune system and other microbial flora, remaining non-pathogenic under normal physiological conditions. [11]
However, oral candidiasis develops when this microbial balance is disrupted and Candida shifts from a harmless commensal organism to an opportunistic pathogen. This transition is influenced by several predisposing risk factors that promote fungal overgrowth and colonization. These include malnutrition, extremes of age (particularly neonates and elderly individuals), metabolic disorders such as diabetes mellitus, and immunocompromised conditions including HIV/AIDS, cancer chemotherapy, and organ transplantation. Additional contributing factors include concurrent infections, prolonged radiation therapy, long-term use of systemic corticosteroids or broad-spectrum antibiotics, and reduced salivary flow (xerostomia) due to salivary gland dysfunction or certain medications.
In immunocompromised states, the host’s reduced ability to control fungal proliferation allows Candida species to adhere more effectively to oral epithelial surfaces, form biofilms, and transition into invasive hyphal forms. This ultimately leads to tissue invasion and the clinical manifestation of oral candidiasis.
The etiology of oral candidiasis is multifactorial, involving the interaction between Candida species, host immune status, and local environmental conditions within the oral cavity. [12]
Pathology of Oral Candidiasis:
Oral candidiasis is caused substantially by Candida albicans, which typically exists as an inoffensive presence in the oral cavity. When prepping factors such as immunosuppression (e.g., HIV/ AIDS), metabolic diseases like Diabetes Mellitus, prolonged antibiotic or corticosteroid use, xerostomia, or denture wearing fracture the normal oral microbial equilibrium, Candida begins to multiply intolerably. It adheres to the oral epithelial cells through specific adhesins and forms biofilms, particularly on mucosal surfaces and dentures. Latterly, it undergoes a morphological metamorphosis from the non-invasive yeast form to the invasive hyphal or pseudo hyphal form, which enables penetration into the epithelial layers and illusion of host vulnerable defences. The organism again secretes hydrolytic enzymes like as proteases and phospholipases that degrade epithelial cell membranes, directing to tissue damage and desquamation. Although the host mounts an immune response, particularly cell- mediated immunity, this is frequently inadequate in compromised beings, allowing persisted fungal irruption. These pathological fluctuations eventually affect in the characteristic clinical features of oral candidiasis, including white curd-like plaques, erythematous lesions, and a burning sensation in the oral mucosa. [13]
Physicochemical Limitations of Antifungal Drug in Medicated Chewing Gum Formulation
1. Poor Aqueous Solubility
The antifungal drug belongs to the Biopharmaceutics Classification System (BCS) Class II category, which is characterized by low aqueous solubility and high permeability. Although it possesses good membrane permeability, its intrinsic solubility in water is extremely low, which significantly limits its dissolution in biological fluids. In medicated chewing gum formulations, saliva acts as the primary dissolution medium; however, due to the drug’s poor solubility at physiological salivary pH, only a limited amount of drug dissolves during mastication. This leads to incomplete drug release from the gum base, reduced availability at the buccal mucosa, and ultimately suboptimal therapeutic efficacy. Therefore, poor aqueous solubility remains a major formulation challenge in achieving effective drug release and therapeutic performance in medicated chewing gum systems. [14]
2. pH-Dependent Solubility
The antifungal drug exhibits pH-dependent solubility, with significantly higher solubility under acidic conditions and markedly reduced solubility at neutral to alkaline pH. Since saliva maintains a near-neutral pH range of approximately 6.5–7.5, the drug remains predominantly in an undissolved state within the oral cavity. This results in minimal dissolution during mastication, consequently leading to poor and inconsistent release from the dosage form. Furthermore, the reduced dissolution also limits the amount of drug available for absorption through the buccal mucosa, ultimately affecting the overall therapeutic performance of the medicated chewing gum formulation.
3. High Lipophilicity and Partitioning into Gum Base
The drug exhibits high lipophilicity, which results in a strong affinity for the hydrophobic components of the gum base, such as waxes and elastomers. Due to this interaction, the drug tends to remain retained within the gum matrix rather than efficiently partitioning into the aqueous salivary environment. Consequently, its diffusion into saliva is significantly reduced, leading to incomplete and inconsistent drug release during mastication, which may further compromise its overall bioavailability and therapeutic effectiveness. [15]
4. Poor Wettability
The drug exhibits poor wettability, which limits its effective interaction with saliva in the oral cavity. As a result, the drug particles tend to resist wetting and dispersion, leading to particle aggregation within the formulation. This aggregation further reduces the available surface area for dissolution, thereby slowing down the overall drug dissolution process. Consequently, the rate and extent of drug release from the medicated chewing gum are decreased, ultimately affecting its onset of action and therapeutic efficiency. [16]
5. Crystalline Nature and High Lattice Energy
The drug exists in a stable crystalline form characterized by strong intermolecular forces within its lattice structure. This high degree of crystallinity contributes to reduced molecular mobility and makes it more resistant to solubilisation. As a result, the drug exhibits slow dissolution in biological fluids, leading to delayed release from the gum matrix during mastication. Consequently, the rate and extent of drug absorption are reduced, ultimately resulting in decreased bioavailability and suboptimal therapeutic performance. [17]
6. Non -Ionisable Behaviour at Salivary pH
The drug remains largely in a non-ionized form at the physiological pH of saliva in the oral cavity. Since ionization plays a key role in enhancing aqueous solubility, the predominance of the non-ionized form results in poor solubility in saliva. This, in turn, leads to a reduced dissolution rate during mastication in medicated chewing gum formulations. Consequently, the limited dissolution restricts the amount of drug available for absorption through the buccal mucosa, thereby reducing its overall bioavailability and therapeutic effectiveness. [18]
7. Limited Diffusion from Gum Matrix
Drug release from medicated chewing gum is governed by mastication, which generates mechanical forces that gradually liberate the drug into saliva. However, in this case, the drug shows strong affinity toward the hydrophobic gum base and limited compatibility with the hydrophilic salivary environment. This results in poor migration of drug molecules from the matrix into the surrounding medium. Additionally, the high molecular interactions within the gum base further restrict drug mobility. As a consequence, diffusion becomes the rate-limiting step, leading to incomplete drug release, delayed onset of action, and reduced overall bioavailability.[19]
8. Dose Uniformity and Content Distribution Issues
The hydrophobic nature and poor solubility of the drug can lead to aggregation during mixing and processing stages. This aggregation prevents uniform dispersion of the drug throughout the gum base. As a result, some portions of the gum may contain higher drug concentrations while others contain less than the intended dose. Such non-uniform distribution can lead to dose variability between individual chewing gum units. This inconsistency directly affects therapeutic reliability and may result in sub therapeutic or fluctuating drug exposure in patients. [20]
9. Stability Concerns During Processing
Manufacturing of medicated chewing gum involves exposure to elevated temperatures, shear forces, and mechanical stress during mixing, kneading, and molding. These conditions may negatively impact the drug’s physicochemical stability. Potential risks include thermal degradation of the active compound, transformation into less stable polymorphic forms, or partial loss of crystallinity. Such changes may alter dissolution behaviour, reduce drug potency, and compromise batch-to-batch consistency. Therefore, careful control of processing conditions is essential to maintain drug stability. [21]
10. Bitter Taste and Patient Acceptability
The antifungal drug possesses an inherently bitter taste, which becomes more pronounced due to prolonged residence time in the oral cavity during chewing. Since medicated chewing gum remains in contact with taste buds for an extended duration, bitterness significantly affects patient acceptability. Poor palatability may reduce patient compliance, especially in long-term therapy. To overcome this limitation, taste-masking approaches such as the use of sweeteners (e.g., sucrose, mannitol, xylitol), flavouring agents (e.g., menthol, fruit flavors), and coating techniques (e.g., polymer or lipid coatings) are required to improve sensory acceptability.[22]
11. Limited Solubility in Salivary Volume
Saliva volume in the oral cavity is relatively small, typically around 1–2 mL at any given time. This limited volume creates a constrained dissolution environment for the drug. Due to poor aqueous solubility, the drug rapidly reaches saturation in saliva, leading to a plateau in dissolution. Once saturation is achieved, no further dissolution occurs, resulting in incomplete drug release. This limitation directly reduces the fraction of drug available for absorption and ultimately affects therapeutic efficiency. [23]
Table 1: Physicochemical Challenges and Solubility Enhancement Strategies for Antifungal Medicated Chewing Gum
|
Challenge |
Underlying Cause |
Impact on Formulation |
Solubility Enhancement Strategy |
Expected Outcome |
|
Poor aqueous solubility |
BCS Class II nature |
Incomplete dissolution in saliva |
Solid dispersion (PEG, PVP, HPMC) |
Increased dissolution rate |
|
pH-dependent solubility |
Low solubility at salivary pH (6.5–7.5) |
Reduced drug release |
pH modifiers (citric acid, tartaric acid) |
Improved ionization & solubility |
|
High lipophilicity |
Affinity for gum base (waxes, elastomers) |
Drug retention in matrix |
SEDDS / lipid-based systems |
Enhanced drug partitioning |
|
Poor wettability |
Hydrophobic surface of drug |
Slow dissolution |
Surfactants (Tween 80, SLS) |
Improved wetting & dispersion |
|
High crystallinity |
Strong lattice energy |
Slow drug dissolution |
Solid dispersion / nanoparticles |
Reduced crystallinity |
|
Non-ionized at salivary pH |
Weak ionization |
Low aqueous solubility |
pH modification / salt approach |
Increased solubility |
|
Limited salivary volume |
~1–2 mL saliva |
Rapid saturation |
Nanoparticles / nanosuspension |
Higher surface area & solubility |
|
Diffusion limitation |
Strong gum–drug interaction |
Incomplete drug release |
Cyclodextrin complexes |
Improved drug mobility |
|
Dose non-uniformity |
Drug aggregation |
Variable dosing |
Particle size reduction, proper mixing |
Uniform distribution |
|
Stability issues |
Heat & shear during processing |
Drug degradation |
Controlled processing / encapsulation |
Improved stability |
|
Bitter taste |
Intrinsic drug property |
Poor patient compliance |
Flavoring, sweeteners, coating |
Better palatability |
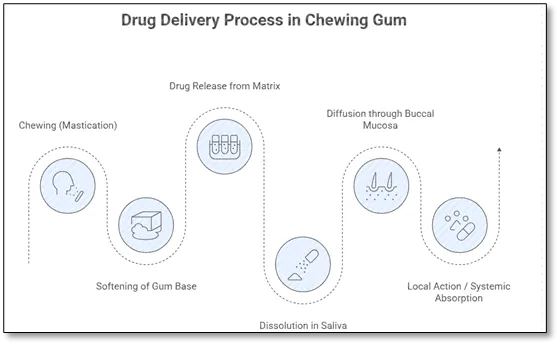
Figure 2: Mechanism of Drug Release from Chewing Gum [24]
3. Formulation Challenges of Antifungal Drug Medicated Chewing Gum
3.1 Drug–Excipient Compatibility Issues
The drug exhibits strong hydrophobic interactions with waxy and polymeric excipients used in gum formulation. These interactions may result in entrapment of drug particles within the gum base, preventing their efficient release into saliva. Incompatibility at the molecular level may also reduce drug availability and retard dissolution, making formulation optimization essential. [25]
3.2 Poor Drug Release from Gum Base
The hydrophobic gum base tends to retain the drug due to strong partitioning effects. As a result, drug molecules preferentially remain within the base rather than diffusing into the aqueous salivary medium. This leads to incomplete release during chewing, thereby reducing both local and systemic bioavailability. [26]
3.3 Polymer-Induced Release Retardation
Hydrophilic polymers such as HPMC and xanthan gum are often used to modify release behavior. Upon hydration, these polymers swell and form a viscous gel layer around the gum matrix. While this can help control release, excessive polymer concentration may significantly increase viscosity, creating a thick diffusion barrier. This barrier slows down drug migration and may lead to over-retarded or incomplete drug release. [27]
3.4 Texture and Chew ability Issues
The physical characteristics of chewing gum are highly dependent on excipient composition. Excess wax content can produce a hard and difficult-to-chew gum, whereas excessive plasticizers may result in a sticky and soft mass. Both extremes negatively affect patient experience and can reduce acceptability. Therefore, a precise balance of base materials, plasticizers, and fillers is essential to achieve optimal chew ability. [28]
3.5 Moisture Sensitivity and Stability
Certain excipients used in gum formulation are hygroscopic in nature and can absorb moisture from the environment. This may lead to changes in texture, microbial contamination risk, and reduced physical stability of the gum. Moisture uptake can also accelerate degradation of both drug and excipients, thereby affecting shelf life and product quality. [29]
3.6 Taste Masking Challenges
Due to the prolonged chewing time, complete taste masking becomes challenging. Although sweeteners and flavoring agents are incorporated, the bitter taste of the drug may still be perceived after initial masking effects diminish. This requires advanced taste-masking techniques such as microencapsulation, ion-exchange resins, or lipid coating systems to ensure sustained palatability. [30]
3.8 Mechanical Strength Issues
The mechanical properties of chewing gum must balance hardness, elasticity, and flexibility. Wax contributes to hardness, plasticizers provide flexibility, and fillers add structural integrity. An imbalance among these components can lead to either brittle gum that breaks easily or overly soft gum that loses structure during chewing. [31]
3.9 Stability with Volatile Components
Flavoring agents used in gum formulations are often volatile and prone to evaporation during processing and storage. Loss of these components over time reduces flavor intensity and overall product acceptability. Encapsulation or use of stabilizing matrices may be required to retain volatile compounds
3.10 Limited Drug Release in Saliva
The combination of limited salivary volume and poor aqueous solubility of the drug results in rapid saturation of the dissolution medium. Once saturation is reached, further dissolution is hindered, leading to incomplete drug release from the gum matrix. This significantly limits the amount of drug available for absorption and reduces therapeutic efficiency. [32]
4. Need for Solubility Enhancement of Antifungal Drug
4.1 Poor Aqueous Solubility
The antifungal drug exhibits extremely low solubility in aqueous media, which significantly limits its dissolution rate in biological fluids. Since dissolution is a prerequisite for absorption, poor solubility directly translates into reduced drug availability and suboptimal therapeutic efficacy, particularly in local delivery systems such as medicated chewing gum. [33]
4.2 Salivary Constraints
In the oral cavity, saliva is the primary dissolution medium; however, its limited volume (approximately 1–2 mL) and buffering capacity restrict the extent of drug dissolution. These physiological constraints make it difficult for poorly soluble drugs to achieve adequate concentration in saliva, thereby limiting release from the dosage form. [34]
4.3 pH Dependency
The drug demonstrates pH-dependent solubility, with higher solubility under acidic conditions and poor solubility at the near-neutral pH of saliva. As a result, in the oral environment, the drug remains largely undissolved, leading to reduced release and absorption. [35]
4.4 Lipophilic Retention
Due to its high lipophilicity, the drug shows strong affinity toward hydrophobic components of the gum base such as waxes and elastomers. This causes retention of drug molecules within the matrix, reducing their partitioning into saliva and limiting overall release. [36]
4.5 Poor Wettability
Poor wettability further reduces the interaction between drug particles and salivary fluid. This leads to inadequate dispersion of particles, decreased effective surface area for dissolution, and slower drug release kinetics.
4.6 Polymer Barrier Effect
Hydrophilic polymers used in gum formulations may swell upon hydration and form a viscous gel layer around the matrix. This gel barrier acts as a diffusion hindrance, slowing down drug migration into saliva and contributing to incomplete release. [37]
4.7 Need for Rapid Action
For the treatment of oral fungal infections, rapid onset of action is essential to reduce symptoms such as discomfort, burning sensation, and lesion progression. Poor solubility delays drug availability, making solubility enhancement critical for achieving faster therapeutic action. [38]
4.8 Drug Wastage
In poorly soluble systems, a significant fraction of the drug remains trapped within the gum base and is not released during mastication. This leads to inefficient drug utilization, increased formulation cost, and reduced therapeutic efficiency. [39]
4.9 Improved Buccal Absorption
Enhancing solubility improves the concentration gradient across the buccal membrane, which is the driving force for passive diffusion. This ultimately increases drug absorption through the oral mucosa, improving both local and systemic bioavailability. [40]
4.10 Patient Compliance
Improved solubility leads to better drug release, more consistent therapeutic action, and faster symptom relief. These factors collectively enhance patient satisfaction and compliance, which is particularly important in long-term antifungal therapy.
5. Solubility Enhancement Strategies
To overcome the inherent limitations of poor aqueous solubility and to improve the performance of medicated chewing gum formulations, several advanced formulation strategies can be employed. These approaches primarily aim to enhance drug dissolution, improve wettability, increase surface area, and promote better drug release in the salivary environment. [41]
5.1 Solid Dispersion Techniques
Solid dispersion involves dispersing the poorly soluble drug in a hydrophilic carrier matrix such as polyethylene glycol (PEG), polyvinylpyrrolidone (PVP), or hydroxypropyl methylcellulose (HPMC). In this system, the drug is molecularly dispersed or converted into an amorphous form, which significantly reduces crystallinity and improves thermodynamic stability in solution. The hydrophilic carrier enhances wettability and promotes faster penetration of saliva into the system, thereby increasing the dissolution rate. Additionally, the reduced particle size and increased surface area further contribute to improved drug release from the gum base. [42]
5.2 Cyclodextrin Inclusion Complexes
Cyclodextrins are cyclic oligosaccharides capable of forming host–guest inclusion complexes with lipophilic drug molecules. In this system, the hydrophobic portion of the drug is encapsulated within the hydrophobic cavity of cyclodextrin, while the hydrophilic outer surface interacts with aqueous media. This dual nature enhances the apparent solubility of the drug and improves its dispersion in saliva. Cyclodextrin complexation also protects the drug from degradation and can improve taste masking, making it particularly useful in oral formulations like medicated chewing gum. [43]
5.3Nanoparticles / Nanosuspensions
Nanotechnology-based approaches involve reducing the drug particle size to the nanometer scale using techniques such as high-pressure homogenization or precipitation methods. This drastic reduction in particle size leads to a significant increase in surface area, which enhances the dissolution rate according to the Noyes–Whitney equation. Nanoparticles also improve saturation solubility and dissolution velocity. In medicated chewing gum, nanosized drug particles disperse more uniformly within the gum matrix, ensuring faster and more complete release into saliva. [44]
5.4 Surfactants (e.g., Tween 80, SLS)
Surfactants such as polysorbate 80 (Tween 80) and sodium lauryl sulfate (SLS) play a key role in improving solubility and dissolution. They reduce interfacial tension between the hydrophobic drug particles and aqueous saliva, thereby enhancing wetting and dispersion. Surfactants also form micelles that can solubilize lipophilic drug molecules, increasing their apparent solubility. In chewing gum systems, they facilitate faster drug partitioning from the gum base into saliva, leading to improved release and absorption. [45]
5.5 pH Modification
pH modification involves the use of acidic or buffering agents such as citric acid, tartaric acid, or phosphates to create a localized microenvironment that favors drug solubility. For weakly basic drugs, lowering the pH in the immediate vicinity of the gum enhances ionization, which improves aqueous solubility and dissolution rate. In medicated chewing gum, this strategy is particularly useful because it compensates for the neutral pH of saliva and promotes faster drug release during mastication. [46]
5.6 Lipid-Based Systems (SEDDS)
Self-emulsifying drug delivery systems (SEDDS) are isotropic mixtures of oils, surfactants, and co-surfactants that spontaneously form fine oil-in-water emulsions upon contact with aqueous media such as saliva. This results in the formation of micro- or nano-sized droplets that significantly increase the surface area available for absorption. SEDDS enhance solubilization of lipophilic drugs and improve their diffusion from the gum matrix. In addition, they promote rapid drug release and may enhance buccal and systemic absorption by maintaining the drug in a solubilized state. [47]
6. Advantages of Medicated Chewing Gum
Medicated chewing gum offers several distinct advantages as an oral drug delivery system, making it particularly suitable for drugs intended for local as well as systemic action. One of the most important benefits is that it bypasses hepatic first-pass metabolism, as the drug absorbed through the buccal mucosa directly enters the systemic circulation. This enhances bioavailability, especially for drugs that are extensively metabolized in the liver. Additionally, it provides direct drug delivery to the oral mucosa, making it highly effective for treating local infections such as oral candidiasis, where a higher local drug concentration is required.[48]
The system also offers a faster onset of action compared to conventional oral dosage forms due to rapid absorption through the buccal lining. Since medicated chewing gum does not require water for administration, it is highly patient-friendly and convenient for use in daily life situations. It is particularly beneficial for paediatric and geriatric patients, who may have difficulty swallowing tablets or capsules. [49]
Furthermore, medicated chewing gum helps in reducing gastrointestinal degradation of drugs, as a portion of the drug is absorbed directly through the oral cavity, bypassing exposure to gastric fluids and enzymes. The system also allows sustained and controlled drug release during mastication, as drug release is gradually triggered by chewing activity, providing prolonged therapeutic action.
medicated chewing gum improves patient compliance when compared to conventional dosage forms such as tablets and lozenges, due to its ease of administration, better taste masking potential, and improved therapeutic effectiveness.[50]
7. Limitations of Medicated Chewing Gum
Despite its several advantages, medicated chewing gum also presents certain limitations that can restrict its broader application in drug delivery. One of the major drawbacks is its limited drug loading capacity, as the gum base can incorporate only a small amount of active pharmaceutical ingredient. This makes it unsuitable for drugs requiring high doses.
Taste masking is another significant challenge, especially for highly bitter drugs, since the drug remains in the oral cavity for an extended period during chewing. If not effectively masked, it can lead to poor patient acceptability and reduced compliance. In addition, there is a risk of dose variability due to differences in individual chewing habits, such as chewing intensity, duration, and frequency, which can directly influence the amount of drug released.
Stability issues are also a concern, particularly when volatile components such as flavoring agents are incorporated, as they may evaporate during processing or storage, affecting product quality. The manufacturing process of medicated chewing gum is relatively complex and requires specialized equipment and precise control of formulation parameters to ensure uniformity and consistency.
Furthermore, this dosage form is not suitable for drugs that require very high doses due to physical limitations of the gum matrix. Lastly, the gum base is sensitive to moisture, which can lead to changes in texture, microbial growth, and reduced shelf stability if proper packaging and storage conditions are not maintained. [51]
8. Mechanism of Drug Release from Chewing Gum
The mechanism of drug release from medicated chewing gum begins with mastication, which provides the mechanical force required for drug liberation. During chewing, the gum base softens and becomes hydrated due to continuous exposure to saliva, allowing the drug to gradually diffuse out of the matrix. This is followed by the disintegration of drug–gum interactions, resulting in the release of drug particles into the salivary fluid. The released drug then undergoes dissolution in saliva, although this step may be limited by factors such as low solubility, neutral pH, and restricted salivary volume. Once dissolved, the drug diffuses across the buccal mucosa and is absorbed through the oral epithelial lining. Finally, the absorbed drug may produce either a local therapeutic effect within the oral cavity or enter the systemic circulation, thereby bypassing first-pass hepatic metabolism and enhancing bioavailability. [ 52].
9. Evaluation Parameters of Medicated Chewing Gum
The evaluation of medicated chewing gum is essential to ensure its quality, performance, and therapeutic effectiveness. These parameters are broadly classified into physical, drug-related, and mechanical evaluations.
Physical Evaluation
Physical characterization includes assessment of weight variation, which ensures uniformity between individual gum units. Hardness and chewiness are evaluated to determine the ease of mastication and patient acceptability. Stickiness is also an important parameter, as excessive adhesiveness may affect handling and consumer compliance. Texture analysis is performed to assess the overall mouthfeel, elasticity, and consistency of the gum base. In addition, the swelling index is determined to evaluate the extent of hydration and expansion of the gum matrix upon contact with saliva, which directly influences drug release behavior.
Drug-Related Evaluation
Drug-related parameters include drug content uniformity, which ensures consistent dose distribution within each gum unit. In vitro drug release studies are conducted using specialized chewing apparatus to simulate mastication conditions and assess the release profile of the drug. Additionally, dissolution studies in simulated salivary fluid are performed to mimic the oral environment and evaluate the rate and extent of drug release under physiological conditions. [53]
Mechanical Evaluation
Mechanical properties are critical for determining the structural integrity and usability of chewing gum. Elasticity measures the ability of the gum to stretch and recover during chewing, while tensile strength assesses its resistance to breaking under applied force. These parameters ensure that the gum maintains its physical stability throughout mastication without disintegration or loss of functionality. [54]
10. In Vitro Drug Release Methods
In vitro drug release testing of medicated chewing gum is designed to simulate the physiological conditions of the oral cavity and mastication process. A modified chewing apparatus is commonly used, which replicates the mechanical action of chewing through compression and movement cycles. Alternatively, a modified USP dissolution apparatus may be employed with appropriate adaptations to accommodate the unique properties of chewing gum dosage forms. [55]
The study is typically conducted using simulated/artificial saliva as the dissolution medium, maintained at physiological conditions. The temperature is strictly controlled at 37 ± 0.5°C to mimic human body temperature. To closely replicate real chewing behavior, mastication simulation cycles are applied, involving repetitive compressive and shearing forces at defined intervals. These conditions together help in accurately evaluating drug release kinetics and predicting in vivo performance. [56]
11. Future Scope of Medicated Chewing Gum
The future development of medicated chewing gum holds significant potential for innovation in drug delivery systems. One of the emerging areas is the integration of nanotechnology-based chewing gums, which can enhance solubility, bioavailability, and controlled release profiles of poorly soluble drugs. Another promising direction is the development of targeted buccal drug delivery systems, designed to improve site-specific therapeutic action with minimal systemic side effects. [57]
There is also growing interest in combination antifungal therapy chewing gums, which can provide synergistic effects against resistant fungal strains and improve treatment outcomes. In addition, herbal antifungal chewing gum formulations are gaining attention due to their safety profile and reduced risk of adverse effects.
Future research may also focus on personalized medicine chewing gum systems, where drug dosage and formulation are tailored according to individual patient needs. Furthermore, the development of improved taste-masked, fast-dissolving chewing gums will enhance patient compliance, especially in pediatric and geriatric populations, making this dosage form more acceptable and widely applicable in modern therapeutics.
CONCLUSION
Medicated chewing gum represents a novel, patient-friendly, and effective oral drug delivery system that offers distinct advantages for both local and systemic therapy. Its ability to deliver drugs directly to the oral cavity, bypass first-pass metabolism, and improve patient compliance makes it particularly suitable for the management of oral candidiasis.
However, the incorporation of antifungal agents into this system is significantly challenged by their poor aqueous solubility, pH-dependent behavior, high lipophilicity, and limited release from the gum matrix. These physicochemical limitations result in incomplete drug release, reduced bioavailability, and variable therapeutic outcomes. Additionally, formulation-related challenges such as drug–excipient incompatibility, dose uniformity issues, stability concerns, and taste masking further complicate the development of effective medicated chewing gum systems.
To overcome these limitations, several solubility enhancement approaches such as solid dispersions, cyclodextrin inclusion complexes, nanosuspensions, surfactant systems, pH modification, and lipid-based drug delivery systems (SEDDS) have shown promising potential. These strategies significantly improve drug dissolution, wettability, and release in the salivary environment, thereby enhancing therapeutic efficacy.
In conclusion, antifungal-loaded medicated chewing gum holds strong potential as an innovative alternative to conventional dosage forms for the treatment of oral candidiasis. With further optimization in formulation technology, drug solubility enhancement, and taste-masking techniques, this system can emerge as a highly effective and commercially viable oral drug delivery platform in the future.
REFERENCES

Tejashree Misal, Suyog Mhatre, Mrunalini Mhatre, Rutika Nare, Prabodh Naik, Mukta Gochade, Formulation Development and Solubility Enhancement of Antifungal-Loaded Medicated Chewing Gum for the Management of Oral Candidiasis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6936-6953, https://doi.org/10.5281/zenodo.20396357
 10.5281/zenodo.20396357
10.5281/zenodo.20396357