
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy, Swami Vivekanand College of Pharmacy (SVCOP)Udgir, Latur, Maharashtra, India.
Oral Rehydration Solution (ORS) is a simple, safe, and effective therapy used for the treatment of dehydration caused by diarrhoeal diseases. It plays a vital role in reducing morbidity and mortality, especially in children. The effectiveness of ORS is based on the sodium-glucose co-transport mechanism, which enhances the absorption of water and electrolytes in the intestine. Standard WHO-recommended ORS contains sodium chloride, potassium chloride, trisodium citrate, and glucose in appropriate proportions. Over time, improved formulations such as low-osmolar ORS have been developed to increase efficacy. Clinical evidence suggests that low-osmolar ORS reduces stool output, vomiting, and the need for intravenous fluid therapy. Additionally, modified ORS formulations containing resistant starch have shown further benefits in reducing the duration of diarrhoea. These advancements have strengthened the role of ORS as the primary treatment for acute diarrhoeal conditions. Despite its effectiveness, several challenges are associated with ORS use, particularly regarding product quality and appropriate formulation selection. Studies have shown that many commercially available ORS products do not meet standard pharmacopeial requirements for electrolyte content, especially sodium and potassium levels. Such variations may reduce therapeutic effectiveness and pose risks to patients. Furthermore, the use of inappropriate formulations in specific conditions, such as cholera or severe malnutrition, may lead to complications like hyponatremia. Special formulations like Reseal are recommended for malnourished children to prevent electrolyte imbalance. Continuous quality control, post-market surveillance, and proper awareness among healthcare professionals are necessary to ensure safe and effective use. In conclusion, ORS remains a cost-effective, accessible, and life-saving intervention, but its optimal benefits depend on quality assurance and correct clinical application
1.1 Oral Rehydration Salts (ORS): -
Oral Rehydration Solution (ORS) was developed in the early 1970s as an effective method to treat dehydration caused by severe diarrhoea, particularly acute infectious diarrhoea. This condition leads to significant loss of fluids and electrolytes from the body, which can become life-threatening if not treated promptly. Although intravenous (IV) fluid therapy has been used for many years to manage dehydration, its use becomes difficult in situations where a large number of patients are affected, such as during outbreaks of diseases like cholera. In developing countries, especially in rural or emergency conditions, the availability of sterile IV fluids, proper sanitation, and electricity is often limited, making IV therapy less practical. To overcome these challenges, ORS was introduced as a simple, cost-effective, and easily administrable alternative. The original formulation of ORS consists of a balanced mixture of glucose and essential electrolytes, designed to match the osmolarity of body fluids (iso-osmolar solution). It also contains a base component, such as citrate, which helps in correcting metabolic acidosis along with dehydration.[7]
1.2 Development Of Oral Rehydration Salts (ORS): -
The development and widespread use of Oral Rehydration Solution (ORS) in the treatment of acute diarrhoea was influenced by three major scientific and practical events during the 1960s and 1970s. The first important discovery was related to the mechanism of absorption in the small intestine. It was found that glucose absorption requires the presence of sodium (Na⁺), and the absorption of sodium is significantly increased when glucose is present. This process occurs through a specific transporter known as SGLT1 (Sodium-Glucose Transporter 1), which plays a key role in the co-transport of glucose and sodium across the intestinal lining. This finding became the scientific basis for including both glucose and electrolytes in ORS. The second key observation came from studies on Cholera. Researchers found that the toxin produced during cholera infection increases the level of cyclic AMP in intestinal cells, leading to excessive secretion of fluids and electrolytes, which causes diarrhoea. However, it was also discovered that this toxin does not interfere with the absorption of sodium when glucose is present. This means that even during severe diarrhoea, the glucose-sodium absorption mechanism remains functional. Therefore, ORS can effectively promote the absorption of fluids and electrolytes despite ongoing fluid loss. The third and most significant event was the large-scale use of ORS during the Bangladesh Liberation War. During this period, ORS was widely used in refugee camps where outbreaks of diarrhoea and cholera were common.[7,8]
1.3 Composition of Oral Rehydration Salt ORS: -
prepared Oral Rehydration Salts (ORS) formulation consists of sodium chloride, potassium chloride, trisodium citrate dihydrate, dextrose anhydrous, and a small amount of zinc sulphate. Sodium chloride helps in restoring sodium and chloride ions, which are essential for maintaining fluid balance in the body. Potassium chloride provides potassium, which supports proper cellular and muscle function. Trisodium citrate dihydrate acts as an alkalizing agent and helps in correcting metabolic acidosis associated with dehydration. Dextrose anhydrous plays a vital role in enhancing sodium and water absorption through the sodium-glucose co-transport mechanism. The addition of zinc sulphate helps in reducing the duration and severity of diarrheal episodes and improves intestinal health. Overall, this formulation is designed to effectively manage dehydration and electrolyte imbalance.
Table 1: Composition Of Oral Rehydration Salts (ORS)
|
SR.NO |
COMPONENTS |
QUANTITY |
|
1. |
Sodium Chloride |
2.6 gm |
|
2. |
Potassium Chloride |
1.5 gm |
|
3. |
Trisodium Citrate Dihydrate |
2.9 gm |
|
4. |
Dextrose (Anhydrous) |
13.5gm |
|
5. |
Zinc Sulphate |
0.015 gm |
1.4 Composition of Marketed Oral Rehydration Salt (ORS): -
The marketed Oral Rehydration Salts (ORS) formulation contains sodium chloride, potassium chloride, sodium citrate, dextrose anhydrous, and excipients in sufficient quantity (qasr.). Sodium chloride helps in replenishing sodium and chloride ions, which are essential for maintaining fluid balance. Potassium chloride provides potassium required for proper cellular and muscle function. Sodium citrate acts as an alkalizing agent and helps in correcting metabolic acidosis during dehydration. Dextrose anhydrous enhances the absorption of sodium and water through the sodium-glucose co-transport mechanism.
The excipients present improve the stability, taste, and overall acceptability of the formulation. This composition makes the marketed ORS effective in managing dehydration and electrolyte imbalance.
Table 2: Composition of Marketed (ELECTRAL) Oral Rehydration Salts (ORS)
|
SR NO. |
COMPONENTS |
QUANTITY |
|
1. |
Sodium Chloride |
2.60gm |
|
2. |
Potassium Chloride |
1.50gm |
|
3. |
Sodium Citrate |
2.90gm |
|
4. |
Dextrose (anhydrase) |
13.50gm |
|
5. |
Excipients |
Q. S |
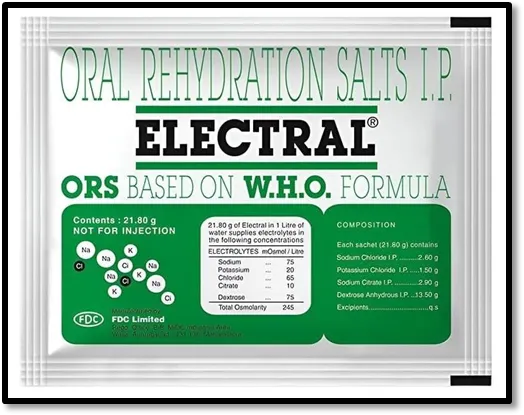
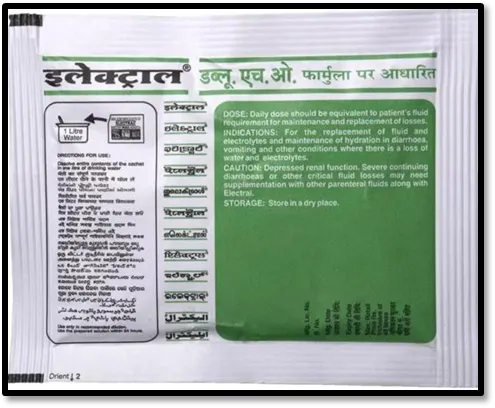
Fig .NO 1: - Marketed (ELECTRAL) Oral Rehydration Salts (ORS)
1.5 Mechanism Of Action of Oral Rehydration Salts (ORS): -
The mechanism of action of Oral Rehydration Salts (ORS) is based on the sodium-glucose co-transport system present in the small intestine. Glucose present in ORS facilitates the absorption of sodium through a specific transporter known as SGLT1 (Sodium-Glucose Transporter 1). When sodium is absorbed, water follows passively by osmotic movement, leading to effective rehydration of the body. This mechanism remains functional even during diarrheal conditions, where there is excessive loss of fluids and electrolytes. As a result, ORS helps in restoring fluid balance, correcting electrolyte imbalance, and preventing dehydration. Additionally, components like citrate help in correcting metabolic acidosis, further improving the patient’s condition.
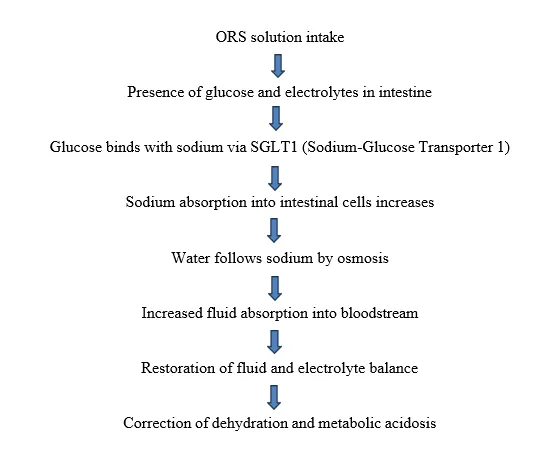
Mechanism Of Action of Oral Rehydration Salts (ORS)
1.6 Advantages: -
• Advantages of ORS (in detailed points):
• Prevents dehydration by replacing lost body fluids during diarrhoea, vomiting, and sweating.
• Restores electrolyte balance by supplying essential ions like sodium, potassium, and chloride.
• Easy to prepare by simply dissolving ORS powder in a specific amount of clean water.
• Cost-effective and affordable, making it suitable for use in all economic conditions.
• Reduces the need for intravenous (IV) fluids in mild to moderate dehydration cases.
• Safe for all age groups, including infants, children, adults, and elderly.
• Helps in faster recovery by maintaining proper hydration and energy levels.
• Prevents serious complications such as severe dehydration, shock, and death.
1.7 Application: -
• Treats acute diarrhoea in children and adults.
• Prevents dehydration due to vomiting.
• Replaces lost fluids and electrolytes.
• Useful in cholera patients.
• Helps in gastroenteritis recovery.
• Prevents heatstroke-related dehydration.
• Supports post-fever recovery.
• Maintains sodium and potassium balance.
• Reduces mortality from severe dehydration.
• Can be used in field and home settings due to easy preparation
2.REVIEW OF LITERATURE: -
1. David Nalin et.al (2021): -
Concerns about mild and temporary hypernatremia had previously led to the use of ORS formulations associated with a higher incidence of hyponatremia. Studies showed that hypernatremia complications were rare, whereas hyponatremia-related issues, including seizures, were more commonly reported. In severely dehydrated patients, the occurrence of hyponatraemic seizures was notable, indicating a significant clinical concern. It was observed that the effectiveness of low-sodium ORS varied depending on the type of diarrhoea, showing better outcomes in Cholera compared to non-cholera conditions. Alternative formulations containing rice or amino acids demonstrated improved efficacy in cholera by reducing the duration and severity of diarrhoea while maintaining electrolyte balance. However, in non-cholera cases, these benefits were limited. The studies suggested that further research was necessary to optimize ORS composition and ensure both safety and effectiveness, especially regarding electrolyte balance and prevention of complications.[2]
2. Sidra Tahir, et.al (2021): -
The incidence and requirement of unscheduled intravenous fluid therapy in children treated with low osmolar ORS is lower compared to those receiving standard ORS in the management of acute diarrhoea with some dehydration. Therefore, low osmolar ORS demonstrates better acceptance and effectiveness in the treatment of acute diarrhoea [3]
3. Rhondi Kauna, et.al (2019): -
The ORS tolerance test is a valuable tool to assess whether a child with gastroenteritis and moderate dehydration can be safely managed at home. Children who are able to consume at least 25 ml/kg of ORS without vomiting during an observation period of more than two hours are likely to respond well to home-based therapy. It is essential to identify children at higher risk of failure of oral rehydration therapy, including those with signs of severe dehydration, associated comorbidities such as malnutrition, or those who do not tolerate the ORS test. Home-based ORS therapy is considered safe only when appropriate criteria are followed, caregivers are adequately educated about ORS preparation and use, and proper clinical follow-up is ensured. The implementation of clear guidelines, risk assessment criteria, and dedicated ORS corners in emergency departments plays a crucial role in ensuring safe and effective management of children with diarrhoea and dehydration.[5]
4. Kirsty A. Houston, et.al (2014): -
Current WHO guidelines strongly recommend the use of Reseal, although this recommendation is based on low-quality evidence. Studies have reported a significant risk of hyponatraemia associated with Reseal in Asian children. However, no similar studies have been conducted in African populations, where the mortality rate due to severe acute malnutrition (SAM) remains high. Therefore, further research is necessary in Africa to determine the most appropriate ORS for children with SAM and to develop practical, evidence-based guidelines.[6]
5. Henry J. Binder et.al (2014): -
Oral rehydration therapy (ORT) has been developed over the past four decades and is now established as the standard treatment for dehydration and metabolic acidosis associated with acute diarrhoea. The widespread use of ORS has significantly contributed to the reduction in morbidity and mortality caused by acute infectious diarrhoea. However, despite its proven effectiveness, ORS is not utilized by mothers as widely as expected, leading to continuous efforts to improve its formulation. This review focuses on the incorporation of fermentable (resistant) starch into ORS. Such starch reaches the colon, where it is fermented to produce short-chain fatty acids (SCFAs), which in turn enhance sodium absorption through a cyclic AMP-independent mechanism. Consequently, these newly developed ORS formulations act as a “dual-action” system, promoting sodium and fluid absorption in both the small and large intestine.[7]
6. Norbert Hirschhorn et.al (2004): -
Studies conducted on reduced-osmolarity ORS for the treatment of non-cholera diarrhoea showed variable outcomes. The reduction in diarrhoea rate was minimal, and the duration of diarrhoea remained largely unchanged. Although a decrease in the need for intravenous fluids was reported, it was not strongly supported by laboratory evidence. The use of reduced-osmolarity ORS also increased the risk of hyponatremia, especially in adults with Cholera, without providing significant clinical benefit. In paediatric cholera cases, the findings were inconsistent. Therefore, further well-designed studies were required to determine the most suitable ORS formulation. Alternative solutions, such as those containing glucose with glycine or rice-based substrates, were found to be more effective in maintaining electrolyte balance and reducing complications.[8]
7. Hirschhorn N, et.al (2001): -
Treatment with reduced osmolarity ORS solution resulted in a significant 33% decrease in the requirement for unscheduled intravenous therapy. It showed no notable effect on stool output or duration of illness when compared to the standard WHO ORS solution. Therefore, reduced osmolarity ORS may provide beneficial outcomes in children suffering from acute diarrhoea. However, findings from studies evaluating the efficacy and safety of reduced osmolarity ORS in adult cholera patients should also be considered before establishing a final consensus on the composition of oral rehydration formulations.[9]
8. Dr. N. H Alam, et.al (1992): -
Studies showed that reduced osmolarity ORS solutions were safe and effective for children with acute non-cholera diarrhoea. These formulations, containing lower sodium and appropriate glucose levels, resulted in reduced stool output, less vomiting, and decreased need for intravenous fluid therapy compared to standard ORS. Solutions with sodium levels below 75 me/L showed slightly better improvement in reducing stool output and vomiting. However, both low-sodium and standard reduced osmolarity ORS showed similar effectiveness in reducing the requirement for IV therapy. In children suffering from Cholera, reduced osmolarity ORS was found to be equally effective as standard ORS and appeared to be safe, although further studies were recommended to confirm its long-term safety.[10]
3. NEED OF STUDY: -
Dehydration caused by diarrhoea, vomiting, and excessive fluid loss is a major public health problem, especially in developing countries like India. Oral Rehydration Solution (ORS) is a simple, effective, and economical therapy used to prevent and treat dehydration, working on the principle of sodium–glucose co-transport to enhance water and electrolyte absorption in the intestine. It is widely recommended by the World Health Organization (WHO) and used in both hospitals and community settings. However, marketed ORS formulations may differ in quality, stability, and palatability due to variations in raw materials, formulation methods, and storage conditions, which can affect their therapeutic effectiveness and patient compliance. Therefore, it is important to evaluate these formulations to ensure they meet standard requirements. The formulation and evaluation of ORS in the laboratory help in understanding pharmaceutical principles and quality control parameters such as PH, osmolarity, clarity, taste, and stability. This study aims to formulate and compare laboratory-prepared ORS with marketed products to ensure quality, safety, efficacy, and patient acceptability, while also enhancing practical knowledge in pharmaceutical formulation and evaluation.
4. AIM AND OBJECTIVE: -
4.1 Aim: -
To formulate, evaluate, and perform a comparative study of Oral Rehydration Salt (ORS) with standard marketed formulations.
4.2 Objectives: -
• To formulate Oral Rehydration Salt (ORS) using standard ingredients such as sodium chloride, potassium chloride, trisodium citrate, and Dextrose as per recommended guidelines.
• To evaluate the prepared ORS for physicochemical parameters including PH, solubility, osmolarity, and palatability.
• . To compare the formulated ORS with marketed ORS in terms of composition, osmolarity, dissolution characteristics, and stability.
• . To assess the quality and uniformity of the prepared ORS formulation.
• To study the stability of the formulation under different storage conditions.
• To evaluate the effectiveness and acceptability of the prepared ORS based on standard parameters.
• . To develop an improved ORS formulation with better patient compliance, such as enhanced taste, or packaging.
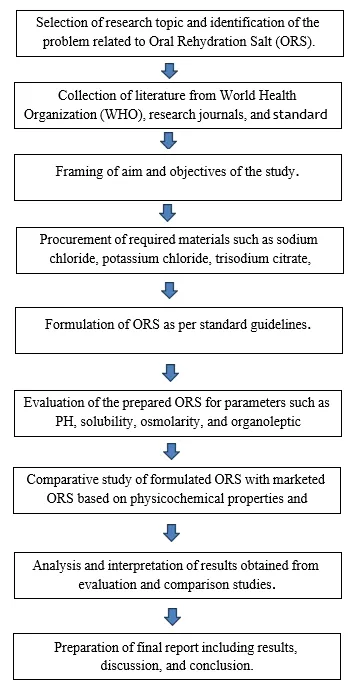
5. PLAN OF WORK: -
6. MATERIAL AND METHODOLOGY:
Table 3: - Materials Name with Molecular Formula, Molecular Weight and Brand Name
|
SR.NO |
DRUG PROFILE |
MOLECULAR FORMULA |
MOLECULAR WEIGHT |
BRAND NAME |
|
1. |
Sodium Chloride |
NaCl |
58.44g/mol |
RLS Chemicals |
|
2. |
Potassium Chloride |
KCL |
74.55g/mol |
SRL Chemicals |
|
3. |
Trisodium Citrate Dehydrate |
C6H5Na3O7`2H2O |
294.10g/mol |
AR Chemicals |
|
4. |
Dextrose (anhydrous) |
C6H12O6 |
180.16g/mol |
NICE Chemicals |
|
5. |
Zinc Sulphate |
ZnSO4 |
161.47g/mol |
AMICHEM LAB |
6.1 Material: -
• Drug Profile: -
I. Sodium Chloride
II. Potassium Chloride
III. Trisodium Citrate Dehydrate
IV. Dextrose(anhydrous)
V. Zinc Sulphate
1. Sodium Chloride: -
Sodium Chloride is one of the essential components used in the formulation of Oral Rehydration Salts (ORS). It plays a crucial role in maintaining electrolyte balance and preventing dehydration. It is commonly known as table salt and is widely used in pharmaceutical preparations for its ability to replenish sodium and chloride ions lost during conditions such as diarrhoea and vomiting.
Sodium chloride is a white, crystalline, doorless compound with a characteristic salty taste. In ORS formulations, it helps restore extracellular fluid volume and supports proper nerve and muscle function. It also aids in glucose absorption in the intestine through the sodium-glucose co-transport mechanism, which is vital for effective rehydration.
• Scientific Classification
1. Chemical Name: Sodium Chloride
2. Molecular Formula: NaCl
3. Molecular Weight: 58.44 g/mol
• Category
1. Electrolyte replenisher
2. Rehydrating agent
• Description
1. White crystalline powder
2. Odourless
3. Salty taste
4. Freely soluble in water
• Role in ORS
1. Maintains osmotic balance
2. Replaces sodium loss during diarrhoea
3. Enhances water and glucose absorption in intestines
• Uses
1. Treatment of dehydration
2. Used in Oral Rehydration Therapy (ORT)
3. Maintains fluid and electrolyte balance
• Storage
1. Store in a well-closed container
2. Protect from moisture
• Safety
Sodium chloride is generally safe when used in recommended quantities. However, excessive intake may lead to electrolyte imbalance or increased blood pressure.
Fig.No:-2 Structure of Sodium Chloride
Fig.No:-3 Sodium Chloride Compound
2. Potassium Chloride :-
Potassium chloride is an essential inorganic compound widely used in pharmaceutical preparations, particularly in Oral Rehydration Salts (ORS). It acts as a major source of potassium ions required for maintaining normal cellular functions. During conditions like diarrhoea and dehydration, the body loses significant amounts of potassium, and potassium chloride helps in restoring this loss.
It is a white crystalline substance, doorless, and has a saline taste. It is highly soluble in water, making it suitable for oral formulations. Potassium plays a crucial role in maintaining intracellular fluid balance, nerve conduction, and muscle contraction, especially the proper functioning of the heart.
• Scientific Classification: -
1. Chemical Name: Potassium Chloride
2. Molecular Formula: KCI
3. Molecular Weight: 74.55 g/mol
• Category: -
1. Electrolyte
2. Rehydrating agent
• Description
1. White crystalline powder
2. Odourless
3. Saline taste
4. Freely soluble in water
• Role in ORS
1. Replaces potassium lost during diarrhoea and dehydration
2. Maintains intracellular fluid balance
3. Supports nerve transmission and muscle contraction
4. Helps in proper functioning of heart muscles
• Uses
1.Used in Oral Rehydration Salts (ORS) 2.Treatment and prevention of hypokalaemia 3.Maintains electrolyte balance in the body
• Storage
1. Store in a well-closed container
2. Protect from moisture and humidity
• Safety
Potassium chloride is safe when used in recommended quantities. Excessive intake may lead to hyperkalaemia, which can cause serious cardiac complications
Fig.No :-4 Structure of Potassium chloride

Fig. No:- 5 Potassium chloride Compound
3. Trisodium Citrate Dihydrate
Trisodium citrate dihydrate is an important pharmaceutical compound used in Oral Rehydration Salts (ORS) formulations. It acts as an alkalinizing agent and helps in correcting metabolic acidosis, which commonly occurs during severe diarrhoea and dehydration. It also enhances the stability and effectiveness of ORS solutions.
It appears as a white crystalline powder, doorless, and has a slightly saline taste. It is highly soluble in water and contributes to maintaining the acid-base balance in the body. In ORS, it plays a vital role in improving electrolyte absorption and overall rehydration efficiency.
• Scientific Classification
1. Chemical Name: Trisodium Citrate Dihydrate
2. Molecular Formula: C₆H₅Na₃O₇·2H₂O
3. Molecular Weight: 294.10 g/mol
• Category
1. Alkalinizing agent
2. Electrolyte stabilizer
• Description
1. White crystalline powder
2. Odourless
3. Slightly saline taste
4. Freely soluble in water
• Role in ORS
1. Helps correct metabolic acidosis
2. Maintains acid-base balance
3. Improves electrolyte absorption
4. Enhances stability of ORS formulation
• Uses
1. Used in Oral Rehydration Salts (ORS)
2. Treatment of acidosis
3. Buffering agent in pharmaceutical formulations
• Storage
1. Store in a well-closed container
2. Protect from moisture
• Safety
Trisodium citrate dihydrate is generally safe when used in recommended quantities. Excessive use may lead to alkalosis or electrolyte imbalance.
Fig.no 06: - Structure of Trisodium Citrate Dihydrate

Fig. No : - 7 Trisodium Citrate Dihydrate Compound
4. Dextrose Anhydrous
Dextrose anhydrous is a purified form of glucose widely used in pharmaceutical formulations, especially in Oral Rehydration Salts (ORS). It plays a crucial role in promoting rapid absorption of water and electrolytes in the intestine through the sodium-glucose co-transport mechanism. This makes it an essential component in the treatment of dehydration caused by diarrhoea.
Dextrose anhydrous appears as a white crystalline powder with a sweet taste and is freely soluble in water. It provides a quick source of energy and enhances the effectiveness of ORS by facilitating sodium and water uptake in the intestinal tract.
• Scientific Classification
1. Chemical Name: Dextrose Anhydrous (D-Glucose)
2. Molecular Formula: C₆H₁₂O₆
3. Molecular Weight: 180.16 g/mol
• Category
1. Carbohydrate
2. Energy source
• Description
1. White crystalline powder
2. Odourless
3. Sweet taste
4. Freely soluble in water
• Role in ORS
1. Enhances sodium and water absorption
2. Provides instant energy
3. Facilitates electrolyte transport in intestine
4. Improves overall rehydration efficiency
• Uses
1. Used in Oral Rehydration Salts (ORS)
2. Energy source in pharmaceutical preparations
3. Treatment of dehydration and hypoglycaemia
• Storage
1. Store in a well-closed container
2. Protect from moisture and heat
• Safety
Dextrose anhydrous is generally safe when used in recommended amounts. Excess intake may lead to hyperglycaemia, especially in diabetic patients.
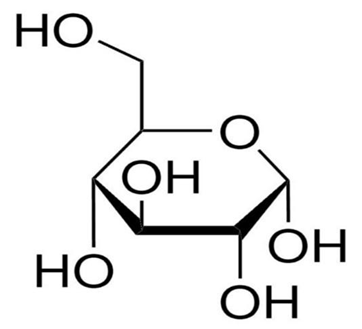
Fig.no 08: - Structure of Dextrose Anhydrous
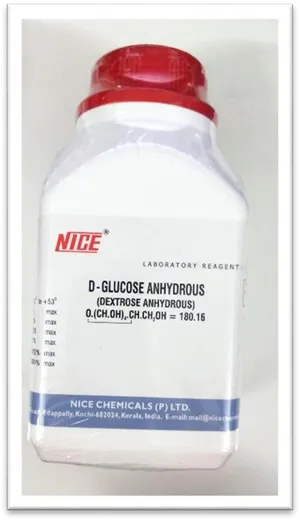
Fig.no 09: - Dextrose Anhydrous Compound
5. Zinc Sulphate
Zinc sulphate is an important mineral supplement used in pharmaceutical formulations, especially in Oral Rehydration Salts (ORS). It plays a significant role in reducing the severity and duration of diarrhoea and helps in faster recovery of the intestinal lining.
Zinc sulphate appears as a white crystalline powder, doorless, and has an astringent taste. It is highly soluble in water. In ORS formulations, zinc helps in improving immune function, enhancing intestinal absorption, and reducing the recurrence of diarrheal episodes, especially in children.
• Scientific Classification
1. Chemical Name: Zinc Sulphate
2. Molecular Formula: ZnSO₄
3. Molecular Weight: 161.47 g/mol
• Category
1. Mineral supplement
2. Antidiarrheal agent
• Description
1. White crystalline powder
2. Odourless
3. Astringent taste
4. Freely soluble in water
• Role in ORS
1. Reduces duration and severity of diarrhoea
2. Enhances immune response
3. Promotes intestinal healing
4. Decreases recurrence of diarrhoea
• Uses
1. Used in Oral Rehydration Salts (ORS)
2. Treatment of zinc deficiency
3. Management of acute diarrhoea
• Storage
1. Store in a well-closed container
2. Protect from moisture
• Safety
Zinc sulphate is safe when used in recommended doses. Excessive intake may cause nausea, vomiting, or gastric irritation.
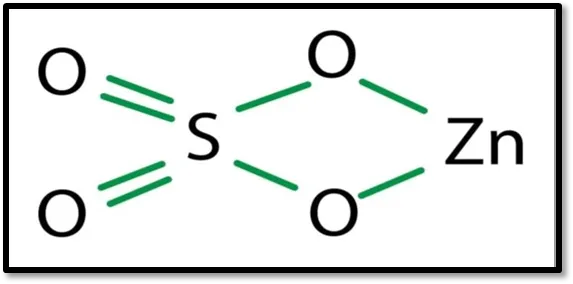
Fig.no 10: - Structure of Zinc Sulphate

Fig.no 11: - Zinc Sulphate Compound
6.2 Methodology: -
Formulation of Oral Rehydration Salts (ORS):
Different Oral Rehydration Salt (ORS) formulations were prepared using standard procedures. The selection of ingredients was done based on their ability to restore electrolyte balance, improve hydration, and enhance palatability. The formulation includes essential electrolytes and glucose which are required for effective oral rehydration therapy.
Accurately weighed quantities of each ingredient such as sodium chloride, potassium chloride, trisodium citrate dihydrate, dextrose anhydrous, and zinc sulphate were taken. All the ingredients were mixed thoroughly using mortar and pestle to obtain a uniform powder mixture.
The prepared mixture was then dissolved in a specified quantity of distilled water with continuous stirring to ensure complete solubility. The final solution was made up to the required volume using distilled water. The prepared ORS solution was then transferred into a clean, dry, and well-closed container.
FLOW CHART OF METHOD OF ORAL REHYDRATION SALT (ORS)
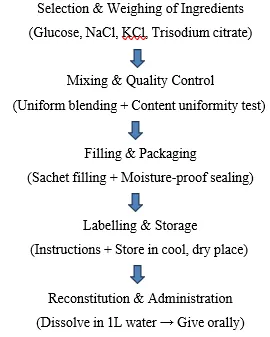
Procedure For Oral Rehydration Salt (ORS): -
Firstly, take all the required apparatus and clean them properly. Then take the required ingredients such as glucose, sodium chloride, potassium chloride, and trisodium citrate as per the formula. Weigh all the ingredients accurately using a weighing balance. After that, transfer all the weighed powders into a clean and dry mortar or mixing vessel. Mix the powders thoroughly to obtain a uniform mixture. Then check the mixture for uniformity. After proper mixing, fill the prepared ORS powder into sachets in accurate quantities. Seal the sachets properly to prevent moisture entry and label them with necessary instructions. Store the prepared ORS sachets in a cool and dry place. When required, dissolve one sachet in the specified quantity of clean water (usually 1 litter) and administer orally.
Table No 4: - Formulation For Oral Rehydration Salts (ORS)
|
SR.NO |
COMPONENTS |
QUANTITY |
USES |
|
1 |
Sodium Chloride |
2.6gm |
restores lost sodium and helps water absorption. |
|
2 |
Potassium Chloride |
1.5gm |
Replaces potassium, prevents deficiency |
|
3 |
Trisodium Citrate Dehydrate |
2.9gm |
Corrects acidosis, maintains pH |
|
4 |
Dextrose (anhydrous) |
13.5gm |
Provides energy, aids absorption |
|
5 |
Zinc Sulphate |
0.015gm |
Reduces diarrhoea, boosts immunity |
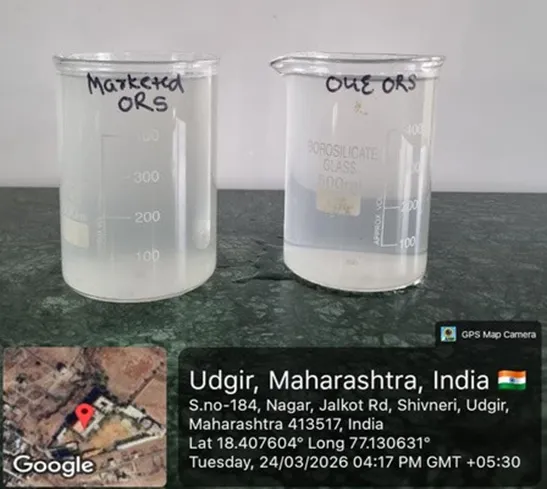
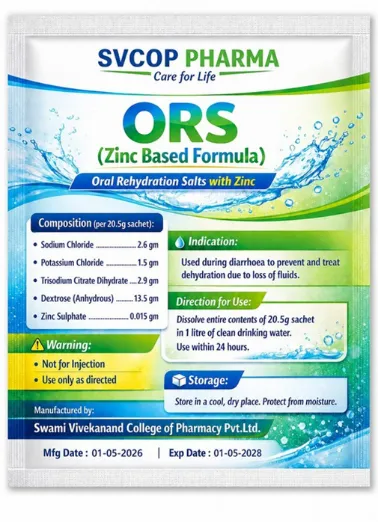
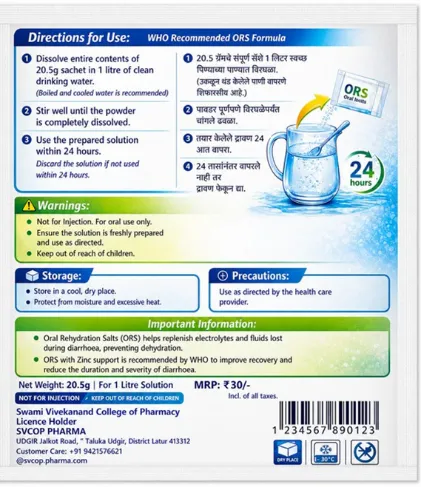
Fig. No 12: - Formulated Oral Rehydration Salts(ORS)
8. EVALUATION TEST: -
8.1 Physical Appearance and Clarity Test
8.2 PH Determination Test
a. Using Digital PH Meter
b. Using PH Paper
8.3 Stability Studies
8.4 Taste and palatability Test
8.5 Solubility Test
8.1 Physical Appearance and Clarity Test: -
a. The physical parameters such as colour, odour, and clarity were examined by visual inspection.
b. The prepared ORS solution was checked for transparency and absence of suspended particles.
8.2 PH Determination Test: -
PH Determination is an important evaluation parameter for ORS to ensure stability, compatibility, and patient acceptability.
The PH of ORS solution should be near neutral to avoid irritation of the gastrointestinal tract and to maintain electrolyte balance.
a. Using digital PH Meter (Accurate Method): -
The PH of the prepared ORS solution was measured using a calibrated digital pH meter. The instrument was standardized using buffer solutions before use.
The electrode was dipped in the solution and reading was noted.
b. Using PH Paper: -
A strip of PH paper was immersed in the ORS solution. The colour change was compared with the standard chart.
8.3 Stability Studies: -
a. The prepared ORS powder/solution was stored at room temperature and elevated Temperature 40 Celsius
b. Samples were observed for changes in colour, clarity, PH, and overall appearance over a period of time.
8.4 Taste and Palatability Test: -
The prepared ORS solution was evaluated for taste and acceptability
8.5 Solubility Test: -
a. ORS powder was added to 1 litter of water and stirred properly.
b. Time taken for complete dissolution was noted.
RESULT AND DISCUSSION
The prepared Oral Rehydration Salt (ORS) formulation was evaluated using various parameters such as physical appearance, PH, Stability, Osmolality, Taste and Palatability, and Solubility.
1. Physical Appearance and Clarity: -
The physical appearance and clarity of the prepared ORS formulation were evaluated by visual inspection. The solution was prepared using distilled water and observed under standard lighting conditions for colour, transparency, and presence of any particulate matter.
Table No 5: - Physical Appearance and Clarity
|
SR.NO |
EVALUATION PARAMETER |
MARKETED ORS |
PREPARED ORS |
RESULT |
|
1 |
Colour |
Colourless |
Colourless |
Pass |
|
2 |
Odour |
Odourless |
Odourless |
Pass |
|
3 |
Taste |
Slightly salty sweet |
Slightly salty sweet |
Pass |
|
4 |
Clarity |
Clear |
Clear |
Pass |
|
5 |
Transparancy |
Transparant |
Transparant |
Pass |
|
6 |
Turbidity |
Absent |
Absent |
Pass |
|
7 |
Suspected particles |
Absent |
Absent |
Pass |


Fig.no 13: - Physical Appearance and Clarity of ORS
2. PH Determination Test: -
The pH of the prepared ORS formulation was determined using a digital PH meter and PH paper. The solution was prepared in distilled water and measured under standard conditions.
A. By using Digital PH Meter: -
The PH of the prepared ORS solution was determined using a calibrated digital pH meter. The electrode was immersed in the solution and the reading was recorded. The measurement was carried out at room temperature.
Result: -
Table No 6: -PH Meter
|
SR.NO |
EVALUATION TEST |
MARKETED ORS |
PREPARED ORS |
RESULT |
|
1. |
PH (Digital) |
7.26 |
7.29 |
Pass |


Fig.no 14: - PH Meter of ORS
B. By using PH paper: -
The PH of the ORS solution was determined using PH paper. A strip was dipped into the solution and the colour change was compared with the standard colour chart to obtain the PH value.
Result: -
Table NO 7: -PH Paper
|
SR.NO |
EVALUATION TEST |
MARKETED ORS |
PREPARED ORS |
RESULT |
|
1. |
PH paper |
Basic (Alkaline in Nature) |
Basic (Alkaline in Nature) |
Pass |
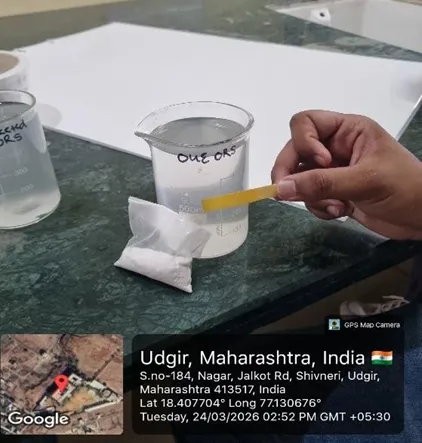

Fig.no 15: - PH Paper of ORS
3. Stability Studies: -
The stability of the prepared ORS formulation was evaluated by observing changes in colour, Odor, texture, and pH over a period of time.
Result: -
Table No 8: - Stability Studies
|
SR. NO |
PARAMETER |
PREPARED ORS |
MARKETED ORS |
OBSERVATION |
|
1. |
Colour |
Colourless clear |
Colourless clear |
No difference |
|
2. |
Odour |
Odourless |
Odourless |
No difference |
|
3. |
Taste |
Slightly sweeter |
Salty |
Comparable |
|
4. |
Clarity |
Clear solution |
Clear solution |
No difference |
|
5. |
PH |
7.0-7.5 |
7.2-7.6 |
Within Acceptable range |


Fig.no 16: - Stability Studies of ORS
4. Taste and Palatability Test: -
The taste and palatability of the prepared ORS solution were evaluated by sensory method. The solution was observed for sweetness, saltiness, and overall acceptability and compared with marketed ORS.
Result: -
Table No 9: - Taste and Palatability Test
|
SR NO |
TEST |
MARKETED ORS |
PREPARED ORS |
RESULT |
|
1. |
Taste |
Sweet and salty |
Slightly salty less sweet |
Acceptable |
6.Solubility Test: -
The solubility of the prepared ORS formulation was evaluated by dissolving the specified quantity in water. The solution was observed for complete dissolution and clarity.
Result: -
Table No 10: - Solubility Test
|
SR.NO |
EVALUATION TEST |
MARKETED ORS |
PREPARED ORS |
RESULT |
|
1. |
Solubility |
Completely soluble |
Completely soluble |
Clear solution no residue |
|
2. |
Time taken to dissolve |
44.57 Second |
55.02 Second |
Clear solution no residue |
CONCLUSION
The Oral Rehydration Salts (ORS) formulation containing zinc was successfully prepared using standard pharmaceutical ingredients such as sodium chloride, potassium chloride, trisodium citrate dihydrate, dextrose and zinc sulphate. The formulation process was carried out carefully to ensure proper mixing and uniformity of all components. The prepared ORS was subjected to various evaluation tests and the results obtained were found to be within acceptable limits. The PH of the prepared ORS solution was found to be near neutral and comparable with that of the marketed ORS, indicating its suitability for oral administration and its non-irritant nature to the gastrointestinal tract. The comparative study between the prepared ORS and marketed ORS showed that there was no significant difference in the observed parameters, which confirms the effectiveness of the prepared formulation. The physical characteristics such as colour, odour and clarity were found to be satisfactory and similar to the marketed product. The stability study indicated that the formulation remained stable under different storage conditions without any significant change in its properties. The presence of zinc sulphate in the formulation provides additional therapeutic advantage in reducing the severity and duration of diarrhoea. The formulation also helps in restoring electrolyte balance and preventing dehydration effectively. The overall results of the study demonstrate that the prepared ORS formulation is reliable and meets the standard requirements. Hence, it can be concluded that the prepared ORS is safe, effective and comparable to the marketed ORS formulation for the management of dehydration caused due to diarrhoea.
REFERENCES
Yugoslavia: Savremena Administracija; 1973:1048-1057.
Yugoslavia: Savremena Administracija; 1973:1048-1057.
Belkone Vishwajeet, Bansode Supriya, Achintalwar Nikita, Bagawe Shreyash, Alat Vaishnavi, Maheshwar Mukta, Formulation and Evaluation, and Comparative Study of Oral Rehydration Salts (ORS), Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 724-743, https://doi.org/10.5281/zenodo.21157923
 10.5281/zenodo.21157923
10.5281/zenodo.21157923