
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
¹ DCS's A.R.A College of Pharmacy, Nagaon, Dhule.
2 NES’s Gangamai College of Pharmacy, Nagaon, Dhule
Diabetes mellitus is a chronic metabolic disorder characterized by elevated blood glucose levels and remains a major global health concern. Several widely used oral antidiabetic drugs, including glibenclamide, glimepiride, pioglitazone, and repaglinide, belong to the Biopharmaceutics Classification System (BCS) Class-II category, exhibiting low aqueous solubility and high permeability. Poor solubility limits drug dissolution and absorption, resulting in reduced and variable oral bioavailability. To overcome these challenges, various formulation strategies have been developed, including micronization, nanonization, solid dispersions, and crystal engineering. Advanced drug delivery systems such as self-emulsifying drug delivery systems (SEDDS), self-nanoemulsifying drug delivery systems (SNEDDS), nanoemulsions, solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), polymeric nanoparticles, and nanosuspensions have shown significant potential in enhancing solubility and bioavailability. Recent studies demonstrate that lipid-based and nanotechnology-driven formulations improve pharmacokinetic performance and therapeutic efficacy. Future advancements involving Quality by Design (QbD), artificial intelligence, and multifunctional nanocarriers may further optimize antidiabetic drug delivery and treatment outcomes.
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both. It represents one of the most significant public health challenges worldwide due to its increasing prevalence and associated complications (International Diabetes Federation [IDF], 2021). According to the IDF Diabetes Atlas, approximately 537 million adults aged 20–79 years were living with diabetes in 2021, and this number is projected to increase to 643 million by 2030 and 783 million by 2045 (IDF, 2021).
Type 2 diabetes mellitus (T2DM) accounts for nearly 90–95% of all diabetes cases and is closely associated with obesity, sedentary lifestyle, unhealthy dietary habits, and aging populations (American Diabetes Association [ADA], 2024). The disease is associated with various microvascular and macrovascular complications, including diabetic nephropathy, retinopathy, neuropathy, coronary artery disease, and stroke, leading to substantial morbidity and mortality worldwide (Forbes & Cooper, 2013).
Oral antidiabetic therapy remains the first-line treatment for most patients with T2DM due to its convenience, cost-effectiveness, and improved patient compliance (ADA, 2024). However, the therapeutic effectiveness of several oral antidiabetic agents is often compromised by poor aqueous solubility and low oral bioavailability, necessitating the development of advanced formulation approaches (Kalepu & Nekkanti, 2015).
Table 1: Global Prevalence and Projected Growth of Diabetes Mellitus (2021–2045) (International Diabetes Federation [IDF], 2021)
|
Year |
Adults with Diabetes (Millions) |
Global Prevalence (%) |
Source |
|
2021 |
537 |
10.5 |
IDF Diabetes Atlas (2021) |
|
2030 |
643 |
11.3 |
IDF Diabetes Atlas (2021) |
|
2045 |
783 |
12.2 |
IDF Diabetes Atlas (2021) |
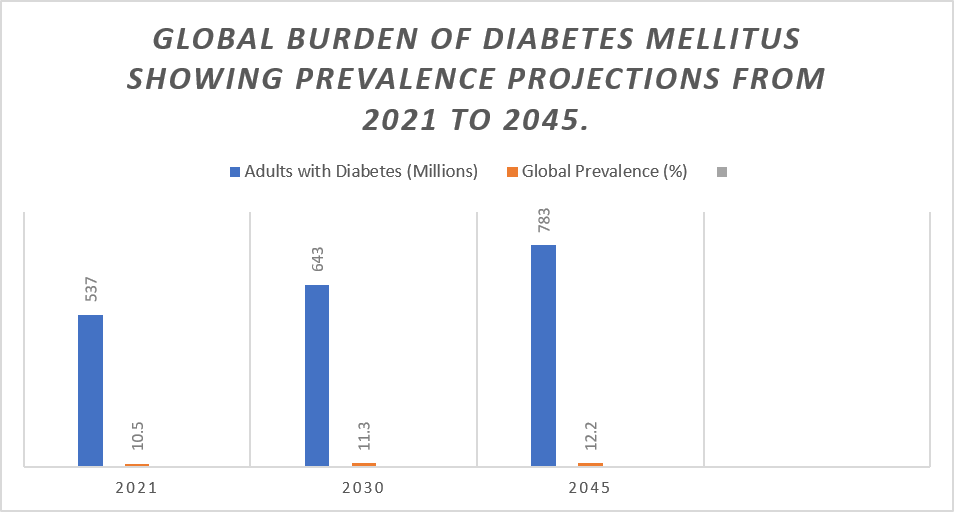
Figure 1: Global burden of diabetes mellitus showing prevalence projections from 2021 to 2045.
Oral administration remains the most preferred route of drug delivery because of its ease of administration, non-invasive nature, patient acceptance, and suitability for chronic therapy (Patel et al., 2020). Nevertheless, successful oral drug delivery requires adequate dissolution of the drug in gastrointestinal fluids followed by permeation across the intestinal epithelium into systemic circulation (Amidon et al., 1995).
Bioavailability refers to the rate and extent to which an active pharmaceutical ingredient reaches systemic circulation and becomes available at the site of action (Shargel & Yu, 2016). Several physiological and physicochemical factors influence oral bioavailability, including aqueous solubility, dissolution rate, intestinal permeability, gastrointestinal pH, gastric emptying time, metabolism, and transporter-mediated drug efflux (Savjani et al., 2012).
Poor aqueous solubility is recognized as one of the major obstacles in oral drug delivery. It has been estimated that nearly 40% of marketed drugs and approximately 70–90% of newly discovered drug molecules exhibit poor water solubility (Kalepu & Nekkanti, 2015). Inadequate solubility often results in slow dissolution rates, incomplete absorption, and high variability in therapeutic response (Dressman & Reppas, 2020).
For antidiabetic drugs with low aqueous solubility, insufficient dissolution in gastrointestinal fluids significantly limits the amount of drug available for absorption, ultimately reducing therapeutic efficacy and increasing inter-patient variability (Patel et al., 2020).
Table 2: Physiological and physicochemical factors affecting oral bioavailability.
|
Factor |
Category |
Impact on Bioavailability |
|
Aqueous Solubility |
Physicochemical |
Influences drug dissolution |
|
Dissolution Rate |
Physicochemical |
Controls amount available for absorption |
|
Particle Size |
Physicochemical |
Smaller particles improve dissolution |
|
Lipophilicity (Log P) |
Physicochemical |
Affects membrane permeation |
|
pKa |
Physicochemical |
Determines ionization and absorption |
|
Gastric Emptying Time |
Physiological |
Influences residence time |
|
Intestinal Transit Time |
Physiological |
Affects absorption window |
|
Gastrointestinal pH |
Physiological |
Influences solubility |
|
Food Effect |
Physiological |
May increase or decrease absorption |
|
First-Pass Metabolism |
Biological |
Reduces systemic availability |
|
Efflux Transporters (P-gp) |
Biological |
Decrease drug absorption |
|
Metabolic Enzymes (CYP450) |
Biological |
Increase drug elimination |
The Biopharmaceutical Classification System (BCS) was proposed by Amidon et al. (1995) to classify drug substances according to their aqueous solubility and intestinal permeability characteristics. The BCS provides a scientific framework for predicting oral drug absorption and guiding formulation development strategies.
According to the BCS, drugs are classified into four categories:
Among these categories, BCS Class-II drugs present significant formulation challenges because their absorption is primarily limited by dissolution rather than permeability (Takagi et al., 2006). Although these drugs possess excellent membrane permeability, their poor aqueous solubility delays dissolution in gastrointestinal fluids, thereby limiting systemic absorption (Savjani et al., 2012).
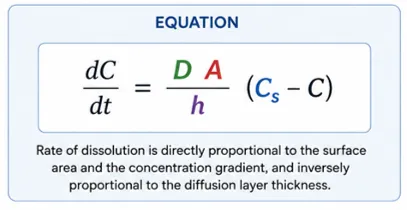
The dissolution behavior of poorly soluble drugs can be explained by the Noyes–Whitney equation, which states that dissolution rate is directly proportional to surface area and saturation solubility (Noyes & Whitney, 1897). Consequently, formulation approaches aimed at increasing surface area, improving wettability, or enhancing saturation solubility can significantly improve bioavailability.
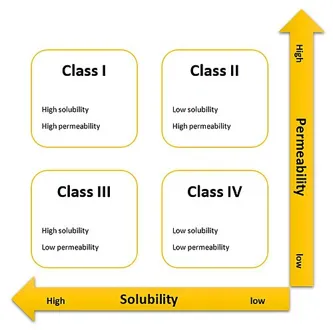
Figure 2: Biopharmaceutical Classification System (BCS) matrix.
Table 3: Characteristics and examples of BCS Classes I–IV drugs.
|
BCS Class |
Solubility |
Permeability |
Absorption Limitation |
Examples |
|
Class I |
High |
High |
None |
Metformin, Paracetamol |
|
Class II |
Low |
High |
Dissolution Limited |
Glibenclamide, Glimepiride, Pioglitazone |
|
Class III |
High |
Low |
Permeability Limited |
Cimetidine, Atenolol |
|
Class IV |
Low |
Low |
Solubility and Permeability Limited |
Hydrochlorothiazide |
1.4 BCS Class-II Antidiabetic Drugs and Their Limitations
Several commonly prescribed oral antidiabetic agents belong to BCS Class-II because of their poor aqueous solubility and high membrane permeability. These include glibenclamide, glimepiride, pioglitazone, and repaglinide (Dahan et al., 2009).
Glibenclamide exhibits very low aqueous solubility, which contributes to dissolution-limited absorption and variable bioavailability (Sweetman, 2020). Similarly, glimepiride possesses poor water solubility, resulting in delayed dissolution and inconsistent plasma concentrations (Kawabata et al., 2011).
Pioglitazone, a thiazolidinedione derivative, demonstrates low aqueous solubility and undergoes extensive hepatic metabolism, which further contributes to variability in systemic drug exposure (Patel et al., 2020). Repaglinide, despite exhibiting rapid absorption, suffers from dissolution-related limitations due to its hydrophobic nature (Dahan et al., 2009).
The major challenges associated with BCS Class-II antidiabetic drugs include:
These limitations often necessitate higher doses and frequent administration, increasing the likelihood of adverse effects and compromising patient adherence (Kalepu & Nekkanti, 2015).
Table 4: Physicochemical properties of BCS Class-II antidiabetic drugs.
|
Drug |
Molecular Weight (g/mol) |
Log P |
Water Solubility |
pKa |
Half-Life (h) |
BCS Class |
|
Glibenclamide |
494.0 |
4.8 |
0.004 mg/mL |
5.3 |
10 |
II |
|
Glimepiride |
490.6 |
3.2 |
0.004 mg/mL |
6.2 |
5–8 |
II |
|
Pioglitazone |
356.4 |
2.3 |
0.04 mg/mL |
5.2 |
3–7 |
II |
|
Repaglinide |
452.6 |
3.8 |
0.034 mg/mL |
4.2 |
1 |
II |
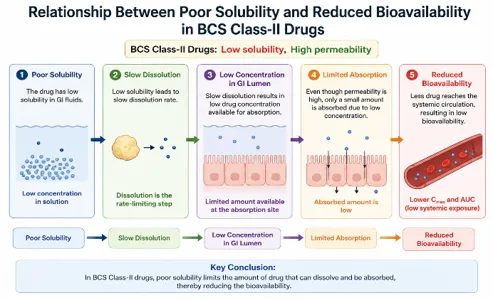
Figure 3: Relationship between poor solubility and reduced bioavailability in BCS Class-II drugs.
1.5 Formulation Strategies for Bioavailability Enhancement
To overcome the challenges associated with BCS Class-II antidiabetic drugs, numerous formulation strategies have been investigated. Conventional techniques include micronization, nanosizing, crystal engineering, salt formation, and solid dispersion technology (Savjani et al., 2012).
Recent advances in nanotechnology have enabled the development of sophisticated drug delivery systems capable of significantly improving drug solubility and oral bioavailability. These systems include nanoemulsions, self-emulsifying drug delivery systems (SEDDS), self-nanoemulsifying drug delivery systems (SNEDDS), solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), polymeric nanoparticles, liposomes, and nanosuspensions (Patel et al., 2020).
Among these approaches, nanoemulsion-based systems have attracted considerable attention due to their ability to improve drug solubilization, enhance intestinal permeability, increase surface area, and facilitate lymphatic uptake (Sharma & Jain, 2018). Several studies have reported significant enhancement in the oral bioavailability of glibenclamide, glimepiride, and pioglitazone through nanoemulsion formulations (Patel et al., 2020).
1.6 Scope and Objective of the Review
Given the increasing prevalence of diabetes mellitus and the formulation challenges associated with poorly soluble antidiabetic drugs, there is a pressing need to evaluate available formulation strategies for enhancing oral bioavailability. This review critically discusses conventional and advanced formulation approaches employed for BCS Class-II antidiabetic drugs, with particular emphasis on nanoemulsions, lipid-based delivery systems, and nanotechnology-driven drug delivery platforms.
Furthermore, the review summarizes recent advancements, comparative effectiveness of different formulation strategies, regulatory considerations, commercialization challenges, and future research opportunities in the field of oral antidiabetic drug delivery.
2.1 Characteristics of BCS Class-II Drugs
The Biopharmaceutical Classification System (BCS) categorizes drug molecules based on their aqueous solubility and intestinal permeability characteristics. According to the BCS proposed by Amidon et al. (1995), Class-II drugs are characterized by low aqueous solubility and high membrane permeability. For these compounds, the rate-limiting step in oral absorption is drug dissolution rather than permeation across the gastrointestinal membrane. Consequently, improving solubility and dissolution rate is critical for enhancing their oral bioavailability.
Many modern therapeutic agents belong to BCS Class-II because advances in medicinal chemistry often favor highly lipophilic molecules with strong receptor-binding affinity. However, increased lipophilicity generally results in poor aqueous solubility, creating significant formulation challenges (Kalepu & Nekkanti, 2015). It is estimated that approximately 40% of marketed drugs and nearly 70–90% of new chemical entities exhibit poor aqueous solubility, emphasizing the importance of solubility enhancement technologies in pharmaceutical development (Savjani et al., 2012).
Low Aqueous Solubility
Aqueous solubility refers to the maximum amount of drug that can dissolve in a given volume of water under specified conditions. BCS Class-II drugs exhibit limited water solubility because of their hydrophobic molecular structures, high crystallinity, and strong intermolecular interactions within the crystal lattice (Kawabata et al., 2011).
Poor aqueous solubility directly affects the dissolution behavior of oral dosage forms. Since only dissolved drug molecules can permeate biological membranes, inadequate dissolution results in reduced absorption and suboptimal therapeutic efficacy. The challenge becomes more pronounced in antidiabetic drugs that require consistent plasma concentrations for effective glycemic control.
High Membrane Permeability
Despite poor solubility, BCS Class-II drugs generally possess high intestinal permeability due to their lipophilic nature. High permeability allows these molecules to readily diffuse across biological membranes once dissolved in gastrointestinal fluids (Amidon et al., 1995).
The permeability of a drug is often correlated with its partition coefficient (Log P). Drugs with moderate to high Log P values demonstrate greater membrane partitioning and transcellular transport. Antidiabetic agents such as glibenclamide, glimepiride, pioglitazone, and repaglinide possess favorable permeability characteristics but remain limited by dissolution rate.
Dissolution-Limited Absorption
For BCS Class-II drugs, oral absorption is primarily controlled by dissolution kinetics. The relationship between dissolution rate and drug absorption can be explained by the Noyes–Whitney equation, which states that dissolution rate increases with surface area and saturation solubility (Noyes & Whitney, 1897).
Since dissolution is the rate-limiting step, formulation strategies that increase drug surface area, improve wettability, reduce crystallinity, or enhance saturation solubility can significantly improve bioavailability. Consequently, BCS Class-II drugs are ideal candidates for advanced drug delivery systems such as nanoemulsions, self-emulsifying systems, nanosuspensions, and lipid nanoparticles (Porter et al., 2007).
Table 5: Comparison of BCS Classes and Absorption Characteristics
|
BCS Class |
Solubility |
Permeability |
Limiting Factor |
|
I |
High |
High |
None |
|
II |
Low |
High |
Dissolution |
|
III |
High |
Low |
Permeability |
|
IV |
Low |
Low |
Solubility and Permeability |
2.2 Common BCS Class-II Antidiabetic Drugs
Several widely prescribed oral antidiabetic agents belong to BCS Class-II and exhibit poor aqueous solubility despite possessing excellent membrane permeability.
Glibenclamide (Glyburide)
Glibenclamide is a second-generation sulfonylurea that stimulates insulin secretion from pancreatic β-cells. Although highly potent, it exhibits extremely poor aqueous solubility (approximately 0.004 mg/mL), resulting in dissolution-limited absorption and variable bioavailability (Sweetman, 2020).
Numerous formulation strategies including solid dispersions, nanosuspensions, and nanoemulsions have been investigated to improve the dissolution behavior of glibenclamide.
Glimepiride
Glimepiride is another second-generation sulfonylurea used extensively in the treatment of Type 2 diabetes mellitus. Similar to glibenclamide, glimepiride exhibits poor aqueous solubility and belongs to BCS Class-II (Kawabata et al., 2011).
Studies have shown that nanotechnology-based delivery systems can significantly enhance the dissolution rate and oral absorption of glimepiride.
Pioglitazone
Pioglitazone belongs to the thiazolidinedione class and acts by improving insulin sensitivity through activation of peroxisome proliferator-activated receptor gamma (PPAR-γ). Despite its therapeutic efficacy, pioglitazone exhibits limited water solubility and undergoes extensive hepatic metabolism, contributing to variable bioavailability (Patel et al., 2020).
Lipid-based formulations and nanoemulsion systems have demonstrated substantial improvements in the bioavailability of pioglitazone.
Repaglinide
Repaglinide is a meglitinide derivative characterized by rapid onset and short duration of action. The drug exhibits poor aqueous solubility but favorable membrane permeability, making it an ideal candidate for solubility enhancement technologies (Dahan et al., 2009).
Table 6: Physicochemical Properties of Common BCS Class-II Antidiabetic Drugs
|
Drug |
Molecular Weight (g/mol) |
Solubility (mg/mL) |
Log P |
pKa |
BCS Class |
|
Glibenclamide |
494.0 |
0.004 |
4.8 |
5.3 |
II |
|
Glimepiride |
490.6 |
0.004 |
3.2 |
6.2 |
II |
|
Pioglitazone |
356.4 |
0.04 |
2.3 |
5.2 |
II |
|
Repaglinide |
452.6 |
0.034 |
3.8 |
4.2 |
II |
2.3 Pharmacokinetic Limitations
Slow Dissolution
The primary pharmacokinetic limitation of BCS Class-II drugs is slow dissolution within gastrointestinal fluids. Poor dissolution delays drug absorption and reduces the amount of drug reaching systemic circulation (Dressman & Reppas, 2020).
Variable Absorption
Variability in gastrointestinal pH, gastric emptying rate, and intestinal transit time contributes to inconsistent absorption patterns among patients. This variability often results in fluctuating plasma drug concentrations and unpredictable therapeutic outcomes.
Food Effect
Food intake can significantly influence the absorption of poorly soluble drugs. High-fat meals may enhance the solubilization of lipophilic drugs, whereas certain foods may delay gastric emptying and alter dissolution behavior (Porter et al., 2007).
First-Pass Metabolism
Several BCS Class-II antidiabetic drugs undergo extensive hepatic metabolism before reaching systemic circulation. This first-pass effect further reduces oral bioavailability and contributes to inter-individual variability in therapeutic response.
Table 7: Pharmacokinetic Limitations of BCS Class-II Antidiabetic Drugs
|
Limitation |
Mechanism |
Clinical Impact |
|
Slow Dissolution |
Poor aqueous solubility |
Reduced absorption |
|
Variable Absorption |
GI variability |
Inconsistent efficacy |
|
Food Effect |
Altered solubilization |
Variable plasma levels |
|
First-Pass Metabolism |
Hepatic drug loss |
Reduced bioavailability |
2.4 Clinical Consequences
The poor aqueous solubility and dissolution-limited absorption of BCS Class-II antidiabetic drugs have important clinical implications.
Reduced Therapeutic Efficacy
Incomplete dissolution may prevent attainment of optimal plasma drug concentrations, reducing therapeutic effectiveness and compromising glycemic control.
Dose Variability
Variability in absorption often necessitates dose adjustments and individualized therapy, particularly in patients with altered gastrointestinal physiology.
Increased Side Effects
Higher doses are frequently required to compensate for poor bioavailability. Increased dosing may elevate the risk of adverse effects, including hypoglycemia in sulfonylurea-treated patients.
Reduced Patient Compliance
Frequent dose adjustments and inconsistent therapeutic outcomes may negatively impact patient adherence and long-term disease management.
Table 8: Clinical Consequences of Poor Bioavailability in BCS Class-II Antidiabetic Drugs
|
Challenge |
Clinical Outcome |
|
Poor Dissolution |
Reduced efficacy |
|
Variable Absorption |
Inconsistent glycemic control |
|
High Dose Requirement |
Increased side effects |
|
Food Effect |
Variable therapeutic response |
|
Bioavailability Variability |
Reduced patient compliance |
3.1 Drug Solubility Issues
Oral bioavailability is largely dependent on the ability of a drug to dissolve in gastrointestinal fluids before permeating the intestinal membrane. Although BCS Class-II drugs possess high membrane permeability, their poor aqueous solubility significantly restricts the amount of drug available for absorption (Amidon et al., 1995). Consequently, dissolution becomes the rate-limiting step in oral drug absorption.
The low aqueous solubility of BCS Class-II antidiabetic drugs is primarily attributed to their physicochemical properties, including high lipophilicity, strong crystal lattice energy, low wettability, and tendency to aggregate in aqueous media (Kalepu & Nekkanti, 2015). Drugs such as glibenclamide, glimepiride, pioglitazone, and repaglinide possess hydrophobic molecular structures that limit their interaction with water molecules, resulting in poor dissolution behavior.
Crystalline Structure
The crystalline nature of drug substances is one of the most important factors influencing aqueous solubility. In crystalline materials, drug molecules are arranged in highly ordered lattices stabilized by intermolecular forces such as hydrogen bonding, van der Waals interactions, and electrostatic forces (Hancock & Parks, 2000).
A large amount of energy is required to break these interactions during dissolution. Consequently, highly crystalline drugs exhibit lower apparent solubility compared with amorphous forms. Most commercially available BCS Class-II antidiabetic drugs are manufactured in crystalline forms because of their superior physical stability. However, this stability often comes at the expense of reduced solubility and slower dissolution rates.
Polymorphism further complicates the situation. Different crystal forms may exhibit different lattice energies and consequently different dissolution characteristics. Less stable polymorphs generally possess higher solubility than thermodynamically stable crystal forms (Brittain, 2009).
Hydrophobicity
Hydrophobicity is commonly expressed using the partition coefficient (Log P), which reflects the affinity of a compound for lipid versus aqueous environments. BCS Class-II drugs generally exhibit moderate to high Log P values, indicating strong lipophilic characteristics (Savjani et al., 2012).
Although lipophilicity facilitates membrane permeation, excessive hydrophobicity decreases interaction with aqueous gastrointestinal fluids. As a result, drug particles remain poorly wetted and dissolve slowly. For example, glibenclamide possesses a Log P value of approximately 4.8, contributing to its extremely poor water solubility.
Particle Aggregation
Another factor limiting solubility is particle aggregation. Fine drug particles possess high surface free energy and tend to aggregate to minimize their total surface area. Aggregation reduces the effective surface area exposed to dissolution media, thereby decreasing dissolution rate and drug absorption (Danaei et al., 2018).
Poor wettability further exacerbates aggregation, particularly in hydrophobic drugs. Consequently, surfactants and wetting agents are frequently incorporated into formulations to improve particle dispersion and enhance dissolution.
Table 9: Drug-Related Factors Affecting Solubility
|
Factor |
Mechanism |
Impact on Bioavailability |
|
Crystallinity |
Strong lattice energy |
Reduced dissolution |
|
Hydrophobicity |
Poor wettability |
Slow dissolution |
|
Aggregation |
Reduced surface area |
Low absorption |
|
Large Particle Size |
Lower surface exposure |
Reduced dissolution |
3.2 Dissolution Rate Limitations
For BCS Class-II drugs, dissolution is the primary determinant of oral absorption. The dissolution process controls the availability of drug molecules for permeation across the intestinal membrane.
Noyes–Whitney Equation
The dissolution behavior of poorly soluble drugs is commonly described by the Noyes–Whitney equation (Noyes & Whitney, 1897):
Equation 1: Noyes–Whitney Equation
Where:
The equation demonstrates that dissolution rate can be enhanced by:
This equation forms the theoretical basis for many formulation strategies such as particle size reduction, solid dispersions, nanoemulsions, and nanosuspensions.
Surface Area Effect
Particle size has a direct influence on dissolution behavior. Reduction in particle size increases surface area available for interaction with dissolution media (Kawabata et al., 2011).
Micronization and nanonization technologies exploit this principle to improve dissolution rates. Nanocrystals, in particular, provide enormous surface area, resulting in significantly enhanced dissolution and absorption.
Table 10: Variables Affecting Dissolution Rate According to Noyes–Whitney Equation
|
Parameter |
Effect on Dissolution |
|
Surface Area (A) ↑ |
Dissolution Increases |
|
Saturation Solubility (Cs) ↑ |
Dissolution Increases |
|
Diffusion Layer Thickness (h) ↓ |
Dissolution Increases |
|
Diffusion Coefficient (D) ↑ |
Dissolution Increases |
3.3 Gastrointestinal Factors
In addition to drug properties, gastrointestinal physiology plays a crucial role in determining oral bioavailability.
pH Variations
The pH of the gastrointestinal tract varies considerably, ranging from approximately 1–3 in the stomach to 6–8 in the intestine. Changes in pH influence drug ionization, solubility, and dissolution behavior (Dressman & Reppas, 2020).
Weakly acidic drugs such as glibenclamide often exhibit poor solubility under gastric conditions but improved dissolution in intestinal fluids. Conversely, pH-dependent precipitation may occur upon transit between different gastrointestinal compartments.
Gastric Emptying
Gastric emptying determines the residence time of drugs within the stomach. Delayed gastric emptying may prolong exposure to acidic conditions and affect dissolution patterns (Shargel & Yu, 2016).
Food intake, disease states, and patient variability can significantly influence gastric emptying rates and ultimately drug absorption.
Intestinal Transit Time
Intestinal transit time determines the duration available for drug absorption. Rapid transit may limit dissolution and reduce absorption of poorly soluble drugs, whereas prolonged residence time may improve bioavailability (Dressman & Reppas, 2020).
Table 11: Gastrointestinal Factors Influencing BCS Class-II Drug Absorption
|
Factor |
Influence on Absorption |
|
Gastric pH |
Alters ionization |
|
Intestinal pH |
Influences dissolution |
|
Gastric Emptying |
Changes residence time |
|
Transit Time |
Alters absorption window |
|
Food Intake |
Affects solubilization |
3.4 Drug–Excipient Interactions
Excipients play a critical role in formulation development and may significantly influence drug dissolution, stability, and bioavailability.
Influence on Dissolution
Hydrophilic carriers such as polyethylene glycol (PEG), polyvinylpyrrolidone (PVP), hydroxypropyl methylcellulose (HPMC), and Soluplus® improve wettability and dissolution of poorly soluble drugs (Kalepu & Nekkanti, 2015).
Surfactants such as Tween 80, Cremophor EL, and Poloxamers reduce interfacial tension and facilitate drug solubilization.
Stability Concerns
Although excipients can improve dissolution, they may also influence drug stability. Potential concerns include:
Therefore, compatibility studies are essential during formulation development.
Table 12: Common Excipients Used for Solubility Enhancement
|
Excipient |
Function |
Example Application |
|
PEG |
Hydrophilic carrier |
Solid dispersions |
|
PVP |
Amorphous stabilization |
Solid dispersions |
|
HPMC |
Dissolution enhancement |
Tablets |
|
Soluplus® |
Polymeric solubilizer |
Amorphous dispersions |
|
Tween 80 |
Surfactant |
Nanoemulsions |
|
Poloxamer 188 |
Wetting agent |
Nanosuspensions |
4.1 Particle Size Reduction
Particle size reduction is one of the oldest and most widely employed approaches for enhancing the dissolution rate and oral bioavailability of poorly water-soluble drugs. According to the Noyes–Whitney equation, dissolution rate is directly proportional to the surface area available for dissolution (Noyes & Whitney, 1897). Therefore, reducing particle size increases the surface area-to-volume ratio, leading to improved wettability and dissolution.
For BCS Class-II antidiabetic drugs such as glibenclamide, glimepiride, pioglitazone, and repaglinide, particle size reduction has been extensively investigated as a means of overcoming dissolution-limited absorption (Kawabata et al., 2011).
Micronization
Micronization refers to the reduction of particle size into the micrometer range (typically 1–10 μm). The process is commonly performed using jet milling, ball milling, hammer milling, or fluid energy milling techniques (Savjani et al., 2012).
Principle
Micronization increases the surface area exposed to dissolution media, thereby accelerating drug dissolution and improving oral absorption.
Advantages
Limitations
Studies on micronized glibenclamide formulations have demonstrated enhanced dissolution rates and improved hypoglycemic activity compared with conventional formulations (Sweetman, 2020).
Nanonization
Nanonization reduces drug particles into the nanometer range (10–1000 nm), providing a significantly larger surface area than micronized particles (Müller & Keck, 2004).
Wet Milling
Wet milling involves the mechanical reduction of particle size in the presence of stabilizers and aqueous media. The technique produces stable nanosuspensions suitable for oral delivery.
High-Pressure Homogenization
High-pressure homogenization forces drug suspensions through narrow gaps at high pressure, generating intense shear forces that reduce particle size.
Drug Nanocrystals
Drug nanocrystals consist of pure drug particles stabilized by surfactants or polymers. Their increased surface area and enhanced saturation solubility result in superior dissolution characteristics (Müller & Keck, 2004).
Several studies have reported significant enhancement in the dissolution and bioavailability of glimepiride and pioglitazone nanocrystals compared with their coarse counterparts.
Applications in Antidiabetic Drugs
Particle size reduction has been successfully applied to:
These systems have shown improved dissolution profiles, faster onset of action, and enhanced oral bioavailability.
Table 13:Comparison of Micronization and Nanonization
|
Parameter |
Micronization |
Nanonization |
|
Particle Size |
1–10 μm |
10–1000 nm |
|
Surface Area |
Moderate |
Very High |
|
Dissolution Enhancement |
Moderate |
High |
|
Bioavailability Improvement |
Moderate |
High |
|
Cost |
Low |
Higher |
4.2 Solid Dispersion Technology
Solid dispersion technology is among the most effective approaches for improving the dissolution behavior of poorly soluble drugs. The technique involves dispersing a hydrophobic drug within a hydrophilic carrier matrix to improve wettability, reduce crystallinity, and enhance apparent solubility (Chiou & Riegelman, 1971).
Principle
When dispersed at the molecular or amorphous level within a carrier, the drug exhibits:
Types of Solid Dispersions
Eutectic Systems
Drug and carrier crystallize separately but in finely divided forms.
Solid Solutions
Drug molecules are molecularly dispersed within the carrier matrix.
Amorphous Solid Dispersions
Drug exists in an amorphous state, exhibiting higher apparent solubility than crystalline forms (Hancock & Parks, 2000).
Carriers Used
Polyethylene Glycol (PEG)
Polyvinylpyrrolidone (PVP)
Hydroxypropyl Methylcellulose (HPMC)
Soluplus®
Applications in Glibenclamide and Glimepiride
Solid dispersions of glibenclamide using PEG and PVP have demonstrated several-fold increases in dissolution rates. Similarly, glimepiride-Soluplus® dispersions have shown substantial improvements in bioavailability.
Mechanism of Solid Dispersion
Crystalline Drug
+
Hydrophilic Carrier
↓
Molecular Dispersion
↓
Improved Wettability
↓
Enhanced Dissolution
Table 14: Common Carriers Used in Solid Dispersion Systems
|
Carrier |
Type |
Function |
|
PEG |
Hydrophilic Polymer |
Wettability enhancement |
|
PVP |
Amorphous Stabilizer |
Dissolution enhancement |
|
HPMC |
Polymer |
Recrystallization inhibition |
|
Soluplus® |
Amphiphilic Polymer |
Solubilization |
4.3 Crystal Engineering
Crystal engineering refers to the modification of crystal structure to improve physicochemical properties such as solubility, dissolution rate, and stability (Brittain, 2009).
Polymorphism
Polymorphism occurs when a drug exists in multiple crystalline forms.
Different polymorphs may exhibit:
Metastable polymorphs generally possess higher solubility than stable crystal forms.
Co-Crystals
Co-crystals consist of an active pharmaceutical ingredient and a co-former held together through non-covalent interactions.
Advantages include:
Several glibenclamide and pioglitazone co-crystals have shown significantly improved dissolution profiles.
Amorphous Systems
Amorphous drugs lack long-range molecular order and possess higher free energy than crystalline forms (Hancock & Parks, 2000).
Advantages:
However, physical instability and recrystallization remain major concerns.
Impact on Solubility
Crystal engineering modifies molecular packing and lattice energy, reducing the energy required for dissolution. Consequently, crystal-engineered systems frequently exhibit enhanced dissolution behavior and oral absorption.
Table 15: Crystal Engineering Strategies for BCS Class-II Drugs
|
Strategy |
Mechanism |
Advantage |
Limitation |
|
Polymorphism |
Crystal modification |
Improved dissolution |
Stability issues |
|
Co-crystals |
Molecular complexation |
Improved solubility |
Co-former selection |
|
Amorphous Systems |
Reduced crystallinity |
High solubility |
Recrystallization |
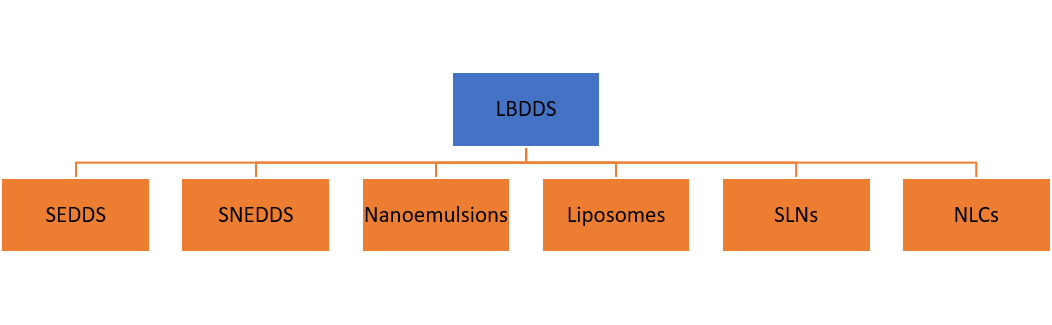
Lipid-based drug delivery systems (LBDDS) have emerged as one of the most effective approaches for improving the oral bioavailability of poorly water-soluble drugs. These systems utilize lipids, surfactants, and co-surfactants to enhance drug solubilization, facilitate intestinal absorption, and reduce the impact of dissolution-limited absorption (Porter et al., 2007). The ability of lipid-based formulations to maintain drugs in a solubilized state throughout gastrointestinal transit makes them particularly attractive for BCS Class-II antidiabetic drugs such as glibenclamide, glimepiride, pioglitazone, and repaglinide.
The mechanisms by which lipid-based formulations enhance bioavailability include improved drug solubilization, increased surface area for absorption, stimulation of lymphatic transport, inhibition of efflux transporters, and protection against enzymatic degradation (Pouton, 2006). Consequently, numerous lipid-based systems have been developed, including self-emulsifying drug delivery systems (SEDDS), self-nanoemulsifying drug delivery systems (SNEDDS), nanoemulsions, liposomes, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs).
Classification of Lipid-Based Drug Delivery Systems
5.1 Self-Emulsifying Drug Delivery Systems (SEDDS)
Introduction and Principle
Self-emulsifying drug delivery systems (SEDDS) are isotropic mixtures of oils, surfactants, and co-solvents that spontaneously form fine oil-in-water emulsions upon dilution with gastrointestinal fluids under gentle agitation (Pouton, 2006).
The spontaneous emulsification process significantly increases the interfacial surface area available for drug release and absorption. Unlike conventional formulations, SEDDS maintain poorly soluble drugs in a dissolved state, thereby minimizing precipitation during gastrointestinal transit.
Components of SEDDS
Oils
The oil phase serves as the primary solubilization medium for lipophilic drugs.
Common oils include:
Surfactants
Surfactants reduce interfacial tension and facilitate self-emulsification.
Common surfactants include:
Co-Surfactants
Co-surfactants improve flexibility of the interfacial film and facilitate nano-droplet formation.
Examples include:
Advantages of SEDDS
Applications in Antidiabetic Drugs
SEDDS formulations of glibenclamide and repaglinide have demonstrated significant improvements in dissolution rate and oral bioavailability compared with conventional tablets (Patel et al., 2020).
Mechanism of Self-Emulsification
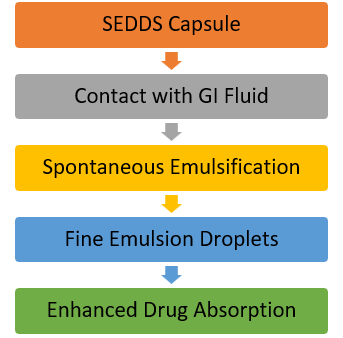
Table 16: Common Components Used in SEDDS Formulations
|
Component Type |
Examples |
Function |
|
Oils |
Capryol®, Oleic Acid |
Drug Solubilization |
|
Surfactants |
Tween 80, Cremophor RH40 |
Emulsification |
|
Co-Surfactants |
PEG 400, Transcutol P |
Interfacial Stabilization |
5.2 Self-Nanoemulsifying Drug Delivery Systems (SNEDDS)
Formulation Design
SNEDDS are advanced versions of SEDDS that produce nano-sized emulsions with droplet diameters generally below 200 nm upon dilution (Porter et al., 2007).
The formulation design process typically involves:
Mechanism of Bioavailability Enhancement
SNEDDS improve bioavailability through:
Recent Research Findings
Several studies have demonstrated:
Table 17: Recent SNEDDS Formulations for Antidiabetic Drugs
|
Drug |
Oil |
Surfactant |
Outcome |
|
Glibenclamide |
Capryol® |
Tween 80 |
Enhanced Bioavailability |
|
Pioglitazone |
Oleic Acid |
Cremophor RH40 |
Improved Dissolution |
|
Glimepiride |
MCT Oil |
Labrasol® |
Faster Absorption |
5.3 Nanoemulsions
Introduction
Nanoemulsions are thermodynamically or kinetically stable colloidal dispersions consisting of oil droplets dispersed in an aqueous phase with droplet sizes typically ranging from 20–200 nm (McClements, 2012).
Nanoemulsions offer several advantages:
Components
Oil Phase
Surfactant
Co-Surfactant
Aqueous Phase
Preparation Methods
High-Energy Methods
Low-Energy Methods
Characterization
Key characterization parameters include:
Applications in Glibenclamide and Pioglitazone
Nanoemulsions have demonstrated:
Structure of a Nanoemulsion
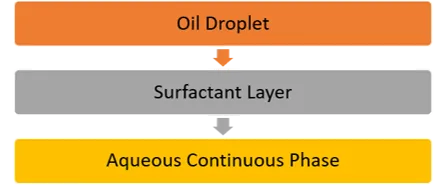
Table 18: Nanoemulsion Formulations Reported for Antidiabetic Drugs
|
Drug |
Oil Phase |
Droplet Size (nm) |
Bioavailability Enhancement |
|
Glibenclamide |
Capryol® |
90–150 |
3–5 Fold |
|
Pioglitazone |
Oleic Acid |
80–120 |
2–4 Fold |
|
Glimepiride |
IPM |
70–130 |
3 Fold |
5.4 Liposomes
Structure
Liposomes are vesicular systems composed of phospholipid bilayers surrounding aqueous compartments (Akbarzadeh et al., 2013).
Preparation Techniques
Advantages
Antidiabetic Applications
Liposomal formulations of pioglitazone have demonstrated improved pharmacokinetic profiles and reduced systemic toxicity.
Liposome Structure
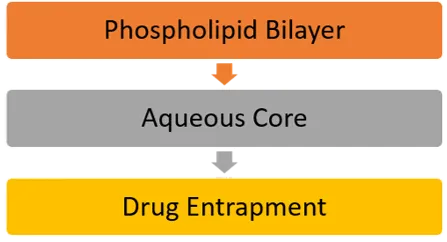
Table 19: Advantages and Limitations of Liposomes
|
Advantages |
Limitations |
|
Biocompatible |
High Cost |
|
Controlled Release |
Stability Issues |
|
Enhanced Absorption |
Scale-Up Challenges |
5.5 Solid Lipid Nanoparticles (SLNs)
Composition
SLNs consist of:
Advantages
Recent Developments
SLN formulations of glibenclamide and pioglitazone have shown enhanced oral absorption and prolonged therapeutic effects.
Structure of Solid Lipid Nanoparticles
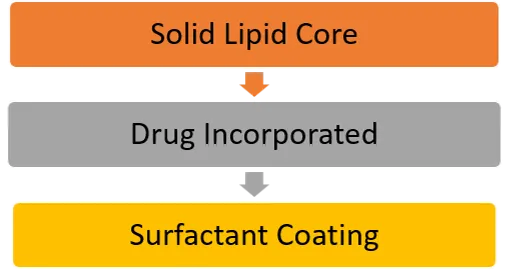
Table 20: SLN-Based Antidiabetic Formulations
|
Drug |
Lipid Used |
Outcome |
|
Glibenclamide |
Glyceryl Monostearate |
Improved Bioavailability |
|
Pioglitazone |
Stearic Acid |
Sustained Release |
5.6 Nanostructured Lipid Carriers (NLCs)
Formulation
NLCs are second-generation lipid nanoparticles consisting of a mixture of solid and liquid lipids (Müller et al., 2002).
Advantages Over SLNs
Therapeutic Applications
NLC formulations of antidiabetic drugs have demonstrated:
Table 21: Comparison of SLNs and NLCs
|
Parameter |
SLNs |
NLCs |
|
Drug Loading |
Moderate |
High |
|
Stability |
Good |
Excellent |
|
Drug Expulsion |
Possible |
Reduced |
|
Bioavailability |
High |
Very High |
Polymeric nanocarriers have emerged as highly promising drug delivery platforms for improving the oral bioavailability of BCS Class-II antidiabetic drugs. These systems offer several advantages, including enhanced solubility, controlled drug release, protection from degradation, prolonged circulation time, and targeted drug delivery. Polymeric nanocarriers can encapsulate hydrophobic drugs within their matrix or core, thereby improving dissolution and absorption characteristics (Danhier et al., 2012).
For poorly water-soluble antidiabetic drugs such as glibenclamide, glimepiride, pioglitazone, and repaglinide, polymeric nanocarriers have demonstrated significant improvements in bioavailability and therapeutic efficacy. The major polymeric nanocarrier systems include polymeric nanoparticles, polymeric micelles, dendrimers, hydrogels, and nanogels.
6.1 Polymeric Nanoparticles
Polymeric nanoparticles are colloidal systems typically ranging from 10–1000 nm in size, composed of biodegradable and biocompatible polymers. Depending on their structure, polymeric nanoparticles may be classified as nanospheres or nanocapsules (Danhier et al., 2012).
Mechanism of Bioavailability Enhancement
Polymeric nanoparticles improve oral bioavailability through:
Natural Polymers
Natural polymers possess excellent biocompatibility and low toxicity.
Chitosan
Chitosan is a cationic polysaccharide obtained from chitin. It exhibits:
Chitosan nanoparticles have been extensively investigated for oral delivery of glibenclamide and pioglitazone, showing improved absorption and prolonged hypoglycemic effects (Agnihotri et al., 2004).
Alginate
Alginate is an anionic polysaccharide derived from brown seaweed.
Advantages include:
Alginate-based nanoparticles have shown potential in improving oral delivery of antidiabetic drugs.
Synthetic Polymers
Synthetic polymers offer greater control over physicochemical properties and degradation kinetics.
Poly(lactic-co-glycolic acid) (PLGA)
PLGA is one of the most extensively studied biodegradable polymers approved by regulatory agencies.
Advantages:
PLGA nanoparticles have been successfully employed for pioglitazone and glimepiride delivery (Makadia & Siegel, 2011).
Polycaprolactone (PCL)
PCL is a semi-crystalline biodegradable polymer characterized by:
PCL nanoparticles have shown promising results for long-term antidiabetic therapy.
Classification of Polymeric Nanoparticles
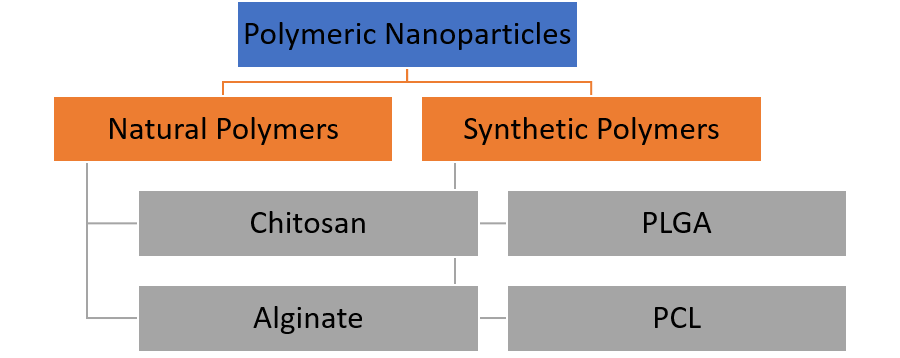
Table 22: Natural and Synthetic Polymers Used in Antidiabetic Drug Delivery
|
Polymer |
Type |
Advantages |
Applications |
|
Chitosan |
Natural |
Mucoadhesive |
Glibenclamide |
|
Alginate |
Natural |
pH-sensitive |
Oral delivery |
|
PLGA |
Synthetic |
Controlled release |
Pioglitazone |
|
PCL |
Synthetic |
Long-term release |
Sustained therapy |
6.2 Polymeric Micelles
Polymeric micelles are self-assembled nanostructures formed from amphiphilic block copolymers in aqueous environments. They typically possess sizes ranging from 10–100 nm (Torchilin, 2007).
Structure
Polymeric micelles consist of:
The hydrophobic core acts as a reservoir for poorly soluble drugs, while the hydrophilic shell stabilizes the system in biological fluids.
Drug Loading
Hydrophobic antidiabetic drugs are incorporated into the micellar core through:
Solubilization Mechanism
Micelles significantly enhance apparent solubility by maintaining drug molecules within the hydrophobic core in a dissolved state.
Advantages include:
Table 23: Characteristics of Polymeric Micelles
|
Parameter |
Description |
|
Size Range |
10–100 nm |
|
Core |
Hydrophobic |
|
Shell |
Hydrophilic |
|
Drug Loading |
High |
|
Solubility Enhancement |
Excellent |
6.3 Dendrimers
Dendrimers are highly branched, monodisperse macromolecules characterized by a tree-like architecture. Their unique structure provides multiple functional groups for drug loading and surface modification (Tomalia et al., 2005).
Classification
Dendrimers are classified according to generation number:
Higher generations possess:
Drug Encapsulation
Drugs may be incorporated through:
Advantages
Dendrimer-based systems have demonstrated improved solubilization of several hydrophobic antidiabetic drugs.
Limitations of Dendrimers
6.4 Hydrogels and Nanogels
Hydrogels are three-dimensional polymeric networks capable of absorbing large quantities of water while maintaining structural integrity (Peppas et al., 2000).
Nanogels are nanosized hydrogel particles that combine hydrogel properties with nanotechnology-based advantages.
Preparation
Common preparation methods include:
Controlled Release Potential
Hydrogels and nanogels offer:
Applications in Antidiabetic Therapy
Hydrogel systems have been investigated for:
Stimuli-Responsive Hydrogels
Advanced hydrogels respond to:
These smart systems may facilitate personalized diabetes management in the future.
Comparative Analysis of Polymeric Nanocarriers
Table 24: Comparison of Polymeric Nanocarrier Systems
|
System |
Size Range |
Drug Loading |
Release Control |
Bioavailability Enhancement |
|
Polymeric Nanoparticles |
50–1000 nm |
High |
Excellent |
High |
|
Polymeric Micelles |
10–100 nm |
Moderate–High |
Moderate |
Very High |
|
Dendrimers |
5–20 nm |
Very High |
Excellent |
High |
|
Hydrogels |
Variable |
Moderate |
Excellent |
Moderate |
|
Nanogels |
20–200 nm |
High |
Excellent |
High |
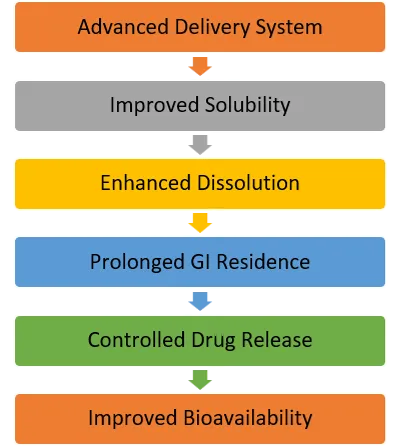
Advanced drug delivery systems have gained considerable attention for overcoming the solubility and bioavailability limitations associated with BCS Class-II antidiabetic drugs. While conventional and lipid-based formulations improve dissolution and absorption, advanced delivery systems provide additional advantages such as controlled release, targeted delivery, enhanced stability, improved mucoadhesion, and prolonged therapeutic action. Among these technologies, nanosuspensions, inclusion complexes, mesoporous silica nanoparticles, and mucoadhesive systems have demonstrated significant potential for improving the oral delivery of poorly soluble antidiabetic drugs such as glibenclamide, glimepiride, pioglitazone, and repaglinide.
7.1 Nanosuspensions
Introduction
Nanosuspensions are submicron colloidal dispersions of pure drug particles stabilized by surfactants or polymers. The particle size typically ranges from 100–1000 nm, resulting in a dramatic increase in surface area and dissolution rate (Müller & Keck, 2004).
Unlike lipid-based systems, nanosuspensions contain minimal excipients and are particularly suitable for drugs with poor solubility in both aqueous and lipid media.
Preparation Methods
Top-Down Technologies
Top-down approaches reduce the size of larger drug particles through mechanical processes.
Wet Media Milling
Drug particles are milled in the presence of stabilizers using grinding media.
Advantages:
High-Pressure Homogenization
Drug suspensions are forced through narrow gaps under high pressure.
Advantages:
Bottom-Up Technologies
Bottom-up approaches involve precipitation of drug molecules from solution.
Solvent–Antisolvent Precipitation
Drug dissolved in solvent
↓
Addition to antisolvent
↓
Rapid nucleation
↓
Nanoparticle formation
Advantages
Applications in Antidiabetic Drugs
Studies have reported:
Table 25: Nanosuspension Technologies
|
Method |
Principle |
Advantages |
Limitations |
|
Wet Milling |
Particle size reduction |
Scalable |
Equipment wear |
|
High-Pressure Homogenization |
Shear force generation |
Uniform particles |
High energy requirement |
|
Precipitation |
Controlled nucleation |
Small particles |
Solvent removal required |
7.2 Inclusion Complexes
Introduction
Inclusion complexation is a molecular encapsulation technique used to improve the solubility, dissolution rate, and stability of poorly soluble drugs. The most commonly used complexing agents are cyclodextrins (Loftsson & Brewster, 2010).
Cyclodextrins possess:
This unique structure allows hydrophobic drug molecules to be accommodated within the cavity while maintaining aqueous solubility.
Cyclodextrin-Based Complexes
Common cyclodextrins include:
Solubility Enhancement Mechanism
Poorly Soluble Drug
↓
Inclusion into Cyclodextrin Cavity
↓
Improved Aqueous Solubility
↓
Enhanced Dissolution
↓
Improved Absorption
Applications in Antidiabetic Drugs
Cyclodextrin complexes have been reported for:
These complexes significantly improve dissolution and oral bioavailability.
Table 26: Cyclodextrins Used for Solubility Enhancement
|
Cyclodextrin |
Characteristics |
Pharmaceutical Application |
|
α-CD |
Small cavity |
Small molecules |
|
β-CD |
Most common |
Solubility enhancement |
|
γ-CD |
Large cavity |
Large molecules |
|
HPβCD |
Highly water soluble |
Oral formulations |
7.3 Mesoporous Silica Nanoparticles (MSNs)
Introduction
Mesoporous silica nanoparticles are inorganic nanocarriers characterized by highly ordered pore structures and large surface areas (Vallet-Regí et al., 2007).
Typical properties include:
Drug Loading
Drug molecules are loaded into nanopores through:
The confined environment inside pores often converts crystalline drugs into amorphous forms, significantly improving dissolution behavior.
Controlled Release Mechanism
MSNs can provide:
Applications in Antidiabetic Drugs
Research has demonstrated enhanced dissolution of:
through incorporation into mesoporous silica matrices.
Mesoporous Silica Nanoparticle Structure
Porous Silica Matrix
↓
Drug Loaded Nanopores
↓
Controlled Drug Release
Table 27: Advantages of Mesoporous Silica Nanoparticles
|
Property |
Benefit |
|
Large Surface Area |
High drug loading |
|
Mesoporous Structure |
Enhanced dissolution |
|
Surface Functionalization |
Targeting capability |
|
Physical Stability |
Improved shelf life |
7.4 Mucoadhesive Systems
Introduction
Mucoadhesive systems are designed to adhere to the mucus layer covering gastrointestinal tissues, thereby prolonging residence time and improving drug absorption (Andrews et al., 2009).
For BCS Class-II antidiabetic drugs, extended residence time can significantly enhance dissolution and absorption.
Mechanism of Mucoadhesion
The mucoadhesion process involves:
Stage 1: Contact
Drug delivery system comes into contact with mucus layer.
Stage 2: Interpenetration
Polymer chains interpenetrate mucus glycoproteins.
Stage 3: Adhesion
Hydrogen bonding and electrostatic interactions establish strong attachment.
Common Mucoadhesive Polymers
Natural Polymers
Synthetic Polymers
Bioavailability Benefits
Mucoadhesive systems improve:
Applications in Antidiabetic Drug Delivery
Mucoadhesive formulations of glibenclamide and pioglitazone have shown:
Mechanism of Mucoadhesion
Drug Carrier
↓
Contact with Mucus
↓
Polymer-Mucin Interaction
↓
Adhesion
↓
Enhanced Drug Absorption
Table 28: Mucoadhesive Polymers Used in Oral Drug Delivery
|
Polymer |
Type |
Function |
|
Chitosan |
Natural |
Permeation enhancer |
|
Alginate |
Natural |
Sustained release |
|
Carbopol |
Synthetic |
Strong adhesion |
|
HPMC |
Synthetic |
Controlled release |
Comparative Analysis of Advanced Drug Delivery Systems
Table 29: Comparison of Advanced Drug Delivery Systems for BCS Class-II Drugs
|
System |
Solubility Enhancement |
Drug Loading |
Controlled Release |
Scale-Up Potential |
|
Nanosuspension |
High |
Excellent |
Moderate |
High |
|
Inclusion Complex |
Moderate–High |
Moderate |
Low |
Excellent |
|
Mesoporous Silica Nanoparticles |
High |
High |
High |
Moderate |
|
Mucoadhesive Systems |
Moderate |
Moderate |
High |
High |
Mechanisms of Bioavailability Enhancement in Advanced Drug Delivery Systems
8.1 Comparative Evaluation of Solubility Enhancement Strategies
The primary objective of formulation development for BCS Class-II drugs is to improve aqueous solubility and dissolution rate. Different technologies achieve this goal through distinct mechanisms.
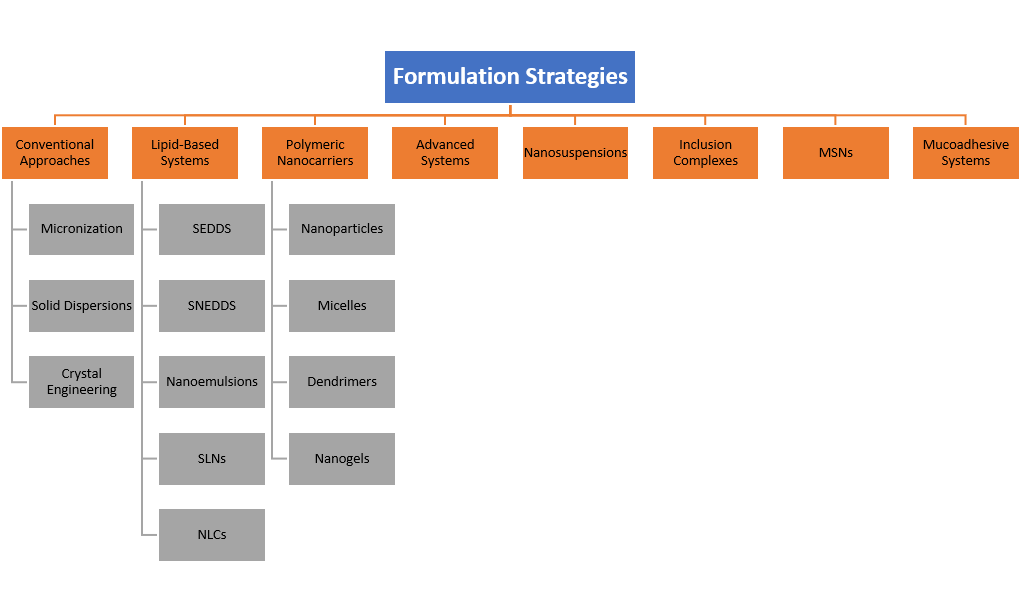
Conventional Approaches
Micronization, nanonization, solid dispersions, and crystal engineering primarily improve dissolution by increasing surface area or reducing crystallinity (Kawabata et al., 2011).
Advantages:
Limitations:
Lipid-Based Systems
Lipid-based formulations improve drug solubilization through incorporation within lipid matrices and emulsified systems.
Advantages:
Limitations:
Polymeric Nanocarriers
Polymeric systems improve bioavailability through encapsulation, controlled release, and enhanced mucosal interaction.
Advantages:
Limitations:
Advanced Drug Delivery Systems
Technologies such as nanosuspensions, inclusion complexes, and mesoporous silica nanoparticles provide additional flexibility for enhancing dissolution and drug release characteristics.
Advantages:
Limitations:
Classification of Formulation Strategies for BCS Class-II Drugs
8.2 Comparative Analysis of Solubility Enhancement
The magnitude of solubility enhancement varies among formulation strategies.
Solid dispersions generally improve dissolution by converting crystalline drugs into amorphous forms. Nanoemulsions and SNEDDS often provide greater solubilization due to the presence of lipidic solubilization reservoirs (Porter et al., 2007).
NLCs frequently demonstrate superior drug loading and long-term stability compared with SLNs because of their imperfect lipid matrices.
Polymeric micelles and dendrimers exhibit exceptional solubilization capacity for highly lipophilic compounds but may be associated with manufacturing complexity.
Table 30: Comparison of Solubility Enhancement Potential
|
Technology |
Solubility Enhancement |
Mechanism |
|
Micronization |
Moderate |
Surface area increase |
|
Nanocrystals |
High |
Surface area increase |
|
Solid Dispersion |
High |
Amorphization |
|
SEDDS |
Very High |
Self-emulsification |
|
SNEDDS |
Very High |
Nanoemulsification |
|
Nanoemulsion |
Very High |
Drug solubilization |
|
SLNs |
High |
Lipid encapsulation |
|
NLCs |
Very High |
Imperfect lipid matrix |
|
Polymeric Micelles |
Very High |
Core encapsulation |
|
Inclusion Complexes |
Moderate–High |
Molecular complexation |
8.3 Stability Considerations
Formulation stability is critical for commercial success.
Physical Stability
Challenges include:
Nanoemulsions and SNEDDS generally exhibit excellent thermodynamic stability, while solid dispersions may experience recrystallization during storage (Hancock & Parks, 2000).
Chemical Stability
Factors affecting chemical stability include:
Polymeric nanoparticles and NLCs often provide superior protection against degradation.
8.4 Scale-Up and Manufacturing Considerations
Commercial translation requires scalable and reproducible manufacturing processes.
High Scale-Up Potential
These technologies are already utilized in several marketed pharmaceutical products.
Moderate Scale-Up Potential
Scale-up may require specialized equipment and process optimization.
Low-to-Moderate Scale-Up Potential
Manufacturing complexity remains a major challenge.
Table 31: Manufacturing and Scale-Up Comparison
|
Technology |
Manufacturing Complexity |
Scale-Up Potential |
|
Micronization |
Low |
Excellent |
|
Solid Dispersion |
Low–Moderate |
Excellent |
|
SEDDS |
Moderate |
Excellent |
|
SNEDDS |
Moderate |
Excellent |
|
Nanoemulsion |
Moderate |
Good |
|
SLNs |
Moderate–High |
Good |
|
NLCs |
Moderate–High |
Good |
|
Polymeric Nanoparticles |
High |
Moderate |
|
Dendrimers |
Very High |
Limited |
8.5 Suitability for Antidiabetic Drugs
The selection of formulation strategy depends on the physicochemical characteristics of individual antidiabetic drugs.
Glibenclamide
Most suitable systems:
Glimepiride
Most suitable systems:
Pioglitazone
Most suitable systems:
Repaglinide
Most suitable systems:
8.6 Decision-Making Framework for Formulation Selection
A rational formulation development strategy should consider:
Drug Factors
Formulation Factors
Regulatory Factors
Table 32: Comprehensive Comparison of Formulation Strategies for BCS Class-II Antidiabetic Drugs
|
Technology |
Solubility Enhancement |
Stability |
Drug Loading |
Scale-Up Potential |
Clinical Potential |
|
Micronization |
Moderate |
High |
Excellent |
Excellent |
Moderate |
|
Solid Dispersion |
High |
Moderate |
Good |
Excellent |
High |
|
SEDDS |
Very High |
High |
High |
Excellent |
Very High |
|
SNEDDS |
Very High |
High |
High |
Excellent |
Very High |
|
Nanoemulsion |
Very High |
Moderate |
High |
Good |
Very High |
|
SLNs |
High |
High |
Moderate |
Good |
High |
|
NLCs |
Very High |
High |
High |
Good |
Very High |
|
Polymeric Nanoparticles |
High |
High |
High |
Moderate |
High |
|
Polymeric Micelles |
Very High |
Moderate |
Moderate |
Moderate |
High |
|
Inclusion Complexes |
Moderate |
High |
Moderate |
Excellent |
Moderate |
REFERENCES


Chetan Jain, Dr. Vaibhavkumar Jagtap, Formulation Strategies to Enhance the Bioavailability of BCS Class-II Antidiabetic Drugs: Current Advances and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 5967-6001. https://doi.org/10.5281/zenodo.20815200
 10.5281/zenodo.20815200
10.5281/zenodo.20815200