
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Vivekanandha Pharmacy College, Sankari, Salem, Tamil Nadu, India - 637 303
Diabetes mellitus is a long term metabolic disease, which is initially characterized by impaired secretion and action of insulin, resulting in chronic hyper glycemia and complication. Traditional insulin therapy in form of subcutaneous injection usually causes low patient compliance, topical pain, and intermittent glucose levels. Microneedle technology has also become a painless, efficient, and minimally invasive system of trans-dermal delivery in recent years of macromolecules such as insulin. The addition of herbal bio-actives to the epidermal needle is an innovative and comprehensive solution to diabetes. The patches are made of herbs and have the ability to combine the pharmacological properties of natural anti-diabetic compounds- poly-phenols, flavonoids, alkaloids, terpenoids with the accuracy of controlled insulin delivery. In addition to their capability to release drugs in a sustained and localized manner, these systems have other positive effects of antioxidant, anti-inflammatory, and beta-cell protective mechanism. Natural biopolymers such as chitosan, alginate, cellulose, starch, and silk fibroin improve biocompatibility, mechanical strength and biodegradability of Micro-needle matrices. Moreover, codelivery of insulin with herbal extracts, such as Gymnema sylvestre, Momordica charantia, or Trigonella foenum graecum, provides a synergistic effect with respect to enhancing glycemic control due to a variety of action mechanisms. Preclinical data evidence high levels of insulin absorption, glucose regulation and reduction of oxidative stress using these systems. In general, herbal-based micro-needle patches are an enormous potential of the next generation, patient-friendly approach to non-invasive, sustained, and successful diabetes treatment. Nevertheless, their successful translation into clinical use requires further clinical validation, herbal formulation standardization as well as scalable manufacturing.
Diabetes Mellitus
Diabetes mellitus is a worldwide health condition that causes a high level of glucose in the blood due to the inadequacy in producing insulin or the inability to utilize it properly [1]. Diabetes mellitus is a disease marked by hyper glycemia as a result of insulin resistance, low secretion of insulin or high secretion of glucagon. Diabetes mellitus is a non-infectious illness, which is triggered by the imbalance in the carbohydrate metabolism of which culminates in sustained hyper glycemia [2]. In relation to insulin deficiency, Type 2 diabetes mellitus (T2DM) also called insulin non-dependent diabetes mellitus / adult onset diabetes is the fourth leading cause of death in the varied developed nations besides possibilities of cardiac diseases such as coronary heart diseases and is also going to grow to 134.2 million cases in 2045 [3] with India having over 77 million people of 20-79 years old already with diabetes and predisposed to develop cardiac diseases like coronary heart diseases and stroke [4] The effects of diabetes are not merely evident since over 1 million deaths in India can be linked to diabetes and its complications [5].
Current Therapeutic Approaches
Recently several innovative strategies have been followed in managing the diabetes mellitus which include nanotechnology based insulin delivery systems founded on enhancing the accuracy, efficiency and patient compliance of insulin therapy [6] Nano-particle based glucose monitoring, such as, gold nano particle and quantum dots have distinct optical and electrical characteristics that can be used to design sensitive glucose sensors [7] smart insulin delivery system innovations are based on advanced technology to offer precise and automated control of insulin therapy [8].
Challenges in Traditional Insulin Delivery
Problems in the conventional delivery of insulin, There are various significant limitations of conventional methods of delivering insulin that affect patient compliance and overall glycemic control. The key problems are the following:
Subcutaneous injection is the most common insulin administration method that often causes pain on the injection location. This pain can de-motivate the patients to take the prescribed insulin despite the fact that they have to inject it several times per day [9, 10].
Treatment with intensive insulin can lead to a high risk of hypo glycemic events and this is particularly observed when one or more than one dose is used during the day. The risk prevents the efforts of tight glycemic control and can cause patient anxiety [9, 10].
Need of Advanced Drug Delivery System as Micro-needle
2.1 Avoidance of first pass metabolism
The key advantage of using micro needles is the fact that they do not experience hepatic first pass metabolism of the orally administered drug. This contributes towards better bio-availability and lower doses can be used with the same therapeutic effect as oral drugs [11, 12].
2.2 Minimally invasive administration
Micro needle technology provides an opportunity of painless skin puncture, but not piercing of the stratum corneum, which is the greatest obstacle to trans-dermal drug delivery. It minimizes pain with traditional subcutaneous injection and, therefore, is better than patients [12].
2.3 Controlled and sustained release
Insulin micro needle patches can be developed such as controlled and sustained release of insulin that improves glycemic regulation in diabetic patients. Drug loading flexibility provides the possibility to dose the drug correctly based on the needs of individual patients [12].
2.4 Enhanced stability of drugs
The formula used in micro needle patches can protect the sensitive drugs like insulin against destruction. Micro needle Dissolution can be used to store insulin in a biodegradable polymer matrix which maintains insulin in a stable form until the time of administration [12].
Microneedle in Drug Delivery System
A Micro-needle drug delivery system may thus be defined as a new approach of drug delivery where the needles inject the drug into the systemic circulation and may consequence in an easy entryway of the desired molecules into the body. The system where micron sized needles penetrate the top layer of the skin and diffuse to the epidermis layer which is later transported into the blood capillary area becomes active by taking in the drug since it reaches the location without causing pain to the patient as micro needles are short and long. This may be done through the use of Micro fabrication technology [13]. Microneedle patches also consists of a layer of adhesive which is applied to stick on the skin as well as the needles that pierce the skin to assist in the delivery of drugs [14].
Concept of Combining Herbal Bioactives with Microneedle System
Introduction of herbal bio-actives like Gymnema sylvestre, Trigonella foenum-graecum and Momordica charantia into the micro-needle systems is a new method of improving the efficiency of drug delivery [15]. These antidiabetic and metabolic regulatory medicinal plants have poor oral bioavailability and stability as a result of gastrointestinal degradation and first-pass metabolism, and can be delivered by microscopic projections (microneedles) that penetrate the stratum corneum without accessing the pain receptors. This enables direct systemic absorption, controlled release and better patient compliance. Incorporating herbal extracts to Microneedle patches has the potential to enhance therapeutic efficacy in managing diabetes. Therefore, integration of herbal bioactives with Microneedle technology will create a promising non-invasive patient friendly format of chronic disease management [16, 17].
Aim and Scope of the Review
Innovative and Non invasive method of managing diabetes; herbal based micro-needle patches, whereby ability to improve patient compliance is the objective. Future outlook on incorporation of herbal extracts in micro-needle devices with the objective of effective diabetes treatment is also discussed in this review.
Concept of Microneedle Technology
The diffusion mechanism is succeeded by the microneedle delivery system whereby the drug is administered by use of topical route through disruptive diffusion of surface over the skin temporarily. Hundreds of microneedles are spots of a patch and this helps to deliver sufficient
amount of drug that produces a therapeutic effect [18, 19]. The size of the needle should be optimized and should be restricted to a size of skin epidermis. In case the needles are excessively long and thick they may traumatize the nerves in the dermis area resulting in pain and discomfort [20]. The epidermis of the skin is 50-100um thick in general and local palm and sole 1500um. Typically, these microneedle have a sharp tip that measures between 150-1500 um in length, between 50-250 um in width and tip thickness between1-25 um [18]. The shape of microneedle tips may vary, such as pointed, pentagonal, cylindrical, triangular, Octagonal and numerous others [21].
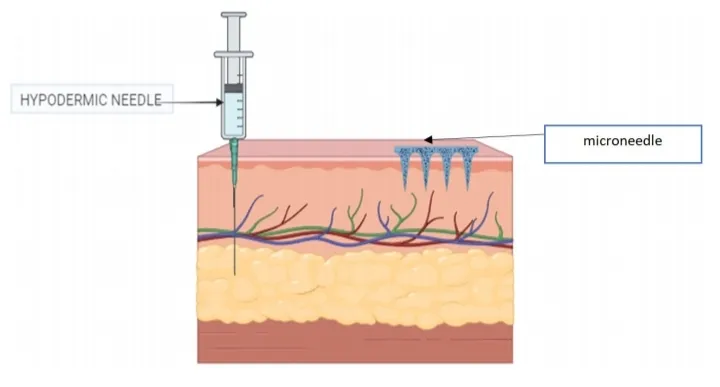
Fig. 1.1 Microneedles delivery system
Mechanism
Mechanism of Action of Microneedle in Insulin Delivery
Micro needles are the small and less invasive objects which pierce the outermost layer of the skin or stratum corneum. They create micro channels, in which insulin may be directly injected into the dermis, where it may be absorbed into the blood. The micro needles break down quickly upon insertion releasing insulin payload. Substances like starch and gelatin are generally used because they are biocompatible and dissolve rapidly in the interstitial fluid of the skin hence offering effective and efficacious delivery of insulin [22.]. The mechanisms of micro-needle devices which react to glucose are fitted to enhance the amount of insulin released as per the present concentration of glucose in blood. The application of hypoxia-sensitive vesicles is one of them. These vesicles would secrete insulin in case there is an increase in the blood glucose level. The concept of such a mechanism is to mimic the natural functioning of the pancreas which releases insulin when the blood glucose level is high. The hypoxia-sensitive vesicles are sensitive to the changes in the oxygen levels of the body, which are associated with high blood glucose. In case of high blood glucose, vesicles chemically transform resulting in the release of insulin at the action site. This glucose sensitive technology would be able to regulate the level of blood glucose much better reducing the risk of hyperglycemia and hypoglycemia. The micro-needles have low oxygen sensitive vesicles. Metabolism of glucose in the region forms a hypoxic (low oxygen) environment. This causes the vesicles to secrete insulin in a regulated way that makes sure that when the insulin is needed, it is released based on the oxygen levels in the locality [23].
Advantages of Microneedles in Insulin Delivery
1. Micro-needle patches are designed to penetrate the skin dermal layer without causing pain or blood loss, which makes them more acceptable than the traditional needles. The micro-needles are small and have a design that ensures that they are less intimidating and more acceptable to the users, which in turn may lead to improved compliance to the treatment of insulin.
2. The patch uses a bio-sensor based on graphene to detect glucose levels and release insulin, and an electro osmotic micro-pump delivers insulin in a controlled and stable way to regulate glucose during the long term period [24].
3. Microneedles have a high bio-availability of insulin of approximately 98.8% compared to most bioavailability with injections or oral administration. They do this through the direct delivery of insulin into the skin by bypassing the first-pass metabolism of the liver, which maintains its potency. This results in the more effective control of glucose using low doses and reduced frequently.
4. Various types of micro-needle structures such as hydro-gel and dissolving insulin are available to allow a customized insulin-release profile to meet the needs of diverse diets. The use of innovations like microneedles that are thermo sensitive can also deliver insulin depending on the level of blood glucose thereby providing a reactive treatment remedy [25].
Types of Microneedles
Micro-needles are very small needles that are applied in different ways, mostly during drug administration and diagnostics. Micro-needles are available in five major types with specific characteristics and use:
3.1 Solid Micro-needles
This type of needle permeates the skin making micro incisions whereby drug solutions seep into the skin. They are simple to produce, but they may cause infections when they are not handled. It is applicable as drug delivery agent and cosmetics agent [26].
3.2 Coated Micro-needles
These are coated with a drug that dissolves when placed in the skin enabling the drug to be absorbed. They make the application process easy and have restrictions in the quantity of drug they can impart as a result of the thin layer [27].
3.3 Hollow Micro-needles
These needles have a hollow canal that can receive the direct delivery of drugs out of the reservoir. They are capable of delivering bigger doses though they might have 3. problems such as leakage and clogging. They have common application in disease diagnosis [28].
3.4 Dissolvable micro-needles
These needles consist of such materials as sugar or polymers and are dissolved in the skin when the needle is inserted releasing the drug they carry. They are useful in the delivery of vaccines and cosmetic treatments and are more complicated to produce [26].
3.5 Hydro-gel-forming micro-needles
These distend when in contact with the body fluids that results in the quick development of hydro-gel that promotes the release of drugs. In comparison to dissolvable microneedles, they do not dissolved, so they stay there until taken off together with the patch. They are appropriate in the delivery of hydrophilic drugs [29].
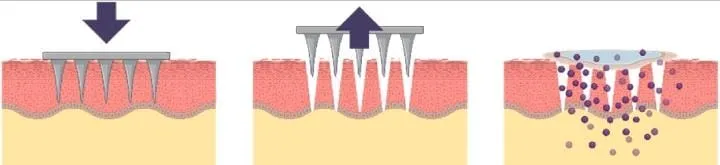
Fig. 1.2 Solid microneedle
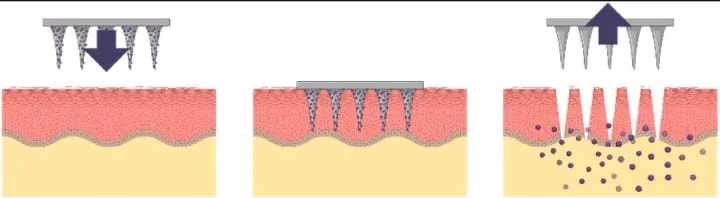
Fig. 1.3 Coated microneedle
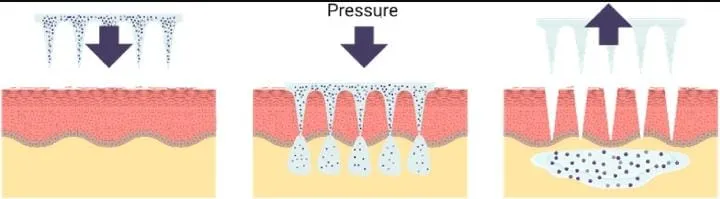
Fig. 1.4 Hollow microneedle
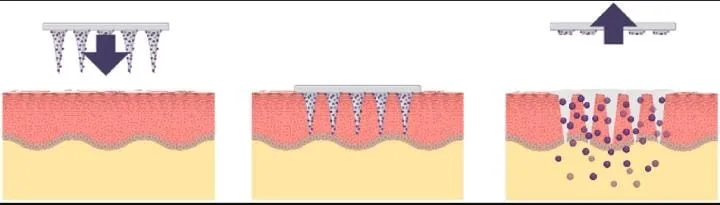
Fig. 1.5 Dissolving microneedle
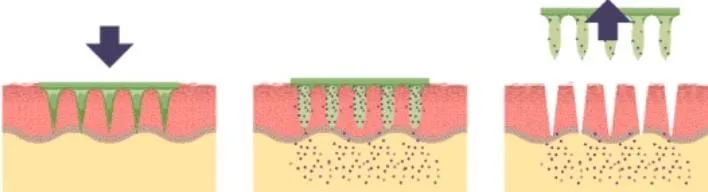
Fig. 1.6 Hydro-gel microneedle
Table 1.1 Overview of types of microneedles [29]
|
S. No |
Microneedle types |
Characteristics |
Advantages |
Disadvantages |
Application |
Materials |
|
1 |
Solid microneedles |
Creates channel in the skin to allow drugs reach the lower skin layer. Adequate mechanical strength. Sharper tips. |
Allow more drugs to pass into the skin. Easy to manufacture. |
Damage to the skin and micro incisions need to the closed to avoid infection. |
Drug delivery. Cosmetics |
Silicon, metal, polymers |
|
2 |
Hollow microneedles |
Empty shape to be filled with the drug. Ability to control drug release over time. |
Handles a large dose /amount of drug solution |
Weak needles. Requires intensive care in terms of needle design and insertion method. Might cause leakage and clogging. |
Disease diagnosis. |
Silicon |
|
3 |
Coated microneedles |
Carries less amount of the drug due to design. Ability to deliver the proteins and DNA in a minimally invasive manner. |
Deliver the drug quickly to the skin. |
Prone to infection. |
Drug delivery. Vaccine delivery |
Silicon |
|
4 |
Dissolving microneedles |
Facilitates rapid release of macromolecules. |
Ease of administration for patients with one step application. |
Requires technical expertise to manufacture. Takes time to dissolve |
Drug delivery. Cosmetics. Vaccine delivery. |
Polymer |
|
5 |
Hydro-gel microneedles |
Bio ompatibility, control release, non-invasive application |
Sustained and control drug release, minimally invasive and painless |
Insufficient mechanical strength, toxicity from crosslinking agent, variable swelling and degradation |
Skin and chronic disease, vaccine delivery |
Polymer |
Herbal Bioactives With Antidiabetic Potential
Plant-derived phytochemical have potential to serve as insulin mimetics, i.e. agents that replicate the effect of insulin, and as beta cell protective/ regenerative agents, reduce beta cell oxidative stress and promote regenerative. Insulin resistance and progressive beta cell dysfunction characterizes type 2 diabetes, and multi-target phytochemicals have the potential to enhance insulin signalling and protect beta cell simultaneously, becoming interesting complementary agents [30].
Mechanism of action
Many extract enhance insulin signalling or stimulate GLUT-4 recruitment in muscle/adipose, increasing glucose uptake.
Some botanicals stimulate insulin release directly example: Gymnema.
Preclinical reports of increased beta cell proliferation or expression of beta cell transcription factors after treatment with specific extracts [31, 32].
Gymnema Sylvestre
Gymnema sylvestre is considered as one of the plants with strong anti diabetic effect. Gymnema tea is also used as a control measure of obesity using this plant. The active ingredient of the plant is a complex of acids, called as gymnemic acids. It is seen that a potential association may be present between obesity, Gymnemic acids and diabetes. The plant is native to central and western India, tropical Africa and Australia. Other names in Tamil: Adigam, cherukurinja [33]. It is a powerful antidiabetic herb and is applied in folk, ayurvedic, and homeopathic medicine. Also, it is applied in treating asthma, eye conditions, inflammations, and snakebites [34]. Moreover, it has antimicrobial, anti hypercholesteroleic, hepato protective and sweet suppressing properties. Gymnemic acids are antidiabetic, anti inflammatory and anti sweetener. It was later found that the anti diabetic array of molecules is a family of closely related gymnemic acids having been successfully isolated and purified in the leaves of Gymnema sylvestre [35, 36].

Fig. 1.7 Gymnema Sylvestre
Mechanism of action of Gymnemic acid
Gymnema sylvestre is a plant leaf that has been known to induce hypoglycemia in laboratory animals, and has been used in herbal medicine to treat adult onset diabetes mellitus (Type 2). The administration of the Gymnema leaf extract to a patient with diabetes has been shown to stimulate the pancreas due to which an increase in the faecal excretion of cholesterol has been found [37], although more research is needed to demonstrate their clinical importance in managing hypercholesterolemia (high serum cholesterol). Other applications of the Gymnema leaf extract include the fact that it is used as a laxative, diuretic, and cough suppressant. These other processes would be regarded as the adverse reactions in case of involving Gymnema in its glucose lowering action in diabetes:
1) It enhances secretion of insulin.
2) It induces repair of islet cells.
3) It enhances the use of glucose: it is demonstrated to stimulate the work of enzymes to use glucose through insulin-independent pathways and thus the activities of phosphorylase, the decrease of gluconeogenes enzymes and sorbitol dehydrogenases.
4) It brings about an inhibition of intestinal glucose absorption. The gymnemic acid ingredients are thought to inhibit the glucose absorption in the small intestine in the mechanism that is not well known. It might be engage one or more mechanisms [39].
Bioactive anti diabetic compounds
In Gymnema sylvestre metabolites are found in secondary forms. These are oleanane saponins and dammarane saponins. There are two types of oleanane saponin i.e. gymnema saponins and gymnemic acid saponins. Gymnemasaponins are made up of two a-glycone saponins such as gymnemagenin and gymnestrogenin [40]. Gymnemasides [41, 42] are dammarane saponins. These antidiabetic properties belong to all these secondary metabolites. Other than these triterpenoid saponins and other antidiabetic compounds are anthraquinone, flavones, flavonoid such as epicatechin, apigenin, luteolin, phytin, resins, tartaric acid, formic acid, butyric acid, lupeol, bamyrin related glycosides [43]. An athraquinones and their derivatives, alkaloids- conduritol, gymnamine, a and b chlorophyll, polypeptide (Gurmarin), d-quercitol, stigma sterol, nonacosane, parabin, calcium oxalate, cellulose, lignin etc. also have antidiabetic potential [44, 45].
Table 1.2 Gymnema sylvestre and their mode of action
|
S. No |
Bioactive anti diabetic compound isolated from gymnema sylvestre |
Mode of action |
Reference |
|
1 |
Oleanane |
Hypoglycemic activity |
[46] |
|
2 |
Gymnemic acid |
Reduction of blood sugar because gymnemic acid molecules fill the receptors location in the outer layer of intestine, thereby preventing sugar absorption in intestine |
[47] |
|
3 |
Gymnemasides |
Inhibitory effects on increased level of serum glucose |
[48, 49] |
|
4 |
Gymnemasaponins [gymnemagenin and gymnestrogenin] |
Hypoglycemic activity, B cell regeneration Gymnemagenin inhibits glucose absorption |
[50] |
Momordica Charantia
Bitter melon or Momordica Charantia is a common plant that is consumed by the indigenous people of the Asian continent, South America, India, the Caribbean and East Africa as a form of treating diabetes related conditions [51, 52]. The fruit possesses a characteristic bitter flavour much stronger in succession of growing older, therefore the name bitter melon or bitter gourd. Momordica Charantia has demonstrated strong antidiabetic effects and strong hypolipidemic effects such that it can be employed as an adjuvant together with allopathic treatment of medicine to treat diabetes as well as to prevent the late complications of diabetes [54]. Phenols, flavonoids, isoflavones, terpenes, anthroquinones, and glucosinolates are among those that contribute to its bitter flavour giving bitter melon medicinal value because of their high antioxidant properties [55].

Fig. 1.8 Momordica Charantia
Polypeptide-p
One of the most widely used vegetable, which contains polypeptide-p and is used in the control of diabetes in a natural manner, is Polypeptide-p Bitter melon [56]. Polypeptide-p or p-insulin is an insulin like hypoglycemic protein, which has been demonstrated to reduce the level of blood glucose in gerbils, langur and human beings when injected subcutaneously [57]. The p-insulin is initiated by the action of human insulin in the body and can therefore be utilized as an insulin replacement in patients with type-1 diabetes is a plant based insulin [58]. It has been recently cloned and expressed the 498 bp gene sequence of the Momordica Charantia polypeptide p gene and Wang et al. have also demonstrated the hypoglycemic activity of the recombinant polypeptide in alloxan induced diabetic mice [59]. The oral administration of bitter melon seeds extract does exert hypoglycemic effects in streptozotocin (STZ) elicited type-1 diabetic rats. This suggests that bitter melon seeds have other compounds that can be also involved in the treatment of type-1 diabetes besides the p-insulin [60].
Anti-diabetic effect of Momordica charantia
Momordica Charantia and its several extracts and constituents have been speculated to implement their hypoglycemic actions through various physiological, pharmacological and biochemical mechanisms [61, 62]. Hypoglycemic effect [63, 64], stimulation of peripheral and skeletal muscle glucose utilisation [65, 66], intestinal glucose uptake inhibition [67, 68], adipocyte differentiation inhibition [69], suppression of major gluconeogenic enzymes [70, 71], HMP pathway stimulation [70], and islet 0 cell and functions preservation [72] are the possible modes of the hypoglycemic actions of Momordica Charantia. The anti-hyperglycemic and hypoglycemic effects of the various extracts and components in Momordica charantia have been studied in more than 140 studies on the world today [73, 74, 61]. MomordicaCharantia has been identified to have a strong neuroprotective effect against global cerebral ischemic perfusion caused neuronal injury and resultant neurological impairment in diabetic mice [75]. A negative insulin signal regulator, protein tyrosine Phosphatase 1B (PTP1B) has been a possible therapeutic target in treating type 2 diabetes [76].
Momordica Charantia and glucose metabolism
Insulin has a significant biochemical effect of stimulating the uptake of glucose by various body cells in the production of energy [77, 78]. Momordica Charantia has direct effect in inhibiting the activities of fructose 1, 6diphosphatase and glucose-6-phosphatase and at the same time inducing the action of glucose-6- phosphatase dehydrogenase [79].
Mechanism
To start with, it has the ability to control the amount of glucose the gut releases into the blood after a meal and secondly it can increase the uptake of glucose by the skeletal muscle cells similarly to that of insulin. In addition, it appears to have its action through the same intracellular signaling pathways as insulin in the control of glucose metabolism within the body [80].
Advantages of Herbal Extract
Natural origin
The plants are used to produce herbal extracts and hence are abundant in naturally occurring bioactive compounds like alkaloids, flavonoids, terpenoids, saponins and phenolic acids. The fact they are naturally produced implies that they are better compatible with the human body as opposed to synthetic agents. Also, as renewable and biodegradable, they are environmentally friendly. Also, the history of traditional use of medicinal plants among cultures facilitates their safety and efficacy profiles [81].
Synergistic effect
Depending on the type of herbal extract, there can be many phytoconstituents, unlike synthetic medications which often have one active ingredient, which will work together in a synergistic manner. These elements have the ability to attack multiple biochemical pathways at once, which increases the overall treatment effect. An example is that antioxidant, anti-inflammatory, or antidiabetic effects of herbal formulations are more effective with the combination of flavonoids and saponins than with isolated compounds [82].
Minimal side effects
Herbal extracts have fewer adverse reactions than conventional synthetic drugs mainly because they are naturally composed and have a long history of use by man. Patients can more easily tolerate them especially in long-term treatments. Moreover, administration of whole plant extracts will aid in maintaining a balanced pharmacological profile, which can minimize the chances of toxicity that can be caused by the administration of pure compounds in large doses [83].
Formulation Design of Herbal Based Microneedle Patches: Development of The Microneedle Selecting The Base Material
The microneedle matrix is usually based on biocompatible polymers like hyaluronic acid, gelatin or polyvinyl alcohol since the materials are readily degradable, possess easy dissolution properties and can be used to make dissolvable or biodegradable microneedles [84].
Incorporating Herbal Extracts
Add 100g Herbal Extracts to the mixture. The agents are the herbal extracts which are added to the base polymer in either solution form or as a dispersed solid. Herbs and concentrations are selected to address the desired therapeutic effect, e.g. wound healing, anti inflammatory effect or targeting microbial infections.
To Prepare a Homogenous Mixture
The herbal extracts and the base polymer are combined to achieve a homogenous performance and dosage. The step is essential to attain a uniform distribution of the active components in the microneedle matrix [85].
Materials
The main development of microneedles is that they will be able to penetrate the skin and they will not bend or break. In order to overcome the difficulties related to microneedle fabrication, the material used, manufacturing methods and design of structure has been widely examined Micro needles have been made using numerous materials such as silicon, metals, ceramics and polymers to name but a few. The hybrid versions of these materials have also been used to achieve better results in biomedical applications namely drug delivery, tissue engineering, and the development of medical implants [86].
Silicon
Micro needles were initially made out of silicon in the 1990s. Silicon has a number of benefits among them being natural flexibility and the ability to be constructed into different shapes and sizes with no trouble It has also been extensively exploited to make solid micro needles, hollow micro needles and coated micro needles. Nevertheless, silicon-based microneedles have drawbacks, including the time-consuming fabrication procedures, and great chances of fracturing under the skin when using these needles [87].
Metals
Microneedle fabrication is largely based on the use of metals because of their good mechanical characteristics and biocompatibility. They are more robust and less likely to break the silicon they are also more resistant to fractures due to their high fracture toughness and yield strength. Microneedle development used stainless steel then titanium as the most common metal. Although it is effective in skin penetration, metal microneedle can cause cases of allergy in others [88].
Ceramic
Micro needle fabrication has utilized ceramic materials, such as alumina, calcium sulfate dihydrate, and calcium phosphate dihydrate due to their good chemical stability and high compression property. Such materials are susceptible to micro-molding methods that can be used to sustain scalable and cost-efficient production. Ceramics such as alumina do not however have high tensile strength and it has been shown that microneedles made out of such materials may fracture when inserted manually into the skin [89].
Polymer
Micro-needles made of polymers are gaining momentum in the fabrication of microneedles because of their great biocompatibility, low toxicity, and the low cost. Polymers are particularly immune to mechanical limitations because they are weaker than silicon and metals, and are particularly useful in designing dissolvable and hydrogelforming arrays of microneedles. They are also applicable to solid, coated and hollow types of microneedles. Biodegradable polymers like poly methyl methacrylate, polylastic acid, polycarbonate, polystyrene, and SU-8 photo resist have been utilized in the delivery of various drugs through the skin hence it is useful in transdermal therapeutic use [90].

Fig. 1.9 Schematic diagram of microneedle material of construction
Plasticizers and stabilizers
4.1 Plasticizers
Polymer Plasticizers like glycerol, sorbitol, are also added to minimize brittleness and increase the elasticity of polymeric network example: chitosan, or hyaluronic acid. They operate by suppressing the intermolecular forces between polymer chains thus enhancing mobility and flexibility of the matrix. This alteration contains the cracking in the process of microneedle drying and insertion [91].
Glycerol
A biocompatible plasticizer is a polyhydric alcohol that is frequently used. Glycerol improves the mechanical strength, flexibility, and moisture retention, and it is particularly significant in the case of hydrophilic polymers such as poly vinyl alcohol, poly vinyl pyrrolidone. It also assists in keeping the needles sharp and it does not fracture when they penetrate the skin [92].
Sorbitol
Sorbitol is another sugar alcohol that is applied as a plasticizer and humectant and enhances the integrity and stability of microneedles by maintaining a sufficient level of moisture content. It gives it a smoother surface and helps in uniform distribution of drugs or herbal extracts through microneedle matrix [93].
4.2 Stabilizers
Glycerol and sorbitol are both capable of stabilising bioactive herbal compounds and serve to protect them against drying, oxidation or changes in temperature. They are hygroscopic, which preserves the hydration condition of the delicate phytochemicals and guarantees extended shelf-life as well as uniform liberation action [94].
Preparation Methods
Solvent Casting Micro Molding
The most widespread technique to make dissolving microneedles is solvent casting micro-molding where no extra heat is needed and thus dissolving microneedles can be utilized to deliver heat-sensitive proteins and peptides [96]. Moreover, the fairly easy production of dissolving microneedles can also be implemented at an industrial scale and is beneficial to the production of protein-based microneedles [97]. Dissolving microneedles are commonly prepared by pouring a liquid formulation into a prepared microneedle mold [98]. Laser machining has been an eminent alternative or complementary technique to lithography-based microfabrication in the late 1980s. Carbondioxide lasers are typically employed to fabricate prototypes quickly and at low cost, and in microfabrication. The micro channel engraving has been effective in the production of microfluidic devices. Also, laser drilling can be termed as ablation, a conventional method of producing arrays of microstructures, e.g. concavities or through-holes, in a variety of industrial and research applications [99].
This process is effective, easy, and efficient in saving time hence more appropriate in mass production and more economical than other technologies. Specifically, it is a good choice in sugar and polymeric microneedles [100]. As such, mold filling techniques are required to defeat surface tension. Researchers have come up with various processes among them being vacuum-assisted processes, centrifugation, spinning coating, imprinting, infiltration and atomized spray to address this challenge of filling a mold. Micromolding has limitations regardless of these attempts. It finds it difficult to form complicated structures like the adhesive structure with barbs or hollow structure. Moreover, the stress of demolding may possibly harm end structures especially soft and delicate ones such as hydrogels. Besides, it cannot process materials like metal, silicon and glass through this technique [101]. The solvent-casting micromoulding process is divided into two types in the development process which are onestep and two-step casting.
One step casting
Microneedle manufacturing process can be dissolved and a single step can be used to cast the micromoulding which is known as one step casting micromoulding. Cast polymer solution containing the active substance into the polydimethylsiloxane molds and centrifuged or vacuum dried [102]. Prepared insulin filled dissolving microneedle with GantrezTM AN-139 polymer one-step casting method. The insulin at 2.5 and 10mg was combined with the GantrezTM aqueous solution, poured in silicone moulds, centrifuged and dried at room temperature in 24 hours. Micro needles of insulin were put on the skin of neonatal porcine and it was found that at doses of 2.5mg and 10mg insulin in 1 dissolving microneedle only 40% and 55% of the insulin in whole dissolving microneedle was delivered, respectively. As a result of this finding, the author mentioned that the insulin that was in the needles entered the skin, but the insulin in the base plate was not administered. This was due to the fact that the microneedle base plate was no longer in the dried form as it turned into a gel after 24 hours and no holes in the skin were observed after 24 hours [103].
Two step casting
To eliminate the issues brought about by one-step casting, it is best to design a technique whereby the active substance will solely be concentrated at the tip of the microneedles or needles referred to as two-step casting. In this procedure, two sets of polymer mixtures will be prepared, the first solution will contain both polymer and active substances, and the second solution will contain purely blank polymer, i.e. devoid of active substances. The initial water-based polymer solution will be transferred into poly dimethylsiloxane molds and dried, and the second water-based polymer solution will be added on the top of the former one in such a way that the active substance will only be concentrated in the needle. This will save on waste of drugs since the drugs incorporated in the base plate are not wasted [104]. Exenatide is one such peptide that is incorporated in the dissolving microneedles system through the two-step casting method [105].
3D Printing
The two-photon polymerization process which involves the use of two-photon absorption in triggering polymerization was the first photopolymerization technique that was utilized in the fabrication of the microneedles. This stereolithography method can print microneedle arrays that have excellent resolution, a good printing quality and have a high level of accuracy. In recent researches, the two-photon polymerization is implemented in the direct and indirect production of microneedle arrays. Cordeiro et al. revealed the fabrication of the three-dimensional structures by the two-phyton polymerization technique as they created templates of various shapes and sizes and fabricated dissolvable and hydrogel forming micro-needles with another type of microfabrication known as micro-molding [106].
There are other types of photopolymerization techniques that can be used to 3D-printing of microneedles. Laser or light-emission technologies can also be used instead of the two-photon absorption of the polymerization of materials in order to accomplish the same purpose of polymerization that is Digital light processing, Continuous liquid interface production and laser stereolithography. The micro-molding of biodegradable microneedles can be developed further by obtaining the direct printing of the molds with the laser stereolithography method. The polymer microneedles coated anti-cellulite herbal product was also studied, characterized, and pharmacologically tested [107]. Following a similar method, 3D- printed masters of micro-needle which were produced and recapsulated into molds using cheap and fast production methods. These scientists could reproducibly and customize recombinable microneedle molds [108]. Three-dimensional-printed cone-shaped microneedles were directly produced one step [109]. There was a fabrication of a heterogeneous mixing and transport of fluids using microfluidic-enabled hollow microneedles. This research led to the implementation of hollow microneedles in the delivery of various drug formulations through the transdermal routes by creating microchannels on the human skin using the patch of microneedles manufactured by one-step laser stereolithography [110].
It has been found out that the human skin which has been treated with microneedles has a comparatively enhanced permeability [111]. Microneedles are needles measuring height of 25-2000 mm with a height of 25-2000 m. All the 3D-printing technologies can be used to manufacture the microneedles of the above-mentioned range in a repeatable way with a high level of quality and resolution. Depending on the material and the type of application, one can use a specific 3D-printing technology. As it has been mentioned above, there are four different types of microneedles: solid, hollow, coated, dissolvable, and hydrogel-forming microneedles. Table 1.3 demonstrates the various forms of 3D-printing technologies depending on the type of the microneedle, the smallest resolution of the layer, and the type of application. The optimal features of the 3D-printed microneedle are the optimal size, the adequate mechanical stability, the efficient drug delivery, and the capability to be leak-free [112, 113]. The figure of scanning electron microscopy of the microneedles fabricated using the various kinds of 3D-printing technologies is depicted in table 1.3
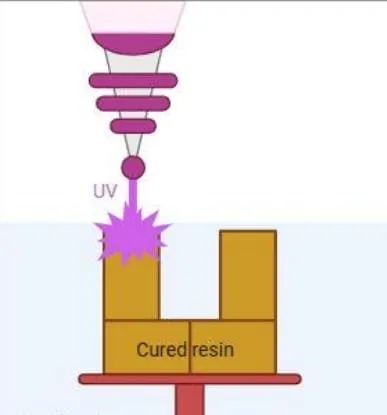
Fig. 1.10 Schematic diagram of stereolithography 3d printing process
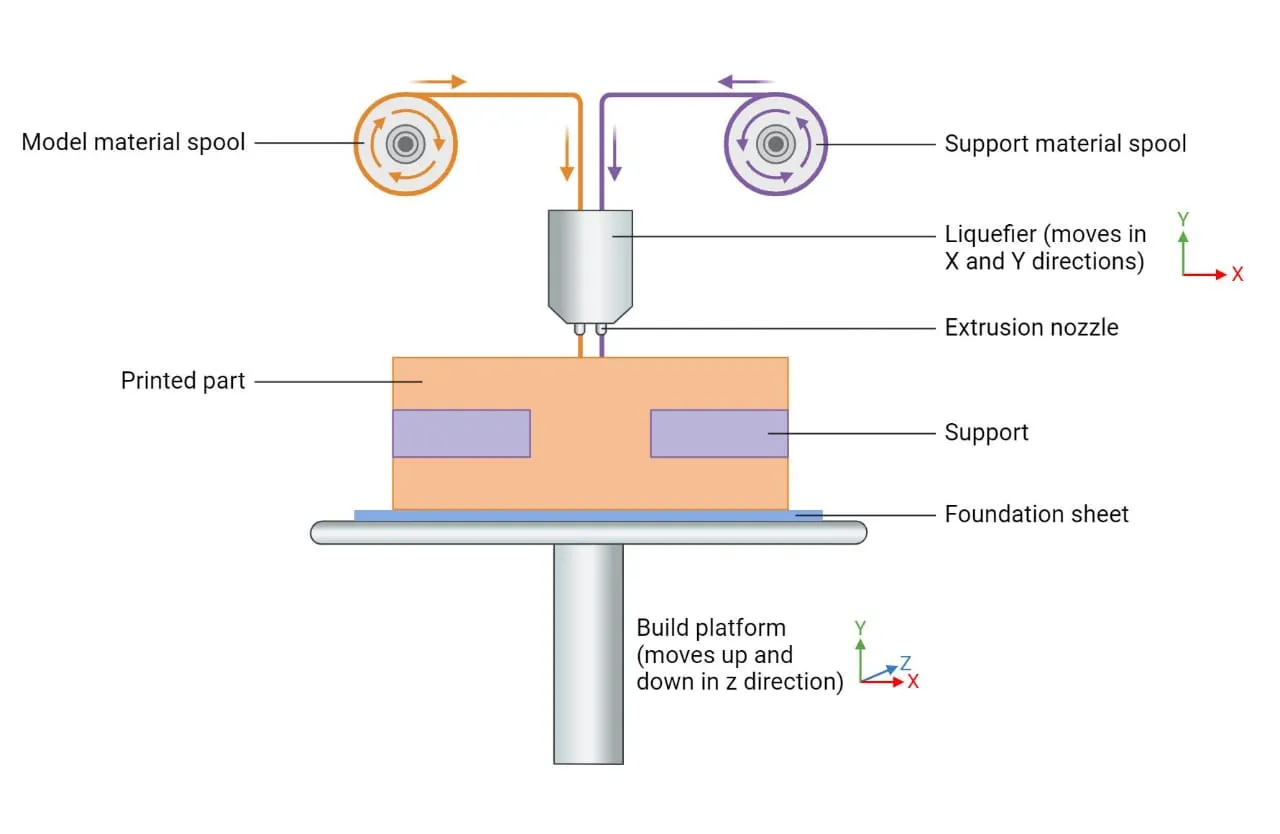
Fig. 1.11 Schematic diagram of fused deposition modelling 3D printing
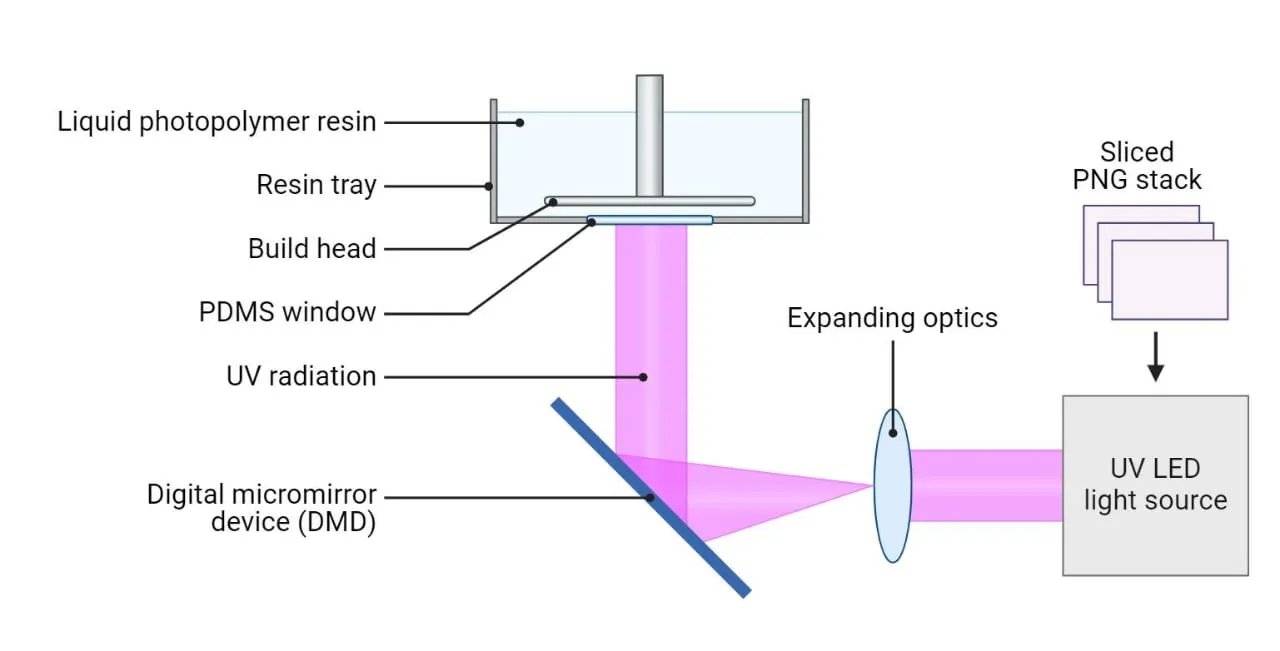
Fig. 1.12 Schematic diagram of digital light processing 3D printing
Table 1.3 Different 3D printing technologies used for the fabrication of microneedles based on the microneedle type and application [112, 113, 114]
|
S. No |
Technology |
Microneedle type |
Minimum layer resolution |
Power source |
Application |
|
1 |
Stereolithography |
Solid, hollow coated |
50-100 µm |
UV light |
Drug and anticancer agent delivery |
|
2 |
Selective laser sintering |
Solid, hollow |
80 µm |
Laser beam |
Drug delivery and disease treatment |
|
3 |
Digital light processing |
Solid, hollow, coated, hydrogel |
25-150 µm |
UV light |
Skin treatment, wound healing, drug delivery |
|
4 |
Fused deposition modelling |
Solid |
10-100 µm |
heat |
Transdermal drug delivery and insulin |
|
5 |
Continuous liquid interface production |
Solid,coated,hyd rogel |
50nm-100µm |
UV light |
Drug delivery,Diagnostics |
|
6 |
Two photon polymerization |
Solid, hollow |
100nm-5 µm |
UV light |
Drug delivery, blood extraction |
Fabrication
These methods are applied either separately or together to form implantable biomedical device. Implants are usually micro fabricated in silicon or other similar substances as they are easy to produce. Once the demonstration of concept has been presented, the implant can then be reshaped to be cast in other materials through methods like micromolding. The most widespread method of fabrication is micromolding of microneedles. Polymer casting is done in this technique with negative elastomeric polydimethylsiloxane mold to make microneedles [115].
3D Printed Microneedle patches Filling with polydimethylsiloxane Drying in the oven


Filling with polymer mixture Centrifugation and drying Ready to use Dissolvable Patches
Table 1.4 Fabrication methods of microneedles [115]
|
S. No |
Methods of fabrication |
Types of microneedles produced |
|
1 |
Micromolding and melt casting |
Dissolvable, hydrogel forming |
|
2 |
Dipping |
Coated type |
|
3 |
Photo lithography |
Dissolvable, hydrogel forming, hollow type |
|
4 |
Metal electoplating |
Hollow type |
|
5 |
Dry etching |
Hollow type |
|
6 |
Micro stereo lithography |
Metallic |
|
7 |
Continuous liquid interface production |
Coated type |
Mechanism Of Drug Delivery And Action
The mechanism of drug delivery and action are described in the following way Drug permeation through microneedle-created microchannels, Controlled and sustained insulin/herbal release, Enhanced bioavailability compared to topical or oral routes, Dual mechanism: herbal bioactives and insulin co-delivery to improve glycemic control.
Microneedle created micro channel
The insertion of the microneedles into the skin surface forms micro pores or microchannels of depth 10-200 µm depending on Microneedle geometry, material and force of insertion. Contrary to hypodermic needles, microneedles do not approach the nerve ends or blood vessels hence giving the administration of the drug without any pain. The formed microchannels interfere with the lipid-enriched structure of stratum corneum and establish aqueous pores in which drug molecules are allowed to transverse [116]. These microchannels stay open over a few hours and they ultimately close because of the skin restoration processes in the form of migration of keratinocytes and production of lipids in the barriers. Drug Permeation Pathways: Drugs passed through the microneedle created microchannels using a concentration found between the formulation and the interstitial fluid within the skin using a concentration gradient which is the first law of diffusion according to Fick. Convective Flow and Capillary Action: When the skin and microchannels become moist, the diffusion process of dissolved drug molecules is enhanced, and it moves deeper into the dermal tissue. The pathways formed by microneedles, to a large extent, enhance the permeability coefficient and lower the resistance to diffusion and thus maximize flux when compared to intact skin [117].
Factors Affecting Drug Permeation: Several parameters control the level of drug permeation by the microneedlecreated microchannels: Microneedle Geometry and Material: The length, tip sharpness, density of needles and materials (metal, silicon or polymer) determine the level of needle insertion and the depth of the pore. An example is polymeric dissolving microneedles which are capable of sustained release due to dissolution in the skin [118]. Drug Properties: The Molecular size, charge, and solubility determine the ease with which the drug diffuses through the aqueous channels. Insulin and peptides, as well as vaccines, are some of the examples of macromolecules with increased permeation relative to standard patches. Formulation Design: Coated or encapsulated microneedles release the drug when exposed to interstitial fluid. Microneedle swelling Hydrogelforming microneedles swell to create a controlled drug release environment [119].Skin Recovery Time: The microchannels do tend to close within 24-72 hours, depending on skin site and depth of microneedles, which amplifies the length of enhanced permeability [120].
Controlled and Sustained Insulin Release
Polymers that are derived out of herbs are also significant in the regulation of drug release of microneedles. Chitosan is a natural polymer of chitin and can offer good film-forming and muco-adhesive characteristics as well as biocompatibility. Microneedles based on chitosan allow indirect, extended (up to 24 hours) release of insulin or phytochemicals because of the adjustment of its molecular weight or mild crosslinking [121]. On the same note, guar gum and alginate are employed due to their gelling and swelling properties to create diffusion controlled matrices that release drugs in a prolonged fashion. Gum acacia and derivatives of starch have also been used to control hydration and degradation rates therefore regulating the release kinetics of herbal actives [122].Individual phytoconstituents have also been investigated to be used as sustained release in diabetes therapy. Berberis aristata (is an isoquinoline alkaloid called berberine) acts as an activator of the AMPK pathway and enhances insulin sensitivity. Incorporated into HA -chitosan Microneedles, berberine showed prolonged dermal release and increased pharmacological activity [123].
Curcumin is a polyphenolic compound that is found in Curcuma longa; it exhibits antioxidant and beta cellprotective properties; the addition of curcumin to the nanocarrier-loaded PVP Microneedles would allow a constant release of this compound up to 48 hours, eliminating the burst effect [124]. Likewise, flavonoid quercetin of Moringa oleifera or Allium cepa and resveratrol of Vitis vinifera have been successfully loaded to produce bi phase or sustained release curves in Microneedles to provide short- and long-term glycemic regulation results [125]. Indicatively, Microneedles patches comprising of insulin plus extracts of Gymnema sylvestre delivered an initial insulin spurt and a prolonged herbal discharge, which has shown to be a great way to offer effective postprandial as well as basal glucose control [126]. Likewise, the concurring effect of Insulin with curcumin or fenugreek extracts in polymeric Microneedles led to an increase in antioxidant and hypoglycemic effect [127].
Enhanced Bioavailability
Physical Microneedle patches circumvent stratum corneum by either making micron size punctures or injecting drug into viable epidermis or dermis. This bypasses first-pass hepatic metabolism and a lot of digestive enzymes and results in much higher fractions of the nominal dose to reach the local capillaries and lymphatics thus better systemic bioavailability. Systemic bioavailability of phytochemicals which would otherwise be rapidly metabolised is also increased by avoidance of gastrointestinal degradation and hepatic first-pass metabolism [117]. Most phytochemicals such as poly phenols, alkaloids, saponins and peptides exhibit a low permeability over intestinal membrane leading to low absorption by the systemic system and low therapeutic effect. Likewise, the traditional topical preparations like creams or gels have drawbacks because of the barrier characteristics of stratum corneum which inhibits the permeation of hydrophilic or high-molecular-weight substances. Consequently, it becomes challenging and unreliable to obtain herbal actives at their therapeutic relevant plasma concentrations by oral or topical administration [128].
Microneedle technology can offer an exciting solution to such problems, as it will make microscopic pores in the stratum corneum and direct delivery of herbal bioactives into the viable epidermal and dermal layers that have plentiful vascular and lymphatic networks. This transdermal system is particularly useful in bypassing gastrointestinal degradation and hepatic first-pass metabolism, rendering the system improved systemic absorption and bioavailability of the drug [129] in the case of gymnemic acids of Gymnema sylvestre, charantin and polypeptide-P of Momordica charantia, or 4-hydroxyisoleucine of Trigonella foenum-graecum, oral bioavailability is low, but transdermal delivery using microneedle systems Herbal-based microneedle patches can be used to increase the bioavailability of herbal antidiabetic agents in comparison with oral or topical preparations because it overcomes biological barriers to bioavailability of gastrointestinal and stratum corneum. They offer patient-friendly, efficient, and non-invasive route of delivery that enables the discharge of phytoconstituents in a rapid and sustained manner that ensure the maintenance of study therapeutic level and enhanced control of diabetes [130].
Dual Mechanism
Dual delivery of herbal bioactives and insulin by the use of microneedle patches is an up-and-coming technology in transdermal diabetes therapeutics, which is intended to treat several pathophysiological factors of diabetes mellitus, especially insulin inadequacy and insulin resistance, by means of a synergistic medication modality [131]. The exogenous insulin and herbal bioactive loading capabilities of these hydrophilic polymers, e.g., chitosan, hyaluronic acid, polyvinyl alcohol and polyvinyl pyrrolidone, provide both immediate and long-term benefits in glucose homeostasis due to the speed of glycemic control with exogenous insulin and the long-term metabolic modulation, antioxidant and protective effects of the biology on the 2 -cell [132].The polymeric matrices employed to produce the microneedle. As an example, insulin can be trapped into the tip of dissolving microneedles to release quickly at the beginning and herbal substances trapped in the bottom layer release slowly or slowly to keep the plasma glucose levels constant over a period. This two-way action also solves the problem of insulin stability [133]. Numerous herbal antioxidants, e.g. curcumin or quercetin, have the opportunity to stabilize insulin molecules by inhibiting aggregation and oxidative degradation processes during storage and administration. Besides, their local anti-inflammatory actions lower dermal irritation, which occasionally happens in repeated use of the microneedles [134]. Such a twofold system of protection does not only make patients comfortable, but also prolongs the life of patches and improves the overall results of the treatment process [135].
Evaluation And Characterization Of Microneedle Patches Microneedle Patch Morphology
Digital microscope is applied to examine the dimension and morphology of prepared patch such as length, width, height of patch and of the inter-space of patch and the microneedle patch. It then analyzed and the outcome compared with the master mold [136].
Weight variation
Three patches are picked and weigh each one separately through electrical balance to find the mean weight value [137].
Thickness uniformity
The drug content may be determined by placing the prepared patch of the microneedle patch in 100 ml of phosphate buffer with pH 7.4 within 30 min. Subsequently, the solution obtained is filtered and examined using the drug content [138].
Folding test
Folding test may be described as the folds that are obtained with no patch breaking, in case the folding was repeated in the same place. This is a triplicated test, to record the average of the value [139].
PH measurement
The patch is dipped into a glass vessel that has contained 10 ml of deionized water. Measurement of the pH is done by immersing the pH electrode in contact with patch surface during one minute to bring to equilibrium [140].
Percentage of moisture loss
Three patches are individually weighed and put in a desiccator with anhydrous calcium chloride over a period of three days at the room temperature. The patch is then reweighed again to determine the difference between the weights. Lastly, the loosing of moisture percentage is determined using the following equation PML = [( W0 0− Wt )/W0 ) × 100 W0= weight at the beginning, Wt= weight at the end [141]. Percentage of moisture absorbed Individual weighing of three patches is followed by placing it in a desiccator with saturated solution of potassium sulphate over a period of three days at room temperature. The patch is reweighed again afterwards [142].
Measurement of axial needle fracture force
The axial needle fracture force can be explained as the lowest force that acts against microneedle axis that leads to microneedles breakdown. This test is measured with TA texture analyzer. XT apparatus. A microneedle patch is inserted in this test, a microneedle patch is placed on an affixed cylinder platform, and the instrument programmed to compress the axially the patch of the microneedle. The highest force which apply instantly prior to patch deflection is deemed as the axial needle fracture force and the immediate force loss which is documented as a needle failure [143].
In vitro skin permeation study
In vitro skin permeation experiment was carried out by using a Franz cell diffusion apparatus having effective diffusion area and an opposite receptor volume. In this case, the animal skin is laid between the donor and the receptor where the subcutaneous layer is laid on the face of the donor cell. The media of receptor were agitated to ensure consistent receptor dispersion during the experiment, some volume of the sample leaving receptor fluid and substitution with an equal volume at particular time interval. Lastly, a comparison of the profile of cumulative permeation of microneedle treated and untreated skin was conducted [144].
Histological study
The efficiency of the microneedle patch of stratum corenum penetration is investigated through rat skin by applying microneedle patch on the rat skin, after 1min by using soft thumb pressure then the skin was put in 10% formalin solution and allowed to stay overnight. The paraffin-impregnated tissue is then embedded in the tissue, paraffin removed by using of microtome, followed by cutting a thin section and then attaching the tissue to the slide followed by staining by use of haematoxylin and eosin pigment[145].
In vitro release study
A patch of a microneedle is mounted between the donor and the receptor compartment of diffusion cell by using Franz cell diffusion. The liquid of receptor is stirred in the presence of magnetic stirrer; this receptor is filled with a certain volume of phosphate buffer pH 7.4 and the temperature of receptor is adjusted at 32C. Sample withdrawals at some time interval and substituted with same volume of phosphate buffer pH7.4. Following this, measured at specific wave length following a specific dilution, thereafter, the test repeated thrice sub-sequently assume the average value [146].
Advantages
Minimally Invasive and Painless Delivery: Herbal based microneedles enter the stratum corneum without moving past the dermis to the pain receptors and therefore, painless and blood-free delivery is possible. This improves compliance in patients, particularly in the long term management treatments such as diabetes management [119].
Improved Bioavailability of Herbal Actives: Herbal bioactives do not have high bioavailability rate because of low solubility and first-pass metabolism when orally administered. Microneedle delivery avoids the gastrointestinal tract and hepatic metabolism and introduces the herbal drugs directly to the systemic circulation via the microchannels of the dermis, which greatly enhances the therapeutic concentration of herbs [147].
Sustained and Controlled Release: Biodegradable polymers in herbal Microneedles (including chitosan, hyaluronic acid allow active and controlled delivery of herbal products or insulin mimics, so that plasma drug levels remain steady and the number of injections is lowered [128].
Synergistic Therapeutic Action: Synergistic effects of herbal bioactives (with or without insulin in MNs) may be observed (antioxidant, anti-inflammatory, and 6-cell protective effects) to improve glycemic control and decrease diabetic complications.
Less Systemic Systemic Side Effects: The nature of the delivery is localized, and gastrointestinal absorption is avoided; therefore, herbal-based MNs are less toxic, irritable, and degrading by systemic routes compared to the oral or injected counterparts [148].
Challenges And Limitations
Microneedle patches of herbal-based have a number of challenges which restrict their clinical translation. There is also a change in the herbal extract makeup with change in the plant source and mode of extraction resulting in unreliable treatment effect. Polymer materials and bioactive herbs can lead to incompatibility with herby bioactives causing either instability or inefficiency. Balance between dosage and drug loading and controlled release of the herbal compounds is challenging to achieve. Micro needles can also be made weak by the high concentration of herbal ingredients thus not penetrating the skin fully. Also, insufficient clinical trials, regulatory not very clear pathways, and scalability are disadvantages to commercialization. Long-term stability and safety are another factor that creates restrictions to these innovative systems [117].
Recent Advances
Biodegradable Polymers
Biodegradable polymer-based micro-needles are now getting more popular as the polymer is bio-compatible, costeffective, and dissolves or degrades in the skin upon drug delivery.
Material Innovations
Polymers Poly-lactic acid, poly lactic-co-glycolic acid, and polyvinyl pyrrolidone are considered to be common because of their mechanical strength and degradation controlled properties [149,150].
Printing Processes
FDM has facilitated accurate production of micro-needles with shaped, sizeable, and identifiable shapes and sizes. The chemical etching after fabrication enables tip sizes to a small 1 μm, which produces better penetration and drug release.
Metal-Based Micro-needles
Metal micro-needles are appreciated because of mechanical strength, durability and bio-compatibility. The most common metals that are used are stainless steel and titanium, which are robust and can be used with the biological tissues. Nickel and palladium are some of the other metals that are under investigation to be used in particular applications.
Applications
The metal micro-needles are specially chosen to be used in high mechanical strength application, like vaccine administration or cancer treatment. They have a high accuracy in dosage and quick acting.
Market Growth
Metal micro-needles took a large percentage of revenues in the world market in 2024, and the fact that they have become common in clinical treatments indicates their popularity [150].
Table 1.5 Comparative Studies with Conventional Method [156, 157, 158].
|
S. No |
Features |
Traditional insulin delivery |
Herbal based microneedle patch for insulin delivery |
|
1 |
Method of delivery |
Insulin is delivered through a syringe or a device that an individual inhales |
Insulin is administered through tiny, painless microneedle in the patch |
|
2 |
Needle insertion |
Required a needle for injection |
Insulin is administered through tiny, painless microneedle in the patch |
|
3 |
Frequency of administration |
Multiple injection throughout the day or continuous infusion through an insulin pump |
Either worn for long periods as a patch, releasing insulin slowly |
|
4 |
Pain level |
Injection is painful and uncomfortable, particularly for people with needle phobia |
Microneedles are very invasive and inflict minor to no pain |
|
5 |
Ease of use |
It requires one to adminster appropriately, especially with self injection |
Simple to use, it is matter of applying a patch to the skin without the necessity for manual injections |
|
6 |
Skin irritation |
Provides high accuracy with each dose administered |
Provides high accuracy with each dose administered |
|
7 |
Side effect |
Risk of hypoglycemia when dosing is inappropriate, reaction at the injection site |
Less side effect, risk of irritation or allergic reaction to patch material |
FUTURE PROSPECTIVES
The prospects of micro-needle insulin patches are good in the future, fancements and increase in the demand of non-invasive diabetes care solutions.
Technological Advances
5.1 Wearable Systems
Recently, a wearable micro-needle patch was presented and it is made of a graphene composite inkprinted sensor and an electrosmotic micro-pump. This system enhances stability and allows proper glucose monitoring and insulin delivery indicating successful blood glucose control in animal models. Such technologies have the potential to alter closed-loop diabetes control system to be more accessible and efficient to patients [151].
5.2 Micro-needle Designs Diversity
The hollow, dissolving and hydro-gel-forming types of micro-needles are being investigated. These kinds of designs are meant to optimize the delivery of insulin through the skin with the least invasiveness. One such example includes the hollow micro-needle which portrays good pharmacokinetic properties that match the conventional subcutaneous injections, implying that there can be a wide clinical usage of this product [152,153]
5.3 Clinical Trail and Research
Continued Clinical Evaluations: To determine the effectiveness and safety of insulin delivery by different micro-needle products, there are ongoing clinical trials of these products. These trials play a significant role in learning the actual usefulness of these technologies besides overcoming regulatory problems that have slowed down development in the past [154].
5.4 Increased Bio-availability:
Investigations indicate that micro-needle systems can possess an equivalent bio-availability as other standard subcutaneous injections. An example study established that insulin was administered by a micro-needle patch, which had larger pharmacological availability compared to conventional injections. This is to suggest that insulin delivery with micro-needles may be more effective [152].
Market Trends and Challenges
Commercialization Programs: There is an increased interest in commercialization of the micro-needle drug delivery systems as both researchers and pharmaceutical companies show their interest in this field. Effective commercialization will however depend on the ability to overcome challenges of scalability of the manufacturing process, regulatory clearance processes as well as patient safety [154,155].
Personalized Medicine:
The technology of digital twins may allow the design of micro-needle patches to suit the individual requirements of the patient. Individualized treatment might increase the outcomes because they enhance the delivery of insulin based on personal patient features [154].
CONCLUSION
The herbal-based microneedle patches are a prospective and multifaceted breakthrough in the management of diabetes, which integrates the minimally invasive and point delivery potential of microneedle technology with the pharmacological and excipient advantages of botanically produced compounds. In preclinical studies and formulation development, these systems have demonstrated high potentials to enhance glycemic control by enabling controlled, sustained or responsive insulin delivery and adding complementary herbal bioactivities antioxidant, anti-inflammatory, -cell protecting, insulin-sensitizing that may help in diabetic complications and metabolic dysfunction beyond that of glycemia alone. The major strengths of herbal-based microneedle patches include improved patient acceptability due to pain-free or low pain transdermal administration as compared to in Further, the platform design of the microneedles is modular, enabling the addition of glucose-responsive as well as combination therapies in a wearable and small size. Moreover, efficacy, dosing equivalence, and patient selection parameters will still need to be determined by rigorous pharmacokinetic/pharmacodynamic data, long-term safety studies and head-to-head clinical trials with standard insulin regimens. several high-value research directions would still have to be pursued. Through the development of glucose responsive microneedles that couple herbal actives with smart polymers or enzyme based sensing, closed loop, on-demand insulin dosing in combination with adjunctive therapy will be possible. Developed manufacturing 3D printing, roll micro-fabrication and lyophilization plans may enhance scalability and shelf life. Last but not least, patient-centred design with regards to wearability, user training, affordability, and cultural acceptability of herbal formulations will be essential to be adopted in various healthcare environments, with resource-constrained environments with cold-chain issues and injection phobia being key factors.
REFERENCES

Dhanasekar J.*, Madhumitha G., Kaviya C., Monika P., Selvakumar M., Sudhamani T., Lathamani L., Nandhakumaran S., Snehal P., Herbal Based Microneedle Patches for Diabetes Management: A Novel Approach to Insulin Delivery, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 7385-7420. https://doi.org/10.5281/zenodo.20412655
 10.5281/zenodo.20412655
10.5281/zenodo.20412655