
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
St. Soldier Institute of Pharmacy, Lidhran Campus Behind NIT (R.E.C) Jalandhar – Amritsar Bypass Nh-1, Jalandhar, Punjab, India 144011
Both HIV and TB constitute a lethal syndemic in which each pathogen accelerates the other’s progression and severely undermines host immunity. HIV depletes CD4? T cells, disrupts granuloma composition, and increases susceptibility to active tuberculosis, while TB-induced inflammation boosts HIV replication. The complications in the diagnosis are increased when paucibacillary disease, limited sputum production, and uneven access to rapid molecular tests such as Xpert MTB/RIF Ultra occur. The person suffering from the co-infection is advised to receive the anti-TB therapy along with initiation of antiretroviral therapy (ART), within 2 weeks, for a patient with a CD4 cell count of less than 50cells/µL. The treatment of the disease becomes more complicated when drug-drug interactions are seen between rifamycin and ART, along with the risk of TB-immune reconstitution inflammatory syndrome. Prevention of these diseases primarily involves the routine HIV testing, regular screening of TB, isoniazid preventive therapy and scaling-up of rapid diagnosis tests. Instead of advancement in the diagnostic tools, multidrug-TB, adherence difficulties and socioeconomic barriers are the major challenges. Thus, to reduce the mortality due to HIV-TB co-infection, the coordinated, patient-centred care that combines early detection, integrated therapy and psychosocial support is essential.
HIV is a global-scale pandemic that majorly targets the body’s natural barriers, including CD4⁺ T lymphocytes, macrophages, and dendritic cells, which weaken the immune system and further progress to acquired immunodeficiency syndrome (AIDS). The primary reason for the lethal nature of this retrovirus is its great diversity due to a higher rate of replication and mutation, which leads to the generation of multiple subtypes and variants. HIV mainly spreads through the use of unsterile needles, unprotected sexual intercourse, from an infected mother to the baby and less often due to blood transfusion and workplace exposure [1]. In a year, approximately 1.7 to 1.8 million new HIV infection cases are being reported, even though there has been a great advancement in the ART(Antiretroviral Therapy) and protection from the pandemic[2]. Globally, in the 1980s, there were approximately 80 million infections due to HIV and more than 35 million deaths; however, the highest burden of the disease is in sub-Saharan Africa[3]. The percentage of the HIV infected people dropped by 22%, and approximately 40 % deaths were recorded across the interval of 2010 to 2021; however, the better clinical outcomes have escalated the number of infected people to 40 million[2]. Nowadays, through the rapid diagnostic platforms, healthcare workers can easily confirm if someone has HIV or not and can also identify whether the infection has happened recently or over a long period of time. These tests are very accurate to identify the infections with 90% sensitivity and 98% specificity, and by estimating if an infection has happened in the last 6 months, these tools help in epidemic monitoring and prevention[4].
Tuberculosis is a kind of serious infectious disorder that spreads through the air by a bacterium named Mycobacterium tuberculosis. It is a great threat to human health, even though this disease can be clinically managed and avoided. Mycobacterium tuberculosis mainly attacks the lungs of the body but may also affect other organ systems, resulting in cough, fever, weight loss, impairment in body functioning and the immune system[5]. By exceeding HIV/AIDS, TB has become one of the most serious single infections in the world in the 21st century, resulting in fatalities[6]. In the past year,2016, there were 10.4 million new cases that were being detected globally and across 1.7 million people died with TB[7]. The latest survey of 2019 indicated that even providing the foremost clinical facilities and medicines, the rate of TB-infected cases had not declined, following 1.2 million mortality cases and 10 million TB-infected cases[8]. According to the estimation of the Global Burden of Disease (GBD) 2015 study, more than 10 million people of world population were struggling with the infectious disease, while 1.3 million individuals died[9]. The treatment of TB becomes more expensive and complicated when the body of a person battling TB becomes resistant to the drugs. For example, in 2016, nearly 600,000 rifampicin-resistant TB cases were observed, which clearly points towards the multidrug-resistant TB (MDR-TB)[7]. The children and infants are also at high risk of developing tuberculosis, and chronic illness may affect the body organs, including the brain, resulting in meningitis[10].
On the other hand, when these two syndromes occur together, lead to a fetal HIV-TB co-infection, which causes a considerably more malignant impact on global health than that of HIV or TB alone[11]. The severe impact of HIV TB co-infection is majorly seen in countries where more than 90% of the population is suffering from Tuberculosis with limited income and inefficient clinical conditions. The mortality and morbidity rate, due to HIV-TB co-infection, is nearly 80% in sub-Saharan Africa, as compared to the world; however, there occur across 500,000 deaths and 1.3 million HIV-TB co-infections annually in the world[12]. The recent Global Burden of Disease 2021 analyses further complexities of the disorder, according to which the age-standardised incidence rate of HIV-associated drug-susceptible TB was 11.59 per 100,000 population, whereas the rates of HIV-MDR-TB and HIV-XDR-TB were 0.55 and 0.02 per 100,000 population, respectively [11]. It has been observed in the United States that the percentage for the lifetime risk of development of tuberculosis in HIV-negative persons and those HIV patients who are not receiving ART(Antiretroviral Therapy) is nearly the same, i.e. up to 8% per year[13]. In the last few years, it has been observed that the death rate due to HIV-TB co-infection is greater in women(60% more) than in men [14]. On the other hand, the extreme and different drug doses of early Anti-retroviral Therapy may result in several body complications, including immune reconstitution inflammatory syndrome (IRIS), toxicity of drugs, reduced adherence, etc. and even death; however, the outcomes remain the same even though the patient receives ART late[15].
HIV and Mycobacterium tuberculosis act as a deadly duo, where each accelerates the progression of the other. HIV weakens the immune system of the body, making individuals more prone to develop active TB, while TB infection increases the replication and speeds up the progression to AIDS. Despite advancements, TB remains the leading opportunistic infection and primary cause of death among people living with HIV worldwide. Co-infection often leads to atypical presentation, such as extrapulmonary TB and smear-negative results, which significantly delay diagnosis and treatment. Concurrent treatment of both diseases may cause drug-drug interactions and risk of IRIS. This review is necessary to bridge the gap in understanding how HIV specifically disrupts CD4+ T cell function within granulomas, which is essential for developing new vaccines or immune-based therapies.
Pathogenesis and Immunology of Co-infection:
The risk of occurrence of tuberculosis is increased during HIV infection due to a lower count of CD4+ T cells; however, it may reach to the normal range, causing other respiratory problems like water in the lungs or lymphadenitis, according to public health research. On the other hand, tuberculosis accelerates the HIV infection by providing the homeostatic adjustments related to the viral replication through attachment of HIV to the chemokine receptor present on the immune cells and later on the proliferation of the virus from CCR5 to CXCR4receptor, a sign of faster disease progression[16].
The immunological response of the body can be seen at the interaction of the cytokines with the virus, resulting in immunomodulation, which causes cytolysis of CD4 +T cell, promoting the co-infection due to the deficiency of the defence system of the host[17]. Due to the depletion of the CD4+ T cells promoting the infection to the lungs during AIDS, and according to research, there is a loss of approximately 1,00,000,000 -2,00,000,000 CD4+ T cells per day, which further leads to the co-infection [18], [19]. Thus, during the HIV TB co infection, there occurs destruction of CD4+ T cells, followed by the disorganisation of TB induced granuloma, resulting in the spread of HIV to the entire body along with an increase in bacterial load[20]. Also, a protein released by the white blood cells, i.e. TNF alpha act as a bridge for the acceleration of both disorders. TB infection triggers the release of TNF alpha, which then fuels the HIV replication, while on the other hand, when HIV enters the body, it enhances the TNF alpha signalling, further causing an increase in the inflammation resulting in the stimulation of CD4+ T cells, the immune cells required to control the TB infection[17], [21]. In addition to the loss of CD4+ T cells, the induction of HIV replication results in the stimulation of cells and tissues, leading to an insufficient immune response in tissues and organs of the body, which may cause reactivation of latent tuberculosis[20], [22]. Since the Antiretroviral Therapy(ART) has reduced the risk of TB for HIV patients, but the risk cannot be eliminated; even the incidence of developing TB is 4 to 7 times higher in the hyperendemic regions, instead of giving ART to the population[22], [23], [24].
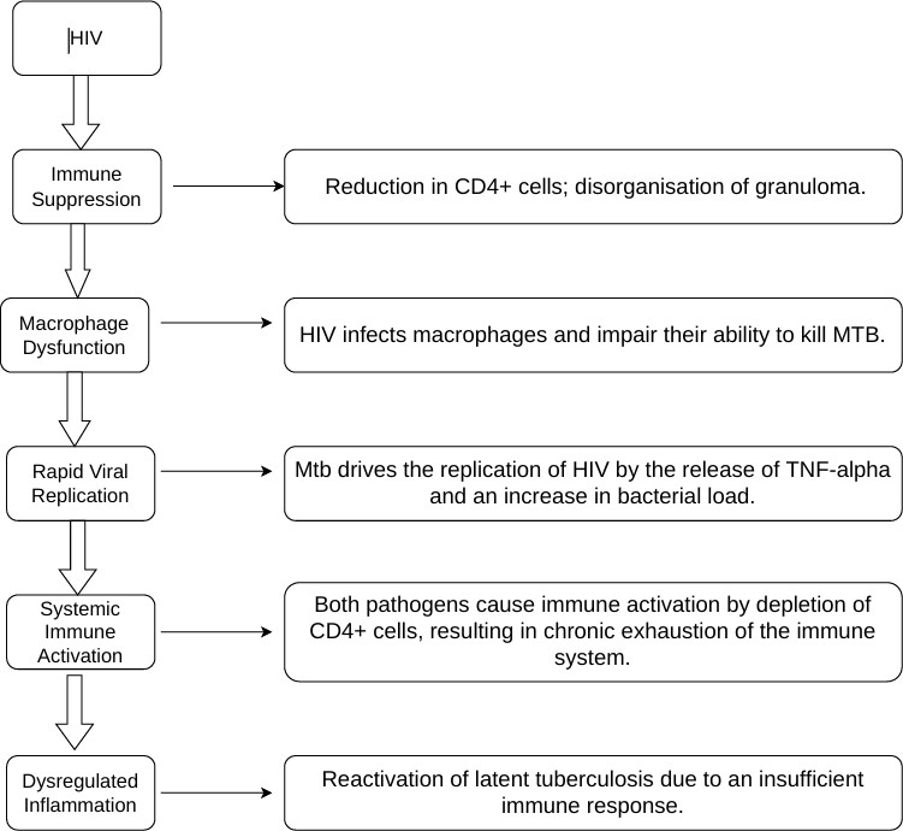
Flow chart of pathogenesis of HIV-TB Co-infection
Diagnostic Challenges and Tools:
The HIV and TB co-infection can be detected conventionally by several methods, including Symptoms screening and clinical assessment, the primary and cost-effective approach, which is based on analysing the symptoms of the patient in comparison to HIV or TB; but it has low sensitivity, especially in advanced HIV[25], [26], [27].
Chest Radiography a widely used tool for the diagnosis of pulmonary and disseminated tuberculosis, but it does not show any abnormalities with a single X-ray pattern, even though the patient has been suffering from the disorder [26], [28].
Sputum smear microscopy has been used for years to detect pulmonary tuberculosis. It involves the staining of bacteria with dyes. Since these bacteria are acid-fast bacteria, they retain the dye even after washing and are easily visualised under the microscope or under fluorescence. But it may not be regarded as a systemic approach due to less sensitivity for HIV detection in the bacterial and less sputum production for the diagnosis[25], [26], [29].
Mycobacterial culture method involves the decontamination of the collected samples, including sputum, blood or serum, followed by isolation of low levels of bacteria. Then, samples are inoculated into liquid media for rapid growth detection within 10 to 14 days. It has been regarded as the best method for diagnosis of HIV TB co infection because of its very good sensitivity, and also permits the Drug susceptibility testing; however, it requires very much time along with a well-trained and experienced staff with BSL-3(Biosafety Level 3)[26], [30], [31].
Another type of diagnosis which are based on the molecular analysis of the sample. For example, Xpert MTB/RIF and Xpert Ultra (GeneXpert platform), which have advanced smear microscopy for the screening of pulmonary tuberculosis through the culture-based methodology[26], [32].
Line Probe Assay (LPA) is another method for screening rifampin and isoniazid resistance MDR/XDR. It is based on Polymerase Chain Reaction (PCR) and DNA-strip technology for detecting MTB and drug resistance. But one of its drawbacks is that it requires a good testing methodology and qualified staff[26], [32].
The driving factor behind the complications of the diagnosis of HIV TB co infection is that when these disorders are diagnosed in the laboratory, there are several other diseases, like TB, that give the same outcomes during the molecular testing of the sputum and chest X-rays, which instantaneously hide the tuberculosis infection, may complicate the diagnosis[26], [31], [33]. Also, the late-stage HIV results in failure of granuloma formation and the spread of the Mycobacteria in the entire body, resulting in less sputum production, due to which the sensitivity of the smear microscopy and other assays gets reduced, giving an atypical clinical presentation[26], [29], [34].
Since, for the diagnosis of HIV TB co-infection, the large-scale diagnostic tools like Xpert, LPA, etc., which give accurate results, are localised in the urban areas, and there is a lack of advanced testing in the rural areas, which are still based on smear microscopy; this leads to missed or late diagnosis and further spread of the diseases[28], [32], [35].
Clinical management and Therapeutic strategies:
The main point regarding the clinical management of the HIV TB co infection is that the patient should be in integrated care by the healthcare systems, so that there is management of the interaction of TB and HIV drugs and contraindications due to the immune response of the body[25], [36].
The WHO has set up some standard medication plans according to which all HIV patients should be tested for tuberculosis as soon as possible to prevent complications during the treatment of co-infection. A TB-infected patient undergoes drug therapy for 60 days with isoniazid, rifampicin, pyrazinamide, ethambutol, then 4 months of isoniazid + rifampicin combination, which is also acceptable in HIV positive patients. The same duration is used for the drug-sensitive TB in HIV negative patients; however, for advanced TB, this been under evaluation[25], [36]. When the Susceptible TB get switched to the Multiple Drug Resistant TB, then new drugs(bedaquiline, linezolid, fluoroquinolones, pretomanid ) are included in the therapy, which may give positive results of the treatment, but may cause complications when given to children and pregnant ladies or to the ART-receiving patient[37], [38].
The ART should be started early in HIV patients as it has reduced the risk of occurrence of tuberculosis and the death rates. After several clinical examinations, the health professionals suggest initiating the ART within 15 days of tuberculosis for CD4 <50 cells/µL and within 8 weeks for a large number of CD4+ T cells, which has supported the survival against TB-IRIS risk[36]. Also, to control the TB-associated immune reconstitution inflammatory syndrome (TB-IRIS), the corticosteroids and NSAIDs should also be added with ART and anti-TB drugs to manage the inflammatory response of the body[24], [38].
On the other hand, the interaction of HIV and TB drugs leads to a decrease in the efficacy of anti-TB drugs, for example, the drugs for HIV or ART lower the concentration of tuberculosis drugs in the blood, especially rifampicin and ethambutol in children, due to drug-related interaction other than the individual action (enzyme boosting pathway) of the rifampicin[39]. Thus, for the patient suffering from HIV TB co-infection, the proper treatment regimen should be established with 6 months course of first-line drugs (isoniazid, rifampicin, pyrazinamide, ethambutol), and the same protocol should be followed for the HIV negative patients with intensive clinical management to prevent the adverse drug reactions. Another core principle that has to be followed for the management of HIV associated TB is that ART should be given to any stage of the co-infected patient, without considering the number of CD4 + T cells. Giving Antiretroviral Therapy has decreased the deaths of people and improved their survival[24], [36], [40].
Prevention and Control:
The core biomedical strategy to prevent and control the HIV TB co-infection is to give Antiretroviral Therapy to the HIV patients, regardless of whether the CD4+ T cell count is high or low. Consequently, the rate of co-infection in the developing countries with dense populations will decline[41]. The World Health Organisation has developed various programs regarding the prevention of tuberculosis in TB patients and in co-infected patients. These programs include End TB Strategy, STOP TB Partnership, and Global Fund programs and these initiatives have prevented over a million TB deaths[42]. In addition to this, there should be well-equipped laboratories and healthcare systems in order to improve the diagnosis of patients, and regular screening for HIV in TB patients and for tuberculosis in HIV patients should be carried out to control the HIV-TB co-infection[43], [44], [45]. Along with the initiative programs of the government, there is a need to provide knowledge regarding the HIV-TB co-infection and the significance of various diagnostic testing, so that people get awareness about the co-infection and overcome the stigma regarding the epidemic[46].
The screening and early diagnosis of tuberculosis, especially through high sensitivity assay like Xpert MTB/RIF Ultra and lateral-flow urine lipoarabinomannan (LF-LAM, has proved very beneficial for the HIV patients who are unable to produce sputum and it is also effective in preventing the further co infection; in West Africa and Ethiopia a significant downward trend in new infections and deaths can be observed after following these systemic guidelines[38], [42], [47], [48]. HIV and TB usually spread through using non-sterile needles, working in crowded areas, due to a lack of services like nutrition, food, etc. Therefore, by changing the behavioural habits, HIV-TB co-infection can be controlled to a large extent [47], [48]. In general, the burden of HIV TB co infection can be minimized though the global action plan of the WHO, including diagnosis of the disease on time, along with proper medical treatment and clinical approaches[24].
Challenges and Future Directions:
The key complications behind the co infection is difficulty in the diagnosis of the epidemics, which leads to less sputum production during the systemic and paucibacillary tuberculosis, due to which the tuberculosis sometimes stays hidden in HIV patients, making the cases of co-infection more aggravated [46], [49], [50]. During the treatment of co-infection, the combination therapy of different drugs is provided to the patients. Hence, there occurs a treatment burden to all age groups, especially to the children and elderly population[51]. For example, Rifampicin and rifapentine show interaction with the Antiretroviral Drugs due to stimulation of drug metabolising enzymes and transporters, and minimise the bioavailability of the ART drugs[52].
In addition to this, although the death rate decreases when patients receive ART on time, the probability of occurrence of TB-IRIS is enhanced, driven by an increase in the number of cytokines in blood, immune activation and proteolytic degradation by MMP8 and MMP9[50], [53], [54]. In the developing countries, due to economic instability, lack of social and community context, transport is a huge obstacle to fighting against the co-infection[43], [50]. The clinical, along with digital healthcare services, will help to minimise the co-infection case through providing information and financial support regarding the proper intake of ART, reducing stigma in Co-infected patients, to the people via SMS, apps, etc. Consequently, there will decrease in the death rate of co-infected patients[43], [50], [55].
CONCLUSION:
HIV/TB co-infection represents a lethal “syndemic” where the two pathogens work in a dangerous cycle to accelerate each other’s progression and compromise the host’s immune system. TB remains the leading cause of death and hospitalisation for people living with HIV, often presenting with atypical or severe extrapulmonary symptoms that make early diagnosis exceptionally difficult. Effective management requires a dual approach-immediate initiation of anti-TB treatment and timely introduction of antiretroviral therapy (ART) to restore immune functions and improve survival outcomes. Despite medical advancements in rapid molecular testing and shorter treatment regimens, challenges such as drug-drug interactions, treatment adherence, and the rise of multidrug-resistant strains continue to strain public health systems. Ultimately, integrated care that combines screening, prevention, and early treatment is critical for reducing the high mortality rates associated with this dual burden.
REFERENCES




Babita, Rajesh Kumar, Ajeet Pal Singh, Amar Pal Singh, Pardeep Kaur, HIV-TB Co-infection: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 1929-1939. https://doi.org/10.5281/zenodo.21280648
 10.5281/zenodo.21280648
10.5281/zenodo.21280648