
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1BAMS PG Scholar, Department Rasashastra and Bhaishajya kalpana, Govt. Ayurved college Nanded, India
2MD. (Ayu), Guide, Professor, Department Rasashastra and Bhaishajya kalpana, Govt. Ayurved college Nanded, India
3Head of Department MD. (Ayu), Guide, Professor, Department Rasashastra and Bhaishajya kalpana, Govt. Ayurved college Nanded, India
Hypothyroidism is a common endocrine disorder characterized by inadequate secretion of thyroid hormones, leading to metabolic dysfunction and multisystem involvement. Classical biomedical descriptions emphasize reduced basal metabolic rate, fatigue, weight gain, and neurocognitive impairment. In Ayurvedic nosology, the condition can be interpreted through the lens of Kapha Vata doshic Dushti, Rasavaha Srotas Dushti, Medo Dushti, and Agnimandya, which collectively contribute to impaired metabolism and systemic manifestations.Case Presentation: A 23 year old female presented with persistent symptoms despite three years of conventional allopathic therapy. Her complaints included Sthaulya (weight gain), Daurbalya (weakness), Tvak ruk?ata (dry skin), Kesa patana (hair loss), periorbital puffiness, mood disturbances, impaired cognition, depression, drowsiness, headache, Amlapitta (hyperacidity), and lethargy. These features correspond to both biomedical hypothyroidism and Ayurvedic descriptions of Kapha Vata imbalance with Agnimandya.Intervention: A regimen of Herbo mineral formulations was administered for four months, tailored to correct do?ha Dushti, restore Agni, and normalize Rasavaha Srotas function. The therapeutic approach emphasized Rasayana and shamana strategies, aiming at systemic rejuvenation and metabolic regulation.Outcome: Following the intervention, the patient demonstrated complete remission of clinical symptoms, normalization of thyroid profile parameters, and was able to discontinue allopathic medication. The therapeutic response highlights the potential of integrative Ayurvedic management in endocrine disorders, particularly hypothyroidism.Conclusion: This case underscores the relevance of Ayurvedic principles in addressing chronic endocrine dysfunctions. By targeting Kapha Vata imbalance, Medo Dushti, and Agnimandya, Herbo mineral formulations facilitated both symptomatic relief and biochemical normalization. Such evidence contributes to the growing body of literature supporting Ayurveda’s role in managing hypothyroidism and warrants further systematic clinical evaluation.
Thyroid disorders constitute a significant proportion of endocrine pathologies and are broadly classified into structural abnormalities such as colloid goitre, abscesses, and malignancies and functional disorders [1], including hyperthyroidism and hypothyroidism. A third category may represent a blend of both structural and functional disturbances [2], exemplified by conditions like Graves’ disease, which often manifests with overlapping features and systemic complications Over hypothyroidism describes moderate to severe thyroid failure resulting in high serum TSH level with low serum concentration of total thyroxine. Subclinical hypothyroidism refers to mild thyroid failure in which serum TSH levels are moderately increased, but total serum thyroxine T4 remain within the normal limit [3].
Among these, hypothyroidism is one of the most prevalent functional disorders, defined as a state of deficient thyroid hormone activity in peripheral tissues, resulting in impaired cellular metabolism [4,5]. It may be further categorized into:
The clinical spectrum of hypothyroidism has evolved over decades. Early descriptions emphasized classical features such as weakness, dry skin, lethargy, and weight gain, while more recent literature highlights fatigue, mood instability, constipation, alopecia, and neurocognitive disturbances. Given the systemic role of thyroid hormones, hypothyroidism manifests as a multi?system disorder, affecting metabolic, cardiovascular, dermatological, and neuropsychological domains.
From an Ayurvedic perspective, hypothyroidism is interpreted as a consequence of Jatharagni, Bhutagni, and Dhatwagni derangement, coupled with Kapha?Vata dosha dushti and Medodushti.[6] These imbalances culminate in the formation of Ama toxic metabolic byproducts that obstruct Srotas (channels) and impair systemic metabolism. The clinical presentation of hypothyroidism closely parallels Sthaulya (obesity/metabolic imbalance) described in classical Ayurvedic texts, thereby warranting management through Sthaulya Chikitsa.[7]
Therapeutic strategies in Ayurveda emphasize Shodhana (purification), Shamana (pacification), and Vyadhihara Rasayana (rejuvenative therapy aimed at disease alleviation).[14] While hormone replacement therapy remains the cornerstone of modern management, Ayurvedic interventions particularly Rasayana and Shamanoushadhi offer promising complementary approaches, with growing evidence of their efficacy in restoring systemic balance and alleviating symptoms.
Patient Information
Case Report
A female patient aged 23 years was consulted in the outpatient department with complaints of progressive weight gain, generalized weakness, dryness of skin, hair loss, puffiness around the eyes, mood swings, impaired memory, depression, drowsiness, headache, hyperacidity, hoarseness of voice, and lethargy. She was a known case of hypothyroidism for the past three years and was on regular medication with Thyronorm 75 mcg daily before food, but reported inadequate relief in symptoms. Her previous weight was 58 kg, which had increased to 62 kg at the time of consultation.
There was no history of diabetes, hypertension, cardiac illness, or any other major systemic disease. Family history was not significant for thyroid disorders. Appetite was reduced, sleep was sound, bowel habits were regular, and micturition was 4–5 times per day.
Clinical Examination
Thyroid Local Examination
On Inspection
On Palpation
MATERIALS AND METHODS
Treatment was planned after assessing dosha and dhatu involvement. The regimen included:
Table No.1: Treatment given to the patient
|
S. No. |
Name of Drug |
Dosage |
Time of Administration |
Frequency and Anupana |
|
1. |
Dhatri Loha |
1 tablet |
Before food |
Thrice daily with lukewarm water |
|
2. |
Nityananda Rasa |
21tablets |
After food |
twice daily with lukewarm water |
|
3. |
Arogyavardhini Vati |
2 tablets |
After food |
Twice daily with lukewarm water |
|
4. |
Kanchanar Guggulu |
2 tablets |
After food |
Twice daily with lukewarm water |
|
5. |
Varunadi kashay |
20 ml |
Before meal |
Twice daily with lukewarm water |
Allopathic medication was gradually tapered from 75 mcg to complete discontinuation.
RESULTS:
Table No.2 :Percentage variations of symptom’s before and after treatment
|
Parameter |
Before Treatment (BT) |
After Treatment (AT) |
|
Weight |
62kg |
57 kg |
|
Fatigue |
80% |
20% |
|
Hair loss |
90% |
30% |
|
Skin texture |
70% |
40% |
|
Hyperacidity |
80% |
2% |
|
T3 (ng/dl) |
90.0 |
94.0 |
|
T4 (µg/dl) |
4.10 |
6.64 |
|
TSH (µIU/ml) |
6.81 |
0.073 (within normal range) |
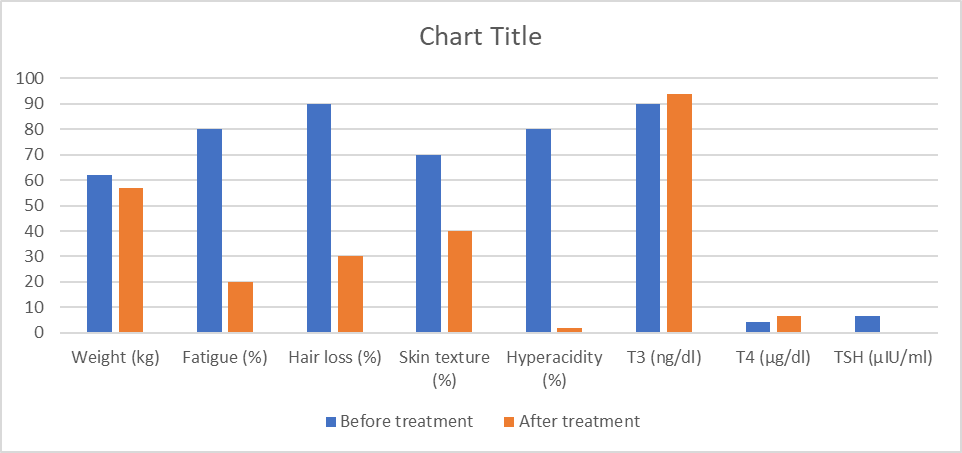
Figure No.1 :Graphical representation of % of variation of symptoms before and after treatment
DISCUSSION
Ayurvedic pathogenesis emphasizes Kapha?Vata imbalance and Agnimandya, leading to Ama formation and obstruction at the Srotas level. The therapeutic approach targeted:
Table No.3: Drug Ingreadient and Their Properties
|
Drug |
Ingredients / Composition [8] |
Properties & Action [15] |
|
Dhatri Loha [16] |
Amalaki, Loha Bhasma, Yashtimadhu, Guduchi |
Tridosha?hara, Rasayana: Balances Vata, Pitta, Kapha; rejuvenative, hematinic, supports digestion and immunity |
|
Nityananda Rasa [17] |
Herbo?mineral blend (Parada, Gandhaka, Tamra Bhasma, Vanga Bhasma, Kansya Bhasma, Hingula, etc.) |
Lekhana, Glandular Regulation: Useful in gout, lymphadenitis, fibroids, obesity; regulates metabolism and supports thyroid health |
|
Arogyavardhini Vati [11] |
Katuki, Triphala, Trikatu, Shuddha Parada, Shuddha Gandhaka, Loha Bhasma |
Deepana, Pachana: Enhances digestion, stimulates metabolism, detoxifies liver, purifies blood |
|
Kanchanar [9] Guggulu |
Kanchanar bark, Guggulu, Triphala, Trikatu, Varuna, Ela, Tvak, Patra |
Granthi?hara, KaphaMedoghna: Reduces glandular swellings, thyroid nodules, cysts; regulates metabolism and clears Kapha disorders |
|
Varunadi Kashaya [10] |
Decoction of Varuna, Punarnava, Gokshura, Chitraka, Brihati, Haritaki, Amalaki, etc. |
Kapha?Medoghna, Agni?deepana: Improves digestion, prevents weight gain, reduces oedema and Kapha?related disorders |
|
Chandraprabha Vati [12] |
Shilajit, Guggulu, Musta, Haridra, Amalaki, Daruharidra, Lauha Bhasma, Abhraka Bhasma, Tamra Bhasma |
Rasayana, Mutrala, Balya: Enhances immunity, supports urinary tract health, reduces inflammation, improves systemic resilience |
This integrative approach restored thyroid function, normalized biochemical parameters, and eliminated symptoms without adverse effects.
CONCLUSION
This case demonstrates the efficacy of Ayurvedic Herbo?mineral formulations in hypothyroidism management. The patient achieved complete remission, biochemical normalization, and discontinuation of allopathic therapy. The absence of adverse effects underscores the safety of Ayurvedic interventions. Larger clinical studies are warranted to validate these findings and establish Ayurveda as a complementary or alternative therapeutic modality for hypothyroidism.
REFERENCES


Dr. Sharda Raosaheb Giram, Nalini Hedaoo, Rajesh Ingole, Integrative Ayurvedic Approach in Hypothyroidism: A Clinical Case Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2407-2412, https://doi.org/10.5281/zenodo.21324153
 10.5281/zenodo.21324153
10.5281/zenodo.21324153