
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
IEC University, IEC School of Pharmacy, Baddi, Solan, Himachal Pradesh, 174103,India.
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The global prevalence of diabetes continues to rise, posing significant challenges to healthcare systems and emphasizing the need for effective, safe, and affordable therapeutic approaches. Although conventional antidiabetic drugs are widely used, their long-term administration may be associated with adverse effects, high treatment costs, and limited efficacy in preventing disease progression. Consequently, medicinal plants have attracted considerable attention as complementary and alternative therapeutic options for diabetes management.This review provides a comprehensive overview of medicinal plants used in the management of diabetes mellitus, with particular emphasis on their phytochemical composition, mechanisms of action, safety considerations, and future perspectives. Several medicinal plants, including Momordica charantia, Trigonella foenum-graecum, Gymnema sylvestre, Azadirachta indica, Ocimum sanctum, Aloe vera, Curcuma longa, and Syzygium cumini, have demonstrated promising antidiabetic potential. The therapeutic effects of these plants are primarily attributed to the presence of bioactive phytochemicals such as flavonoids, alkaloids, saponins, terpenoids, phenolic compounds, and glycosides.The antidiabetic actions of medicinal plants involve multiple mechanisms, including stimulation of insulin secretion, enhancement of insulin sensitivity, inhibition of ?-amylase and ?-glucosidase enzymes, promotion of glucose uptake through GLUT4 translocation, attenuation of oxidative stress, suppression of inflammatory pathways, and protection of pancreatic ?-cells. The multitarget nature of these phytochemicals offers potential advantages in addressing the complex pathophysiology of diabetes mellitus. Despite their therapeutic promise, concerns regarding toxicity, herb–drug interactions, variability in phytochemical composition, and lack of dosage standardization remain significant challenges. Therefore, rigorous safety evaluation, quality control, authentication, and regulatory oversight are essential for the development of reliable herbal medicines. Recent advances in phytochemistry, nanotechnology-based drug delivery systems, molecular docking, artificial intelligence-assisted screening, and personalized herbal medicine are expected to accelerate the discovery and development of novel plant-derived antidiabetic agents. Overall, medicinal plants represent a valuable source of bioactive compounds with significant potential in diabetes management. Continued research focusing on standardization, safety assessment, and mechanistic elucidation will be crucial for translating traditional knowledge into evidence-based therapeutic applications
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The disease has emerged as one of the most significant global health challenges of the twenty-first century, affecting millions of individuals across different age groups and socioeconomic backgrounds. Prolonged elevation of blood glucose levels can lead to serious complications involving the cardiovascular system, kidneys, eyes, nerves, and other vital organs, thereby reducing quality of life and increasing healthcare expenditures.
The prevalence of diabetes has increased dramatically over recent decades due to rapid urbanization, sedentary lifestyles, unhealthy dietary habits, obesity, population aging, and genetic predisposition. Type 2 diabetes mellitus (T2DM) accounts for the majority of diabetes cases worldwide and is closely associated with insulin resistance and impaired pancreatic β-cell function. Type 1 diabetes mellitus (T1DM), although less common, results from autoimmune destruction of insulin-producing β-cells and requires lifelong insulin therapy. The growing burden of diabetes poses substantial challenges to healthcare systems and highlights the need for effective, accessible, and sustainable management strategies.
Current therapeutic approaches for diabetes include lifestyle modifications, oral hypoglycemic agents, injectable therapies, and insulin preparations. These interventions are effective in controlling blood glucose levels and reducing the risk of complications when used appropriately. However, conventional antidiabetic therapies may be associated with several limitations, including adverse effects, high treatment costs, reduced patient adherence, drug interactions, and the inability to completely prevent disease progression in some patients. Additionally, the multifactorial nature of diabetes necessitates therapeutic approaches that target multiple pathogenic pathways simultaneously.
Medicinal plants have been used for centuries in traditional healthcare systems such as Ayurveda, Traditional Chinese Medicine, Unani, and other indigenous medical practices for the management of metabolic disorders, including diabetes. Plant-derived remedies contain a diverse array of bioactive compounds, including flavonoids, alkaloids, terpenoids, phenolic acids, saponins, tannins, and glycosides, which may contribute to their therapeutic properties. These phytochemicals have been reported to exert various biological activities relevant to diabetes management, such as enhancement of insulin secretion, improvement of insulin sensitivity, inhibition of carbohydrate-digesting enzymes, modulation of glucose transport, reduction of oxidative stress, and attenuation of inflammatory responses.
The increasing scientific interest in medicinal plants is driven by their chemical diversity, multitarget mechanisms of action, cultural acceptance, and potential for the development of novel therapeutic agents. Furthermore, advances in phytochemical analysis, molecular biology, and pharmacological research have facilitated a better understanding of the bioactive constituents responsible for antidiabetic effects. Nevertheless, concerns regarding safety, standardization, quality control, herb–drug interactions, and regulatory oversight remain important considerations in the utilization of herbal medicines.
Given the growing global burden of diabetes and the continued interest in plant-based therapeutics, a comprehensive evaluation of medicinal plants and their bioactive constituents is warranted. This review aims to provide an overview of medicinal plants used in diabetes management, with particular emphasis on their phytochemical composition, proposed mechanisms of action, safety considerations, and future research directions. By synthesizing current knowledge in these areas, the review seeks to highlight the potential role of medicinal plants in advancing diabetes care and supporting the development of evidence-informed therapeutic strategies.
Literature Review on Medicinal Plants Used in Diabetes Mellitus Management
Medicinal plants have been utilized for centuries in traditional healthcare systems to manage symptoms associated with diabetes mellitus. The increasing prevalence of diabetes and the limitations associated with conventional pharmacotherapy have stimulated scientific interest in plant-based interventions. Numerous medicinal plants contain bioactive phytochemicals that influence glucose metabolism through diverse mechanisms, including enhancement of insulin secretion, improvement of insulin sensitivity, inhibition of carbohydrate digestion, modulation of glucose transport, and reduction of oxidative stress. Research conducted over recent decades has identified several plants with promising antidiabetic properties, contributing to a growing body of literature in the field of herbal medicine.
Among the most extensively studied medicinal plants is Momordica charantia (bitter melon), which has traditionally been used in Asian and African countries for glycemic control. The plant contains biologically active compounds such as charantin, vicine, and polypeptide-p, which have been reported to exhibit hypoglycemic effects. Experimental studies suggest that these constituents may promote glucose uptake, improve insulin sensitivity, and support pancreatic β-cell function. The multifaceted actions of bitter melon have made it one of the most frequently investigated botanical agents for diabetes management.
Another important medicinal plant is Trigonella foenum-graecum (fenugreek), whose seeds are rich in soluble fiber, alkaloids, flavonoids, and amino acids. Fenugreek has been traditionally consumed as both a culinary spice and a medicinal herb. The high fiber content may slow gastric emptying and carbohydrate absorption, while specific phytochemicals are believed to contribute to improved glucose homeostasis. Research has highlighted its potential role in regulating postprandial blood glucose levels and enhancing insulin activity.
Gymnema sylvestre, commonly known as gurmar or “sugar destroyer,” occupies a prominent position in Ayurvedic medicine. The plant contains gymnemic acids, triterpenoid saponins, and flavonoids that may influence glucose metabolism through multiple pathways. Studies have suggested that these compounds can reduce intestinal glucose absorption, support pancreatic function, and modulate sweet taste perception. Such properties have contributed to its longstanding use as a traditional antidiabetic remedy.
Azadirachta indica (neem) has also attracted considerable attention due to its broad pharmacological profile. Leaves, bark, and seeds of the plant contain bioactive compounds such as nimbin, nimbidin, and azadirachtin. These constituents possess antioxidant and anti-inflammatory properties that may help mitigate metabolic disturbances associated with diabetes. Investigations have indicated that neem extracts may influence glucose utilization and improve metabolic parameters through multiple biological mechanisms.
The leaves of Ocimum sanctum (holy basil or tulsi) are widely used in traditional medicine for the management of various chronic disorders. The plant contains eugenol, ursolic acid, rosmarinic acid, and several flavonoids. These compounds exhibit antioxidant and anti-inflammatory activities that may contribute to improved glycemic regulation. Tulsi has gained recognition for its potential to support glucose metabolism while simultaneously addressing oxidative stress, a key factor in diabetes-related complications.
Aloe vera is another medicinal plant frequently investigated for its antidiabetic potential. The plant contains polysaccharides, anthraquinones, vitamins, minerals, and phenolic compounds that may influence carbohydrate metabolism. Experimental findings suggest that Aloe vera may support insulin action and contribute to improved glucose utilization. Its diverse phytochemical composition has made it an attractive candidate for further pharmacological exploration.
The culinary spice Cinnamomum verum (cinnamon) has received substantial attention because of its potential role in glucose regulation. Cinnamon contains cinnamaldehyde, eugenol, procyanidins, and polyphenolic compounds that may affect insulin signaling pathways and glucose transport mechanisms. The plant has been widely studied for its ability to influence carbohydrate metabolism and reduce oxidative stress associated with hyperglycemia.
Curcuma longa (turmeric) is another well-known medicinal plant with significant therapeutic potential. Curcumin, the principal bioactive constituent of turmeric, possesses potent antioxidant, anti-inflammatory, and metabolic regulatory properties. Research indicates that curcumin may modulate signaling pathways involved in insulin resistance, inflammation, and oxidative damage, thereby supporting glucose homeostasis and reducing diabetes-related metabolic disturbances.
Other medicinal plants frequently discussed in the literature include Allium sativum (garlic), Allium cepa (onion), Syzygium cumini (jamun), Pterocarpus marsupium, Tinospora cordifolia, and Moringa oleifera. These plants contain diverse classes of phytochemicals that have demonstrated antioxidant, anti-inflammatory, and glucose-regulating properties in preclinical investigations. Their traditional use across different cultures has inspired ongoing scientific efforts to identify active constituents and elucidate their mechanisms of action.
The existing literature demonstrates that medicinal plants represent a valuable source of bioactive compounds with potential applications in diabetes management. Their therapeutic effects are often attributed to multiple mechanisms acting simultaneously, which may provide advantages in addressing the complex pathophysiology of diabetes. Nevertheless, variability in plant species, cultivation conditions, extraction methods, and phytochemical composition can influence therapeutic outcomes. Consequently, further research focused on standardization, quality control, safety evaluation, and mechanistic understanding remains essential to support the rational development of plant-derived antidiabetic therapies.
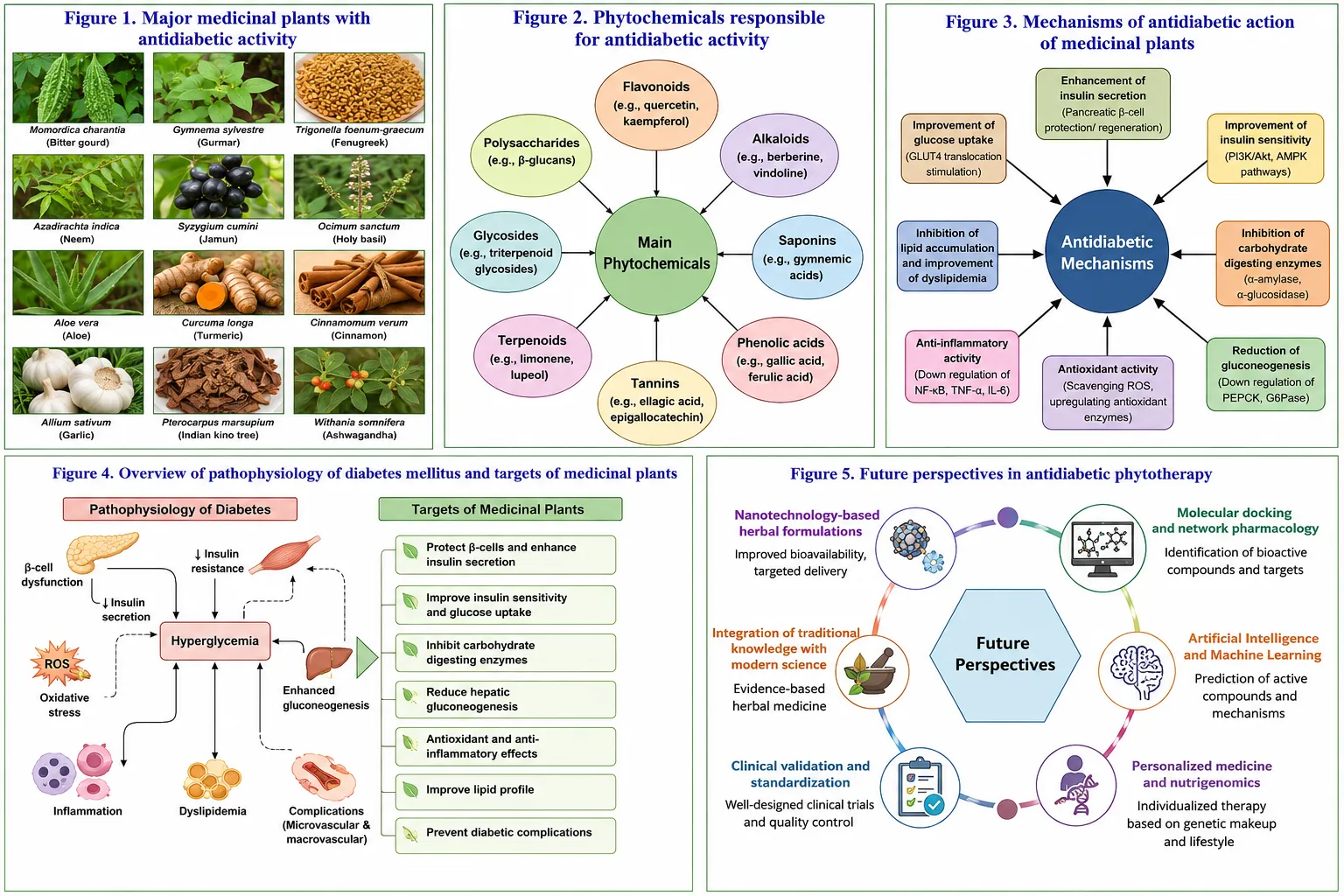
Figure 1. Major medicinal plants investigated for diabetes mellitus management and their traditional therapeutic applications.
Phytochemicals Responsible for Antidiabetic Activity
Medicinal plants contain a wide variety of bioactive compounds known as phytochemicals, which contribute significantly to their therapeutic properties. These naturally occurring substances influence numerous biological pathways involved in glucose homeostasis, insulin signaling, oxidative stress, inflammation, and metabolic regulation. The antidiabetic effects of medicinal plants are largely attributed to the presence of flavonoids, alkaloids, saponins, terpenoids, phenolic compounds, and glycosides. These phytochemicals often act through multiple mechanisms simultaneously, making them attractive candidates for the development of novel antidiabetic therapies.
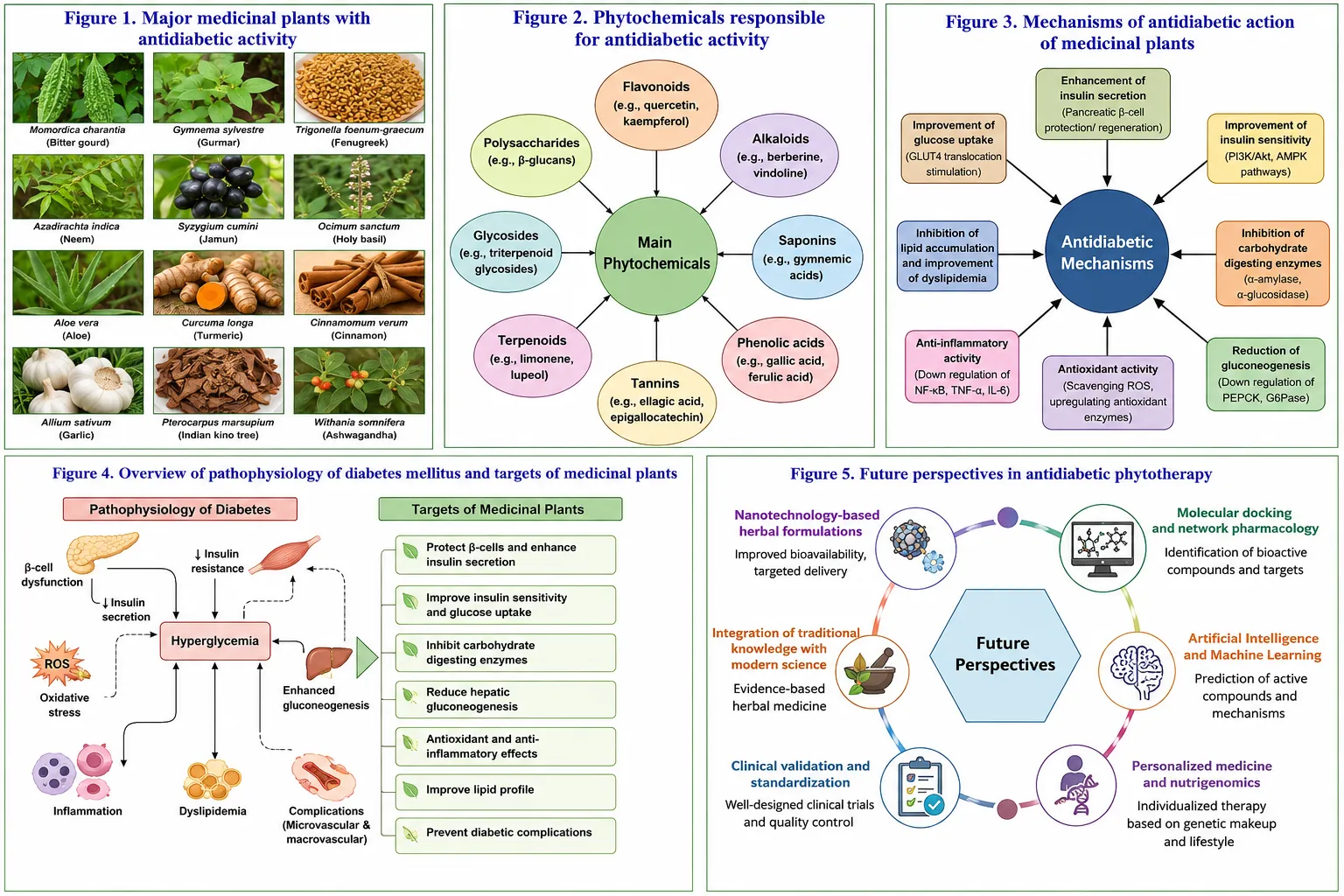
Figure 2. Major phytochemical classes involved in antidiabetic activity, including flavonoids, alkaloids, saponins, terpenoids, phenolics, and glycosides.
Flavonoids
Flavonoids are one of the most abundant classes of plant secondary metabolites and are widely distributed in fruits, vegetables, herbs, and medicinal plants. They possess strong antioxidant, anti-inflammatory, and metabolic regulatory properties. Flavonoids have been reported to improve glucose metabolism by enhancing insulin secretion, increasing insulin sensitivity, promoting glucose uptake in peripheral tissues, and protecting pancreatic β-cells from oxidative damage.
Common flavonoids associated with antidiabetic activity include quercetin, kaempferol, rutin, catechin, and luteolin. These compounds may modulate key signaling pathways involved in glucose transport and energy metabolism. Additionally, flavonoids can inhibit carbohydrate-digesting enzymes such as α-amylase and α-glucosidase, thereby reducing postprandial blood glucose levels. Their antioxidant properties further contribute to the prevention of diabetes-associated cellular damage and complications.
Alkaloids
Alkaloids are nitrogen-containing organic compounds that exhibit a broad range of pharmacological activities. Numerous medicinal plants used in traditional medicine contain alkaloids that contribute to glycemic regulation. These compounds may influence glucose metabolism through stimulation of insulin secretion, enhancement of insulin receptor sensitivity, inhibition of glucose absorption, and modulation of hepatic glucose production.
Berberine, trigonelline, and vindoline are examples of alkaloids that have attracted attention for their antidiabetic potential. Alkaloids may also activate cellular pathways involved in glucose utilization and energy balance. Their diverse mechanisms of action make them valuable candidates for further investigation in diabetes management and drug discovery.
Saponins
Saponins are naturally occurring glycosidic compounds characterized by their soap-like foaming properties. They are widely found in medicinal plants and have demonstrated significant biological activities, including hypoglycemic, antioxidant, and anti-inflammatory effects. Saponins may improve glucose homeostasis by enhancing insulin secretion, increasing glucose uptake by peripheral tissues, and reducing intestinal glucose absorption.
Several studies suggest that saponins can influence lipid metabolism and improve insulin sensitivity, which is particularly important in type 2 diabetes mellitus. In addition, these compounds may protect pancreatic β-cells from oxidative stress-induced damage. Their multifunctional nature contributes to the therapeutic value of many traditional antidiabetic plants.
Terpenoids
Terpenoids represent one of the largest classes of naturally occurring plant compounds. They are synthesized from isoprene units and exhibit diverse biological activities. Various terpenoids have demonstrated potential antidiabetic effects through regulation of insulin signaling pathways, enhancement of glucose uptake, and reduction of inflammatory responses associated with metabolic disorders.
Examples of antidiabetic terpenoids include ursolic acid, oleanolic acid, limonene, and gymnemic acids. These compounds may improve insulin sensitivity and modulate molecular targets involved in glucose metabolism. Furthermore, their antioxidant properties help reduce oxidative stress, which plays a crucial role in the development and progression of diabetes-related complications.
Phenolic Compounds
Phenolic compounds constitute a large and structurally diverse group of phytochemicals characterized by the presence of one or more hydroxyl groups attached to aromatic rings. These compounds are recognized for their strong antioxidant activity and their ability to protect biological systems from oxidative damage.
Phenolic acids such as gallic acid, chlorogenic acid, caffeic acid, and ferulic acid have been reported to exert beneficial effects on glucose metabolism. They may improve insulin action, inhibit digestive enzymes involved in carbohydrate breakdown, and reduce oxidative stress. By scavenging free radicals and suppressing inflammatory mediators, phenolic compounds contribute to the maintenance of metabolic homeostasis and the prevention of diabetes-associated complications.
Glycosides
Glycosides are compounds composed of a sugar moiety linked to a non-sugar component known as an aglycone. They are widely distributed in medicinal plants and possess numerous pharmacological activities. Several glycosides have demonstrated antidiabetic effects through modulation of glucose transport, enhancement of insulin secretion, and regulation of carbohydrate metabolism.
Notable examples include charantin from bitter melon and various flavonoid glycosides found in medicinal herbs. Glycosides may also inhibit intestinal glucose absorption and contribute to improved glycemic control. Their biological activities often depend on both the sugar component and the chemical nature of the aglycone, resulting in a broad spectrum of therapeutic effects.The antidiabetic potential of medicinal plants is largely attributed to the synergistic actions of multiple phytochemical classes. Flavonoids, alkaloids, saponins, terpenoids, phenolic compounds, and glycosides collectively influence insulin secretion, insulin sensitivity, glucose absorption, glucose utilization, oxidative stress, and inflammatory pathways. Understanding the chemical nature and biological activities of these phytochemicals is essential for the development of safe, effective, and standardized plant-based therapies for diabetes mellitus. The continued exploration of phytochemical diversity may facilitate the discovery of novel therapeutic agents capable of addressing the complex pathophysiology of diabetes.
窗体底端
Mechanisms of Antidiabetic Action of Medicinal Plants
The antidiabetic effects of medicinal plants are mediated through multiple biological mechanisms that target various aspects of glucose metabolism and diabetes pathophysiology. Unlike many conventional drugs that act on a single target, plant-derived phytochemicals often exert multitarget effects, contributing to improved glycemic control and metabolic homeostasis. These mechanisms include stimulation of insulin secretion, enhancement of insulin sensitivity, inhibition of carbohydrate-digesting enzymes, promotion of glucose uptake through GLUT4 translocation, antioxidant and anti-inflammatory activities, and protection of pancreatic β-cells.
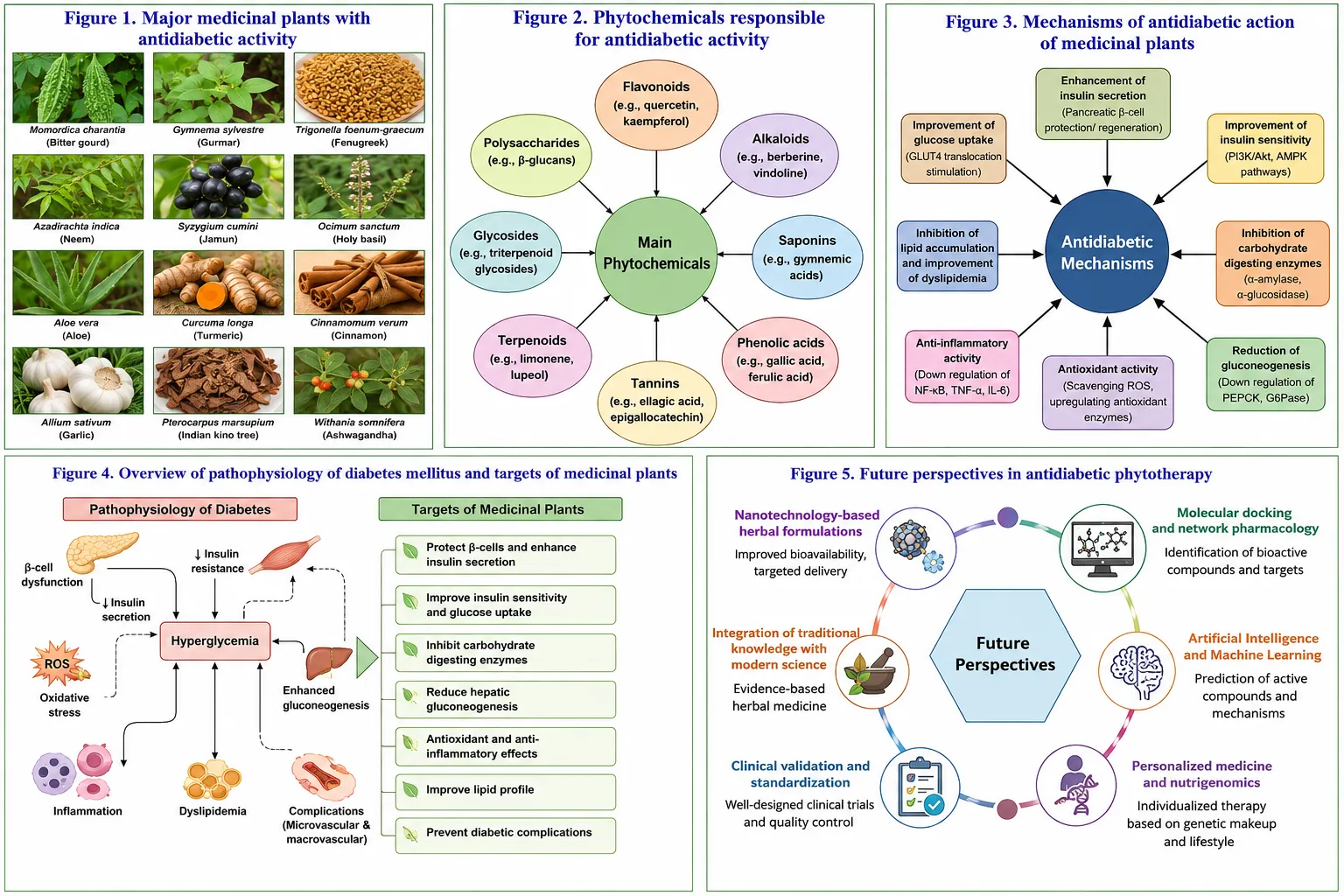
Figure 3. Proposed mechanisms of antidiabetic action of medicinal plants and their bioactive phytochemicals.
Enhancement of Insulin Secretion
Insulin is a key hormone responsible for maintaining blood glucose homeostasis by facilitating glucose uptake into peripheral tissues. In diabetes mellitus, particularly type 2 diabetes, impaired insulin secretion contributes significantly to hyperglycemia. Several medicinal plants contain bioactive compounds capable of stimulating insulin release from pancreatic β-cells.
Phytochemicals such as flavonoids, alkaloids, and saponins may enhance β-cell function by influencing intracellular signaling pathways involved in insulin synthesis and secretion. Certain plant constituents can increase calcium influx into β-cells, thereby promoting insulin exocytosis. Improved insulin secretion contributes to better glucose utilization and maintenance of normal blood glucose levels. This mechanism is particularly relevant in conditions where residual β-cell function is preserved.
Improvement of Insulin Sensitivity
Insulin resistance is a hallmark feature of type 2 diabetes mellitus and is characterized by a reduced cellular response to insulin. As a result, glucose uptake by skeletal muscle, adipose tissue, and other peripheral organs becomes impaired, leading to elevated blood glucose levels.
Numerous phytochemicals have been reported to improve insulin sensitivity by modulating insulin receptor activity and intracellular signaling pathways. Flavonoids, terpenoids, and phenolic compounds may enhance insulin-mediated glucose uptake through activation of pathways such as phosphatidylinositol 3-kinase (PI3K) and protein kinase B (Akt). Improved insulin sensitivity reduces the demand on pancreatic β-cells and contributes to long-term glycemic control.
Inhibition of α-Amylase and α-Glucosidase Enzymes
Dietary carbohydrates must be broken down into simple sugars before absorption in the gastrointestinal tract. The enzymes α-amylase and α-glucosidase play critical roles in this digestive process. Inhibition of these enzymes slows carbohydrate digestion and glucose absorption, thereby reducing postprandial hyperglycemia.
Many medicinal plants contain polyphenols, flavonoids, tannins, and glycosides that exhibit inhibitory activity against α-amylase and α-glucosidase. By delaying carbohydrate breakdown, these phytochemicals help prevent rapid increases in blood glucose concentrations after meals. This mechanism is considered one of the most important pathways through which plant-derived compounds exert antihyperglycemic effects.
Promotion of GLUT4 Translocation and Glucose Uptake
Glucose transporter type 4 (GLUT4) is the primary insulin-responsive glucose transporter found in skeletal muscle and adipose tissue. Under normal physiological conditions, insulin stimulates the movement of GLUT4 from intracellular storage vesicles to the cell membrane, allowing glucose entry into cells.
Certain plant-derived bioactive compounds have been shown to enhance GLUT4 translocation independently or synergistically with insulin signaling pathways. Increased GLUT4 expression and membrane localization improve cellular glucose uptake and reduce circulating glucose levels. This mechanism contributes significantly to improved insulin sensitivity and enhanced metabolic regulation in diabetic conditions.
Antioxidant Effects
Oxidative stress plays a crucial role in the initiation and progression of diabetes mellitus and its complications. Chronic hyperglycemia promotes excessive production of reactive oxygen species (ROS), which can damage cellular proteins, lipids, DNA, and pancreatic β-cells.
Medicinal plants are rich sources of antioxidants, including flavonoids, phenolic acids, tannins, and terpenoids. These compounds neutralize free radicals, enhance endogenous antioxidant defenses, and reduce oxidative damage. Through their antioxidant actions, phytochemicals help preserve cellular integrity, improve insulin signaling, and protect tissues vulnerable to diabetic complications.
Anti-Inflammatory Effects
Low-grade chronic inflammation is increasingly recognized as a major contributor to insulin resistance and diabetes progression. Elevated levels of inflammatory mediators can impair insulin signaling and exacerbate metabolic dysfunction.
Various medicinal plant constituents exhibit anti-inflammatory properties by modulating signaling pathways involved in inflammatory responses. Phytochemicals such as curcumin, quercetin, and other polyphenols may suppress the production of pro-inflammatory cytokines and inhibit activation of inflammatory transcription factors. Reduction of inflammation contributes to improved insulin sensitivity and better metabolic control.
Protection and Preservation of Pancreatic β-Cells
Pancreatic β-cells are responsible for insulin production and secretion. Continuous exposure to hyperglycemia, oxidative stress, and inflammation can lead to β-cell dysfunction and apoptosis, resulting in progressive deterioration of glycemic control.
Several medicinal plants contain bioactive compounds capable of protecting β-cells against oxidative and inflammatory damage. Antioxidant phytochemicals may reduce cellular stress, preserve β-cell integrity, and support insulin-producing capacity. Some compounds have also been reported to stimulate β-cell regeneration and improve pancreatic function. Preservation of β-cell health is considered a critical strategy for slowing the progression of diabetes.
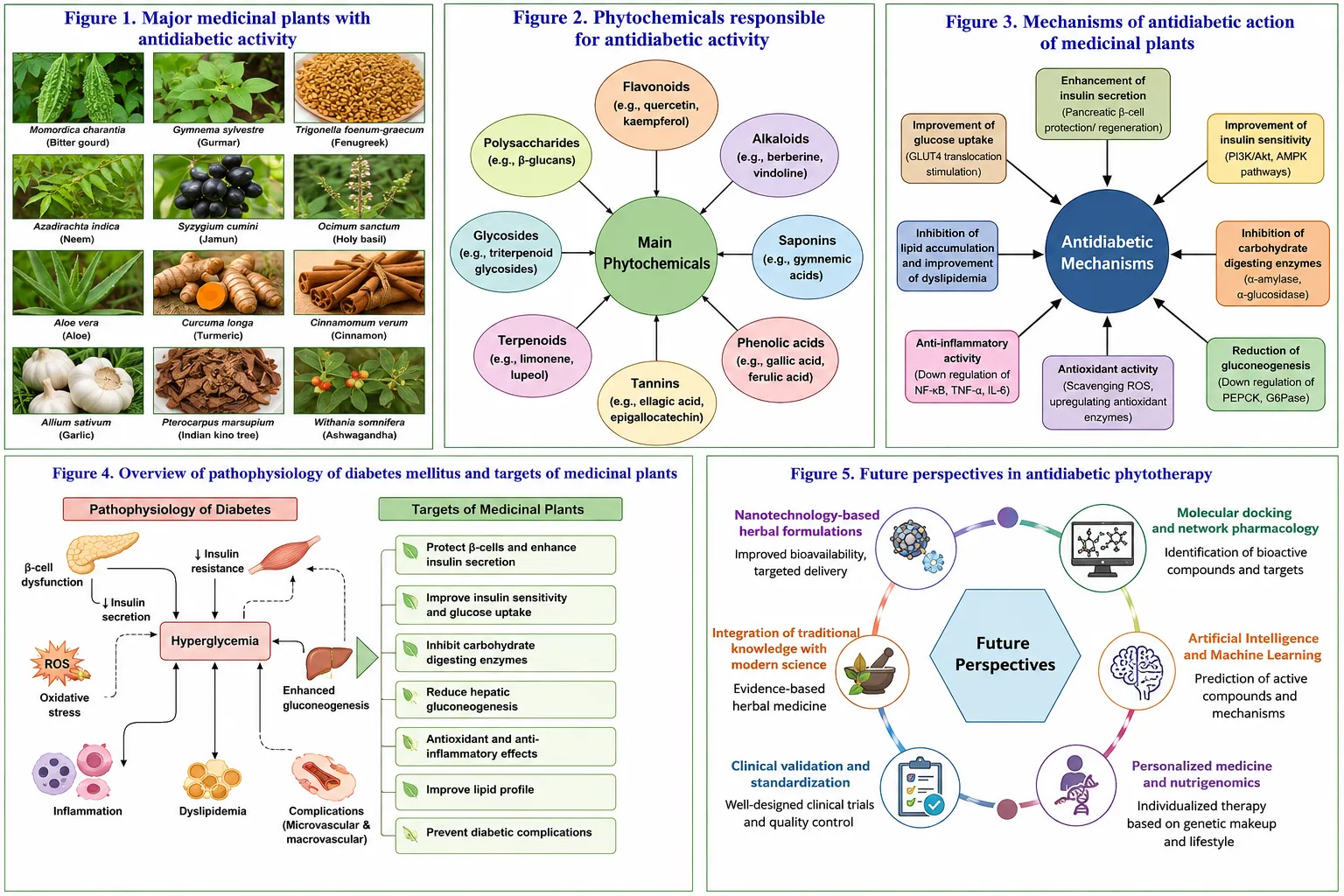
Figure 4. Overview of diabetes mellitus pathophysiology and the therapeutic targets modulated by medicinal plants.
The antidiabetic effects of medicinal plants arise from a complex interplay of multiple mechanisms targeting key pathological processes involved in diabetes mellitus. These mechanisms include stimulation of insulin secretion, enhancement of insulin sensitivity, inhibition of α-amylase and α-glucosidase enzymes, promotion of GLUT4-mediated glucose uptake, antioxidant and anti-inflammatory activities, and protection of pancreatic β-cells. The multitarget nature of phytochemicals provides a scientific basis for the traditional use of medicinal plants and highlights their potential as valuable sources for the development of future antidiabetic therapies.
Safety and Toxicity Considerations
The increasing use of medicinal plants for diabetes mellitus management has highlighted the importance of evaluating their safety and toxicity profiles. Although herbal medicines are often perceived as natural and therefore safe, this assumption is not always accurate. The safety of plant-based therapies depends on multiple factors, including plant species, phytochemical composition, dosage, duration of use, method of preparation, and individual patient characteristics. Comprehensive safety assessment is essential to ensure the effective and responsible utilization of medicinal plants in diabetes management.
Safety Concerns Associated with Medicinal Plants
Medicinal plants contain complex mixtures of bioactive compounds that may produce both therapeutic and adverse effects. Variations in cultivation conditions, harvesting practices, geographical origin, and extraction methods can influence phytochemical composition and safety profiles. In some cases, contamination with heavy metals, pesticides, microorganisms, or adulterants may pose additional health risks.
Furthermore, prolonged or excessive consumption of herbal preparations may lead to undesirable effects on various organ systems. Therefore, systematic evaluation of plant safety remains a critical component of herbal medicine research and development.
Toxicity of Medicinal Plants
Toxicity assessment is an essential aspect of evaluating medicinal plants intended for therapeutic use. Certain phytochemicals may exhibit cytotoxic, hepatotoxic, nephrotoxic, neurotoxic, or gastrointestinal effects when consumed at high doses or for extended periods. Acute toxicity refers to adverse effects resulting from short-term exposure, whereas chronic toxicity develops after long-term administration.
Preclinical toxicity studies typically evaluate parameters such as mortality, behavioral changes, organ function, histopathological alterations, and biochemical markers. These investigations help establish safe dosage ranges and identify potential toxicological concerns before clinical application. The determination of safety margins remains important for minimizing adverse outcomes associated with herbal products.
Herb–Drug Interactions
One of the major challenges associated with herbal medicine use is the potential for herb–drug interactions. Many patients use medicinal plants alongside conventional antidiabetic medications, increasing the possibility of pharmacodynamic or pharmacokinetic interactions.
Pharmacodynamic interactions occur when herbal products enhance or diminish the therapeutic effects of conventional drugs. For example, concomitant use of potent antidiabetic herbs with glucose-lowering medications may increase the risk of hypoglycemia. Pharmacokinetic interactions may result from alterations in drug absorption, distribution, metabolism, or excretion due to the influence of herbal constituents on metabolic enzymes and transport proteins.
Healthcare professionals should therefore be aware of potential interactions and encourage patients to disclose their use of herbal supplements. Further research is required to clarify interaction mechanisms and improve patient safety.
Dosage Standardization
A significant limitation of herbal medicine is the lack of universally accepted dosage standards. Variability in plant material, extraction procedures, and formulation techniques can lead to inconsistent concentrations of active constituents. Consequently, therapeutic efficacy and safety may differ between products derived from the same plant species.
Standardization aims to ensure consistent quality, potency, and safety by establishing defined concentrations of marker compounds or bioactive constituents. Reliable dosage guidelines can improve reproducibility, facilitate clinical evaluation, and reduce the risk of toxicity or therapeutic failure. The development of standardized herbal formulations remains a priority for advancing evidence-based phytotherapy.
Risk–Benefit Assessment
The therapeutic value of medicinal plants should always be evaluated in relation to their potential risks. While many plant-derived compounds demonstrate promising antidiabetic activities, safety considerations must remain central to their development and clinical application. Rigorous toxicological studies, quality assurance measures, and pharmacovigilance systems are necessary to ensure that herbal medicines provide favorable risk–benefit profiles for individuals with diabetes mellitus.
Regulatory and Quality Control Aspects
The growing popularity of herbal medicines has increased the need for robust regulatory frameworks and quality control systems. Effective regulation helps ensure the safety, efficacy, consistency, and authenticity of herbal products while protecting consumers from substandard or adulterated preparations. Regulatory oversight is particularly important in diabetes management, where long-term treatment requires reliable and standardized therapeutic products.
WHO Guidelines on Herbal Medicines
The World Health Organization has recognized the importance of traditional and herbal medicine in global healthcare and has developed guidelines to support their safe and effective use. These guidelines emphasize quality assurance, safety monitoring, standardization, proper manufacturing practices, and scientific evaluation of herbal products.
WHO recommendations encourage the implementation of Good Agricultural and Collection Practices (GACP), Good Manufacturing Practices (GMP), and pharmacovigilance systems for herbal medicines. Such measures contribute to improved product quality and consumer safety.
Standardization of Herbal Products
Standardization is a critical requirement for ensuring batch-to-batch consistency in herbal formulations. Due to natural variations in plant materials, the concentration of active constituents may differ significantly between products unless appropriate quality control measures are implemented.
Standardization involves the identification and quantification of characteristic phytochemical markers, evaluation of physicochemical properties, and establishment of quality specifications. Advanced analytical techniques such as high-performance liquid chromatography (HPLC), gas chromatography (GC), and mass spectrometry (MS) are commonly employed to assess phytochemical consistency and product quality.
Authentication of Medicinal Plants
Accurate identification and authentication of plant materials are essential for maintaining product integrity and preventing adulteration. Misidentification of plant species can compromise therapeutic efficacy and increase the risk of toxicity.
Authentication methods include macroscopic examination, microscopic analysis, phytochemical profiling, DNA-based techniques, and chromatographic fingerprinting. These approaches help verify plant identity and ensure the authenticity of raw materials used in herbal product manufacturing.
Quality Control Measures
Quality control encompasses the systematic evaluation of herbal products throughout the manufacturing process. Important quality parameters include:
Comprehensive quality control procedures help ensure that herbal medicines meet predefined safety and efficacy standards. Implementation of these measures is essential for promoting confidence among healthcare professionals, researchers, regulatory authorities, and consumers.
Regulatory Challenges
Despite significant progress, several challenges remain in the regulation of herbal medicines. Differences in national regulatory frameworks, limited standardization, insufficient safety data, and variability in product quality continue to hinder global harmonization. Addressing these challenges will require collaboration among researchers, regulatory agencies, manufacturers, and healthcare providers to establish internationally recognized quality standards and evidence-based guidelines.
Future Perspectives
The growing scientific interest in medicinal plants has created new opportunities for the discovery and development of innovative antidiabetic therapies. Advances in phytochemistry, biotechnology, computational biology, and pharmaceutical sciences are expected to accelerate the identification of novel plant-derived compounds and improve their therapeutic applications.
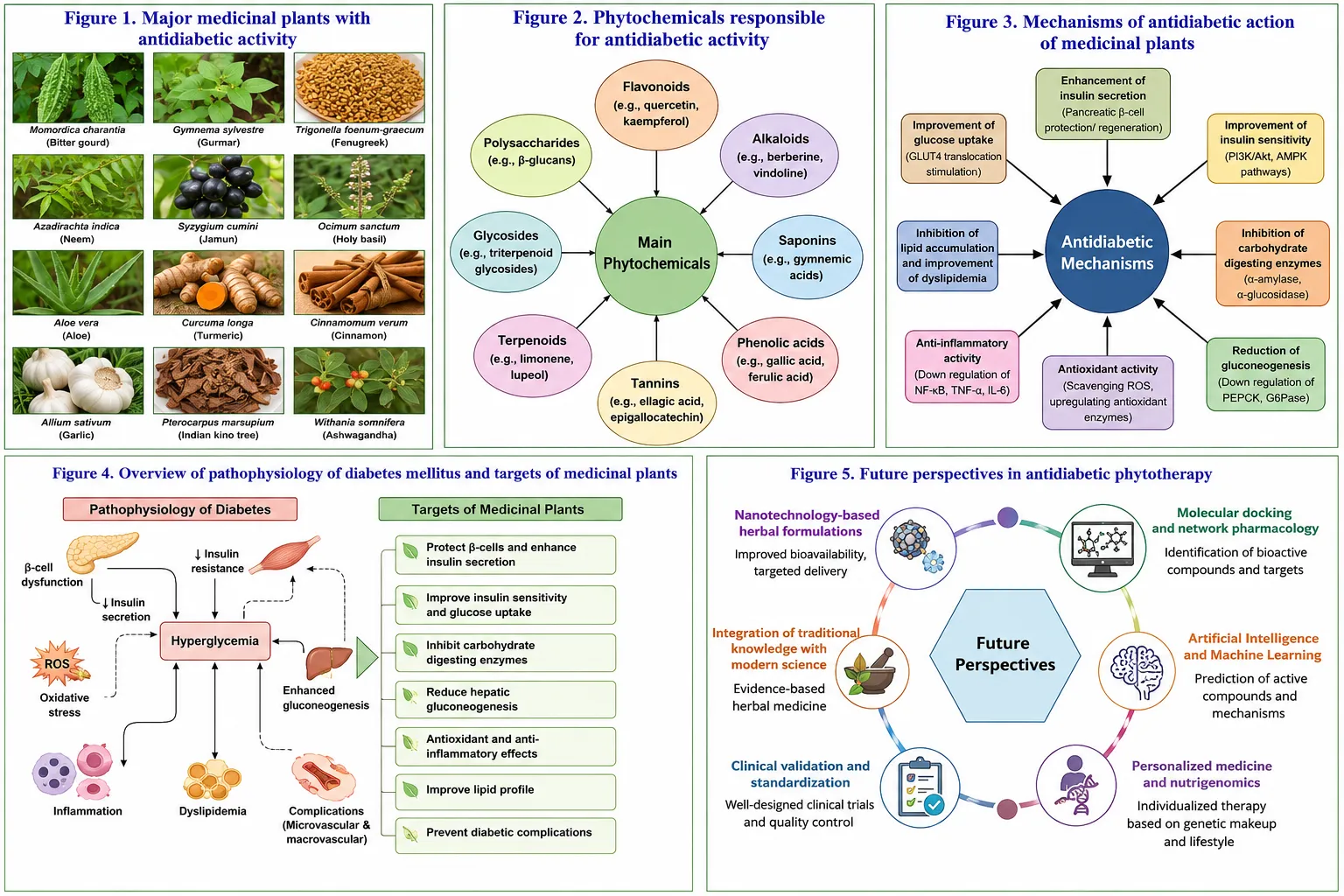
Figure 5. Emerging trends in medicinal plant research, including nanotechnology, molecular docking, artificial intelligence, and personalized herbal medicine.
Discovery of Novel Phytochemicals
Medicinal plants remain a rich source of structurally diverse bioactive compounds with potential antidiabetic properties. Continued exploration of plant biodiversity may lead to the identification of previously unknown phytochemicals capable of targeting multiple pathways involved in diabetes pathogenesis.
Modern analytical technologies facilitate the characterization of complex phytochemical mixtures and support the discovery of new lead compounds for drug development. Future research is likely to focus on identifying molecules with improved efficacy, safety, and pharmacokinetic profiles.
Nanotechnology-Based Herbal Drug Delivery
Nanotechnology offers promising approaches for enhancing the therapeutic performance of plant-derived compounds. Many phytochemicals exhibit limited solubility, poor bioavailability, and rapid degradation, which can restrict their clinical usefulness.
Nanoformulations such as nanoparticles, nanoemulsions, liposomes, and phytosomes may improve stability, absorption, targeted delivery, and controlled release of herbal constituents. These advanced delivery systems have the potential to increase therapeutic efficacy while minimizing adverse effects.
Artificial Intelligence-Assisted Screening
Artificial intelligence (AI) and machine learning technologies are increasingly being utilized in natural product research. AI-assisted screening can analyze large datasets, identify promising phytochemicals, predict biological activities, and accelerate drug discovery processes.
By integrating phytochemical databases with computational models, researchers can prioritize candidate compounds for experimental validation, thereby reducing time and resource requirements. AI-driven approaches are expected to play an increasingly important role in the future development of plant-based antidiabetic therapies.
Molecular Docking and Computational Approaches
Molecular docking has become a valuable tool for investigating interactions between phytochemicals and biological targets associated with diabetes. Computational methods allow researchers to predict binding affinities, identify potential mechanisms of action, and optimize lead compounds before laboratory testing.
The integration of molecular docking, molecular dynamics simulations, and network pharmacology can provide deeper insights into the multitarget actions of medicinal plants and facilitate the rational design of novel therapeutic agents.
Personalized Herbal Medicine
Advances in genomics, metabolomics, and precision medicine are creating opportunities for personalized approaches to herbal therapy. Individual variations in genetics, metabolism, lifestyle, and disease characteristics may influence responses to plant-derived treatments.
Future personalized herbal medicine strategies may involve selecting specific medicinal plants or phytochemical combinations based on patient-specific biological profiles. Such approaches have the potential to improve therapeutic outcomes while minimizing adverse effects.
Integration of Traditional Knowledge and Modern Science
Traditional medical systems contain extensive knowledge regarding the use of medicinal plants for metabolic disorders. Future research should emphasize the integration of traditional knowledge with modern scientific methodologies to validate therapeutic claims and identify new treatment opportunities.
Collaborative efforts involving ethnobotany, pharmacology, phytochemistry, biotechnology, and clinical sciences may facilitate the development of evidence-based herbal medicines that combine historical experience with contemporary scientific understanding.
Conclusion of Future Perspectives
The future of medicinal plant research in diabetes mellitus management is promising and multidisciplinary. Innovations in phytochemical discovery, nanotechnology, artificial intelligence, molecular modeling, and personalized medicine are expected to transform the development of plant-based therapeutics. Combined with rigorous safety evaluation, quality control, and regulatory oversight, these advancements may contribute significantly to the development of effective and scientifically validated herbal interventions for diabetes mellitus.
CONCLUSION
Diabetes mellitus remains one of the most prevalent and challenging metabolic disorders worldwide, with significant implications for public health, healthcare systems, and patient quality of life. Despite considerable advances in conventional pharmacotherapy, the increasing burden of diabetes and the limitations associated with current treatment options continue to stimulate interest in alternative and complementary therapeutic approaches. Among these, medicinal plants have emerged as valuable sources of bioactive compounds with potential applications in diabetes management.
The literature reviewed in this article highlights the extensive diversity of medicinal plants traditionally used for glycemic control and the growing scientific evidence supporting their pharmacological potential. Numerous plant-derived phytochemicals, including flavonoids, alkaloids, saponins, terpenoids, phenolic compounds, and glycosides, have demonstrated the ability to influence key pathways involved in glucose metabolism. These compounds exert antidiabetic effects through multiple mechanisms, including stimulation of insulin secretion, enhancement of insulin sensitivity, inhibition of carbohydrate-digesting enzymes, promotion of glucose uptake via GLUT4 translocation, attenuation of oxidative stress, suppression of inflammatory responses, and protection of pancreatic β-cell function.
A major advantage of medicinal plants lies in their multitarget mode of action, which may be particularly beneficial in addressing the complex and multifactorial nature of diabetes mellitus. Unlike many conventional therapies that focus on a single molecular target, plant-derived compounds frequently interact with multiple biochemical pathways simultaneously. This characteristic offers opportunities for developing holistic therapeutic strategies capable of improving metabolic regulation and reducing the progression of diabetes-related complications.
However, several challenges must be addressed before medicinal plants can be fully integrated into evidence-based diabetes management. Variability in phytochemical composition, differences in cultivation and processing practices, inadequate standardization, potential toxicity, and herb–drug interactions remain important concerns. The lack of universally accepted quality standards and regulatory harmonization further complicates the clinical translation of many herbal products. Therefore, rigorous safety assessments, toxicological investigations, authentication procedures, and quality control measures are essential to ensure the reliability and reproducibility of herbal therapies.
Recent advances in phytochemistry, biotechnology, nanotechnology, artificial intelligence, molecular docking, and systems pharmacology have created new opportunities for accelerating medicinal plant research. These technologies facilitate the identification of novel bioactive compounds, prediction of molecular targets, optimization of drug delivery systems, and development of personalized therapeutic approaches. Such innovations are expected to strengthen the scientific foundation of herbal medicine and enhance its role in future diabetes care.
Future research should focus on comprehensive phytochemical characterization, mechanistic investigations, standardization of herbal formulations, long-term safety evaluation, and the establishment of internationally recognized regulatory frameworks. Greater collaboration among pharmacologists, phytochemists, toxicologists, clinicians, computational scientists, and regulatory authorities will be necessary to translate promising laboratory findings into safe and effective therapeutic products.
In conclusion, medicinal plants represent a valuable reservoir of bioactive molecules with significant potential for diabetes mellitus management. Their diverse phytochemical composition and multifaceted mechanisms of action provide a strong scientific rationale for continued investigation. With advances in research methodologies, quality assurance practices, and innovative technologies, medicinal plants may contribute substantially to the development of future antidiabetic therapies and support a more comprehensive approach to diabetes management.
REFERENCES

Shalini Devi, Mohamed Osman, Jyoti Gupta, Nisha Devi, Medicinal Plants in Diabetes Mellitus Management: Phytochemistry, Mechanisms of Action, Safety Considerations, and Future Perspectives—A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4255-4275, https://doi.org/10.5281/zenodo.20730951
 10.5281/zenodo.20730951
10.5281/zenodo.20730951