
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Kalyani Charitable Trust's, R.G Sapkal College of Pharmacy, Sapkal Knowledge Hub, Kalyani Hills, Anjaneri, Trimbakeshwar Road, Nashik, 422213, Maharashtra, India.
Nanocochleates represent a unique and promising class of lipid-based drug delivery systems (LBDDS) characterized by their distinctive tightly rolled, multilayered cylindrical structure. Formed through the electrostatic interaction of anionic phospholipids most commonly phosphatidylserine (PS) with divalent cations such as calcium (Ca²?), nanocochleates offer a solid, anhydrous lipid matrix that is fundamentally different from conventional liposomes. This structural distinction confers exceptional physicochemical stability, protection of encapsulated therapeutics from enzymatic degradation, harsh pH environments, and oxidative stress. This comprehensive review traces the historical development of nanocochleates from their discovery by Papahadjopoulos in the 1970s through to their modern nanoscale formulations. We systematically examine their composition, methods of preparation, characterization strategies, mechanisms of drug release, and routes of administration. Therapeutic applications are evaluated across antifungal, anticancer, antiviral, gene delivery, vaccine adjuvant, and protein delivery domains, with special emphasis on the landmark cochleate-based amphotericin B (CAMB) formulation. The review also benchmarks nanocochleates against other lipid-based platforms, critically appraises existing limitations, and proposes a roadmap for future clinical translation. Emerging data indicate that nanocochleates are well-positioned to address critical unmet needs in oral delivery of hydrophobic drugs and nucleic acid-based therapeutics. With advances in surface functionalization and stimuli-responsive design, nanocochleates hold considerable promise for the next generation of precision drug delivery.
Drug delivery science occupies a central role in modern pharmaceutical development. Despite decades of advances in medicinal chemistry and biotechnology, a substantial fraction of newly discovered therapeutic agents fail to translate into clinical benefit due to poor aqueous solubility, rapid systemic clearance, unfavourable pharmacokinetics, or susceptibility to pre-systemic degradation.
Among the most challenging categories are Biopharmaceutics Classification System (BCS) Class II and IV compounds poorly water-soluble drugs that account for nearly 40% of marketed pharmaceuticals and up to 90% of drug candidates in discovery pipelines. [1] These agents demand sophisticated formulation strategies to achieve therapeutic plasma concentrations.
Lipid-based drug delivery systems (LBDDS) have emerged as a versatile and clinically validated strategy to overcome these barriers. Liposomes, solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), self-emulsifying drug delivery systems (SEDDS), and lipid nanoparticles (LNPs) have each contributed meaningful advances to the field. However, each platform comes with its own limitations liposomes suffer from aqueous instability and drug leakage; SLNs exhibit polymorphic transitions during storage; and LNPs require cold-chain logistics.
Nanocochleates offer a paradigm-shifting alternative. First conceptualized as "cochleate cylinders" by Dimitrios Papahadjopoulos in the 1970s, these structures were later refined and nano-engineered by Bhosale and colleagues, and commercialized by BioDelivery Sciences International (BDSI). [2] Unlike liposomes, nanocochleates are solid, anhydrous multilayer lipid structures with no internal aqueous compartment, making them inherently resistant to degradation by water, oxygen, and digestive enzymes.
This review aims to provide the most comprehensive, up-to-date synthesis of knowledge on nanocochleates, covering their structural biology, formulation science, mechanistic pharmacology, and therapeutic landscape, while identifying key scientific and regulatory gaps that must be addressed before their full clinical potential is realized.
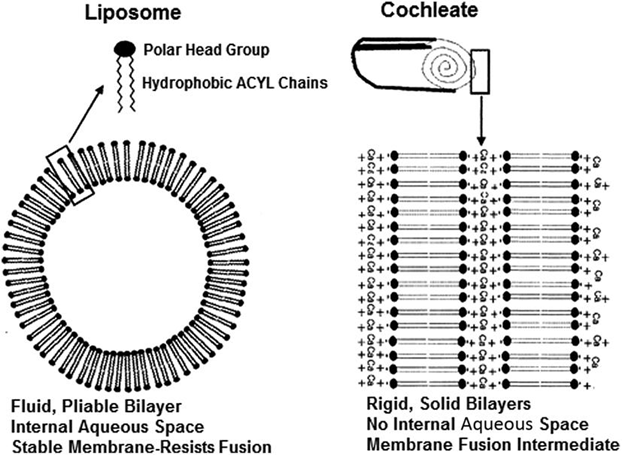
Figure 1: Structural Comparison Between Liposomes and Nanocochleates
2. Historical Background and Development:
2.1 Discovery of Cochleate Cylinders
The foundational work on cochleate cylinders was conducted by Papahadjopoulos and colleagues in the mid-1970s. Studying the interaction of phosphatidylserine (PS) membranes with divalent cations particularly calcium they observed that Ca²⁺ induced an irreversible phase transition in the lipid bilayer, resulting in the formation of tightly packed, rolled lipid sheets. [3] These cylindrical structures were named "cochleates" (from the Latin cochlea, meaning snail shell) due to their spiral, helical morphology observed under electron microscopy.
2.2 Evolution to Nanocochleates
For two decades, cochleates remained largely a biophysical curiosity. Their potential as drug delivery vehicles was first systematically explored by Bhosale et al. and later expanded by Zarif and Mannino in the 1990s and early 2000s. [4] The key innovation was reducing cochleate particle dimensions from the micrometre scale to the nanometre scale typically 50–500 nm to enable parenteral administration and enhance cellular uptake via endocytic pathways.
BioDelivery Sciences International (BDSI) spearheaded the clinical translation of this platform, developing cochleate-encapsulated amphotericin B (CAMB) as a lead product. CAMB offered systemic antifungal activity with a substantially improved safety profile compared to conventional amphotericin B formulations, providing proof-of-concept for nanocochleates as a clinically viable drug delivery platform. [5]
2.3 Key Milestones
Table 1: Historical Development and Major Milestones in Nanocochleate Research and Drug Delivery Applications
|
Year |
Milestone |
Key Investigator(s) |
|
1975 |
Discovery of cochleate cylinders from PS-Ca²⁺ interaction |
Papahadjopoulos et al. |
|
1996 |
First drug encapsulation into cochleates (amphotericin B) |
Zarif, Mannino |
|
2000 |
Nano-sizing and characterization advances |
Bhosale et al. |
|
2004 |
CAMB Phase I clinical trials initiated |
BDSI |
|
2010 |
Gene delivery via cochleates demonstrated |
Gould-Fogerite et al. |
|
2016 |
Oral nanocochleates for protein/peptide delivery |
Various groups |
|
2020–present |
Stimuli-responsive and targeted nanocochleates |
Emerging research |
3. Structure and Physicochemical Properties:
3.1 Structural Architecture
The nanocochleate is a solid, multilamellar lipid structure consisting of continuous, tightly wound lipid bilayer sheets rolled into a spiral cylinder. Crucially, there is no internal aqueous space the entire volume is occupied by densely packed lipid lamellae intercalated with divalent cations. [6] This anhydrous solid-state architecture distinguishes nanocochleates from all vesicular drug carriers.
3.2 Role of Divalent Cations
Divalent cations particularly Ca²⁺ serve as the molecular "zipper" that condenses and rolls the anionic phospholipid bilayer sheets. The positively charged cations neutralize the negatively charged phospholipid head groups, inducing dehydration of the lipid surface, lateral compression, and spontaneous rolling into the cochleate morphology. [7]
Other divalent cations studied include Zn²⁺, Mg²⁺, Ba²⁺, and Fe²⁺. Calcium remains the most widely used due to its biocompatibility, physiological relevance, and optimal binding affinity for PS head groups. The choice of cation influences the inter-lamellar spacing, thermal stability, and drug release kinetics of the resulting nanocochleates.
3.3 Key Physicochemical Parameters
Table 2: Key Physicochemical Parameters and Their Significance in Nanocochleate Characterization
|
Parameter |
Typical Range |
Significance |
|
Particle size |
50–500 nm |
Governs biodistribution, cellular uptake, and route of administration |
|
Polydispersity index (PDI) |
< 0.3 |
Indicates size uniformity; lower PDI = better batch consistency |
|
Zeta potential |
−20 to −40 mV |
Reflects surface charge; drives electrostatic stability |
|
Lamellar repeat spacing |
~5–6 nm |
Measured by SAXS/XRD; confirms bilayer packing |
|
Entrapment efficiency |
60–95% (hydrophobic) |
Depends on lipid composition and drug physicochemistry |
|
Water content |
Near ze |
Critical for stability; anhydrous core resists hydrolysis |
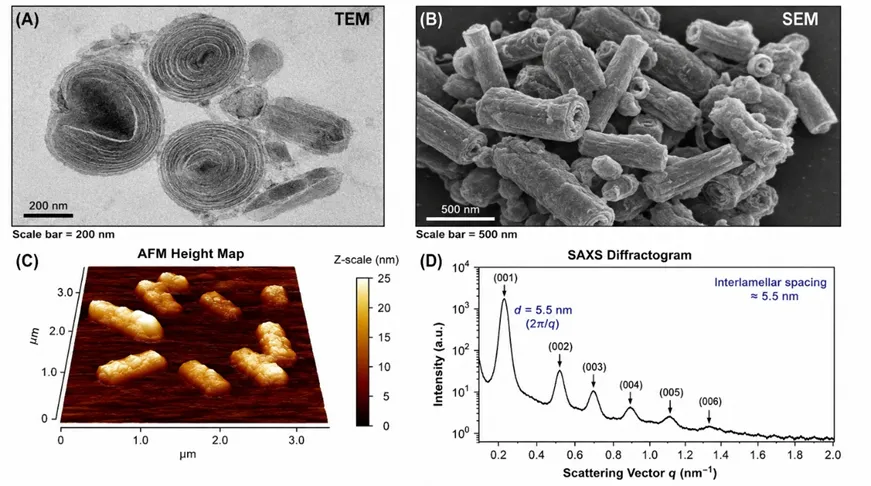
Figure 2: Electron microscopic and structural characterization of nanocochleates: (A) TEM image showing tightly wound cylindrical morphology with lamellar fringes (200 nm scale bar); (B) SEM image illustrating surface morphology and particle distribution; (C) AFM height map confirming nano-scale dimensions; and (D) SAXS diffractogram showing Bragg peaks corresponding to ~5.5 nm interlamellar spacing, confirming crystalline bilayer packing
4. Composition and Materials:
4.1 Lipid Components
Phosphatidylserine (PS) is the archetypal lipid for nanocochleate formation due to its strong anionic character at physiological pH (net charge −1), high affinity for Ca²⁺, and biological abundance. [8] Both synthetic (DOPS: 1,2-dioleoyl-sn-glycero-3-phospho-L-serine; DPPS: 1,2-dipalmitoyl-sn-glycero-3-phospho-L-serine) and soy-derived PS have been employed. Soy-PS offers cost-effectiveness for scale-up, while synthetic PS variants provide precise lipid purity and reproducibility.
Other anionic phospholipids explored include phosphatidic acid (PA), phosphatidylglycerol (PG), and phosphatidylinositol (PI). Neutral co-lipids such as phosphatidylcholine (PC) and phosphatidylethanolamine (PE) are sometimes incorporated at defined molar ratios to modulate membrane fluidity, drug loading capacity, and in vivo performance. [9]
4.2 Divalent Cations Role and Selection Criteria
The ideal divalent cation for nanocochleate formation should: (i) demonstrate strong binding affinity for the target anionic lipid; (ii) be biocompatible at the concentrations employed; (iii) not interfere with drug stability; and (iv) support the desired release profile. Calcium is preferred across most formulations due to its physiological ubiquity and regulatory familiarity. Zinc has been explored for its additional antimicrobial properties, while magnesium is used in formulations where lower structural rigidity is desired.
4.3 Encapsulated Molecules
Table 3: Drug Classes, Representative Examples, and Loading Mechanisms in Nanocochleate Delivery Systems
|
Drug Class |
Examples |
Mechanism of Loading |
|
Hydrophobic small molecules |
Amphotericin B, paclitaxel, curcumin, all-trans retinoic acid |
Intercalation between lipid bilayers |
|
Hydrophilic drugs |
Gentamicin, ara-C, antisense oligonucleotides |
Partial entrapment; modified PS ratio |
|
Proteins & peptides |
Insulin, bovine serum albumin, cytokines |
Encapsulation during formation |
|
Nucleic acids |
Plasmid DNA, siRNA, mRNA |
Electrostatic complexation with lipid |
|
Vaccines/ antigens |
Protein subunit antigens, adjuvants |
Co-formulation with PS matrix |
5. Mechanism of Formation:
5.1 Electrostatic Condensation
Nanocochleate formation is driven by the electrostatic neutralization of negatively charged PS head groups by divalent cations. When Ca²⁺ is introduced to a PS liposome suspension, it bridges adjacent phospholipid molecules, eliminating the repulsive forces that maintain the bilayer in its hydrated vesicular form. [10] This results in dehydration of the lipid surface, reduction of inter-headgroup distance, and a transition from the lamellar-fluid (Lα) to the crystalline (Lc) phase.
5.2 Bilayer Sheet Rolling
The condensation of the lipid bilayer generates mechanical stress due to asymmetric dehydration at the membrane surface. This stress is relieved by the spontaneous rolling of the flattened bilayer sheet into a cylindrical cochleate structure. The rolling is thermodynamically favourable as it minimises exposed hydrophobic edges. Sequential wrapping of additional bilayer sheets around the growing cylinder produces the characteristic multilayer architecture observed by electron microscopy.
5.3 Liposome → Cochleate → Nanocochleate Transition
The lipid-to-cation molar ratio is the most critical formulation variable governing cochleate morphology. Excess cation leads to over-condensation and aggregation, while insufficient cation results in incomplete cochleate formation and residual liposomes. Optimal Ca²⁺:PS ratios typically range from 1:1 to 2:1 (mol/mol), depending on the specific lipid composition employed. [11]
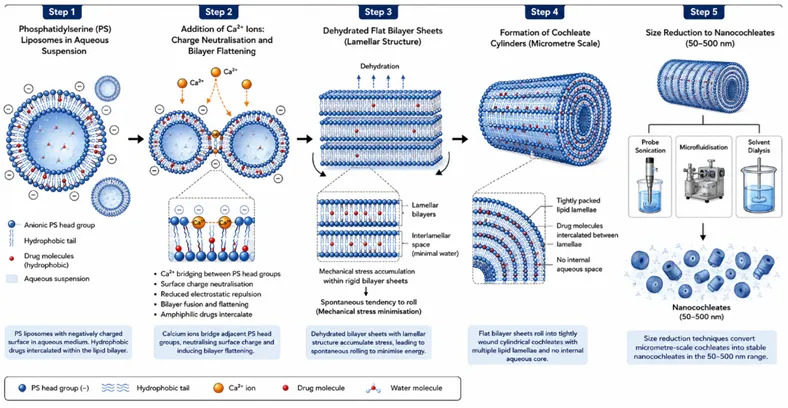
Figure 3: Stepwise Mechanism of Nanocochleate Formation from Phosphatidylserine Liposomes
6. Methods of Preparation:
6.1 Trapping Method
The trapping method is the most widely described approach for nanocochleate preparation. PS liposomes are first prepared by thin-film hydration and extrusion. Drug is loaded during liposome formation (for lipophilic agents) or post-insertion. Calcium chloride is then added dropwise to the liposome suspension under gentle stirring, inducing cochleate formation. [12] The resulting cochleates are collected by centrifugation, washed to remove unencapsulated drug and excess Ca²⁺, and then subjected to probe sonication or high-pressure homogenisation to achieve nanocochleate dimensions.
6.2 Hydrogel Method
The hydrogel method employs a dialysis membrane to slowly introduce Ca²⁺ into a PS liposome suspension through a calcium-containing agarose hydrogel. The slow, controlled release of Ca²⁺ across the gel matrix facilitates the gradual formation of cochleates with more uniform morphology and narrower size distribution compared to direct addition. [13]
6.3 Direct Calcium Dialysis Method
In this technique, PS liposomes are placed inside a dialysis membrane and dialysed against a calcium chloride buffer. The transmembrane calcium gradient drives uniform penetration of Ca²⁺ into the liposome suspension, resulting in cochleate formation with high batch-to-batch reproducibility. This method is particularly suited for encapsulation of fragile biologics that may be damaged by mechanical processing.
6.4 Solvent Injection / Microfluidics
Solvent injection involves the rapid injection of lipid dissolved in an organic solvent (e.g., ethanol) into an aqueous phase containing Ca²⁺ and the drug. The solvent displacement drives self-assembly of nanocochleates in a single step without the intermediate liposome stage. [14] Microfluidic platforms have been adapted to perform this process in a controlled, scalable manner using laminar flow mixing devices, enabling precise control of nanocochleate size and composition.
6.5 Binary Aqueous-Aqueous System
This emerging approach exploits the biphasic separation of two incompatible aqueous polymer phases (e.g., PEG and dextran) to confine and concentrate lipid-Ca²⁺ interactions within defined micro-compartments, resulting in nanocochleate formation without organic solvents. This method is particularly promising for pharmaceutical manufacturing where solvent residues are a regulatory concern.
6.6 Comparative Summary of Preparation Methods
Table 4: Comparative Overview of Preparation Methods for Nanocochleate Formulations
|
Method |
Size Control |
Scalability |
Drug Compatibility |
Key Limitation |
|
Trapping |
Moderate |
Moderate |
Lipophilic +++ |
Batch variability |
|
Hydrogel |
Good |
Low |
Fragile biologics +++ |
Low throughput |
|
Calcium dialysis |
Good |
Moderate |
Broad spectrum |
Long process time |
|
Solvent injection / Microfluidics |
Excellent |
High |
Moderate |
Solvent residues |
|
Binary aqueous-aqueous |
Good |
Moderate |
Broad spectrum |
Emerging; limited data |
7. Drug Loading and Encapsulation:
7.1 Hydrophobic Drug Intercalation
The primary mechanism by which nanocochleates encapsulate hydrophobic drugs is intercalation of drug molecules within the hydrophobic lipid bilayer core during the liposome formation stage. Drug-lipid co-dissolution in an organic solvent, followed by thin-film formation and hydration, ensures intimate drug-lipid association. [15] Entrapment efficiencies for highly lipophilic drugs (log P > 3) typically exceed 80%, driven by their thermodynamic preference for the anhydrous lipid environment.
7.2 Encapsulation of Hydrophilic Molecules
Hydrophilic drug encapsulation in nanocochleates is inherently challenging due to the absence of an aqueous core. Strategies employed include: (i) formation of drug-lipid ion pairs to improve lipid partitioning; (ii) use of modified PS ratios with neutral phospholipids to create hydrophilic domains; and (iii) incorporation of pH-sensitive lipids that create transient hydrophilic pockets. Entrapment efficiencies for hydrophilic drugs typically range from 20–60%.
7.3 Factors Affecting Drug Loading
8. Characterization Techniques:
Comprehensive physicochemical characterization is essential to confirm nanocochleate formation, assess product quality, and predict in vivo performance. A multi-modal approach is recommended, combining structural, morphological, thermal, and analytical techniques.
Table 5: Analytical Techniques and Key Characterization Parameters for Nanocochleate Formulations
|
Parameter |
Technique(s) |
Key Information Obtained |
|
Size & morphology |
TEM, SEM, AFM |
Cylindrical morphology, lamellar fringes, surface texture, nano-scale dimensions |
|
Particle size & PDI |
Dynamic Light Scattering (DLS) |
Hydrodynamic diameter, polydispersity index, colloidal stability over time |
|
Surface charge |
Zeta potential (laser Doppler electrophoresis) |
Electrostatic stability; values below −20 mV indicate adequate repulsion |
|
Drug content & EE |
HPLC, UV-Vis spectrophotometry |
Quantitative drug encapsulation and loading efficiency |
|
Thermal analysis |
DSC, TGA |
Phase transitions, thermal stability, lipid crystallinity, water content |
|
Structural confirmation |
FTIR spectroscopy |
Lipid-drug interactions, phosphate head group shifts, Ca²⁺ coordination |
|
Lamellar spacing |
SAXS / Powder XRD |
Bilayer repeat spacing (~5–6 nm); confirms cochleate crystalline packing |
|
In vitro drug release |
Dialysis membrane / Franz diffusion cell |
Release kinetics; pH-dependent and ion-exchange-triggered release profiles |
|
Stability |
Accelerated stability studies (40°C/75%RH) |
Long-term shelf-life prediction, aggregation tendency |
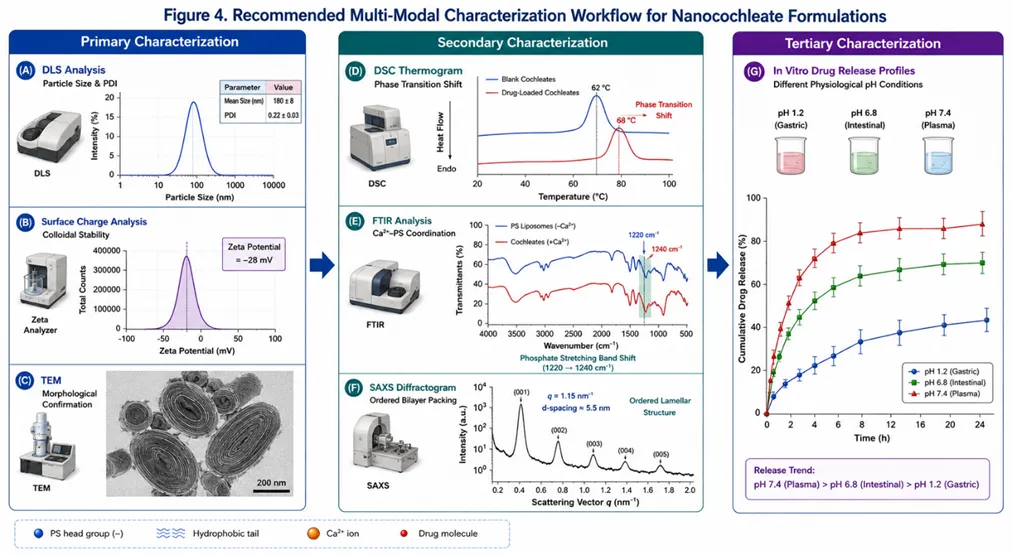
Figure 4: Recommended Multi-Modal Characterization Workflow for Nanocochleate Formulations
9. Mechanisms of Drug Release and Cellular Uptake:
9.1 Ion Exchange-Driven Release
The primary trigger for nanocochleate disassembly in biological environments is displacement of the bridging Ca²⁺ ions by monovalent cations or by endogenous Ca²⁺ chelators. When nanocochleates encounter intracellular environments rich in sodium and potassium ions, or lipid membranes rich in phosphatidylcholine, the Ca²⁺ bridges are progressively disrupted, allowing the lipid lamellae to unfurl and release the encapsulated drug. [19]
9.2 pH-Dependent Release
The stability of the Ca²⁺-PS electrostatic complex is pH-dependent. At the acidic pH of the stomach (pH 1.2–2.0), PS becomes protonated and the Ca²⁺-lipid interaction weakens slightly, yet the anhydrous lipid matrix still provides adequate protection against acid degradation a key advantage over acid-labile formulations. At intestinal pH (6.5–7.4), controlled release is initiated by ion exchange with endogenous bicarbonate ions.
9.3 Endocytic Pathways and Cellular Uptake
Following oral or systemic administration, nanocochleates interact with cell membranes through multiple endocytic mechanisms. Micropinocytosis is the predominant pathway for nanocochleates, particularly for particles in the 200–500 nm range. [20] Clathrin-mediated endocytosis and caveolin-dependent pathways also contribute, depending on particle size and surface properties.
A critically important feature of nanocochleate uptake is their ability to bypass lysosomal degradation. Unlike conventional liposomes that are trafficked to lysosomes (pH 4.5–5.0) where their lipid bilayer is digested by phospholipases, nanocochleates are released into the cytoplasm prior to lysosomal fusion, enabling direct cytoplasmic drug delivery. This property is especially valuable for nucleic acid and protein cargo.
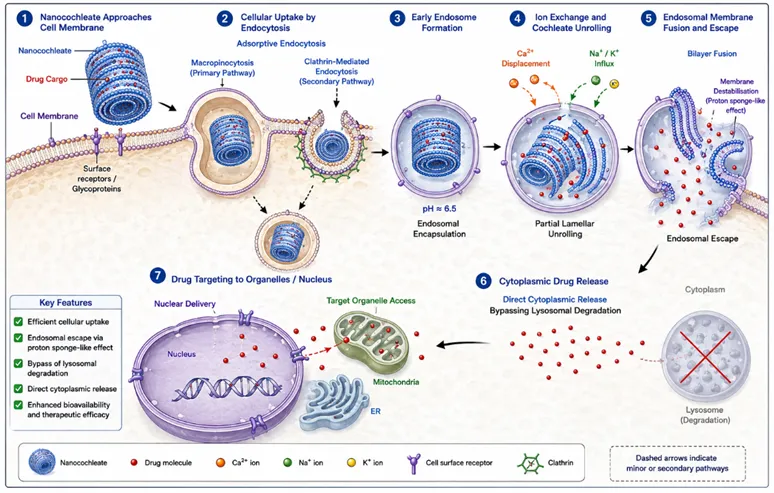
Figure 5: Cellular Uptake and Intracellular Release Mechanism of Nanocochleates
10. Routes of Administration:
10.1 Oral Delivery
Oral delivery represents the most extensively investigated route for nanocochleates and their most compelling clinical opportunity. The anhydrous solid lipid matrix provides robust protection against gastric acid (pH 1.2), pepsin, pancreatic proteases, and bile salts conditions that rapidly degrade conventional liposomes and emulsions. [21] Following gastric transit, nanocochleates are absorbed in the small intestine via the transcellular pathway and lymphatic uptake through Peyer's patches (M-cells), enabling bypass of first-pass hepatic metabolism.
10.2 Parenteral Delivery
Intravenous and intramuscular administration of nanocochleates have been explored for antifungal and antiviral applications. The negative surface charge (zeta potential ~ −30 mV) and nano-scale dimensions (< 200 nm for IV use) facilitate prolonged circulation by reducing opsonisation and macrophage clearance. [22]
10.3 Topical and Transdermal Delivery
The lipid bilayer composition of nanocochleates is inherently compatible with the stratum corneum lipid matrix, facilitating percutaneous penetration. Nanocochleates loaded with antifungal agents (e.g., fluconazole, ketoconazole) have shown enhanced skin penetration in ex vivo studies. Their nano-scale dimensions (< 300 nm) allow penetration through follicular pathways and intercellular lipid channels.
10.4 Pulmonary Delivery
Inhalable nanocochleate formulations are under early investigation for pulmonary fungal infections (e.g., Aspergillus) and lung cancer. Spray-dried nanocochleate powders with optimal aerodynamic particle sizes (mass median aerodynamic diameter 1–5 μm) have been formulated using mannitol as a carrier. The solid lipid matrix resists denaturation during spray-drying, preserving drug integrity.
10.5 Ocular Delivery
The emerging application of nanocochleates in ophthalmic drug delivery exploits their mucoadhesive properties and lipid compatibility with the corneal epithelium. Nanocochleate formulations of antifungal and anti-inflammatory agents have demonstrated extended precorneal residence and enhanced transcorneal penetration in preliminary studies.
11. Therapeutic Applications:
11.1 Antifungal Therapy The Flagship Application
The most extensively studied and clinically advanced application of nanocochleates is the encapsulation of amphotericin B (AmB) cochleate-encapsulated amphotericin B (CAMB). AmB is the gold standard antifungal for invasive fungal infections, but its clinical use is severely limited by dose-dependent nephrotoxicity and infusion reactions associated with conventional deoxycholate formulation (Fungizone). [23]
CAMB, when administered orally in murine models of disseminated candidiasis and aspergillosis, demonstrated antifungal efficacy comparable to IV liposomal AmB (AmBisome) with markedly reduced nephrotoxicity and improved tolerability. [24] The oral bioavailability of AmB in CAMB is substantially higher than all previously reported oral AmB formulations a major unmet clinical need, as oral antifungal therapy for invasive infections remains limited to azoles.
11.2 Anticancer Drug Delivery
Nanocochleates have been investigated as carriers for poorly water-soluble anticancer agents including paclitaxel, curcumin, all-trans retinoic acid (ATRA), and doxorubicin. [25] The intercalation of these hydrophobic agents within the lipid lamellae confers aqueous dispersibility, protects against metabolic inactivation, and enables passive tumour targeting via the enhanced permeability and retention (EPR) effect.
Curcumin-loaded nanocochleates have shown 4–8-fold enhancement in oral bioavailability compared to free curcumin in rodent studies, translating to significantly greater antitumour activity in xenograft models. Paclitaxel nanocochleates have demonstrated comparable in vitro cytotoxicity to Taxol with markedly improved solubility profile.
11.3 Antiviral Therapy
Early proof-of-concept studies demonstrated that nanocochleates could deliver antiretroviral agents (e.g., saquinavir, ritonavir) to HIV-infected macrophages in vitro, exploiting the macro pinocytic preference of macrophages for nanocochleate uptake. [26] Nanocochleate formulations of antiviral peptides and nucleoside analogues for hepatitis C virus (HCV) are also being explored, targeting the hepatic reservoir.
11.4 Gene and Nucleic Acid Delivery
Gould-Fogerite and colleagues demonstrated that cochleates could efficiently deliver plasmid DNA to mammalian cells in vitro, with transfection efficiencies comparable to lipofection but with substantially lower cytotoxicity. [27] Subsequent studies extended this platform to siRNA delivery, where the multilayered lipid matrix protects the fragile RNA cargo from serum nucleases and pH-induced degradation a critical advantage over conventional lipoplexes.
11.5 Vaccine Adjuvants and Immunotherapy
The particulate nature of nanocochleates makes them efficient adjuvant systems for subunit vaccines. Their uptake by dendritic cells and macrophages via macropinocytosis facilitates antigen processing and presentation on both MHC class I and class II pathways, enabling both humoral and cellular immune responses. [28] Intranasal administration of antigen-loaded nanocochleates has elicited strong mucosal IgA responses in addition to systemic immunity, a significant advantage for vaccines against mucosal pathogens.
11.6 Antimicrobial Applications
Nanocochleates loaded with aminoglycosides (gentamicin), polymyxins, and beta-lactams have been explored for treatment of multi-drug resistant (MDR) bacterial infections. The lipid envelope facilitates interaction with and disruption of bacterial membranes, potentially restoring susceptibility of resistant organisms. Zinc-cochleates have demonstrated intrinsic antibiofilm activity attributed to the dual antimicrobial properties of Zn²⁺ and the lipid carrier.
11.7 Protein and Peptide Delivery
Oral delivery of proteins remains one of the most significant challenges in drug delivery due to proteolytic degradation and poor intestinal permeability. Nanocochleates offer protection from gastric and intestinal proteases by physically shielding the protein within the solid lipid matrix. [29] Insulin-loaded nanocochleates administered orally to diabetic rats produced statistically significant and dose-dependent blood glucose reduction, demonstrating functional absorption of intact insulin peptide.
12. Advantages of Nanocochleates:
Table 6. Major Advantages of Nanocochleate Drug Delivery Systems and Their Clinical Implications
|
Advantage |
Mechanistic Basis |
Clinical Implication |
|
Exceptional physicochemical stability |
Anhydrous solid lipid matrix; no aqueous core susceptible to hydrolysis or oxidation |
Long shelf life; ambient temperature storage; suitable for resource-limited settings |
|
Protection from enzymatic degradation |
Multiple lipid bilayer layers physically shield drug from lipases, proteases, nucleases |
Enables oral delivery of proteins, peptides, and nucleic acids |
|
Acid resistance (gastric pH) |
Ca²⁺-PS bonds maintain structural integrity at pH 1.2–2.0 |
Oral delivery without enteric coating required |
|
Enhanced oral bioavailability |
Lymphatic uptake via Peyer's patches; bypass of first-pass metabolism |
Lower effective doses; reduced systemic side effects |
|
Lysosomal bypass |
Cytoplasmic release before lysosomal fusion; avoids phospholipase degradation |
Efficient intracellular drug delivery; gene transfection |
|
Versatile cargo capacity |
Lipid bilayer accommodates hydrophobic, amphiphilic, and nucleic acid cargoes |
Broad applicability across drug classes |
|
Biocompatible and biodegradable |
Natural phospholipids and endogenous Ca²⁺; GRAS-status components |
Favourable safety profile; potential for regulatory approval |
|
Prolonged shelf life |
Solid matrix resistant to aggregation, drug leakage, and lipid peroxidation |
Practical manufacturability and distribution |
13. Limitations and Challenges:
13.1 Manufacturing and Scale-Up
Batch-to-batch reproducibility of nanocochleate size, morphology, and drug loading remains a significant challenge. The kinetics of Ca²⁺-induced bilayer condensation are sensitive to temperature, mixing rate, lipid concentration, and ionic strength, making precise process control essential. [30]
13.2 Hydrophilic Drug Encapsulation
The absence of an aqueous core limits the entrapment efficiency of highly hydrophilic drugs. Modified formulation strategies (drug-lipid complexes, pH-sensitive lipids) only partially address this constraint, and entrapment efficiencies for hydrophilic molecules typically remain below 60%.
13.3 Regulatory and Toxicological Data Gaps
There is currently a paucity of long-term in vivo toxicological data for nanocochleate formulations, particularly regarding the chronic effects of calcium loading from repeated dosing, and the immunogenicity of phosphatidylserine as a lipid component. [31] Regulatory guidance specific to nanocochleate products has not yet been established by the FDA or EMA, creating uncertainty for clinical development programmes.
13.4 In Vitro–In Vivo Correlation (IVIVC)
Standard in vitro drug release models (dialysis membrane, Franz diffusion cell) may not adequately recapitulate the complex ion-exchange environment of the GI tract. This creates challenges in predicting in vivo pharmacokinetics from formulation development data.
13.5 Clinical Translation Gaps
Despite promising preclinical data, very few nanocochleate formulations have advanced beyond Phase I clinical trials. The main barriers include: (i) lack of GMP-compliant large-scale manufacturing processes; (ii) insufficient pharmacokinetic and toxicokinetic data packages; (iii) limited comparative clinical data against existing lipid nanoparticle platforms.
14. Comparative Analysis with Other Drug Delivery Systems:
Table 7: Comparative Evaluation of Nanocochleates and Other Nanocarrier Drug Delivery Systems
|
Feature |
Nanocochleates |
Liposomes |
SLNs |
Niosomes |
Polymeric NPs |
|
Aqueous core |
Absent (solid) |
Present |
Absent |
Present |
Absent |
|
Drug loading (lipophilic) |
High (80–95%) |
Moderate (50–70%) |
High (70–90%) |
Moderate (50–70%) |
Variable |
|
Drug loading (hydrophilic) |
Low (20–60%) |
High (60–90%) |
Low |
Moderate (40–70%) |
High |
|
GI stability |
Excellent |
Poor |
Moderate |
Moderate |
Good |
|
Lysosomal bypass |
Yes |
No |
No |
No |
Partial (pH-responsive) |
|
Storage stability |
Excellent |
Poor–Moderate |
Good |
Good |
Good |
|
Biocompatibility |
High |
High |
Moderate |
Moderate |
Variable |
|
Scale-up feasibility |
Moderate |
High |
High |
Moderate |
High |
|
Clinical stage |
Phase I/II |
FDA-approved |
Phase I/II |
Preclinical |
Phase I/II/III |
|
Cost of manufacture |
Moderate |
High |
Low–Moderate |
Low–Moderate |
Moderate–High |
15. Patents and Regulatory Status:
15.1 Key Patents
BioDelivery Sciences International (BDSI) holds the foundational patent portfolio covering nanocochleate formation methods, lipid compositions, and pharmaceutical applications (US Patents 5,994,318; 6,153,217; 6,592,894). [32] Additional patents from academic institutions cover cochleate-based gene delivery systems, vaccine adjuvant applications, and modified lipid compositions.
15.2 Clinical Development Status
The lead clinical candidate CAMB (cochleate-encapsulated amphotericin B) completed Phase I safety studies demonstrating tolerability in healthy volunteers and patients with invasive fungal infections. Phase II efficacy studies demonstrated activity against Candida and Aspergillus species with reduced nephrotoxicity compared to conventional AmB. Development of CAMB was subsequently deprioritised by BDSI in favour of other pipeline assets, representing a setback for the field.
15.3 Regulatory Pathway
Nanocochleates would be classified as lipid nanoparticle drug products by the FDA and EMA, falling under existing nanomedicine regulatory guidance (FDA Guidance for Industry: Drug Products, Including Biological Products, that Contain Nanomaterials, 2022; EMA Reflection Paper on Nanotechnology-Based Medicinal Products). Comprehensive characterisation packages including physicochemical, toxicological, and immunological data will be required for Investigational New Drug (IND) and Clinical Trial Authorisation (CTA) applications.
16. Recent Advances and Future Directions:
16.1 Surface Functionalization
PEGylation of the nanocochleate surface by incorporation of PEG-phospholipid conjugates (e.g., DSPE-PEG2000) has been shown to extend blood circulation half-life and reduce non-specific protein adsorption (opsonisation) in preclinical models. [33] Ligand-targeted nanocochleates displaying folate, transferrin, or anti-HER2 antibody fragments on their surface have been explored for tumour-targeted delivery, exploiting receptor-mediated endocytosis for enhanced cancer cell specificity.
16.2 Stimuli-Responsive Nanocochleates
Smart nanocochleates that release their cargo in response to specific physiological or pathological triggers represent a frontier in nanocochleate research. pH-responsive formulations using ionisable lipids, redox-sensitive cochleates incorporating disulphide-linked lipids, and thermo-responsive cochleates incorporating lipids with low phase transition temperatures are all under active investigation.
16.3 Combination Therapy
Co-loading of complementary therapeutics within a single nanocochleate formulation enables synchronised delivery of drug combinations with defined molar ratios. [34] This is particularly attractive for oncology (e.g., paclitaxel + curcumin) and HIV therapy (combination antiretroviral agents targeting macrophage reservoirs), where synergistic drug ratios are critical for efficacy.
16.4 AI/ML-Assisted Formulation Optimization
Machine learning algorithms are increasingly being applied to rationalise nanocochleate formulation design by predicting the effects of lipid composition, Ca²⁺ concentration, and preparation conditions on physicochemical outcomes and drug release profiles. High-throughput microfluidic screening combined with AI-driven data analysis promises to dramatically accelerate formulation optimisation timelines.
CONCLUSION
Nanocochleates represent a scientifically compelling and clinically promising drug delivery platform that occupies a unique niche in the lipid nanoparticle landscape. Their defining characteristic the anhydrous, tightly wound multilayer lipid matrix confers a constellation of properties that no other drug delivery system simultaneously possesses: exceptional physicochemical stability, resistance to enzymatic and acid degradation, high entrapment efficiency for lipophilic drugs, lysosomal bypass, and versatility across drug classes ranging from small molecules to nucleic acids.
The landmark CAMB formulation demonstrated that oral delivery of a drug previously restricted to intravenous administration is achievable through nanocochleate technology, with a dramatically improved safety profile. This proof-of-concept, though not yet fully translated to clinical practice, validates the transformative potential of this platform.
Significant challenges remain: manufacturing scale-up, hydrophilic drug encapsulation, regulatory framework establishment, and the generation of comprehensive safety data. However, the convergence of advanced microfluidic manufacturing, AI-assisted formulation design, and surface engineering strategies provides a clear roadmap to address these barriers.
As the pharmaceutical industry confronts an expanding pipeline of poorly soluble drug candidates, RNA therapeutics, and protein biologics, nanocochleates are exceptionally well positioned to offer solutions. The next decade should witness accelerated clinical translation of nanocochleate formulations, particularly in oncology, infectious diseases, and gene therapy, building on the rich preclinical evidence base reviewed herein.
REFERENCES




Priyanka Thakare, Khanderao Jadhav, Rishikesh Bachhav, Sachin Nikam, Nanocochleates: A Novel Lipid-Based Drug Delivery System, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6827-6842. https://doi.org/10.5281/zenodo.20392884
 10.5281/zenodo.20392884
10.5281/zenodo.20392884