
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1College of Pharmaceutical Science Government Medical College, Kannur, Kerala, India
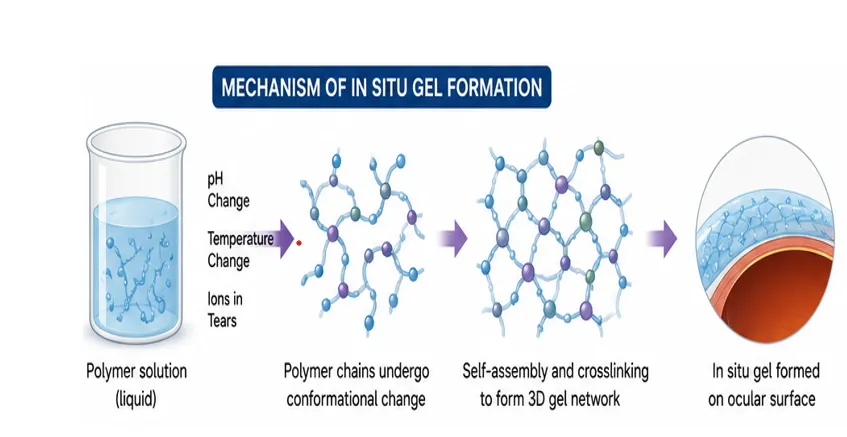
Cataract are a progressive ocular disorder characterized by the clouding of the crystalline lens leading, to impaired vision and are one of the leading causes of blindness worldwide. Surgical removal of the cataractous lens is the most effective treatment; however, non-invasive therapeutic alternatives have been studied because of surgical risks, postoperative complications, high costs, and limited access in resource-constrained settings. Pharmacologic management of cataracts has been extensively researched, but the efficacy of conventional ophthalmic formulations is often compromised by poor ocular bioavailability, rapid tear turnover, nasolacrimal drainage, and low corneal permeability, necessitating frequent administration of the drug. In-situ gel systems have been developed as a promising strategy for ocular drug delivery to enhance the therapeutic efficacy of anti-cataract agents. The formulations are free-flowing solutions prior to administration and undergo sol-gel transition in response to physiological stimuli such as temperature, pH or ionic strength up on administration. The resulting gel prolongs pre-corneal residence time, reduces drug loss, provides sustained drug release and enhances patient compliance. In-situ gels for the prevention and management of cataracts have been extensively studied using a variety of polymers such as poloxamers, chitosan, gellan gum, pectin, carbopol and hydroxypropyl methylcellulose. This review describes the pathophysiology and risk factors of cataract formation and discusses the present treatment strategies and a special focus on in situ gel-based drug delivery systems. Moreover, the review addresses the present challenges and future prospects for the application of in-situ gels as an effective and patient-friendly platform for the enhancing of ocular drug delivery and cataract management.
The human eye is the most important sensory organ that helps in vision and maintains the quality of life. The human eye is generally divided into two major parts: the anterior and posterior segments. The anterior segment consists of the cornea, pupil, iris, ciliary body, anterior chamber, and lens. The anterior part of the eye is filled with aqueous humor by the ciliary body. The posterior segment encompasses the vitreous, choroid, retina, macula and optic nerve. The retinal pigment epithelium is a layer of cells found between the retina and choroid and is vital for the maintenance of the retina. The vitreous is filled with a clear, jelly like fluid called the vitreous humor. Light-sensitive cells in the retina convert light into messages for vision. [1]
According to WHO, 2.2 billion people worldwide have vision impairment [2]. Good sight is so important for maintaining daily life activities, social connections, emotional health, and overall quality of [3]. Therefore, maintaining ocular health is a necessity. Ocular health is the state of eye in which its structural integrity and functions are maintained. Any disturbance in the normal structure and function of the eye results in various ocular disorders. According to WHO, 1 billion people have long-distance vision impairment or blindness, mainly due to ocular disorders such as [4].
Ocular disorders are classified based on the affected anatomical region of the eye. Such as anterior segment disorders and posterior segment disorders. The anterior segment disorders include glaucoma, cataract, blepharitis, anterior uveitis and posterior segment disorders like posterior uveitis, retinitis, age related macular degeneration, diabetic retinopathy etc [5,6].
Cataract
cataracts are cloudy or opaque areas in the lens of the eye, which are normally clear in appearance [7]. This non transparency in lens results in poor vision. About 94 million in world suffer from vision impairment or blindness caused by cataracts [4]. Light enters a healthy eye via the cornea and lens and is focussed to generate a clear, inverted image on the retina. This image is transformed by the retina into electrical signals, which are then transmitted to the brain via the optic nerve and perceived as vision. Protein aggregation and structural alterations cause the normal lens to become hazy in cataracts. Instead of being firmly focused on the retina, light is scattered due to this loss of transparency. As a result, a clean image is not generated, resulting to fuzzy vision, glare, diminished contrast sensitivity, and trouble seeing in dim light. Thus, normal picture development and visual clarity are disrupted by cataracts. This adversely affects the day-to-day activities, socialization within the community, and emotional health of cataract patients. There are different types of cataracts are present, they may be occurred by birth or acquired in life due to age or by some injuries, medicines, diseases, toxic substances, post cataract surgery etc. Cataracts are also classified as nuclear, cortical and posterior subcapsular cataract by its site of formation of opacity in lens. [6,8]
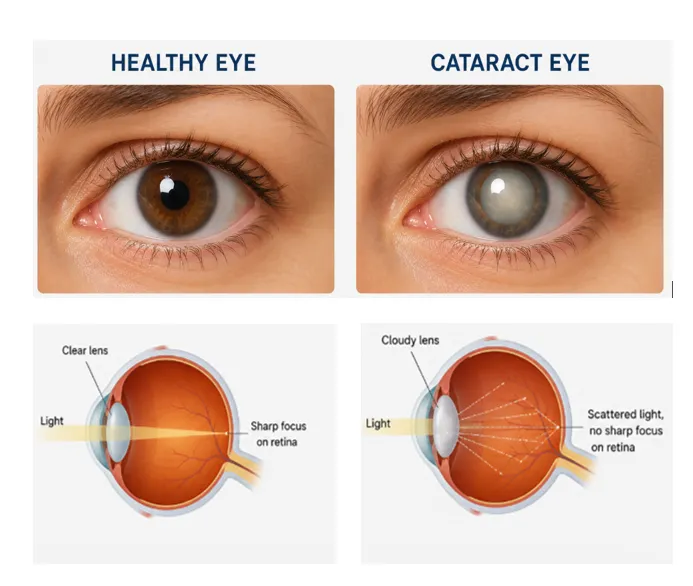
Figure No: 1 Image of Healthy and Cataract Eye
Types
Age - related cataracts: most common when individuals become older.
Congenital or juvenile cataracts: may be due to genetic conditions or congenital disorders.
Secondary cataract: caused by trauma, surgery, other ocular disorders, prolonged use of some medications, radiation exposure and, some metabolic disorders.
Structural cataract: based on the site of opacification formed in the ocular lens, cataracts are mainly of three types:
Symptoms: vision loss, photophobia, myopia shift, changes in vision colour (5).
Risk factors: UV light exposure, genetics, poor nutrition, smoking, metabolic disorders like diabetes. (9)
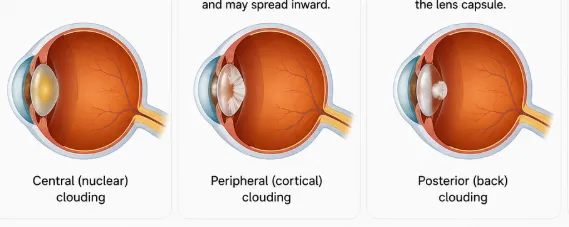
Figure No: 2 Type of Structural Cataract Eyes
The ocular lens
The lens is a biconvex transparent structure of ectodermal origin. From lateral to medial, the lens is divided into lens zonule, capsule, epithelium, and fibers. [10].
The lens capsules were made of type 4 collagen and laminin network resulting in a thin and transparent layer.
The epithelial cell layer has central, intermediate and germinative zones.
Finally, the 3D structure of the nucleus and cortex of the lens was formed.
Lens zonules are made of cysteine they retard by age and have main role accommodation of the [11]
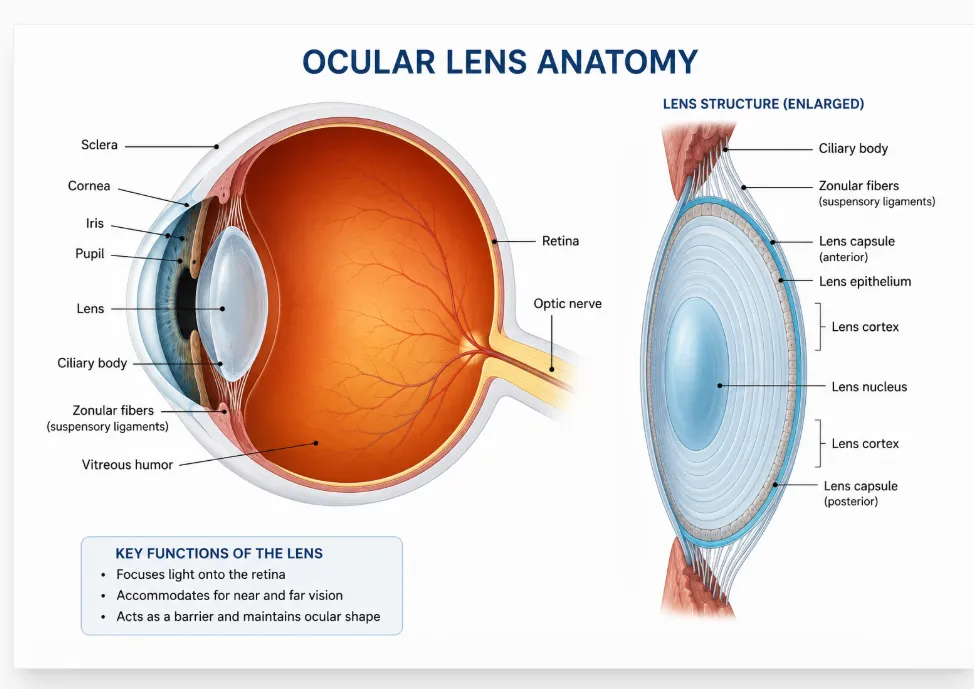
Figure No: 2: Image of Ocular Lens
Mechanism of formation of cataract
Crystallin proteins preserve the lens's transparency. The early onset of cataracts is significantly influenced by structural or genetic changes in α-, β-, and γ-crystallins. Glycation, oxidative stress, and exposure to lipophilic materials are important mechanisms that can result in elevated calcium levels in the lens and crystallin protein aggregation. A significant part of this process is oxidative stress, which is frequently caused by hyperglycaemia and reactive species such as hydroxyl radicals. The formation of oxidative stress in the lens is due to the defective defense of the antioxidant systems in the ocular lens epithelium. They have antioxidant enzymes such as superoxide dismutase, catalase, and GPx and non-enzymes like GSH vitamin E and vitamin C. They help to scavenge the reactive oxygen species formed during the extensive lens epithelial cells metabolism, increased glucose level, UV light etc. the increased glucose level promotes the aldose reductase to aggregates the ocular lens proteins and reduce their solubility and to the opacity. [11,12]
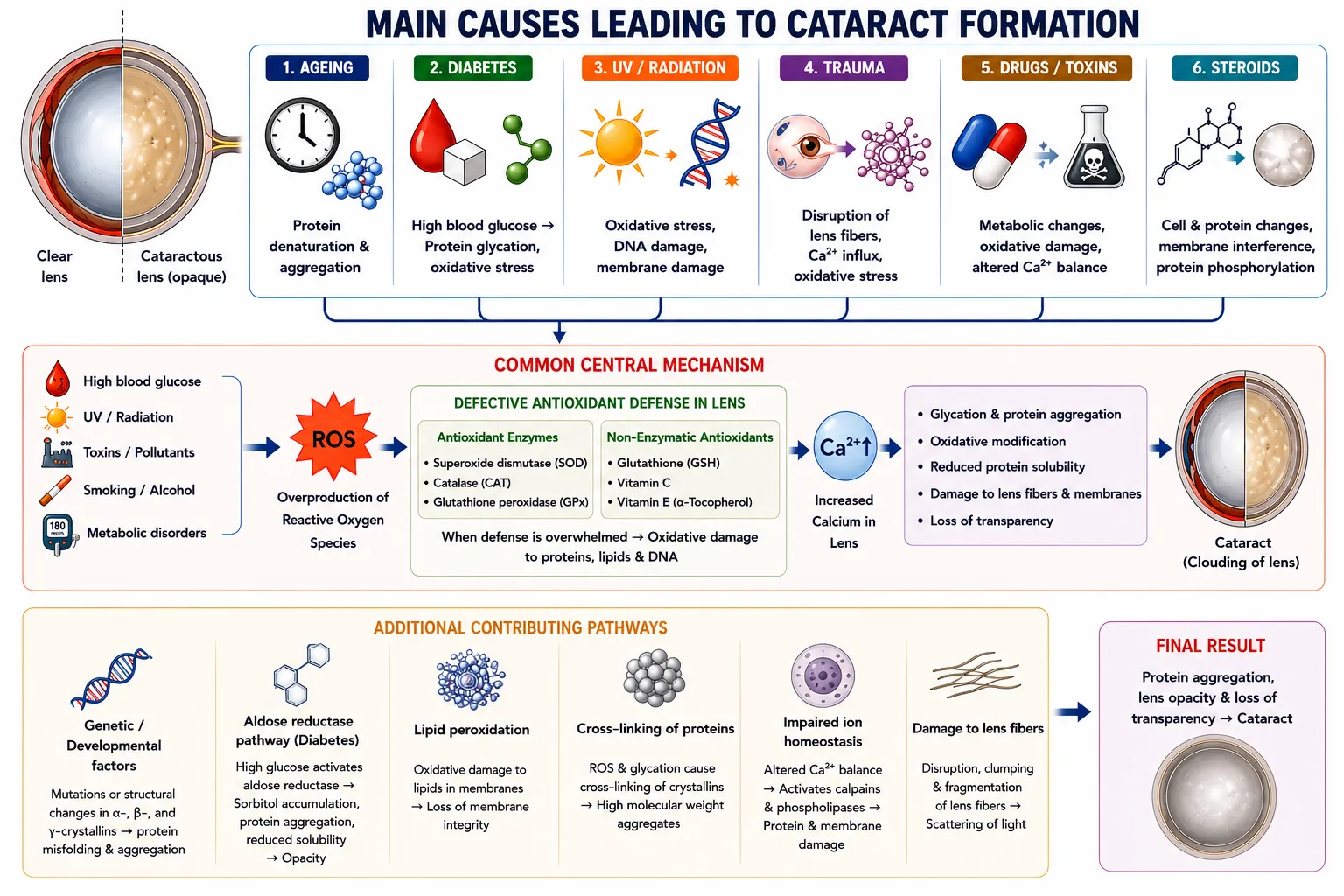
Figure No 3: Image of formation of cataract
Ocular dosage forms
These are sterile pharmaceutical preparations intended to deliver drugs to the eye to diagnose, prevent, alleviate, or treat ocular diseases and conditions.
Liquid dosage forms
Eye drops: These are isotonic and sterile water or oil solutions, suspensions, or emulsions containing therapeutic. Ophthalmic solutions are sterile aqueous preparations used for cleansing eye balls. Ophthalmic microemulsions are inexpensive, easy to prepare, and stable ocular dosage forms. It is suitable for large drug loading to achieve prolonged effectiveness and increased bioavailability. [13,14]
Solid dosage forms
Contact lenses coated with drug: poly-2- hydroxy methacrylate or silicone-based contact lenses in which the drug was absorbed onto their surfaces. Drugs such as timolol, ciprofloxacin, and dexamethasone are used.
Ocular inserts: Solid or semisolid inserts, either insoluble, soluble, or biodegradable ocular dosage forms provides prolonged residence in the conjunctival sac. It provides slow controlled drug release thus reduces systemic side effects, reduces number of doses, and not interrupts the vision. Examples like pilocarpine ocusert.
Minidiscs: These are contact lens like solid dosage forms of 4 -5mm in diameter made from polymeric units of α-ω-bis(4-methacryloxy)-butyl poly(dimethylsiloxane) and poly(hydroxyethyl methacrylate) help deliver both lipophilic and hydrophilic drugs. Gentamicin, and moxifloxacin-like antibiotics were delivery through minidiscs.
Semi solid dosage forms
In-situ gels are liquid formulation that undergo a sol - to - gel transition by external triggered by external such as pH, temperature and ionic structure at the site of application, to providing extended corneal residence and improved bioavailability. Nepafenac in situ gel for postoperative pain [15] dorzolamide hydrochloride nano emulsion in-situ gel for glaucoma [16] and ganciclovir in-situ gel for CMV retinitis [17].
Ophthalmic ointments: made up of hydrocarbons which melts in the body temperature. It forms small drops and prolong the ocular residence in topical use, but it interferes the sight so only can be used at night. Cyclosporin ophthalmic ointment [18].
Advantages of ocular drug delivery systems
Challenges in ocular drug delivery
The major challenges face in ophthalmic drug administration mainly because of the anatomical features of the eye. Barriers in ocular drug delivery includes precorneal barrier, such as cul-de-sac is the lower pit in the lower eyelids with a maximum capacity of 30µL. The movement of lower eyelids reduces its capacity to 80%. Thus, reduces concentration of drugs and also decreases the therapeutic effectiveness. Then the lacrimal drainage, loss of drug by lacrimation, solution drainage, less absorption in conjunctiva, drug metabolism and protein binding also disrupt drug absorption.
The next barrier, Corneal barrier, the cornea provides protection to different chemical and mechanical injuries by its three different layers. First the epithelium layer of 5-7 layers of firmly attached cells act as a barrier for hydrophilic drugs and large molecules. Next is water based compact layer stroma, acts as a barrier for lipophilic drugs. The last endothelium, which has selective access for hydrophilic and macromolecule drugs into the aqueous humor. Generally, drug molecular weight, charge, degree of ionization, and hydrophobicity influence the corneal permeation. Hence, the trans-corneal permeation is known as rate limiting step for drug transfer from the lachrymal fluid into the aqueous humor. About 2.5µL/min of aqueous humor are formed and is replaced in every 100 minutes. So, it increases the dosing frequency to achieve the desired therapeutic effect.
Another barrier was blood ocular barrier, they prevent the entry of foreign substances into the blood stream. The blood ocular barriers are classified into blood-aqueous barrier (BAB) and blood retinal barrier (BRB). Among these is the anterior eye’s blood-aqueous barrier, which limits intraocular access but permits lipophilic, tiny medicines and eliminates at a faster rate than hydrophilic, large ones. The retinal endothelium and pigment epithelial cells make up the blood retinal barrier in the posterior eye, which keeps plasma, water and hazardous substances out of the retina.[20]
The conventional ophthalmic dosage forms provide a 5-10% of bioavailability. To increase it various strategies such as viscosity enhancement, prodrugs, penetration enhancers, in situ gels, novel drug delivery systems, intravitreal and other periocular routes of delivery. [21]
Management of cataract
Cataract is treated mainly by ocular surgeries and there were no approved drugs to cure them. Even though there are many discoveries are emerged in the scientific communities. The use of many different nutraceuticals, new and repurposing of existing drugs, non-surgical methods and surgical methods to delay or prevent the progression of the cataract genesis. [22]
Types:
Many phytochemicals present in plants have anti-inflammatory, antioxidant, anti-protein aggregation, aldose reductase inhibition which make them the potential reason to use as an anticataract agent.
Eg: curcumin, quercetin, tea extract, hesperetin, eugenol.[22]
Local or systemic administration of new or existing drugs helps to delay or prevent cataract. This is possible because of their potential to alter metabolic pathways, reduce glucose levels and glutathione depletion, protein glycation, scavenging reactive oxygen species, maintains calcium level in lens epithelial cells, to promote glucose renal uptake, down regulation of aldose reductase enzymes etc.
Eg: aspirin, ibuprofen, disulfiram, acetyl-L- carnitine, [23–25]
These are only reliable treatment option to cure cataract to improve the quality of life of cataract patients. In which the cloudy natural lens is replaced by synthetic monofocal or multifocal intra ocular lens to restore or to improve sight.
The types of cataract surgeries are;
Because of complexity and high cost of cataract surgeries, it limits treatment to all people in the society and affects their quality of life. So, discovery of new alternative non-surgical methods is more important to decrease the financial burden of surgical methods. They include the lipid nanocarriers, polymeric nanoparticles, inorganic nanoparticles, micelles, hydrogels, inserts and lipid cyclodextrin based nanoparticle systems. These strategies help to encapsulates, increase ocular bioavailability and provide sustained or controlled drug release of the therapeutic agent. They also help to protect the dugs instability such as photooxidation, temperature sensitivity and antioxidation potential. [21]
Eg: solid lipid nanoparticles of N-acetyl carnosine and baicalin, PEG-PLGA coated cerium oxide nanoparticles, lutein-PLGA nanoparticle loaded in situ gel, lanosterol nanoparticle intravitreal injection, nifedipine loaded PLGA nano micelles, chitosan coated baicalin-PLGA nanoparticle. [27–29]
Limitations of cataract treatment
Since surgery where the main treatment option includes demerits such as:
In-situ gel systems for cataract management
In-situ gels are pharmaceutical dosage forms present in the polymeric solutions that changes from its liquid state into a gel state upon the triggering factors such as pH, temperature and ions present in the applied site of action. There three different types of in situ gels are there, pH sensitive, temperature sensitive and ion sensitive in-situ gels.
The in-situ gel upsides drug delivery by increasing residence time, increase in bioavailability, provide sustained drug release, improve patient compliance, reduce the doses, suitable for hydrophilic or lipophilic drugs and easy to administer. The downside is that optimization of concentration of polymer that gellates at the required physiological condition, high drug loading and sterilization of the in-situ gel sometimes changes the properties of gelling characteristics, instability on storage etc. [26]
Even though there are many studies are performed by in-situ gels by selecting suitable polymer with in-situ gelling properties such as poloxamers, gellan gum, and Carbopol. Due to the prolonged retention, sustained drug delivery, higher bioavailability in-situ gels are used to treat ocular conditions. This strategy helps to overcome the ocular barriers and ocular pharmacokinetics to produce effective topical ocular drug delivery. So, in-situ gels are able to deliver the anticataract agents to reduce or delay the opacity of the ocular lens by reducing the frequency and extends the corneal retention to reach the lens.
release from ocular in-situ gel
The nature of gelation trigger and polymers used in the formulation influences the release of drugs from ocular in-situ gels. Drug release in thermosensitive gels, e.g., based on poloxamers, is mainly caused by diffusion and polymer swelling. The formulation in liquid form is converted into a gel matrix when it comes into contact with the ocular temperature, releasing the medication in a slow and continuous manner. pH sensitive gels are often formulated with polymers such as Carbopol and HPMC and gel due to the pH of the tear fluid. The release of drug from these systems is mainly controlled by diffusion process through the wet matrix and swelling of the polymer network. Ion-activated gels contain polymers, e.g., gellan gum, sodium alginate and pectin, that interact with the cations in the tear fluid to form crosslinked gel structures, thereby enabling a controlled medication transport within the gel network.[30] In-situ gels loaded with nanoparticles exhibit dual release mechanism for regulated and sustained drug delivery. The drug is first released from the nanoparticles and then it diffuses into the surrounding gel matrix. In biodegradable hydrogels, especially those for intraocular and implantable applications, drug release is a combination of diffusion and slow polymer erosion or breakdown, providing sustained release over days or weeks. Generally, the ocular in-situ gels exhibit a combination of erosion, swelling and diffusion mechanisms which are sometimes termed as non-Fickian or anomalous transport behaviour. [21,22]
Examples of in-situ gels studied in cataract
So, few examples of in-situ gels used in cataract are Kaempferol ophthalmic gel of pectin and HPMC K4M as a pH-sensitive gelling system to prolong ocular residence time and provide controlled drug release, thereby reducing dosing frequency and enhancing therapeutic effect. The gel developed with HPMC K4M, pectin, Carbopol, and Tween 80 with 1% of drug. The finished formulation was assured good drug [31] Boerhaavia diffusa root extract added ophthalmic in-situ gel prepared by using HPMC and gelatine showed delay in cataract [32].
Esmolol hydrochloride were repurposing in cataract by developing a temperature-sensitive in-situ gel. The gel was formulated using thermosensitive polymer Poloxamer 407, Poloxamer 188 and gellan gum, together with HPMC [33] An ion-activated in-situ gel of estradiol drop using gellan gum, polysorbate-80, mannitol, and potassium sorbate and EDTA to prevent age-related cataracts. The solution transformed into a gel upon contact with simulated tear fluid, confirmed by viscoelastic measurements, and released 80% of estradiol over 8 hours via a non-Fickian mechanism. The formulation was clear, isotonic, pH-suitable, and stable for 6 months under ICH conditions and showed to delay the progression of cataract [34].
The lanosterol nanoparticle in-situ gel eye drops for cataract in rat cataracts model. The formulation by bead milling containing 0.5% lanosterol, 5% 2-hydroxypropyl-β-cyclodextrin, 0.5% methylcellulose, 0.005% benzalkonium chloride, and 0.5% mannitol, yielding 60–250 nm nanoparticles that gelled at 37°C. The nanoparticles entered the cornea via energy-dependent endocytosis and reached the intraocular side. Twice-daily instillation of attenuated age-related space and structure collapse in the lens. It reduced cataract-related factors the lowered nitric oxide, calpain activity, lipid peroxidation, Ca²⁺ content; increased Ca²⁺-ATPase activity and delayed opacification onset. [28]
A thermosensitive intracameral hydrogel system based on F127/F68 and mPEG-PLA developed to deliver dexamethasone, moxifloxacin, and genistein-loaded nanostructured lipid carriers for post-cataract surgery management. Genistein-loaded NLCs of about 39 nm loaded gel matrix at 32 °C within 20 seconds transform to gel and maintained high transparency above 90%. The system provided programmed drug release, where moxifloxacin was completely released within 10 days, dexamethasone showed sustained release up to 30 days, and genistein demonstrated prolonged release up to 40 days. In vitro studies confirmed inhibition of proliferation, migration, and epithelial-mesenchymal transition of lens epithelial cells, indicating potential for reducing postoperative inflammation, infection, and posterior capsular opacification while minimizing dependence on postoperative eye [35]
Thermosensitive dual drug delivery system composed of chitosan/gelatin hydrogel containing prednisolone acetate and levofloxacin-loaded nanoparticles was developed for the prevention of post-operative endophthalmitis after cataract surgery. The nanoparticles of ~155 nm, uniform distribution, and a negative surface charge. The formulation gelled rapidly at 34 °c within 63 seconds and showed physiological osmolarity. Sustained drug release was maintained for up to 7 days. In vitro studies demonstrated reduced inflammation and cell death in tnf-α-induced corneal epithelial cells by lowering inflammatory markers such as tnf-α, il-6, mmp-3, and mmp-9. An, ex vivo rabbit studies confirmed both antibacterial and anti-inflammatory effects against staphylococcus aureus keratitis, indicating its potential as an effective postoperative ocular delivery system. [36]
The disulfiram solid dispersion incorporated into a thermosensitive in-situ gel containing poloxamer 407 and poloxamer 188. Both in vitro and in vivo studies demonstrated prolonged ocular residence time and improved corneal penetration of DSF. Pharmacodynamic evaluation further showed that the formulation delayed the progression of selenium-induced cataract, suggesting its potential as an effective ocular drug delivery system for cataract management. [23]
A multifunctional thermosensitive injectable intraocular lens (IOL) hydrogel was developed to improve visual outcomes and reduce postoperative complications following cataract surgery. The Poloxamer-based hybrid hydrogel incorporated antibacterial, anti-inflammatory, and photothermal components, including black phosphorus nanosheets, tannic acid, and silver nanoparticles. The IOL exhibited high transparency, suitable refractive index, and stability without leakage, closely mimicking the natural lens. In vitro and in vivo studies resulted significant antibacterial and anti-inflammatory activity, highlighting its potential as a multifunctional and adjustable next-generation intraocular lens system. [37]
These studies demonstrate that in-situ gel systems are promising platforms for cataract management due to their ability to increase precorneal retention, improve drug penetration, and provide sustained drug release. pH-sensitive, ion-activated, and thermosensitive gels successfully delivered both natural and synthetic anticataract agents, resulting in delayed cataract progression. The incorporation of nanoparticles and lipid carriers further enhanced ocular bioavailability and therapeutic performance, prolonged anti-inflammatory and antimicrobial effects while reducing postoperative complications. Recent innovations have extended beyond drug delivery to multifunctional injectable intraocular lens hydrogels with therapeutic and optical functions. Among the various approaches, thermosensitive nanoparticle-loaded hydrogels offer the greatest advantages owing to their enhanced corneal penetration, prolonged drug release, and improved therapeutic outcomes.
Future Prospects of In Situ Gels for Cataract Treatment
Cataract surgery is the gold standard, but in situ gel systems have become a promising non-invasive platform for both cataract prevention and post-operative management. These long-acting and patient-friendly ocular dosage forms are delivered as liquids and undergo sol-to-gel transition in response to physiological stimuli, thereby increasing precorneal residence time, ocular bioavailability, and reducing dosing frequency compared to conventional eye drops. Their future potential lies in the delivery of antioxidants, anti-fibrotic agents and other therapeutic compounds to delay cataract progression and prevent postoperative complications such as posterior capsular opacification. Moreover, the incorporation of nanocarriers with in situ gel systems is expected to improve drug solubility, corneal penetration and sustained release. However, challenges such as formulation stability, sterilization, patient comfort, large-scale manufacturing and the need for strong pre-clinical and clinical evidence need to be overcome before widespread clinical use.
CONCLUSION
Cataract is the largest cause of reversible blindness globally, and although surgery is the current gold standard for therapy, there is considerable interest in exploring non-invasive therapeutic techniques to prevent disease progression and improve postoperative results. Because ocular in situ gel systems can undergo a sol-to-gel transition after administration, increasing ocular bioavailability, extending precorneal residence duration, and offering sustained drug release, they have become a viable drug delivery platform. These systems have proven tremendous potential for administering a wide range of therapeutic agents, including antioxidants, natural phytochemicals, corticosteroids, antibiotics, and nanoparticle-based formulations, for both cataract prevention and post-cataract surgery care. Moreover, advances in nanotechnology and multifunctional hydrogel systems have extended the therapeutic potential of in situ gels by improving drug penetration, controlled release and patient compliance. The positive preclinical results notwithstanding, challenges persist in formulation stability, sterilization, upscaling, and clinical validation. More research and well-planned clinical trials are required to convert these promising systems into safe, efficient and financially feasible ophthalmic therapeutics for cataract management
REFERENCES


Theertha P. K.*1, Aswathi P. P., Adithya K. P., Ocular In-Situ Gel Systems for Cataract Management: Emerging Therapeutic Approaches, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 1764-1777. https://doi.org/10.5281/zenodo.21265724
 10.5281/zenodo.21265724
10.5281/zenodo.21265724