We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
2,4,5 General Physician, Corporación Universitaria Rafael Nuñez, Cartagena Colombia
1General Physician, Universitaria del Sinu, Cartagena, Colombia
3General Physician, Universitaria del Norte, Barranquilla, Colombia.
Pediatric malnutrition remains a major global health challenge, significantly impacting morbidity, mortality, and long-term developmental outcomes. Recent conceptual advances emphasize a phenotypic–etiologic framework, integrating anthropometric deficits with underlying pathophysiological mechanisms. This approach enhances diagnostic precision and guides individualized treatment strategies. Phenotypic criteria include wasting, stunting, underweight, and altered body composition, while etiologic classification differentiates between disease-related and non-disease-related malnutrition, with or without inflammation. This review synthesizes current evidence on diagnostic criteria, clinical assessment, and therapeutic strategies, including nutritional rehabilitation, management of complications, and multidisciplinary care. The integration of standardized anthropometric indicators (z-scores, MUAC) with etiologic evaluation improves clinical outcomes and supports targeted interventions. A comprehensive, structured approach is essential for effective management across diverse clinical settings
Pediatric malnutrition constitutes a critical global health problem and remains one of the leading contributors to morbidity and mortality among children under five years of age. It is defined as a state resulting from an imbalance between nutrient
intake and physiological requirements, which leads to alterations in body composition, impaired physical and cognitive development, and decreased functional capacity. This condition encompasses a wide clinical spectrum, ranging from acute forms such as wasting to chronic manifestations such as stunting, as well as micronutrient deficiencies that often coexist and exacerbate outcomes (1, 2).
Traditionally, the diagnosis and classification of pediatric malnutrition have relied heavily on anthropometric indicators, including weight-for-height, height-for-age, and weight-for-age indices expressed as z-scores based on World Health Organization (WHO) growth standards. While these measures provide a standardized and reproducible method for identifying nutritional deficits, they are inherently limited in their ability to capture the underlying pathophysiological mechanisms responsible for malnutrition. Consequently, children with similar anthropometric profiles may present with markedly different clinical conditions, prognoses, and responses to treatment (3, 4).
In recent years, there has been a paradigm shift toward a more comprehensive diagnostic framework that integrates both phenotypic and etiologic components. The phenotypic dimension focuses on measurable clinical manifestations such as wasting, stunting, underweight, and alterations in body composition. In contrast, the etiologic dimension seeks to identify the underlying causes of malnutrition, distinguishing between non-disease-related factors such as inadequate dietary intake or food insecurity and disease-related conditions, which may occur with or without systemic inflammation. This distinction is particularly relevant in clinical practice, as inflammatory processes profoundly influence metabolic responses, nutrient utilization, and the effectiveness of nutritional interventions (5).
The adoption of a phenotypic–etiologic approach allows for a more precise and clinically meaningful classification of pediatric malnutrition. It facilitates individualized management strategies by aligning therapeutic interventions not only with the severity of anthropometric deficits but also with the underlying pathogenesis. For instance, children with malnutrition secondary to chronic illness or acute inflammatory states may require integrated medical and nutritional management, whereas those affected by socioeconomic deprivation may benefit primarily from community-based nutritional support and preventive interventions (6, 7).
Furthermore, pediatric malnutrition has significant long-term implications that extend beyond immediate clinical outcomes. Early-life nutritional deficits are strongly associated with impaired neurodevelopment, reduced educational attainment, and increased risk of chronic diseases in adulthood. These consequences highlight the importance of early detection, accurate diagnosis, and timely intervention, as well as the need for coordinated efforts across clinical, public health, and policy domains (8, 9).
In this context, the present article aims to provide a comprehensive review of pediatric malnutrition through the lens of the phenotypic–etiologic framework, emphasizing its diagnostic utility, clinical relevance, and implications for integrated management.
Pediatric malnutrition must be understood as a dynamic and multifactorial clinical condition in which anthropometric deficits represent only the external manifestation of deeper metabolic, inflammatory, and environmental disturbances. The modern phenotypic–etiologic framework allows clinicians to integrate objective measurements with underlying pathophysiological mechanisms, thereby improving diagnostic precision and therapeutic decision-making (10).
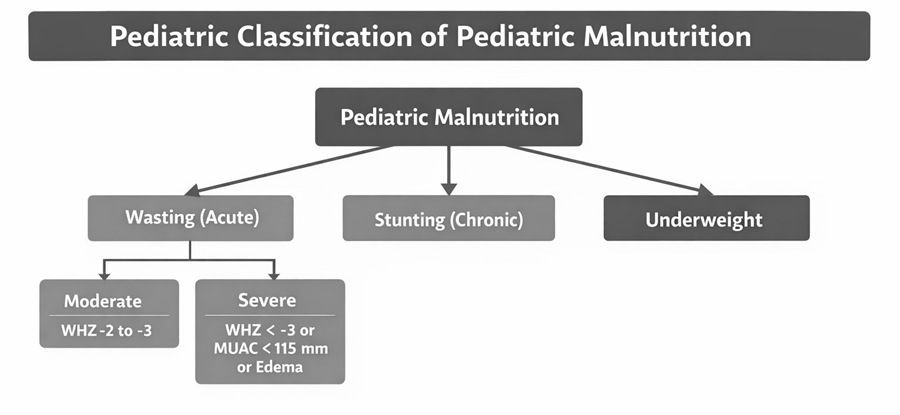
From a phenotypic perspective, malnutrition is primarily identified through standardized anthropometric indicators based on World Health Organization (WHO) growth references. These include weight-for-height (WHZ), height-for-age (HAZ), and weight-for-age (WAZ) z-scores. Wasting (WHZ < −2 SD) reflects acute malnutrition and is associated with recent weight loss or failure to gain weight, often in the context of infection or inadequate intake. Severe acute malnutrition (SAM), defined as WHZ < −3 SD, mid-upper arm circumference (MUAC) < 115 mm, or the presence of bilateral pitting edema, is associated with a markedly increased risk of mortality and requires urgent medical intervention (11, 12).
Stunting (HAZ < −2 SD) represents chronic malnutrition and reflects prolonged nutritional deprivation, frequently beginning during fetal life and continuing through early childhood. It is strongly associated with adverse neurodevelopmental outcomes, impaired immune function, and long-term socioeconomic consequences. Underweight (WAZ < −2 SD) is a composite indicator that may reflect elements of both acute and chronic malnutrition but lacks specificity when used in isolation (13).
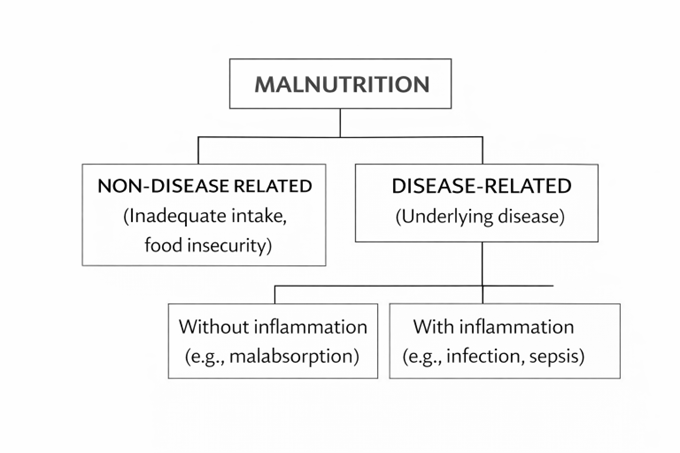
However, exclusive reliance on phenotypic indicators is insufficient to fully characterize pediatric malnutrition. The etiologic dimension introduces a critical layer of understanding by identifying the underlying causes that drive nutritional deficits. This dimension distinguishes between non-disease-related malnutrition and disease-related malnutrition, which may occur with or without inflammation (14, 15).
Non-disease-related malnutrition typically arises from inadequate dietary intake, poor feeding practices, food insecurity, or adverse socioeconomic conditions. In contrast, disease-related malnutrition is associated with underlying pathological conditions such as chronic infections, congenital anomalies, malignancies, gastrointestinal disorders, or neurological impairment. Within this category, the presence or absence of systemic inflammation is of particular clinical importance. Inflammatory processes, mediated by cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor-alpha, induce a hypermetabolic state characterized by increased energy expenditure, proteolysis, anorexia, and impaired nutrient utilization (16, 17).
The integration of phenotypic and etiologic components results in a more comprehensive diagnostic framework. This combined approach allows clinicians to stratify patients more accurately and tailor interventions accordingly. For example, a child presenting with severe wasting in the context of acute infection represents disease-related malnutrition with inflammation, requiring both nutritional rehabilitation and aggressive treatment of the underlying condition. Conversely, a child with isolated stunting in a context of chronic poverty represents non-disease-related malnutrition, where long-term nutritional and social interventions are essential (18, 19)
Clinical assessment must therefore be multidimensional and systematic. Anthropometric evaluation should include serial measurements to assess growth velocity, which is often a more sensitive indicator than single-point measurements. Dietary assessment should evaluate caloric intake, feeding frequency, dietary diversity, and caregiver practices. A thorough medical history is essential to identify underlying diseases, recurrent infections, or conditions affecting nutrient absorption and metabolism (20, 21)
Physical examination provides additional diagnostic clues. The presence of bilateral pitting edema is characteristic of kwashiorkor, while severe muscle wasting and loss of subcutaneous fat are typical of marasmus. Other findings may include skin lesions, hair depigmentation, hepatomegaly, and signs of micronutrient deficiencies such as angular stomatitis or conjunctival pallor (22)
Laboratory evaluation, although supportive, has limitations. Serum proteins such as albumin and prealbumin are influenced by inflammatory states and do not reliably reflect nutritional status in isolation. Inflammatory markers (e.g., C-reactive protein) may help contextualize laboratory findings and differentiate between inflammatory and non-inflammatory states. Micronutrient assessments may be indicated in specific clinical scenarios (23).
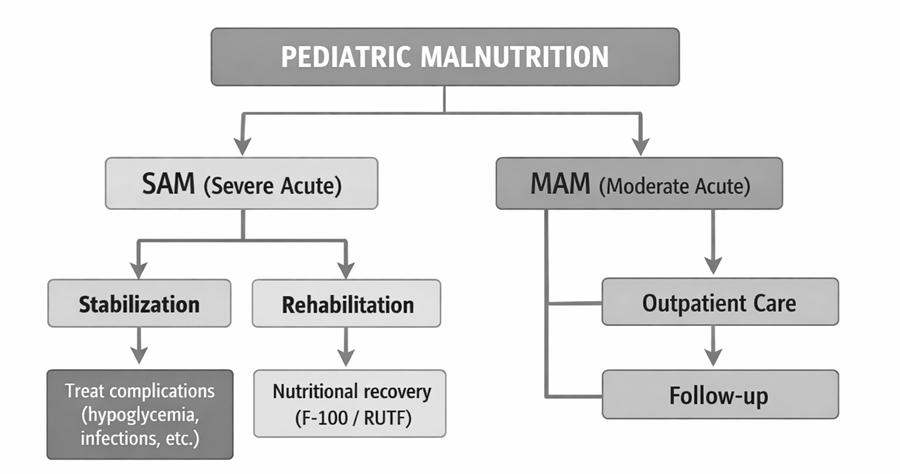
Management strategies are determined by both the severity and etiology of malnutrition. Severe acute malnutrition requires a structured, phased approach consisting of stabilization, transition, and rehabilitation phases. During the stabilization phase, the primary objective is to address life-threatening complications, including hypoglycemia, hypothermia, dehydration, electrolyte imbalance, and infection. Nutritional support is initiated cautiously using low-energy, low-protein therapeutic formulas (e.g., F-75). Once the patient is stabilized, the rehabilitation phase focuses on rapid weight gain using higher-energy formulations such as F-100 or ready-to-use therapeutic foods (RUTF) (23).
Moderate acute malnutrition is generally managed in outpatient settings with supplementary feeding programs, including lipid-based nutrient supplements or fortified blended foods, along with regular monitoring of growth and clinical status (24).
In cases of disease-related malnutrition, management must prioritize treatment of the underlying condition. Nutritional support should preferentially be delivered via the enteral route, as it maintains gut integrity and reduces the risk of complications. Parenteral nutrition is reserved for cases where enteral feeding is contraindicated or insufficient. A multidisciplinary approach involving pediatricians, nutritionists, nurses, and social workers is essential to ensure comprehensive care and long-term recovery (25).
Pediatric malnutrition represents a multifactorial and dynamic clinical condition that cannot be adequately addressed through a purely anthropometric framework. The integration of a phenotypic–etiologic diagnostic model provides a more robust and clinically meaningful approach, allowing clinicians to differentiate between children with similar nutritional deficits but distinct underlying mechanisms. This distinction is particularly relevant in pediatric practice, where the interplay between growth, development, infection, and environmental factors is highly complex (26).
One of the key advantages of this model is its ability to incorporate the role of systemic inflammation as a central determinant of metabolic response. In disease-related malnutrition with inflammation such as in sepsis, chronic infections, or critical illness there is a hypercatabolic state characterized by increased energy expenditure, proteolysis, and altered nutrient utilization. In these cases, nutritional interventions alone are insufficient unless the underlying inflammatory process is simultaneously addressed. This has important implications for clinical decision-making, particularly in hospitalized or critically ill pediatric patients, where delayed recognition of inflammation-driven malnutrition may lead to suboptimal outcomes (27).
Conversely, in non-disease-related malnutrition, the absence of inflammation allows for a more predictable and favorable response to nutritional rehabilitation. These patients, often affected by food insecurity or inadequate dietary intake, benefit significantly from standardized interventions such as ready-to-use therapeutic foods (RUTF) and community-based management programs. However, even within this group, social determinants of health including poverty, caregiver education, and access to healthcare play a critical role in both the development and resolution of malnutrition. Therefore, effective management requires not only clinical treatment but also multisectoral interventions (28).
Another important consideration is the limitation of traditional anthropometric indicators in identifying early or subclinical malnutrition. For example, children with chronic disease may maintain near-normal weight-for-height indices despite significant losses in lean body mass. This highlights the need for complementary assessment tools, such as mid-upper arm circumference (MUAC), body composition analysis, and biochemical markers, to improve diagnostic accuracy (28).
From a therapeutic perspective, the clinical management of pediatric malnutrition must be stage-specific and individualized. In severe acute malnutrition (SAM), especially in the presence of complications, the initial stabilization phase prioritizes the correction of life-threatening conditions such as hypoglycemia, hypothermia, electrolyte imbalance, and infections. This is followed by a rehabilitation phase focused on catch-up growth and nutritional recovery. In contrast, moderate acute malnutrition (MAM) is typically managed in outpatient settings, emphasizing dietary supplementation and close follow-up (29).
Despite advances in diagnostic frameworks and therapeutic strategies, several challenges persist. These include variability in the implementation of guidelines across different healthcare settings, limited access to specialized nutritional products in low-resource environments, and gaps in training among healthcare professionals. Additionally, there is a need for further research to validate and refine the phenotypic–etiologic model in diverse pediatric populations, particularly in low- and middle-income countries where the burden of malnutrition is highest (30).
Ultimately, the integration of clinical, nutritional, and social perspectives is essential to improving outcomes in pediatric malnutrition. A shift toward precision nutrition in pediatrics, guided by both phenotypic presentation and etiologic factors, represents a promising direction for future practice and research.
Pediatric malnutrition remains a significant global health challenge with profound short- and long-term consequences on child survival, growth, and development. The traditional reliance on anthropometric criteria alone is insufficient to capture the complexity of this condition. The adoption of a phenotypic–etiologic diagnostic approach represents a critical advancement, enabling a more comprehensive understanding of the underlying mechanisms and facilitating targeted, individualized interventions.
By distinguishing between non-disease-related and disease-related malnutrition, as well as recognizing the role of inflammation, clinicians can optimize therapeutic strategies and improve clinical outcomes. This approach is particularly relevant in settings with a high burden of infectious and chronic diseases, where malnutrition often coexists with systemic inflammatory states.
Effective management of pediatric malnutrition requires a multidimensional strategy that integrates early diagnosis, appropriate nutritional therapy, treatment of underlying conditions, and addressing social determinants of health. Community-based programs, hospital protocols, and public health policies must be aligned to ensure continuity of care and maximize recovery.
In conclusion, advancing the care of children with malnutrition demands not only improved clinical frameworks but also strengthened health systems, interdisciplinary collaboration, and sustained public health efforts. Future research should focus on refining diagnostic criteria, exploring novel biomarkers, and evaluating the long-term impact of integrated management strategies to further enhance the quality of pediatric nutritional care.
REFERENCES

Andrés Felipe Altahona Acosta, Alex David Blanco Castiblanco, Dayanis Reyes Castellanos, Aura María Amor Escudero, Andrea juliana Rodríguez jalkh, Pediatric Malnutrition: Phenotypic–Etiologic Diagnostic Approach and Comprehensive Clinical Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 716-723, https://doi.org/10.5281/zenodo.21157028
 10.5281/zenodo.21157028
10.5281/zenodo.21157028