
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1. Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune 413114, Maharashtra, India.
2. Guide, Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune 413114, Maharashtra, India.
3. Principal, Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune 413114, Maharashtra, India
Hypertension is one of the most common health problems worldwide and is a major risk Background: One of the main causes of acute hepatic damage is paracetamol overdose, which raises serious health concerns about drug-induced liver impairment. Because of their cytoprotective and antioxidant qualities, herbal remedies have drawn a lot of interest as possible hepatoprotective agents. Objective: The current study sought to assess a herbal extract's hepatoprotective potential against liver damage caused by paracetamol in rats. Methods: Paracetamol (2 g/kg, p.o.) was used to cause hepatotoxicity in Wistar rats. The animals were split into groups for conventional therapy, toxic control, normal control, and herbal extract treatment. For a predetermined length of time, the herbal extract was taken orally at predetermined dosages. Serum biochemical indicators such as total bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP) were measured in order to evaluate hepatic function. To assess structural alterations, histopathological analysis of liver samples was carried out. Results: Hepatic damage was indicated by the substantial elevation in serum ALT, AST, ALP, and bilirubin levels following paracetamol treatment. When compared to the harmful control group, the herbal extract treatment considerably decreased these metabolic markers (p < 0.05). In rats treated with extract, histopathological examinations showed a significant return to normal liver architecture, decreased necrosis, and decreased inflammatory infiltration. Conclusion: The results show that the herbal extract has strong hepatoprotective action against liver damage caused by paracetamol in rats, perhaps via membrane-stabilizing and antioxidant mechanisms. The study validates the herbal extract's therapeutic potential as a natural hepatoprotective drug and calls for more research to determine its active ingredients and underlying processes.
The term "hepatoprotective" describes a substance's capacity to shield the liver against harm brought on by toxins, medications, chemicals, infections, or other dangerous substances.
The liver, the largest internal organ, is crucial for maintaining physiological homeostasis because it plays a role in metabolism, detoxification, storage, and excretion. It is responsible for the biotransformation of both endogenous and xenobiotic substances, including pharmaceuticals, contaminants in the environment, and food products. Due to its vital function in metabolism and detoxification, the liver is particularly susceptible to harm from toxic chemicals, alcohol, narcotics, and pathogenic agents. Liver diseases continue to be a huge global health burden, greatly raising rates of morbidity and mortality worldwide. Despite advances in modern medicine, controlling liver issues is challenging due to the absence of effective hepatoprotective drugs and the adverse effects of long-term pharmacotherapy.
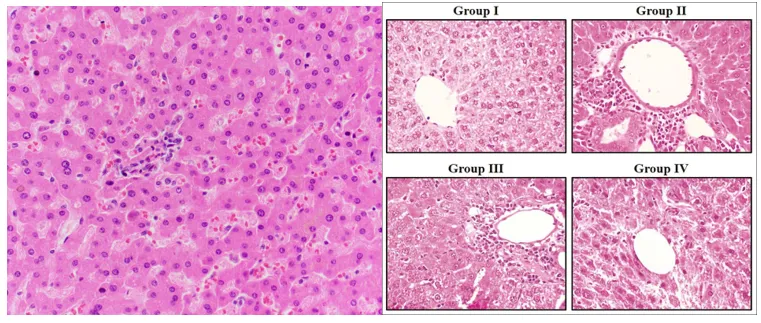
Image No. 01: Normal Liver vs Hepatotoxic Liver Tissue
Drug-induced liver injury (DILI) is one of the most common causes of sudden liver failure. Acetaminophen, another name for paracetamol, is one of the numerous hepatotoxic chemicals that is often used as an analgesic and antipyretic drug and is typically considered safe at therapeutic dosages. However, long-term use or overdosing may result in severe liver damage. The metabolic transformation of paracetamol by cytochrome P450 enzymes into the very reactive intermediate metabolite N-acetyl-p-benzoquinone imine (NAPQI) is the main cause of its hepatotoxicity. NAPQI is usually detoxified by conjugation with glutathione. Overdose-induced glutathione store depletion results in excessive NAPQI accumulation, oxidative stress, lipid peroxidation, mitochondrial dysfunction, and ultimately hepatocellular necrosis.
Experimental models of paracetamol-induced hepatotoxicity are commonly employed to evaluate hepatoprotective medicines because they are reproducible and closely match clinical indications of drug-induced liver damage. Biochemical indicators such as blood levels of bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP) are commonly used to assess liver function and the extent of hepatic damage. Histopathological study can provide further details about cellular and structural alterations in liver tissue.
Recently, there has been a lot of interest in medicinal plants and herbal treatments as potential sources of hepatoprotective compounds. Herbal treatments are rich in bioactive phytoconstituents such flavonoids, phenolic compounds, alkaloids, tannins, terpenoids, and glycosides that have anti-inflammatory, antioxidant, and free radical scavenging qualities. These traits might protect hepatocytes from oxidative damage and promote liver regeneration. Several herbal extracts have demonstrated promising hepatoprotective qualities in experimental animals, supporting their traditional use in the treatment of liver disorders.
The growing interest in natural products has prompted scientific study to establish the therapeutic efficacy of herbal medicines via pharmacological and toxicological tests. However, much remains to be learned about the hepatoprotective properties of many medicinal plants, necessitating thorough evaluation using tried-and-true experimental techniques. The current study was carried out to evaluate the pharmacological hepatoprotective effect of the selected herbal extract against paracetamol-induced liver injury in rats. The study aimed to assess the herbal extract's effects on liver function, biochemical markers and histological changes in hepatic tissue to provide scientific evidence for its potential use as a natural hepatoprotective medication.
Animal Models for Evaluation of Hepatoprotective Activity:
1. Paracetamol-Induced Hepatotoxicity Model
One of the most used experimental models for assessing hepatoprotective action is the paracetamol-induced hepatotoxicity model. In this paradigm, experimental animals, often Wistar rats, are given a high dosage of paracetamol to cause liver injury. N-acetyl-p-benzoquinone imine (NAPQI), a hazardous intermediate produced by the metabolism of excess paracetamol, depletes hepatic glutathione and results in oxidative stress, cellular necrosis, and liver failure. In addition to histological analysis of liver tissues, the hepatoprotective capacity of test substances is evaluated by assessing blood biochemical indicators such ALT, AST, ALP, total bilirubin, and total protein. This model is widely used in hepatoprotective research because of its simplicity, repeatability, and resemblance to drug-induced liver damage in people.
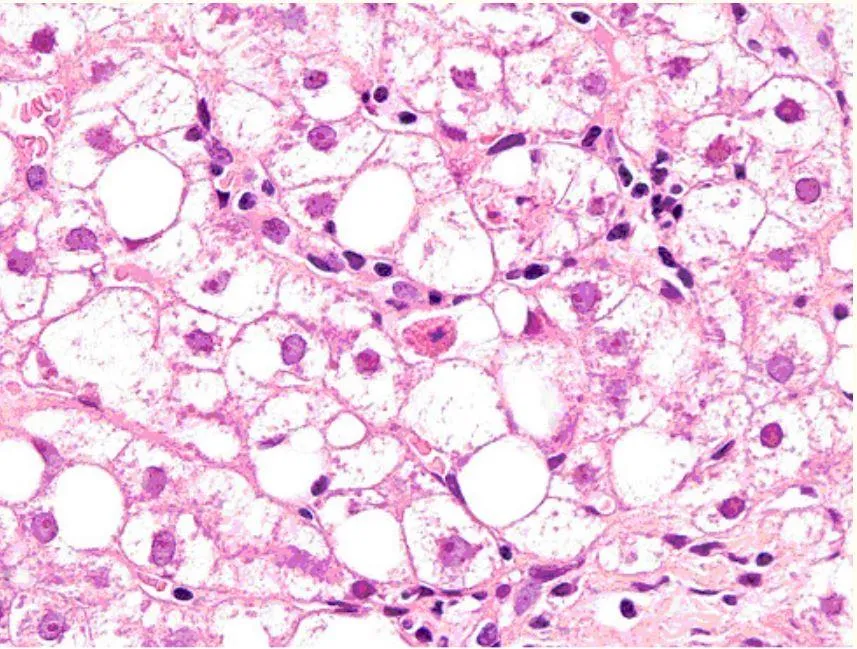
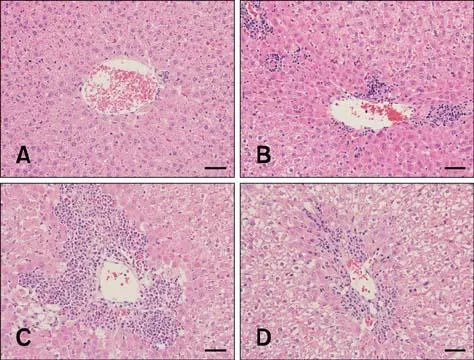
Image No. 02&03: Paracetamol-Induced Hepatotoxicity
2. Carbon Tetrachloride (CCl₄)-Induced Hepatotoxicity Model
For the purpose of screening hepatoprotective drugs, the carbon tetrachloride-induced hepatotoxicity model is regarded as a traditional and reliable technique. When CCl₄ is administered, cytochrome P450 enzymes activate its metabolism, producing very reactive free radicals such as trichloromethyl radicals. These free radicals cause hepatocellular necrosis, inflammation, and damage to membranes by starting lipid peroxidation. Serious histological changes and increased liver enzyme levels are seen in experimental animals given CCl₄. The capacity of hepatoprotective substances to lessen biochemical abnormalities and restore normal liver architecture is used to assess them. When examining the antioxidant and membrane-stabilising qualities of synthetic medications and plant extracts, this model is especially helpful.
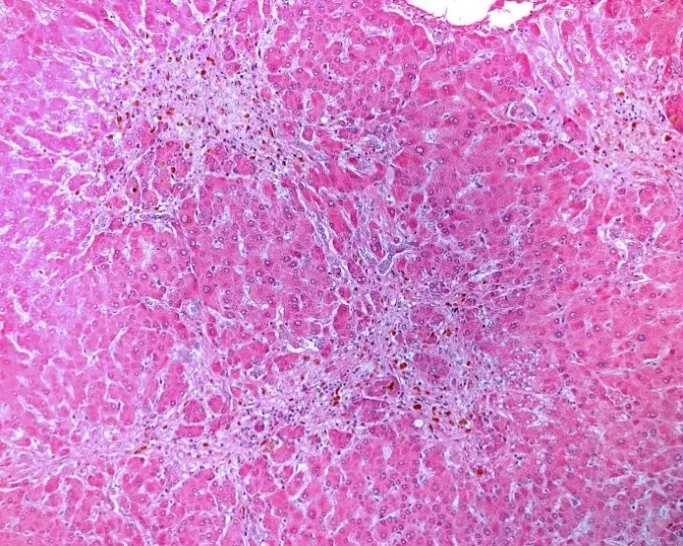
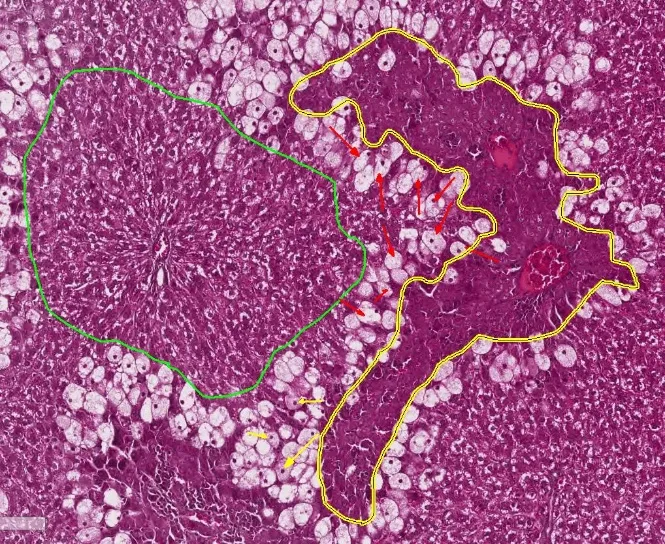
Image No. 04&05: Carbon Tetrachloride (CCl4)-Induced Hepatotoxicity
3. Ethanol-Induced Hepatotoxicity Model:
The ethanol-induced hepatotoxicity model is frequently used to investigate how chemicals might prevent alcohol-related liver damage. Hepatocyte degeneration, oxidative stress, inflammation, and lipid buildup are all brought on by repeated or prolonged ethanol intake. These pathological alterations are similar to those found in human alcoholic liver disease. By evaluating liver function indicators, antioxidant enzyme levels, lipid peroxidation parameters, and histological alterations in liver tissue, hepatoprotective drugs' effectiveness is assessed. This approach is particularly useful for assessing herbal medicines that have anti-inflammatory, anti-steatotic, and antioxidant properties.
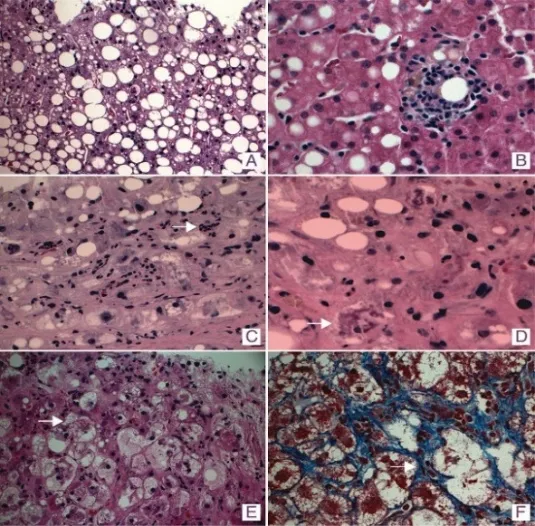
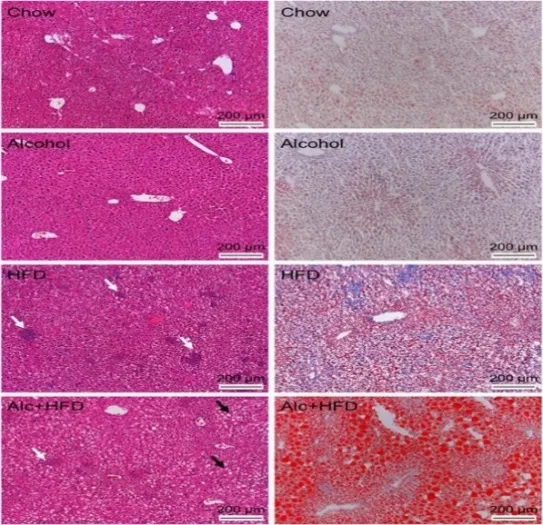
Image No. 06&07: Ethanol-Induced Hepatotoxicity Model
Typical Histopathological Changes in Hepatotoxicity
Damage to the liver brought on by medications, chemicals, poisons, alcohol, or other dangerous substances is referred to as hepatotoxicity. Depending on the kind and pattern of liver damage, it can be divided into many categories.
1. Hepatocellular Hepatotoxicity
Hepatocytes (liver cells) are the main target of this most prevalent kind of liver damage. Serum liver enzyme levels, especially those of ALT and AST, are markedly elevated. Viral infections, some medications, and paracetamol overdose are common causes. Hepatocellular damage is histologically linked to necrosis and cell degeneration.
2. Cholestatic Hepatotoxicity
Bile production or flow is compromised in cholestatic liver damage. Elevated bilirubin and alkaline phosphatase (ALP) values are its hallmarks. Jaundice, itching, and black urine are possible symptoms. Oral contraceptives, anabolic steroids, and certain antibiotics have been shown to cause cholestatic hepatotoxicity.
3. Mixed Hepatocellular-Cholestatic Hepatotoxicity
Hepatocellular and cholestatic liver damage characteristics are present in this kind. There is an increase in both cholestatic indicators and liver enzymes. This heterogeneous pattern of liver damage can be caused by several drugs.
4. Acute Hepatotoxicity
After being exposed to a harmful chemical, acute hepatotoxicity typically appears within hours or days. If severe, it can lead to abrupt liver failure. Acute hepatotoxicity is frequently caused by a paracetamol overdose.
5. Chronic Hepatotoxicity
Prolonged exposure to hazardous chemicals causes chronic hepatotoxicity, which develops gradually over weeks, months, or years. Chronic drug usage and long-term alcohol consumption are frequent factors. Liver cancer, cirrhosis, or fibrosis can develop from chronic damage.
6. Drug-Induced Hepatotoxicity
Drug side effects can lead to drug-induced liver damage (DILI). It is among the most common reasons for acute liver failure. Isoniazid, methotrexate, and paracetamol are a few examples.
7. Alcohol-Induced Hepatotoxicity
Excessive alcohol consumption causes liver damage through oxidative stress and inflammation. The progression typically includes:
8. Chemical-Induced Hepatotoxicity
Liver damage can result from exposure to industrial chemicals, insecticides, and environmental pollutants. Chemicals like carbon tetrachloride (CCl₄) and thioacetamide are frequently used in experimental models to cause hepatotoxicity.
9. Immune-Mediated Hepatotoxicity
In this case, exposure to specific medications or substances causes the immune system to contribute to liver damage. The damage can be similar to autoimmune hepatitis.
CONCLUSION:
The current investigation showed that the herbal extract had important neuroprotective and cognitive-enhancing benefits against epilepsy in rats caused by quinolinic acid or kainic acid. When the extract was administered, it successfully decreased the intensity of seizures, enhanced cognitive function, repaired altered neurochemical parameters, and prevented the degradation of neuronal tissues. The phytoconstituents in the extract have antioxidant, anti-inflammatory, anti-excitotoxic, and neurotransmitter-modulating qualities that may be responsible for the reported neuroprotective action. These results imply that the herbal extract has significant therapeutic potential for the management and prevention of neurological and cognitive deficits linked to epilepsy. It is advised that more research be done to identify and describe the active phytoconstituents as well as to clarify the exact processes behind its neuroprotective and cognition-enhancing properties.
ACKNOWLEDGEMENT
The authors express their sincere gratitude to Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune, Maharashtra, India, for providing the necessary facilities, infrastructure, and academic support to carry out this research work successfully.
AUTHOR CONTRIBUTIONS
Conception and Design of the Work: Yogiraj Dayanand Lokhande, Ulka Mote
Experimental Work and Data Collection: Yogiraj Dayanand Lokhande
Analysis and Interpretation of Data: Yogiraj Dayanand Lokhande, Ulka Mote, Dr. Pravin Uttekar
Drafting of the Manuscript: Yogiraj Dayanand Lokhande
Critical Revision for Important Intellectual Content: Ulka Mote, Dr. Pravin Uttekar
Final Approval of the Version to be Published: Yogiraj Dayanand Lokhande, Ulka Mote, Dr. Pravin Uttekar
AUTHORS AND AFFILIATIONS:
Yogiraj Dayanand Lokhande¹:
Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune 413114, Maharashtra, India.
Ulka Mote² (Guide):
Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune 413114, Maharashtra, India.
Dr. Pravin Uttekar³ (Principal):
Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune 413114, Maharashtra, India.
CONFLICT OF INTEREST:
The authors declare that there is no conflict of interest regarding the publication of this research work.
FUNDING SUPPORT:
The authors declare that no external funding was received for this study. The research work was conducted using the facilities and resources available at Late Laxmibai Phadtare College of Pharmacy, DBATU University, Kalamb, Pune, Maharashtra, India.
REFERENCES

: Yogiraj Lokhande, Ulka Mote, Pravin Uttekar, Pharmacological Evaluation of the Hepatoprotective Potential of Herbal Extract in Paracetamol-Induced Liver Injury in Rats, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4176-4184. https://doi.org/ 10.5281/zenodo.20730473
 10.5281/zenodo.20730473
10.5281/zenodo.20730473