
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Late Laxmibai Phadtare College of Pharmacy A/P-Kalamb-Walchandnagar,Tal : Indapur Dist : Pune.
Background: Isoniazid (INH) and rifampicin (RIF) are the most effective first-line drugs for treating tuberculosis, but their use is frequently complicated by drug-induced liver injury (DILI). INH-RIF hepatotoxicity is a major cause of morbidity and treatment discontinuation. The pathogenesis is multifactorial, involving metabolic bioactivation of INH to toxic hydrazine intermediates, profound oxidative stress, mitochondrial dysfunction, and inflammatory cell infiltration, a process often exacerbated by RIF's potent induction of cytochrome P450 enzymes.Objective: This review provides a comprehensive framework for the pharmacological evaluation of herbal extracts as hepatoprotective agents against INH-RIF-induced liver injury. It synthesizes the current understanding of the molecular mechanisms of toxicity and outlines the key pathways targeted by hepatoprotective phytochemicals.Methods: We review the pathophysiology of INH-RIF hepatotoxicity, detailing the roles of CYP2E1, oxidative stress, and mitochondrial damage. A methodological guide for preclinical evaluation is presented, including in vivo rodent models, key biochemical and histological biomarkers, and relevant molecular endpoints. The hepatoprotective mechanisms of prominent herbal extracts—such as silymarin, curcumin, and glycyrrhizin—are discussed, focusing on their ability to activate the Nrf2 antioxidant response, suppress NF-?B-mediated inflammation, and stabilize mitochondria.Conclusion: Herbal extracts containing flavonoids, polyphenols, and triterpenoids demonstrate significant hepatoprotective potential against INH-RIF DILI in preclinical models. Their ability to counteract oxidative stress and inflammation forms the basis of their therapeutic action. However, significant translational challenges remain, including the need for rigorous standardization, dose-optimization, and careful assessment of potential herb-drug interactions, which could alter the efficacy of the antitubercular regimen. This review provides a roadmap for future research to harness the therapeutic potential of phytomedicines safely and effectively as adjuncts in tuberculosis therapy.
Tuberculosis (TB), caused by Mycobacterium tuberculosis, remains one of the world's deadliest infectious diseases. The standard treatment regimen, a combination therapy including isoniazid (INH) and rifampicin (RIF), is highly effective but carries a significant risk of drug-induced liver injury (DILI) [1]. Hepatotoxicity is the most common adverse reaction leading to the interruption or discontinuation of TB treatment, which can result in therapy failure, drug resistance, and increased mortality [2].
The incidence of INH-RIF-induced hepatotoxicity varies but can affect up to 30% of patients, with severe hepatitis occurring in a smaller but significant subset [3]. The mechanism of injury is complex and involves both metabolic idiosyncrasy and direct cellular toxicity (Figure 1). Isoniazid is metabolized to reactive intermediates, such as acetylhydrazine and hydrazine, which generate free radicals and cause severe oxidative stress [4]. Rifampicin, a potent inducer of hepatic cytochrome P450 (CYP) enzymes (particularly CYP2E1 and CYP3A4), can accelerate the toxic bioactivation of INH, thereby amplifying liver damage when the drugs are used in combination [5].
Given that oxidative stress and inflammation are central to the pathogenesis of INH-RIF DILI, there is growing interest in using hepatoprotective agents as adjuncts to TB therapy. Herbal extracts, rich in antioxidant and anti-inflammatory phytochemicals like flavonoids, polyphenols, and triterpenoids, are particularly attractive candidates [6]. Plants such as Silybum marianum (milk thistle), Curcuma longa (turmeric), and Glycyrrhiza glabra (licorice) have been used for centuries in traditional medicine to treat liver ailments and are now being rigorously investigated for their potential to mitigate DILI [7, 8].
This review provides a comprehensive overview of the pharmacological strategies used to evaluate the hepatoprotective potential of herbal extracts against INH-RIF-induced liver injury, detailing the underlying mechanisms of toxicity and protection, the experimental models employed, and the key translational challenges that must be addressed.
FIGURE 1: MECHANISTIC OVERVIEW OF INH-RIF HEPATOTOXICITY & HERBAL INTERVENTION
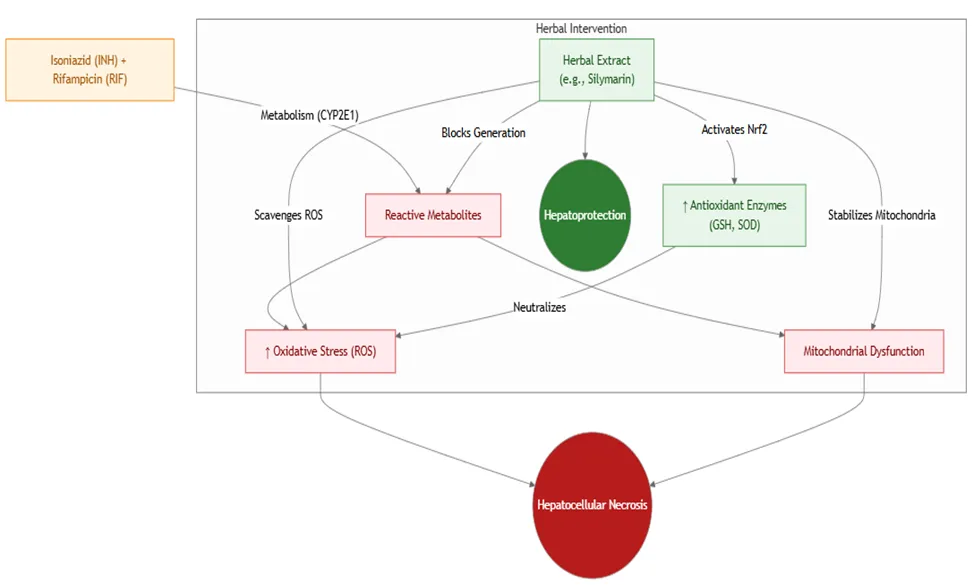
Figure 1: Mechanism of INH-RIF Liver Injury and Herbal Protection
This flowchart illustrates how INH and RIF work together to induce a cascade of cellular injury driven by oxidative stress, and how herbal extracts can intervene at multiple points to confer hepatoprotection.
2. PATHOPHYSIOLOGY OF INH-RIF INDUCED LIVER INJURY
The liver injury induced by antitubercular drugs is a classic example of metabolism-dependent toxicity. The mechanisms for INH and RIF are distinct but synergistic (Table 1).
2.1. Isoniazid (INH) Metabolism and Toxicity
INH is primarily metabolized in the liver. It is first acetylated by N-acetyltransferase 2 (NAT2) to form acetylisoniazid, which is then hydrolyzed to acetylhydrazine. Acetylhydrazine is considered the main hepatotoxic metabolite. It is further oxidized by CYP2E1 to form highly reactive intermediates that covalently bind to cellular macromolecules, deplete glutathione (GSH), and generate substantial oxidative stress, leading to mitochondrial damage and hepatocyte necrosis [4, 9]. Individuals who are "slow acetylators" (due to NAT2 genetic polymorphisms) may have a higher risk of toxicity as more INH is shunted down alternative, more toxic pathways.
2.2. Rifampicin (RIF) and its Role
While RIF can occasionally cause liver injury on its own (often cholestatic), its primary role in INH-RIF DILI is as a potent enzyme inducer. RIF activates the Pregnane X Receptor (PXR), a nuclear receptor that upregulates the expression of numerous drug-metabolizing enzymes, including CYP2E1 and CYP3A4 [5]. By inducing CYP2E1, RIF accelerates the conversion of acetylhydrazine to its toxic electrophilic species, thereby potentiating INH-induced hepatotoxicity. This synergy is the reason the combination therapy carries a much higher risk of DILI than either drug alone.
TABLE 1: COMPARISON OF HEPATOTOXIC MECHANISMS OF INH AND RIF
|
Feature |
Isoniazid (INH) |
Rifampicin (RIF) |
|
Primary Mechanism |
Metabolic bioactivation to reactive hydrazine metabolites. |
Potent induction of drug-metabolizing enzymes (PXR agonist). |
|
Key Enzyme Involved |
CYP2E1 (for toxic activation). |
Inducer of CYP2E1, CYP3A4, and others. |
|
Primary Cellular Damage |
Oxidative stress, mitochondrial dysfunction, hepatocellular necrosis. |
Can cause cholestasis; primarily potentiates INH toxicity. |
|
Key Toxic Metabolite |
Acetylhydrazine and its reactive intermediates. |
Generally considered less directly toxic than INH metabolites. |
|
Synergistic Effect |
Its toxicity is amplified by RIF. |
Amplifies the metabolic activation and toxicity of INH. |
3. PHARMACOLOGICAL EVALUATION METHODOLOGY
A systematic approach is required to evaluate the hepatoprotective potential of an herbal extract. This involves using a validated animal model and measuring a comprehensive panel of biomarkers.
3.1. In Vivo Animal Model
The most common model involves inducing hepatotoxicity in rodents (typically Wistar rats or Swiss albino mice) by co-administering INH and RIF orally for a period of 14 to 45 days.
3.2. Evaluation Parameters and Biomarkers
At the end of the study, blood and liver tissue are collected for a multi-faceted analysis (Table 2).
3.3. Histopathological Examination
Liver sections are stained with Hematoxylin and Eosin (H&E) to observe structural changes such as central vein congestion, inflammatory cell infiltration, hepatocyte necrosis, and fatty changes. A scoring system is often used to quantify the degree of damage. An effective hepatoprotective agent should significantly reduce these pathological features.
4. KEY HERBAL EXTRACTS AND THEIR MECHANISMS
Several herbal extracts have shown significant promise in preclinical models of INH-RIF DILI. Their mechanisms generally converge on antioxidant and anti-inflammatory pathways (Table 3).
4.1. Silybum marianum (Milk Thistle)
The extract of milk thistle, known as silymarin, is the most widely studied and clinically used natural hepatoprotective agent. Its primary active component is silibinin. Silymarin's mechanisms include:
TABLE 2: KEY BIOMARKERS FOR EVALUATING HEPATOPROTECTION
|
Category |
Parameter |
Significance |
Expected Result with Protection |
|
Serum Biochemistry |
Alanine Aminotransferase (ALT) |
Marker of hepatocellular injury. |
↓ Decrease |
|
Aspartate Aminotransferase (AST) |
Marker of hepatocellular injury. |
↓ Decrease |
|
|
Alkaline Phosphatase (ALP) |
Marker of cholestasis and biliary injury. |
↓ Decrease |
|
|
Total Bilirubin |
Marker of liver excretory function. |
↓ Decrease |
|
|
Oxidative Stress Markers (Liver Tissue) |
Malondialdehyde (MDA) |
Product of lipid peroxidation. |
↓ Decrease |
|
Reduced Glutathione (GSH) |
Key endogenous antioxidant. |
↑ Increase / Restoration |
|
|
Superoxide Dismutase (SOD) |
Antioxidant enzyme. |
↑ Increase / Restoration |
|
|
Catalase (CAT) |
Antioxidant enzyme. |
↑ Increase / Restoration |
|
|
Inflammatory Markers (Liver Tissue) |
Tumor Necrosis Factor-alpha (TNF-α) |
Pro-inflammatory cytokine. |
↓ Decrease |
|
Interleukin-6 (IL-6) |
Pro-inflammatory cytokine. |
↓ Decrease |
|
|
Histopathology (Liver Tissue) |
H&E Staining |
Visualization of necrosis, inflammation, steatosis. |
↓ Reduced cellular damage |
|
Masson’s Trichrome Staining |
Visualization of collagen deposition (fibrosis). |
↓ Reduced fibrosis |
FIGURE 2: MOLECULAR TARGETS OF HEPATOPROTECTIVE PHYTOCHEMICALS
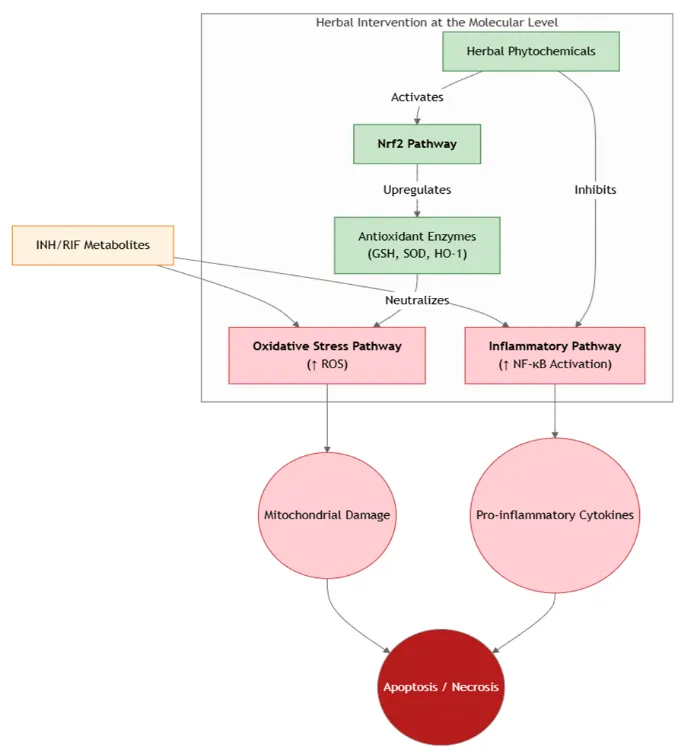
Figure 2: Molecular Targets for Hepatoprotection
This diagram illustrates the key intracellular pathways targeted by herbal phytochemicals. They primarily act by boosting the cell's own antioxidant defense system via the Nrf2 pathway and by suppressing the pro-inflammatory NF-κB pathway.
4.2. Curcuma longa (Turmeric)
Curcumin, the active polyphenol in turmeric, is a powerful anti-inflammatory and antioxidant agent. It protects the liver by:
4.3. Glycyrrhiza glabra (Licorice)
The main active component of licorice root is glycyrrhizin, a triterpenoid saponin. It has demonstrated hepatoprotective effects through:
5. TRANSLATIONAL CHALLENGES AND FUTURE DIRECTIONS
While preclinical results are promising, several critical hurdles must be overcome before herbal extracts can be safely used as adjuncts in clinical TB therapy.
5.1. Herb-Drug Interactions
This is the most significant concern. Many herbal extracts, including some mentioned above, can inhibit or induce CYP enzymes.
TABLE 3: EXAMPLES OF HEPATOPROTECTIVE HERBS AND THEIR MECHANISMS
|
Herbal Extract |
Key Active Constituent(s) |
Primary Hepatoprotective Mechanism(s) |
|
Silybum marianum (Milk Thistle) |
Silymarin (Silibinin) |
Antioxidant, membrane stabilization, anti-fibrotic. The "gold standard" positive control. |
|
Curcuma longa (Turmeric) |
Curcuminoids (Curcumin) |
Potent Nrf2 activator, NF-κB inhibitor, direct ROS scavenging. |
|
Glycyrrhiza glabra (Licorice) |
Glycyrrhizin, Glabridin |
Anti-inflammatory, antioxidant, membrane stabilization. |
|
Andrographis paniculata |
Andrographolide |
Reduces oxidative stress, inhibits NF-κB, protects mitochondria. |
|
Phyllanthus amarus |
Phyllanthin, Hypophyllanthin |
Antioxidant, anti-inflammatory, hepatocyte membrane protection. |
|
Green Tea Extract |
Epigallocatechin gallate (EGCG) |
Potent antioxidant, modulates drug-metabolizing enzymes. |
5.2. Standardization and Quality Control
The chemical composition of herbal extracts can vary significantly based on plant source, growing conditions, and extraction methods. For clinical use, extracts must be standardized to a specific concentration of one or more bioactive marker compounds to ensure batch-to-batch consistency in potency and safety.
5.3. Dose-Finding and Safety Studies
Effective and safe doses need to be established. High doses of some herbal compounds can even be pro-oxidant or hepatotoxic themselves. A thorough toxicological evaluation is mandatory.
5.4. Clinical Trials
Ultimately, well-designed, randomized, placebo-controlled clinical trials are needed to prove that an herbal adjunct can reduce the incidence of DILI in TB patients without compromising the efficacy of the antitubercular treatment.
CONCLUSION
INH-RIF-induced hepatotoxicity is a serious clinical problem driven by metabolism-dependent oxidative stress and inflammation. Herbal extracts rich in antioxidant and anti-inflammatory phytochemicals have demonstrated significant hepatoprotective potential in a wealth of preclinical studies. They act by bolstering endogenous antioxidant defenses (often via the Nrf2 pathway), suppressing pro-inflammatory signaling (NF-κB), and stabilizing cellular membranes. While this provides a strong rationale for their use as adjuncts to TB therapy, the risk of clinically significant herb-drug interactions is substantial and cannot be overlooked. Future research must focus on using standardized extracts, elucidating their precise effects on drug metabolism, and conducting carefully controlled clinical trials to validate both their safety and efficacy in the patient population.
REFERENCES

Bhagyashri Ghadage, Ulka Mote, Dr. Pravin Uttekar, Sagar Daitkar, Pharmacological Evaluation of the Hepatoprotective Potential of Herbal Extracts in Isoniazid- and Rifampicin-Induced Liver Injury: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2289-2296, https://doi.org/10.5281/zenodo.20609698
 10.5281/zenodo.20609698
10.5281/zenodo.20609698