
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shreeshakti Shakshanik Sanstha, Divine College of Pharmacy Nampur Road Satana,Nashik - 423 301, Maharashtra, India.
Urolithiasis is a common and recurrent renal disorder characterized by the formation of calcium oxalate calculi, often associated with high recurrence rates and limitations of current therapeutic approaches. This review critically evaluates phytotherapeutic strategies in the management of urolithiasis, focusing on their mechanisms of action, pharmacological evidence, and clinical relevance. A comprehensive analysis of recent literature (2020-2025) highlights the anti-urolithiatic potential of medicinal plants such as Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis. These plants exhibit multi-targeted activity by inhibiting calcium oxalate nucleation, growth, and aggregation; enhancing urinary dilution through diuretic effects; promoting citrate-mediated calcium chelation; and reducing oxidative stress and inflammation within renal tissues. Experimental studies consistently demonstrate improvement in urinary biochemical parameters, reduction in crystal deposition, and protection of renal epithelial integrity, while limited clinical and epidemiological evidence suggests a role in reducing recurrence risk. Overall, phytotherapeutic approaches offer promising adjunctive benefits in urolithiasis management; however, further well-designed clinical studies and standardized formulations are required to establish their efficacy and therapeutic consistency
Medicinal plants have historically served as a primary source of therapeutic agents and continue to contribute significantly to modern drug discovery. Traditional medical systems such as Ayurveda, Siddha, and Traditional Chinese Medicine have long utilized plant-based remedies for the management of urinary disorders, including kidney stone disease. In recent years, there has been renewed scientific interest in phytotherapeutics due to the limitations associated with synthetic drugs, including adverse effects, high cost, and inability to prevent disease recurrence. Natural products offer a multi-targeted mode of action, making them particularly valuable in complex and multifactorial disorders such as urolithiasis [1]. Urolitiasis is a common and recurrent disorder of the urinary tract characterized by the formation of crystalline calculi within the kidneys, ureters, or bladder. The majority of stones are composed of calcium oxalate, followed by calcium phosphate, uric acid, and struvite. The pathogenesis of kidney stone formation involves supersaturation of urinary solutes, nucleation, crystal growth, aggregation, and retention within renal tubules [2]. Oxidative stress, inflammation, metabolic abnormalities, dietary habits, dehydration, and genetic predisposition are recognized as major contributing factors [3]. The disease imposes a significant clinical and economic burden due to severe pain, risk of urinary obstruction, renal epithelial injury, and high recurrence rates.
Current management strategies include extracorporeal shock wave lithotripsy, percutaneous nephrolithotomy, ureteroscopy, and pharmacological interventions such as thiazide diuretics, potassium citrate, and allopurinol. Although these approaches are effective in stone removal, they are associated with several limitations, including incomplete clearance, recurrence, adverse drug reactions, and high treatment costs [4,5]. These challenges have stimulated the search for safer and more effective preventive agents, particularly those derived from medicinal plants [6]. Among the various botanicals traditionally used for urinary disorders, Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis peel have received considerable pharmacological attention due to their reported anti-urolithiatic properties. Tribulus terrestris (Gokharu), a well-known Ayurvedic mutrala (diuretic) drug, is rich in steroidal saponins, flavonoids, and alkaloids that exhibit diuretic, antioxidant, and crystal-inhibitory activities [7]. Bryophyllum pinnatum, commonly referred to as Patharchatta or stonebreaker, contains flavonoids, phenolic acids, bufadienolides, and triterpenoids that contribute to nephroprotective, anti-inflammatory, and lithotriptic effects. Orange peel (Citrus sinensis), an abundant agro-industrial by-product, is a valuable source of flavonoids such as hesperidin and naringin, along with citric acid and essential oils that enhance urinary citrate levels and inhibit calcium oxalate crystallization [8].
Phytochemicals present in these plants are known to interfere with multiple stages of stone formation. Their mechanisms include increasing urinary output, reducing urinary supersaturation of lithogenic ions, inhibiting crystal nucleation and aggregation, chelating calcium ions, modulating urinary pH, and protecting renal tubular epithelium from oxidative and inflammatory damage [9]. Such multi-mechanistic activity makes these plants promising candidates for both prevention and management of urolithiasis [10].
The present review aims to critically compile and analyze the available literature on the phytochemical composition and pharmacological activities of Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis peel with special emphasis on their anti-urolithiatic potential. The review discusses their traditional uses, bioactive constituents, mechanisms of action, experimental evidence, safety profile, and future research prospects [11]. In addition, challenges related to standardization, quality control, and clinical validation of herbal formulations are highlighted. By integrating traditional knowledge with contemporary pharmacological findings, this review seeks to provide a scientific basis for the development of plant-based therapeutic strategies for the effective management of kidney stone disease.
2. Pathophysiology of Urolithiasis
Urolithiasis is a multistep physicochemical and cellular process involving crystal nucleation, growth, aggregation, and retention within the renal tubules. Nucleation may occur spontaneously in supersaturated urine (homogeneous nucleation) or on pre-existing surfaces such as cellular debris, urinary macromolecules, or Randall’s plaques (heterogeneous nucleation). Calcium oxalate monohydrate crystals are the most thermodynamically stable form and exhibit strong adherence to tubular epithelial cells. Subsequent crystal growth results from continued ionic deposition from supersaturated urine, while aggregation leads to the formation of larger particles capable of tubular obstruction [12]. Crystal retention is facilitated by epithelial injury, exposure of the basement membrane, and calcium phosphate plaques in the renal papillae that act as anchoring sites. Oxalate-induced oxidative stress promotes lipid peroxidation, mitochondrial dysfunction, and apoptosis, which up-regulate adhesion molecules such as CD44 and annexin II, enhancing crystal attachment. Inflammatory mediators, including TNF-α and IL-6, further exacerbate epithelial damage. A reduction in endogenous inhibitors such as citrate, magnesium, glycosaminoglycans, and nephrocalcin increases the likelihood of crystallization. Metabolic disorders, dehydration, and dietary factors contribute to urinary supersaturation and disease progression.
3. Mechanisms of Anti-urolithiatic Action
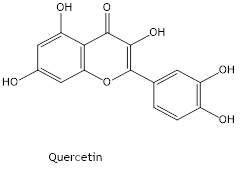
The anti-urolithiatic activity of Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis is mediated through multiple complementary mechanisms that target key stages of stone pathogenesis. One of the primary events in urolithiasis is urinary supersaturation with calcium and oxalate, which initiates crystal nucleation and subsequent growth. Phytoconstituents such as flavonoids (e.g., quercetin and kaempferol) possess hydroxyl groups capable of chelating free calcium ions, thereby lowering ionic activity and reducing the likelihood of nucleation. Citrate derived from citrus peel forms soluble calcium–citrate complexes that inhibit crystal formation and limit further growth. In addition, adsorption of saponins and phenolic compounds onto the crystal surface modifies crystal habit, promoting conversion of the highly adhesive calcium oxalate monohydrate to the less adherent dihydrate form, which diminishes aggregation and facilitates urinary elimination [13-15]. An increase in urinary output represents another important protective mechanism. The diuretic effect attributed to steroidal saponins and potassium salts enhances glomerular filtration and urinary flow, leading to dilution of lithogenic ions and reduced residence time of microcrystals within renal tubules. This mechanical washout effect decreases opportunities for crystal aggregation and retention. Antioxidant activity also plays a central role in nephroprotection. Oxalate-induced reactive oxygen species can damage tubular epithelial cells, generating cellular debris that serves as a nidus for crystal attachment. Polyphenols and related compounds augment endogenous antioxidant defenses, including superoxide dismutase, catalase, and glutathione, while reducing lipid peroxidation markers, thereby preserving epithelial integrity and limiting crystal adherence [16].
Anti-inflammatory actions further contribute to the inhibition of stone formation. Bioactive metabolites suppress pro-inflammatory mediators and cytokine-associated pathways, reducing leukocyte infiltration, tubular injury, and interstitial inflammation. This effect is particularly relevant in preventing Randall’s plaque development and in facilitating the passage of small calculi by decreasing ureteral irritation. Modulation of urinary biochemical parameters constitutes an additional mechanism. Experimental findings indicate reduced urinary excretion of calcium, oxalate, and phosphate, accompanied by increased levels of magnesium and citrate, both of which act as endogenous inhibitors of crystallization. Citrate-mediated alkalinization of urine further limits the formation of calcium-based stones. Improvement in serum creatinine and urea observed in preclinical models reflects restoration of renal function and reduced tubular damage. Collectively, these multi-targeted actions create a urinary milieu unfavorable for crystal formation, promote dissolution of existing microcrystals, and support the prevention of recurrent calculi [17].
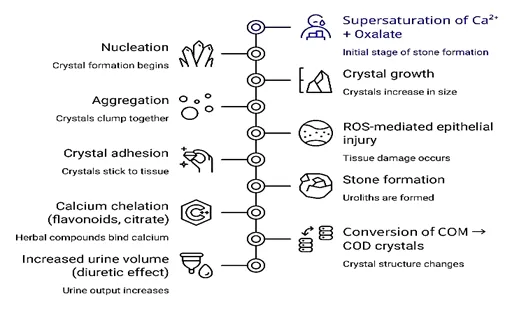
Fig. 1. Mechanism of anti-urolithic action
4. Pharmacological and phytochemical profile of Tribulus terrestris L.
4.1 Botanical Description and Distribution
Tribulus terrestris L. (family: Zygophyllaceae) is a prostrate, mat-forming annual herb widely distributed in tropical and subtropical regions of India, China, Africa, Europe, and the Mediterranean basin. The plant grows in dry, sandy, and wasteland areas and is commonly known as Gokharu or Gokshura in Ayurveda. It is characterized by pinnate leaves, yellow solitary flowers, and distinctive spiny fruits composed of five woody cocci. The fruits and roots are primarily used for medicinal purposes, particularly in urinary disorders. In Ayurvedic texts, Gokshura is classified under “Mutrala dravya,” indicating its diuretic and urinary tract protective properties [18,19].
4.2 Ethnomedicinal Importance in Renal Disorders
Tribulus terrestris (Gokshura) occupies a well-established position in traditional systems of medicine for the management of urinary and renal ailments. In Ayurveda, the drug is classified under Mutravirechaniya (diuretic) and Ashmarighna (anti-urolithiatic) groups, indicating its therapeutic utility in promoting urine flow and alleviating calculi. It is a principal component of classical polyherbal formulations such as Gokshuradi Guggulu and Dashamoola, which are prescribed for dysuria, urinary retention, burning micturition, and stone expulsion. Folk practices describe the use of fruit and whole-plant preparations as soothing agents for irritated urinary passages, where their demulcent properties help reduce mucosal inflammation and discomfort. The herb is traditionally regarded as a lithotriptic, facilitating fragmentation and elimination of urinary stones while restoring normal micturition. These long-standing ethnomedicinal applications are consistent with pharmacological observations showing enhanced diuresis, reduction in urinary supersaturation, and inhibition of crystal formation, thereby providing a scientific rationale for its use in renal stone management [20].
4.3 Phytochemical Constituents
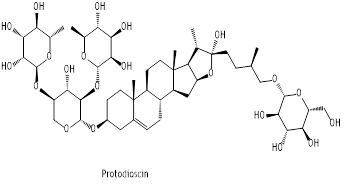
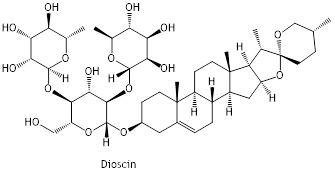
The pharmacological activity of Tribulus terrestris is primarily attributed to its rich and heterogeneous phytochemical composition, which includes steroidal saponins, flavonoids, alkaloids, phenolic glycosides, tannins, and essential mineral elements [21]. Steroidal saponins such as protodioscin, dioscin, tribulosin, and protogracillin constitute the major bioactive fraction and possess furostanol or spirostanol nuclei with glycosidic linkages that are associated with diuretic action, membrane stabilization, and inhibition of calcium oxalate crystallization; protodioscin is commonly regarded as the principal marker compound contributing to anti-urolithiatic efficacy [22]. Flavonoids including quercetin, kaempferol, and isorhamnetin exhibit potent antioxidant and nephroprotective effects by scavenging reactive oxygen species and preventing lipid peroxidation in renal tissues. Minor quantities of harmane-type and β-carboline alkaloids provide smooth muscle relaxant and anti-inflammatory activities that may facilitate ureteral relaxation and stone expulsion. Additionally, phenolic glycosides and tannins confer metal-chelating capacity, reducing free ionic calcium and thereby limiting crystal nucleation and growth, while naturally occurring potassium and magnesium salts help decrease urinary supersaturation of calcium oxalate, collectively supporting the plant’s anti-lithogenic potential [23].
4.4 Pharmacological Potential Relevant to Kidney Stones
Hydroalcoholic and aqueous preparations of Tribulus terrestris exhibit pronounced pharmacological activity against urolithiasis through a multifactorial mode of action. Experimental hyperoxaluric models consistently demonstrate a marked diuretic effect, reflected by increased urine volume and enhanced excretion of sodium and potassium, which dilutes lithogenic solutes and lowers urinary supersaturation [24]. Concomitantly, treatment reduces urinary concentrations of calcium, oxalate, and phosphate while elevating magnesium levels, thereby limiting calcium oxalate crystal deposition and preserving renal
tubular morphology [25]. In vitro crystallization assays further confirm inhibition of nucleation, growth, and aggregation of calcium oxalate crystals. The flavonoid-rich fraction augments endogenous antioxidant defenses by upregulating superoxide dismutase, catalase, and glutathione peroxidase, which protects renal epithelial cells from oxalate-induced oxidative injury and prevents formation of adhesion sites for crystals. Additionally, downregulation of pro-inflammatory mediators such as tumor necrosis factor-α and interleukin-6 mitigates tubular inflammation, maintains epithelial integrity, and facilitates the expulsion of microcrystals. These coordinated actions including enhanced urinary flow, calcium chelation, antioxidant cytoprotection, and anti-inflammatory effects collectively create an unfavorable environment for crystal formation and substantiate the traditional use of the plant as a primary herbal intervention for kidney stone management [26].
4.5 Preclinical and Clinical Studies
Multiple experimental investigations have substantiated the anti-urolithiatic efficacy of Tribulus terrestris in ethylene glycol- and sodium oxalate–induced lithiasis models. Administration of aqueous and hydroalcoholic extracts has been shown to significantly decrease urinary oxalate, calcium, and phosphate concentrations while enhancing urine volume and magnesium excretion, thereby lowering lithogenic risk. Histopathological evaluations consistently demonstrate reduced calcium oxalate crystal deposition, preservation of renal tubular integrity, and attenuation of interstitial inflammation [27].
Dose-dependent normalization of serum creatinine, urea, and uric acid levels, along with improved creatinine clearance, indicates restoration of renal function. The anti-lithic efficacy has been reported to be comparable to standard herbal formulations such as Cystone in certain preclinical models. In sodium oxalate–induced nephrolithiasis, treatment with T. terrestris extracts reduces lipid peroxidation and restores endogenous antioxidant enzymes, confirming protection against oxalate-mediated oxidative injury [28].
Acute toxicity studies reveal a wide safety margin, with no mortality or significant behavioral changes observed at doses up to 2000 mg/kg in rodents, suggesting a favorable therapeutic index. Although controlled clinical trials remain limited, traditional usage and preliminary clinical observations support its role as an adjuvant therapy in the management of urolithiasis, particularly for small calculi and recurrent stone formers. Rigorous randomized clinical studies are necessary to establish standardized dosage regimens, long-term safety, and definitive clinical efficacy [29].
5. Pharmacological and phytochemical profile of Bryophyllum pinnatum
5.1 Botanical Description and Distribution
Bryophyllum pinnatum (Lam.) Oken, belonging to the family Crassulaceae, is a perennial succulent herb widely recognized for its medicinal properties. The plant is commonly known as Pattharchatta, Panphuti, or life plant in traditional systems of medicine. It is characterized by fleshy, ovate leaves with crenate margins that bear adventitious plantlets, a hollow erect stem, and pendulous tubular flowers that are greenish-purple in color. The plant exhibits xerophytic adaptations and thrives in warm, humid climates.
Geographically, Bryophyllum pinnatum is distributed across tropical and subtropical regions, including India, Sri Lanka, China, Africa, Madagascar, and parts of South America. In India, it is commonly cultivated in household gardens and grows abundantly in Maharashtra, Gujarat, and southern states. Its ease of vegetative propagation through leaf buds contributes to its widespread availability and ethnomedicinal use in renal and urinary disorders [30].
5.2 Ethnomedicinal Importance in Renal Disorders
Bryophyllum pinnatum holds a prominent position in Ayurveda and folk medicine for the management of urolithiasis and urinary tract ailments. The fresh leaf juice is traditionally administered orally to dissolve kidney stones and relieve dysuria. It is also used as a diuretic, anti-inflammatory agent, and urinary antiseptic. Tribal communities employ leaf decoctions to promote urine flow and reduce burning micturition, while paste preparations are used for nephritic pain. The ethnomedicinal relevance of the plant in renal disorders is supported by its lithotriptic reputation, indicating its ability to fragment urinary calculi and facilitate their expulsion [31]. These traditional claims have prompted extensive pharmacological investigations validating its role in preventing crystal aggregation and protecting renal tissue from oxidative damage [32].
5.3 Phytochemical Constituents
The phytochemical composition of Bryophyllum pinnatum is characterized by a broad spectrum of bioactive molecules that collectively contribute to its anti-urolithiatic and nephroprotective potential. Flavonoids such as quercetin, kaempferol, and their glycosidic derivatives constitute major polyphenolic components and exert strong antioxidant effects by neutralizing reactive oxygen species generated during calcium oxalate–induced renal injury; their metal-chelating capacity also lowers the availability of free calcium and oxalate ions, thereby hindering crystal nucleation and growth [33]. The plant is further enriched with phenolic acids including gallic, caffeic, and p-coumaric acid derivatives, which enhance the antioxidant status of urine, suppress lipid peroxidation in renal tissues, and stabilize cellular membranes under lithogenic stress. Distinctive bufadienolides such as bryophyllin A, bryophyllin B, and bersaldegenin-1,3,5-orthoacetate, although primarily recognized for cytotoxic properties, exhibit anti-inflammatory and membrane-protective effects that may indirectly reduce epithelial damage associated with crystal adherence. In addition, triterpenoids like bryophyllol and phytosterols such as β-sitosterol contribute to attenuation of inflammatory signaling and oxidative injury within renal tubules. The synergistic interaction of these phytoconstituents supports the plant’s ability to modulate oxidative stress, inflammation, and crystal formation processes involved in urolithiasis [34].
5.4 Pharmacological Potential Relevant to Kidney Stones
Bryophyllum pinnatum exhibits pronounced anti-urolithiatic activity through direct inhibition of calcium oxalate nucleation, aggregation, and crystal growth. In vitro crystallization assays demonstrate a reduction in crystal size and decreased adherence to renal epithelial cells. In sodium oxalate–induced urolithiasis models, administration of the hydroalcoholic extract normalizes serum creatinine, urea, and uric acid levels and restores renal antioxidant enzymes while reducing malondialdehyde content, indicating nephroprotection against oxidative injury. The plant also enhances urinary output, increases urinary pH, and promotes magnesium excretion, thereby lowering lithogenic potential. Anti- inflammatory effects mediated through down-regulation of pro-inflammatory cytokines and cyclooxygenase pathways further limit epithelial damage and crystal retention [35].
5.5 Preclinical and Clinical Studies
Multiple animal studies have validated the anti-urolithiatic potential of Bryophyllum pinnatum using ethylene glycol and sodium oxalate-induced lithiasis models. Administration of aqueous and hydroalcoholic leaf extracts significantly reduced urinary oxalate, calcium, and phosphate levels while increasing urine volume and magnesium excretion. Histopathological analysis revealed marked reduction in calcium oxalate crystal deposition and restoration of normal renal architecture [36].
Dose-dependent reversal of lithogenic biochemical parameters and improvement in creatinine clearance have been reported, with efficacy comparable to standard polyherbal formulations such as Cystone. Additionally, sodium oxalate-induced models demonstrated normalization of urinary and serum biomarkers along with reduced renal oxidative stress following treatment with hydroalcoholic extracts. Acute toxicity studies indicate a high safety margin, with no mortality observed at doses up to 2000 mg/kg in rodents, suggesting a favorable therapeutic index. Clinical evidence remains limited; however, traditional use and preliminary observational data support its role as an adjuvant therapy in urolithiasis, particularly for small calculi and recurrent stone formers. Well-designed randomized clinical trials are required to establish standardized dosing, efficacy, and long-term safety [37].
6. Pharmacological and phytochemical profile of Citrus sinensis
6.1 Botanical Description and Distribution
Citrus sinensis is an evergreen tree belonging to the family Rutaceae and is extensively cultivated in tropical and subtropical regions such as India, China, Brazil, and Mediterranean countries. The fruit peel, which constitutes a significant portion of the fruit mass, is an abundant source of pharmacologically active constituents. The dried pericarp is commonly used in herbal medicine and nutraceutical formulations. Due to its high flavonoid, essential oil, and citrate content, the peel has gained attention as a potential natural agent for the prevention of calcium oxalate urolithiasis [38].
6.2 Ethnomedicinal Relevance in Renal Disorders
In traditional medicine, citrus peels are used as mild diuretics and urinary alkalinizing agents. Decoctions prepared from dried peel have been employed to relieve burning micturition, promote urine flow, and reduce the risk of recurrent urinary calculi. The therapeutic value is largely attributed to their potassium citrate content, which increases urinary citrate levels, thereby inhibiting calcium oxalate crystallization. The traditional dietary recommendation of citrus fruits for stone prevention further supports their role in managing urolithiasis [39].
6.3 Phytochemical Profile
The peel of Citrus sinensis is rich in flavonoids such as hesperidin, naringin, nobiletin, and tangeretin, which exhibit strong antioxidant and anti-inflammatory properties. These flavonoids reduce oxidative stress in renal tissues and prevent epithelial injury induced by oxalate crystals. Phenolic acids including ferulic and caffeic acids contribute additional free-radical scavenging activity and membrane stabilization.
The volatile oil fraction is dominated by d-limonene, along with linalool and citral, which possess anti-inflammatory and smooth muscle relaxant properties that may facilitate ureteral stone passage. Importantly, the peel contains significant levels of citrate and potassium salts, which act as natural inhibitors of calcium stone formation by chelating calcium ions, increasing urinary pH, and reducing supersaturation of lithogenic salts [40].
6.4 Pharmacological Potential Relevant to Kidney Stones
The anti-urolithiatic activity of orange peel is mediated through multiple mechanisms. The citrate component binds free calcium ions, preventing nucleation and aggregation of calcium oxalate crystals. Flavonoids reduce lipid peroxidation and restore endogenous antioxidant enzymes such as superoxide dismutase and catalase, thereby protecting renal tubular epithelial cells from oxalate-induced injury. Essential oils exert anti-inflammatory effects and reduce ureteral spasm, which may aid in the expulsion of small calculi. The peel also exhibits moderate diuretic activity, leading to increased urine volume and dilution of lithogenic substances. Experimental studies have demonstrated reductions in urinary calcium, oxalate, and phosphate levels, along with increased urinary citrate and magnesium, which are known inhibitors of stone formation. Histopathological findings indicate decreased crystal deposition and preservation of renal architecture following treatment with citrus peel extracts [41].
6.5 Preclinical and Clinical Studies
Preclinical investigations using ethylene glycol–induced nephrolithiasis models have demonstrated that citrus peel extracts produce significant improvement in lithogenic biochemical parameters, including reductions in urinary calcium, oxalate, creatinine, and urea levels. Treatment has also been associated with enhanced urinary citrate excretion, which plays a key role in inhibiting calcium oxalate supersaturation, along with attenuation of renal oxidative stress. Histopathological analyses consistently show decreased crystal deposition and preservation of normal tubular architecture, indicating a pronounced nephroprotective effect [42]. Although controlled clinical trials evaluating isolated citrus peel extracts remain limited, epidemiological and dietary studies provide substantial supportive evidence, demonstrating an inverse association between citrus fruit consumption and recurrence of calcium oxalate stones. This protective effect is primarily attributed to increased urinary citrate and alkalinization of urine, which reduce lithogenic risk. Collectively, these findings suggest that citrus peel derived phytoconstituents may serve as a promising preventive adjunct in the management of urolithiasis, warranting further well-designed clinical investigations to establish standardized dosing and long-term efficacy [43].
7. Comparative Mechanism of Action-Analysis of Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis
The anti-urolithiatic efficacy of Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis is attributable to their chemically diverse yet mechanistically complementary phytoconstituents. T. terrestris is dominated by steroidal saponins such as protodioscin along with flavonoids and glycosides, which promote diuresis [44], reduce urinary supersaturation, and modify calcium oxalate crystal morphology, thereby limiting aggregation. B. pinnatum contains abundant flavonoids, phenolic acids, bufadienolides, and triterpenoids that primarily protect renal tubular epithelium through antioxidant activity, membrane stabilization, and suppression of inflammatory pathways, leading to reduced crystal adhesion and retention. In contrast, C. sinensis peel is distinguished by high levels of hesperidin, naringin, limonene-rich essential oil, and naturally occurring citrate and potassium salts [45]; citrate forms soluble calcium complexes and increases urinary pH, which inhibits nucleation and crystal growth while also facilitating dissolution of lithogenic salts. Although all three plants interfere with calcium oxalate lithogenesis, their principal targets differ: T. terrestris acts mainly by enhancing urine flow and lowering supersaturation, B. pinnatum by preserving epithelial integrity and preventing crystal attachment, and C. sinensis by citrate-mediated chelation and urinary alkalinization with additional antispasmodic effects that may aid stone passage. Experimental support is most extensive for T. terrestris, with multiple in vitro and in vivo models and its inclusion in established Ayurvedic formulations; B. pinnatum shows robust preclinical nephroprotective and anti-adhesion evidence but limited clinical data; and C. sinensis is backed largely by mechanistic studies and epidemiological findings linking higher citrus intake with reduced recurrence of calcium stones. Collectively, their complementary modes of action provide a strong pharmacological rationale for multi-targeted or polyherbal strategies in urolithiasis management [46].
Table 1. Mechanistic Comparison of the Three Medicinal Plants
|
Parameter |
Tribulus terrestris (Gokharu) |
Bryophyllum pinnatum |
Citrus sinensis (Orange peel) |
|
Primary phytoconstituents |
Steroidal saponins (protodioscin), flavonoids |
Flavonoids, bufadienolides, phenolics |
Flavonoids, citrate, essential oils |
|
Diuretic activity |
Strong (potassium salts, saponins) |
Moderate |
Moderate (potassium citrate) |
|
Nucleation inhibition |
Ca²⁺ chelation, Mg²⁺ ↑ |
Phenolics chelate Ca²⁺ |
Citrate chelation of Ca²⁺ |
|
Crystal aggregation |
Alters crystal morphology (COM→COD) |
Reduces crystal size |
Inhibits aggregation via citrate |
|
Antioxidant activity |
SOD, CAT, GSH ↑ |
High phenolic antioxidant |
Flavonoid antioxidant |
|
Anti-inflammatory effect |
Cytokine suppression |
COX inhibition, membrane stabilization |
Essential oil mediated |
|
Nephroprotection |
Tubular protection |
Strong epithelial protection |
Oxidative stress reduction |
|
Retention inhibition |
↓ epithelial adhesion |
Membrane stabilization |
Anti-inflammatory + citrate |
|
Stone expulsion |
Diuretic flushing |
Mild diuretic |
Smooth muscle relaxation |
|
Clinical relevance |
Widely used in Ayurveda |
Traditional lithotriptic |
Dietary prevention evidence |
8. Formulation Approaches and Future Perspectives
The development of effective phytotherapeutic strategies for urolithiasis requires integrated formulation approaches that address the multifactorial nature of stone pathogenesis. Polyherbal systems combining Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis provide a rational framework because their pharmacological actions are complementary: T. terrestris enhances diuresis and limits crystal aggregation, B. pinnatum offers potent antioxidant and nephroprotective effects that reduce epithelial injury and crystal adhesion, and C. sinensis supplies citrate and potassium that chelate calcium and promote urinary alkalinization. Such combinations may produce synergistic reductions in supersaturation, improve microcrystal clearance, and facilitate stone expulsion while permitting lower doses of individual components. However, optimization of plant ratios, evaluation of pharmacokinetic interactions, and long-term safety assessment remain necessary. The therapeutic translation of these botanicals is also constrained by poor aqueous solubility and limited bioavailability of key phytoconstituents such as flavonoids and saponins; therefore, advanced delivery platforms including phytosomes, nanoemulsions, polymeric nanoparticles, and controlled-release matrices are promising for enhancing renal tissue distribution and sustaining urinary levels of active molecules. Standardization is critical to ensure reproducible efficacy, requiring marker-based quality control (e.g., protodioscin, quercetin/kaempferol, hesperidin/citrate) supported by chromatographic and spectroscopic profiling and by stability and contaminant testing under pharmacopeial specifications. Despite strong preclinical evidence, clinical validation remains limited, with few randomized controlled trials using standardized extracts and well-defined endpoints such as recurrence rate, stone size reduction, and biochemical normalization. Regulatory advancement will depend on robust safety data, demonstration of batch consistency, clarification of herb–herb interaction profiles in polyherbal products, and implementation of pharmacovigilance systems, while harmonization of regional guidelines will be essential for broader acceptance of phytopharmaceutical anti-urolithiatic therapies [47].
9. Safety, Toxicity, and Drug Interaction Considerations
Safety assessment of herbal anti-urolithiatic agents indicates a generally favorable toxicological profile when used within therapeutic limits, although standardization and dose control remain essential. Experimental studies show that Tribulus terrestris possesses low acute toxicity with high tolerated doses and minimal renal or hepatic alterations during sub-chronic administration, but excessive or prolonged intake may produce mild gastrointestinal or hepatocellular changes and can potentiate the effects of diuretics, antihypertensives, or hormone-modulating drugs. Bryophyllum pinnatum is traditionally considered safe, yet the presence of bufadienolides necessitates caution because high concentrations may exert cardiotonic effects and theoretically interact with cardiac glycosides such as digoxin; therefore, controlled dosing and monitoring are advisable, particularly in patients with cardiovascular disorders. Citrus sinensis peel extracts exhibit a wide safety margin in dietary and pharmacological use, although concentrated essential oils may cause gastric irritation or photosensitivity, and flavonoid-mediated modulation of CYP3A4 suggests potential interactions with drugs like statins or calcium-channel blockers. A major limitation across all three botanicals is variability in phytochemical composition due to differences in source material and extraction methods, which complicates dose reproducibility and may lead to subtherapeutic or adverse outcomes. Consequently, marker-based standardization (e.g., protodioscin, quercetin/kaempferol, hesperidin), validated chromatographic profiling, defined therapeutic windows, and pharmacokinetic evaluation are required to ensure consistent safety and efficacy in clinical applications [48].
10. Challenges and Limitations in Herbal Anti-Urolithiatic Research
Research on herbal anti-urolithiatic agents is constrained by several methodological and translational limitations that hinder their progression to evidence-based clinical use. Although extensive experimental data support the efficacy of Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis, well-designed randomized multicentric clinical trials with adequate sample size, placebo control, and long-term follow-up are largely lacking, making it difficult to define optimal dosage, treatment duration, and recurrence prevention. Variability in phytochemical composition arising from geographical, seasonal, and processing differences leads to inconsistent concentrations of key bioactive markers, thereby affecting reproducibility and pharmacological reliability. Many studies employ non-standardized crude extracts without proper quantification of active constituents or uniform extraction protocols, and differences in experimental models and outcome measures further complicate cross-study comparisons. In addition, limited information on pharmacokinetics, bioavailability, and potential herb–drug interactions restricts clinical translation. Addressing these gaps through marker-based standardization, validated lithiasis models, Good Agricultural and Collection Practices, and rigorous clinical evaluation is essential for the development of reproducible and regulatory-acceptable phytopharmaceuticals for urolithiasis.
CONCLUSION
In summary, Tribulus terrestris, Bryophyllum pinnatum, and Citrus sinensis exhibit significant anti-urolithiatic potential through complementary mechanisms including inhibition of calcium oxalate crystallization, enhancement of urinary dilution, antioxidant nephroprotection, and suppression of renal inflammation. Preclinical studies consistently demonstrate improvement in urinary biochemical profiles, reduction of crystal deposition, and preservation of renal histoarchitecture, supporting their role in stone prevention and recurrence control. Their multitargeted pharmacodynamics align with the complex pathophysiology of urolithiasis and indicate value as adjunct or prophylactic therapies. Nevertheless, clinical translation requires standardized extracts, defined pharmacokinetic markers, optimized dosing, and well-designed randomized trials. Future work should emphasize marker-based quality control, synergistic polyherbal strategies, and advanced delivery systems to develop reproducible, evidence-based phytopharmaceutical interventions for kidney stone management.
REFERENCES


Vitthal Kundgir, Chandrashekhar Patil, Kajal Pansare, Jubershaha Fakir, Durgesh Pagar, Sunil Mahajan, Phytotherapeutic Strategies in Urolithiasis: Mechanistic Insights and Clinical Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2995-3011, https://doi.org/10.5281/zenodo.20645022
 10.5281/zenodo.20645022
10.5281/zenodo.20645022