
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Associate Professor, Pachamuthu College of Pharmacy, Krishnagiri Main Road, Dharmapuri, Tamilnadu – 636705, Affiliated to The Tamil Nadu Dr. M.G.R Medical University, Chennai.
2,3,4,5,6B. Pharm, Pachamuthu College of Pharmacy, Krishnagiri Main Road, Dharmapuri, Tamilnadu – 636705, Affiliated to The Tamil Nadu Dr. M.G.R Medical University, Chennai
Preface PTSD is one of the internal health problems common among youthful grown-ups, especially college scholars, due to their exposure to academic and cerebral stresses. This exploration was carried out to determine the frequency rate of PTSD among council scholars based on DSM- 5 criteria and the threat factors associated with PTSD. The present study used an experimental cross-sectional study involving 530 scholars, of whom 473 participants were considered in the analysis. Data collection was done using structured questionnaires and the PSS scale. The average PSS was 21.55, which shows moderate stress. Over half of the participants, i.e., 66.17 of them, faced severe stress. Ladies had higher scores than males regarding PTSD (p = 0.0265). Interestingly, PTSD scores were advanced in those who didn't have any trauma in their lives (p< 0.001). Those with physical injuries and poor academic performance had advanced PTSD scores. The current study set up that there's a frequence of PTSD symptoms among council scholars.
Post-traumatic stress disorder (PTSD) is a stress-related disorder with serious clinical symptoms; The daily activities of affected patients usually change; these changes are accompanied by a significantly reduced quality of life, excessive use of psychoactive substances, and other mental problems such as depression, anxiety, and phobias[1]. That may develop after exposure to exceptionally threatening or horrifying events. PTSD can occur after a single traumatic event or from prolonged exposure to trauma, such as sexual abuse in childhood [2]. Post-traumatic stress disorder (PTSD) is a mental health condition that develops in some people who have experienced or witnessed a traumatic or frightening event, such as a natural disaster, a serious accident or assault, a terrorist attack or military combat, or those who have been threatened with death, sexual violence, or injury [3] intrusive memories of battlefields coupled with the loss of interests, loneliness, and arousal, which are similar to the PTSD diagnostic criteria used today(6).. Subclasses of "internalizing disorders" identified within mood and anxiety disorders are evaluated.[7] Depression is often divided into five subcategories, all of which share the characteristic symptoms of a persistent sense of melancholy, emptiness, or irritability, coupled with somatic, psychic, and cognitive changes that have a significant impact on an individual’s functionality and overall well-being [15]. For example, although the lifetime prevalence of PTSD in veterans of the Vietnam War is around 30 percent, about 50 percent of Vietnam veterans had some clinically significant symptoms of PTSD [8]. A recent epidemiologic survey indicates that approximately 16% of patients with PTSD have one other psychiatric diagnosis, 17% have two other psychiatric diagnoses, and nearly 50% have three or more additional psychiatric diagnoses. These data indicate that for individuals with PTSD, comorbidity with other psychiatric diagnoses is the rule rather than the exception. [11] Based on data from the National Comorbidity Survey, about 60% of men and 50% of women are exposed to a traumatic event that can potentially result in the diagnosis of PTSD. Of these individuals, 8.2% of men and 20.4% of women develop PTSD.[9] The estimated lifetime prevalence of PTSD among these Veterans was 30.9% for men and 26.9% for women. Of Vietnam theater Veterans, 15.2% of males and 8.1% of females were currently diagnosed with PTSD at the time the study was conducted [10]. It has been shown that traumatic situations, such as chronic stress, tend to decrease the density of glutamatergic synapses, as well as being associated with a decrease in gray matter, particularly. at the level of the prefrontal cortex (17). Hence, we analysed the impact of Traumatic experiences on Emotional, cognitive, and Social functioning in college students.
METHODOLOGY
The study was carried out at Pachamuthu College of Pharmacy, with a student survey, for a period of three months. Permission was obtained from the institution of our college. A systematic random sampling was applied. Informed consent was obtained from the student after the nature and purpose of the study were explained. The relevant demographic details were collected in a questionnaire format. Data were collected only from those students who were willing to participate in the study. During the first phase of study, PTSD was assessed and based on the traumatic event, was identified, and then after calculating the student score (low, moderate, high, and severe), marks were assigned based on DSM-5 criteria. Thus, the results were analyzed and documented.
RESULT
A total of 530 participants were initially enrolled in the study. However, 57 participants were excluded due to non-willingness to continue and voluntary withdrawal from the study. Therefore, the final analysis included data from 473 participants. The mean age of the participants was 20 years. Among the analyzed participants, the majority were female (n = 328), while 145 participants were male. The mean Perceived Stress Scale (PSS) score of the participants was found to be 21.55, indicating an overall moderate level of perceived stress. Based on stress severity classification, only 3 participants were categorized as having mild stress, whereas 155 participants had moderate stress. A large proportion of participants (n = 313) experienced severe post-traumatic stress, and 2 participants were found to have very severe stress levels. The detailed demographic characteristics of the study participants are presented in Table:1.
TABLE 1: Demographic Details
|
Variables |
Frequency |
Percentage |
|
Total participants recruited |
530 |
100 |
|
Excluded participants |
57 |
10.75 |
|
No. of participants analyzed |
473 |
89.25 |
|
Mean Age |
20 |
- |
|
Gender Male |
154 |
30.6 |
|
Female |
328 |
69.3 |
|
Mean Stress Score (PSS) |
21.55 |
- |
|
No. Participants were presented with different severity and PSS Score Mild (PSS Score 0 – 9) |
3 |
0.63 |
|
Moderate (PSS Score 10 – 20) |
155 |
32.77 |
|
Severe (PSS Score 21 – 30) |
312 |
66.17 |
|
Very Severe (PSS Score 31 – 36) |
2 |
0.42 |
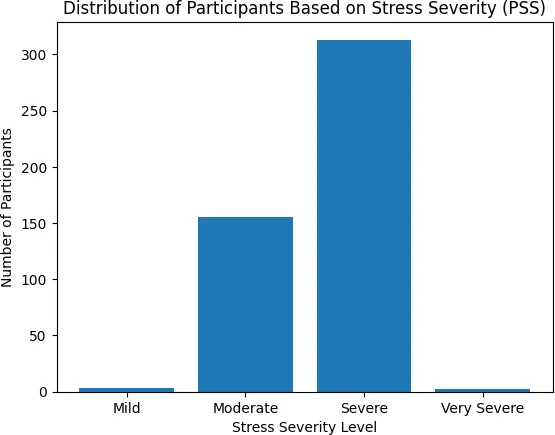
Figure 1: Bar chart showing severity levels of perceived stress among participant
The figure indicates that a significant proportion of the study population experienced high levels of perceived stress, with severe stress being the most predominant category. The mean score was 21.56 ± 5.79, with scores ranging from 7 to 32. The median score was 22, and the interquartile range was 10 (Q1 = 17, Q3 = 27), suggesting moderate variability among participants. The distribution showed slight negative skewness (−0.45) and platykurtic kurtosis (−0.68), indicating a mildly left-skewed and flatter distribution compared to normal distribution. The coefficient of variation was 26.84%, indicating moderate relative variability.
Table 2: shows the descriptive statistics of the study participants
|
Statistics |
score |
|
Count |
473 |
|
Mean |
21.56 |
|
sample variance |
33.48 |
|
sample standard deviation |
5.79 |
|
Minimum |
7 |
|
Maximum |
32 |
|
Range |
25 |
|
standard error of the mean |
0.27 |
|
Skewness |
-0.45 |
|
Kurtosis |
-0.68 |
|
coefficient of variation (CV) |
26.84% |
The normality test using chi-square goodness-of-fit revealed that the data significantly deviated from normal distribution. No outliers or extreme values were detected in the dataset. The normal probability plot showed that the data points did not perfectly follow the straight reference line, indicating deviation from normal distribution. This finding is consistent with the chi-square goodness-of-fit test. Independent-samples t-test and ANOVA were used to analyze the data. Female participants had significantly higher mean scores (Mean = 21.95) compared to male participants (Mean = 20.67), and this difference was statistically significant (p = 0.0265). Participants who had not experienced a traumatic event had significantly higher PTSD scores (Mean = 23.87, SD = 3.79) compared to those who had experienced a traumatic event (Mean = 20.98, SD = 6.05), and this difference was statistically significant, p < 0.001. These findings may be due to indirect trauma exposure, under-reporting of trauma, and general psychological distress among participants. The distribution of traumatic events among participants showed that the majority reported trauma under the "other" category (67.86%), followed by natural disasters (10.99%), accidents (10.15%), and physical abuse (9.30%). War or combat exposure was reported by 1.48% of participants, while sexual abuse was reported by only 0.21%.
Table 3: Classification of participants based on traumatic events.
|
S.no |
Types of Trauma |
Frequency |
Percentage |
|
1 |
Accident |
48 |
10.15 |
|
2 |
Natural disaster |
52 |
10.99 |
|
3 |
Physical abuse |
44 |
9.30 |
|
4 |
Sexual abuse |
1 |
0.21 |
|
5 |
War/ Combat exposure |
7 |
1.48 |
|
6 |
Others |
321 |
67.86 |
|
7 |
Total |
473 |
100 |
From the data, it was also found that Participants who were physically injured had significantly higher PTSD scores (Mean = 23.57, SD = 6.16) compared to those who were not physically injured (Mean = 20.62, SD = 5.36). This difference was statistically significant (t (471) = 5.31, p < 0.001). Participants whose school performance was affected reported significantly higher PTSD scores (Mean = 22.27, SD = 5.33) compared to those whose school performance was not affected (Mean = 19.86, SD = 6.45), and this difference was statistically significant (t (471) = 4.21, p < 0.001). Although participants whose daily activities were affected had higher PTSD scores (Mean = 22.26, SD = 6.41) compared to those whose daily activities were not affected (Mean = 21.34, SD = 5.57), this difference was not statistically significant (t (471) = 1.47, p = 0.143).
DISCUSSION
The present study evaluated the prevalence and determinants of perceived stress and post-traumatic stress among college-aged participants. The findings revealed that the overall mean PSS score was 21.55, indicating a moderate level of perceived stress among the participants. However, severity classification showed that the majority of participants experienced severe stress, highlighting a substantial psychological burden in this population. We then used latent transition analysis to understand the course of PTSD symptoms during this year of transition, and to explicate factors that may influence this course. Our findings revealed significant variability in PTSD symptom course over the first college year. [24] The hypothesis advanced in this study, that there is a significant correlation between psychological distress and academic adjustment in college students, was confirmed.[21] The result came significantly positive between exam stress and psychological distress (r= 0.514, p < .01). The result also showed significant positive correlation between classroom stress and psychological distress (r= 0.457, p < .05). Further, the result showed significant positive relation between classroom stress and exam stress (r= 0.597, p < .001).[22] . Moreover, the college environment can be challenging to navigate, resulting in additional stressors, including the experience of sexual assault. Additionally, the location of individuals within the social hierarchy further increases their chances of encountering stressors, as stressors vary according to one’s social status in society.[23] Only one participant met criteria for PTSD diagnosis. Therefore, an accurate sample to represent the population was not given in this study. This finding highlights the potential [25]. academic consequences of psychological distress and underscores the importance of early identification and intervention.
Overall, the findings of this study highlight the high prevalence of stress and PTSD symptoms among young adults and emphasize the significant role of gender, physical injury, and academic performance in influencing psychological outcomes.
CONCLUSION
Our study found a high prevalence of perceived stress and PTSD symptoms among participants. Female gender, physical injury, and affected academic performance were significantly associated with higher PTSD scores. These findings highlight the considerable psychological burden among young adults and emphasize the need for early screening and appropriate mental health support to improve student well-being.
REFERENCES






Sobana Tamilselvan*, Sivaprakash S, S. Shanmugam, S. Thirumalai, V. Vaishnavi, S. Vinitha, Prevalence, Severity and Predictors of Post -traumatic stress disorder (PTSD) Among College Students: A DSM-5 Based Cross-Sectional Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2906-2913. https://doi.org/10.5281/zenodo.21363374
 10.5281/zenodo.21363374
10.5281/zenodo.21363374