
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Godavari institute of Pharmacy Kolpa
Background: Atypical antipsychotic drugs used in the management of schizophrenia and bipolar disorder are frequently associated with poor patient adherence, in part due to swallowing difficulty, cognitive impairment, and treatment-refusal behavior. Orodispersible tablets (ODTs), which disintegrate rapidly in the oral cavity without water, are widely regarded as a patient-centric solution for this population, but achieving consistent disintegration, mechanical strength, and dissolution performance requires systematic formulation optimization. Method: A narrative review of the literature (predominantly 2009-2026) was conducted using PubMed, ScienceDirect, and Google Scholar to evaluate the application of Quality by Design (QbD) principles — including risk assessment (Ishikawa/FMEA), Design of Experiments (DoE), and design-space development per ICH Q8(R2) — to the formulation of ODTs of atypical antipsychotics, with focused analysis of aripiprazole alongside olanzapine, quetiapine, and risperidone. Results: Across the reviewed studies, DoE-optimized ODT formulations of atypical antipsychotics achieved in vitro disintegration times ranging from approximately 18.7 to 32 seconds depending on drug, disintegrant system, and manufacturing method. For aripiprazole specifically — a BCS Class IV drug with low and pH-dependent solubility — solid-dispersion and co-crystal strategies combined with superdisintegrant optimization produced disintegration times of 22-28 seconds and in vitro drug release exceeding 98% within 45 minutes, while Box-Behnken and factorial designs successfully identified disintegrant, binder, and diluent concentrations as the critical material attributes governing tablet performance. Quetiapine fumarate ODTs optimized by 3² factorial sublimation technique achieved a disintegration time of 18.66 seconds, and QbD-based risk assessment of olanzapine oral lyophilizates identified gelatin concentration and lyophilization process parameters as dominant critical quality attribute drivers. Conclusion: QbD provides a scientifically robust, regulator-preferred framework for translating the disintegration and solubility challenges specific to atypical antipsychotics — most acutely, aripiprazole's BCS Class IV status — into systematically optimized, patient-centric ODT products, though pharmacopeial standardization of natural excipient inputs and expanded in vivo bioequivalence data remain necessary to fully realize this framework's regulatory value.
Schizophrenia, bipolar disorder, and related psychotic conditions are managed predominantly with oral antipsychotic pharmacotherapy, yet medication non-adherence remains one of the principal drivers of relapse in this population. Estimates suggest that a substantial proportion of patients with chronic psychotic disorders have difficulty adhering to daily oral regimens, driven by factors including swallowing difficulty, cognitive impairment, disorganized behavior, and active treatment refusal or medication-hiding behavior. Orodispersible tablets (ODTs) — solid dosage forms that disintegrate or disperse rapidly in the oral cavity using only saliva, per European Pharmacopoeia convention typically within three minutes — have therefore been extensively explored as a patient-centric delivery platform for atypical (second-generation) antipsychotics, since a tablet that dissolves on the tongue cannot readily be concealed or discarded, and offers pre-gastric absorption advantages in patients experiencing acute agitation.
Second-generation antipsychotics such as olanzapine, quetiapine, risperidone, and aripiprazole differ meaningfully in their physicochemical behavior — spanning BCS Class II (olanzapine) to BCS Class IV (aripiprazole) characteristics — which directly affects the formulation strategy required to achieve consistent ODT disintegration and dissolution performance. Achieving a robust ODT formulation for these drugs is therefore not a routine tableting exercise: it requires simultaneous control of disintegrant selection and concentration, taste-masking, mechanical strength, and (for poorly soluble actives) solubility-enhancement strategy, all while meeting compendial disintegration-time and friability targets.
Quality by Design (QbD), as codified in ICH Q8(R2) and supported by ICH Q9 (Quality Risk Management) and ICH Q10 (Pharmaceutical Quality System), offers a systematic, risk-based framework for navigating this multi-variable formulation space. Rather than optimizing a formulation empirically through one-factor-at-a-time experimentation, QbD begins with a Quality Target Product Profile (QTPP), proceeds through structured risk assessment (commonly using Ishikawa/fishbone diagrams and Failure Mode and Effects Analysis, FMEA) to identify Critical Material Attributes (CMAs) and Critical Process Parameters (CPPs), applies Design of Experiments (DoE) to quantify their effect on Critical Quality Attributes (CQAs), and culminates in a defined design space and control strategy that together provide regulatory flexibility and manufacturing robustness. This review examines the published application of QbD principles to ODT development for atypical antipsychotics, with particular emphasis on aripiprazole as a formulation case study given its distinctive BCS Class IV solubility-permeability profile.
1.1 Review Methodology
A structured literature search was conducted across PubMed/MEDLINE, ScienceDirect, and Google Scholar using combinations of the terms "Quality by Design," "QbD," "orodispersible tablet," "orally disintegrating tablet," "atypical antipsychotic," "aripiprazole," "olanzapine," "quetiapine," and "risperidone," restricted predominantly to studies published between 2009 and 2026. Original formulation-optimization studies reporting Design of Experiments methodology, critical quality attribute data (disintegration time, hardness, friability, dissolution), and QbD-specific tools (risk assessment, design space) were prioritized, alongside relevant ICH Q8(R2) guidance documentation and antipsychotic pharmacotherapy/adherence literature providing clinical context.
2. The Quality by Design Framework for ODT Development
ICH Q8(R2) defines Quality by Design as a systematic approach to development that begins with predefined objectives and emphasizes product and process understanding and process control, based on sound science and quality risk management. Within this framework, the design space is defined as the multidimensional combination and interaction of input variables (e.g., material attributes) and process parameters that have been demonstrated to provide assurance of quality; operating within an approved design space is not considered a change requiring regulatory re-approval, offering meaningful post-approval manufacturing flexibility.
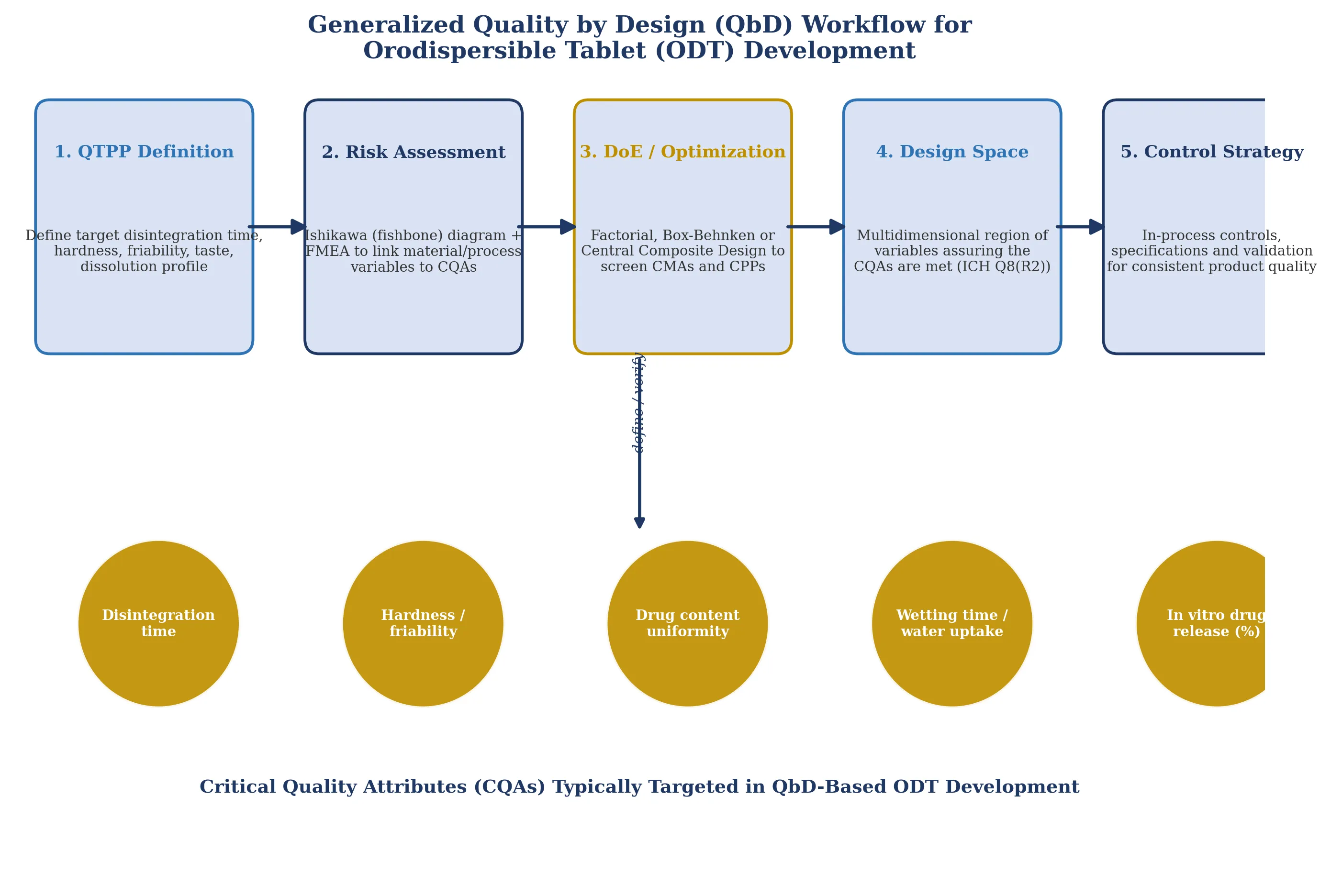
Figure 1. Generalized Quality by Design (QbD) workflow applied to orodispersible tablet (ODT) development, progressing from Quality Target Product Profile (QTPP) definition through risk assessment, Design of Experiments (DoE), design-space establishment, and control strategy, mapped against the critical quality attributes typically targeted for ODT formulations.
Risk assessment is the pivotal early step distinguishing QbD from traditional empirical formulation approaches. Ishikawa (fishbone) diagrams are widely used to visually map the categories of variables — materials, process, equipment, and environment — that may influence a given CQA, while Failure Mode and Effects Analysis (FMEA) is then applied to rank the identified variables by severity, occurrence probability, and detectability, focusing subsequent DoE studies on the highest-risk parameters rather than attempting to study every variable exhaustively.
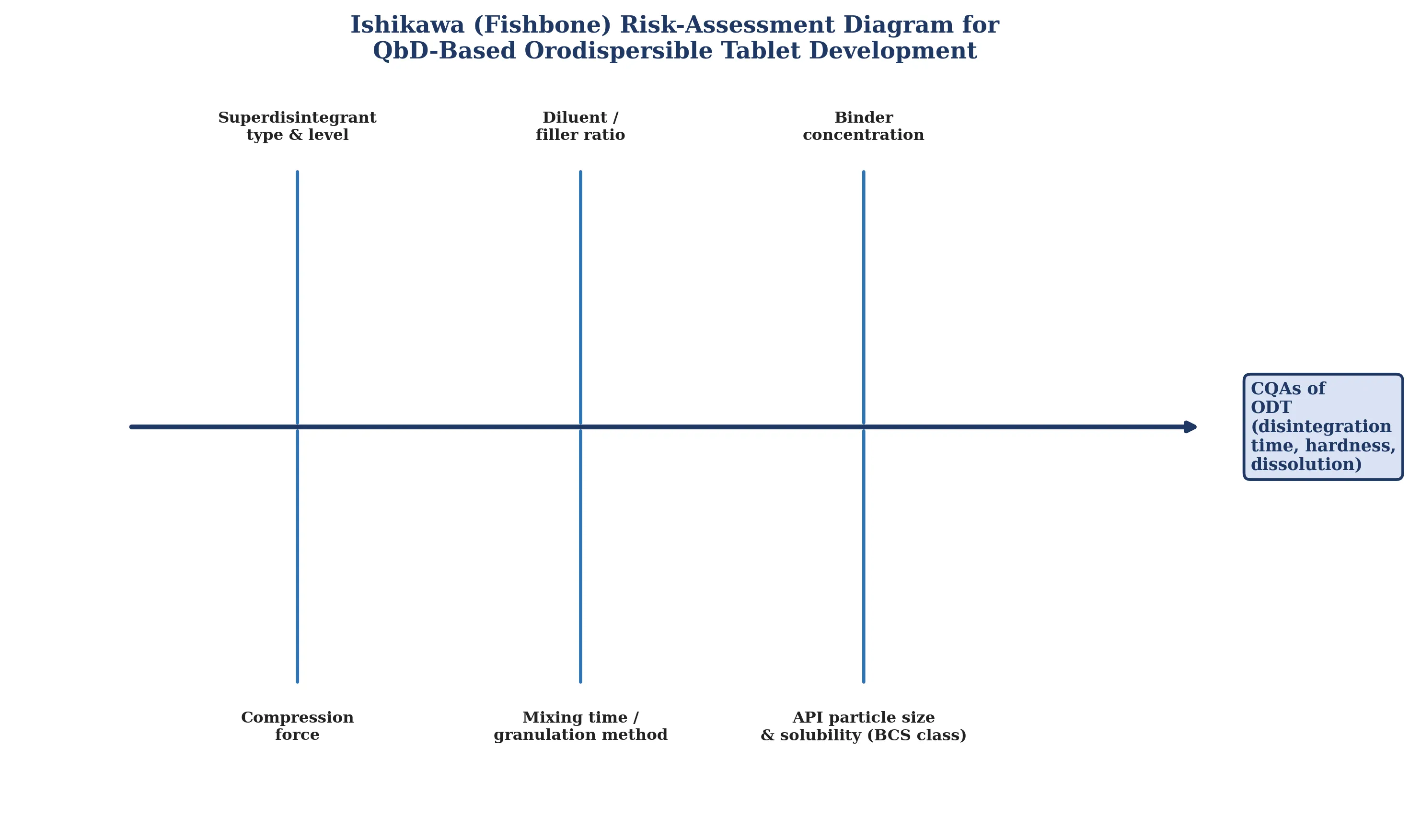
Figure 2. Representative Ishikawa (fishbone) risk-assessment diagram identifying formulation and process variables commonly evaluated as potential critical material attributes (CMAs) and critical process parameters (CPPs) in QbD-based ODT development for atypical antipsychotics.
For ODT formulations specifically, the CQAs most consistently targeted across the reviewed literature are in vitro disintegration time, tablet hardness and friability, drug content uniformity, wetting time/water absorption ratio, and in vitro drug release, with superdisintegrant type and concentration, diluent-to-binder ratio, and compression force recurring as the most frequently identified CMAs/CPPs across DoE studies of ODT systems, including carbamazepine, cannabidiol, trandolapril, fidaxomicin, lornoxicam, and — as detailed below — the atypical antipsychotics.
3. Aripiprazole: A QbD-Relevant Formulation Case Study
Aripiprazole occupies a formulation-critical position among the atypical antipsychotics: it is classified as a BCS Class IV drug (low solubility, low permeability) by several formulation studies, with pH-dependent solubility that declines markedly above pH 5, complicating both dissolution behavior and the tolerability of orally retained (ODT/film) dosage forms due to potential oral-mucosal irritation at low pH. This combination of poor, pH-dependent solubility and the need for rapid oral disintegration makes aripiprazole a particularly demanding — and instructive — case study for QbD-based ODT development, since disintegrant optimization alone is typically insufficient; solubility-enhancement strategy must be integrated into the same risk-assessment and DoE framework.
3.1 Solid Dispersion-Based Aripiprazole ODTs
Navya et al. addressed aripiprazole's solubility limitation by preparing solid dispersions with β-cyclodextrin and PVP K30 (1:1 and 1:2 ratios) via physical mixture and solvent evaporation, subsequently formulating oral disintegrating tablets by direct compression using both natural (tapioca starch, Amorphophallus campanulatus) and synthetic (sodium starch glycolate, crospovidone) superdisintegrants. The optimized formulation (F3, containing 7.5% w/w tapioca starch) achieved a disintegration time of 28 ± 1.52 seconds and in vitro dissolution of 98.64 ± 0.29% at 45 minutes, demonstrating that solubility enhancement via solid dispersion, combined with systematic superdisintegrant screening, can be reconciled within a single formulation-optimization exercise.
3.2 Co-Crystal and Multi-Channel Approaches
A parallel strategy addressed aripiprazole's solubility limitation at the crystal-engineering level: aripiprazole co-crystals were formulated into orally disintegrating tablets using croscarmellose sodium and sodium starch glycolate as superdisintegrants, with croscarmellose sodium producing a shorter disintegration time (22 ± 5 seconds) than sodium starch glycolate at comparable concentrations, attributed to its favorable swelling index. Separately, Han et al. developed a novel multi-channel ODT architecture for aripiprazole using a specialized wet-compression mold, in which the multi-channel structure increased the tablet's contact surface area with water and shortened the effective water-penetration distance, thereby accelerating both in vitro and in vivo disintegration and dissolution relative to conventionally structured ODTs — an engineering-level (rather than purely excipient-level) approach to the same CQA.
3.3 Formal DoE/QbD Optimization of Aripiprazole Tablets
Formal QbD methodology has been applied directly to aripiprazole immediate-release tablet optimization: a Box-Behnken Design (BBD) study using Design-Expert® software selected disintegrant concentration, binder concentration, and diluent concentration as the three independent variables of highest anticipated risk, on the basis that aripiprazole's BCS Class IV status (low solubility and low permeability) makes adequate superdisintegrant concentration essential to achieving target plasma concentrations from an immediate-release dosage form; wet granulation was identified as the necessary manufacturing process over direct compression given the low (~10% w/w) drug loading and poor powder flow properties of the API. Complementary QbD-based approaches have also been reported for non-oral aripiprazole delivery — including microemulsion-based intranasal and liquisolid-compact formulations optimized via Box-Behnken and factorial designs respectively — reflecting the breadth of QbD application across aripiprazole's formulation-development literature even where ODT is not the final dosage form, and reinforcing solubility enhancement as the recurring CMA-level theme specific to this drug.
Table 1. Reported QbD/DoE-relevant formulation parameters and outcomes for Aripiprazole ODT and related oral dosage form studies.
|
Study focus |
DoE / optimization tool |
Key CMA(s)/CPP(s) identified |
Reported outcome |
|
Solid dispersion ODT (β-CD/PVP K30 + tapioca starch) |
Comparative screening (natural vs synthetic superdisintegrants) |
Superdisintegrant type & concentration |
DT 28±1.52 s; 98.64% release at 45 min |
|
Co-crystal ODT |
Comparative concentration screening |
Superdisintegrant type (CCS vs SSG) |
DT 22±5 s with croscarmellose sodium |
|
Multi-channel ODT (wet compression) |
Mold/structure design + disintegrant screening |
Tablet channel architecture, disintegrant type/amount |
Improved in vitro/in vivo disintegration & dissolution vs conventional ODT |
|
Immediate-release tablet (30 mg) |
Box-Behnken Design (3 factors, 3 levels) |
Disintegrant, binder, diluent concentration |
Optimized formulation meeting CQA targets via DoE |
4. QbD-Based ODT Development for Other Atypical Antipsychotics
4.1 Olanzapine
Olanzapine, a BCS Class II drug (poor aqueous and salivary solubility) subject to substantial first-pass metabolism (up to ~40% of dose), has been formulated as both conventional ODTs and freeze-dried oral lyophilizates. An early roll-compaction-based ODT optimization study evaluated disintegrant and binder concentration across six formulations, identifying an optimal batch (F-5) with drug release comparable to a marketed reference product and stable in vitro dispersion time over six-month accelerated (40°C/75% RH) stability testing. More recently, a formal QbD study applied risk assessment (including FMEA) to olanzapine oral lyophilizate development, identifying excipient type, concentration and particle size, and drug/excipient solubility as critical material attributes, and cooling rate, shelf temperature, and chamber pressure during lyophilization as critical process parameters; a design space was established using response-surface modelling (88.69% coefficient of determination), with gelatin concentration above 15% w/w consistently associated with disintegration times exceeding 180 seconds — directly illustrating how QbD-derived design-space boundaries translate into actionable formulation limits. A separate comparative in vitro analysis across eleven marketed olanzapine ODT products (using risperidone ODT as a comparator) further demonstrated that manufacturing method (freeze-dried versus soft-compressed versus conventional hard/dense tablets) was itself a dominant determinant of disintegration time, freeze-dried formulations disintegrating fastest.
4.2 Quetiapine
Quetiapine fumarate, subject to extensive hepatic first-pass metabolism that limits its oral bioavailability, has been formulated as a directly compressible ODT using a sublimation technique, employing Indion 414 as superdisintegrant and camphor as the subliming pore-forming agent. A full 3² factorial design was used to evaluate the effect of Indion 414 (3-5% w/w) and camphor (5-15% w/w) concentration on tablet thickness, weight variation, hardness, friability, content uniformity, wetting time, porosity, disintegration time, and in vitro drug release; the optimized formulation (5% w/w Indion 414, 5% w/w camphor) achieved a disintegration time of 18.66 seconds, with scanning electron microscopy confirming pore formation following camphor sublimation and providing direct mechanistic support for the DoE-identified optimum.
4.3 Risperidone
Risperidone ODT development has been documented in both formal DoE-based formulation optimization (applying QbD methodology analogous to that used for fast-dissolving tablet development of other actives) and in extensive later-phase clinical evaluation: a summary of ten Phase I clinical trials assessed taste, tablet disintegration time, bioequivalence, and tolerability for a rapidly disintegrating risperidone formulation, illustrating the translational pathway from bench-level QbD/DoE optimization through to clinical bioequivalence confirmation — a step that remains comparatively less mature in the aripiprazole, olanzapine, and quetiapine ODT literature reviewed here, and represents a specific opportunity for future work.
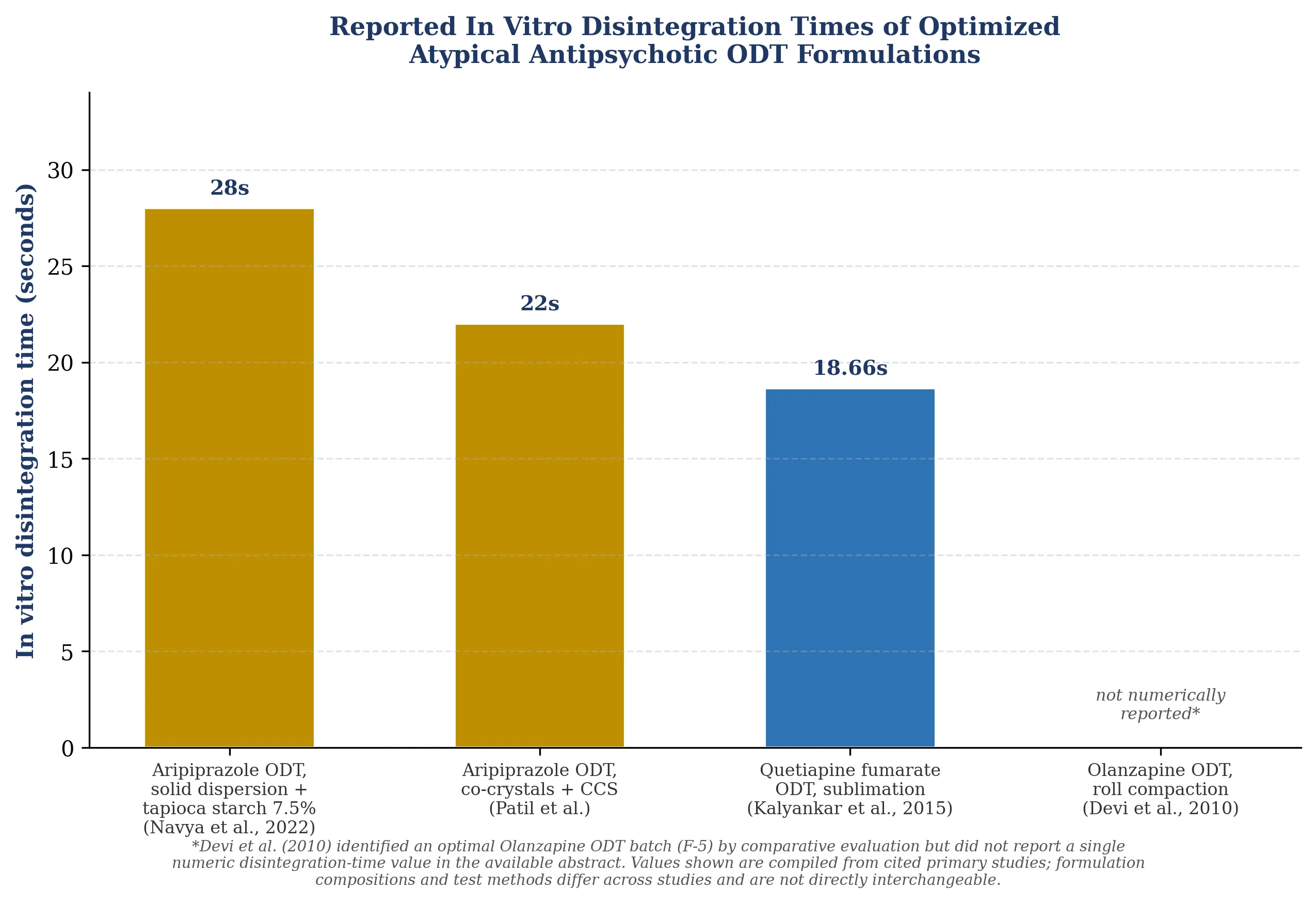
Figure 3. Reported in vitro disintegration times of optimized atypical antipsychotic ODT formulations compiled from cited primary studies. Formulation compositions, manufacturing methods, and test conditions differ across studies; values are shown for illustrative comparison only.
Table 2. Comparative summary of QbD/DoE-based ODT development across the four reviewed atypical antipsychotics.
|
Drug |
BCS class (as reported) |
Key formulation challenge |
DoE tool(s) applied |
Best reported DT |
|
Aripiprazole |
Class IV (low solubility, low permeability) |
Solubility enhancement + rapid disintegration simultaneously |
Box-Behnken Design; comparative factorial screening |
~22 s (co-crystal + CCS) |
|
Olanzapine |
Class II (poor aqueous/salivary solubility) |
First-pass metabolism; lyophilizate disintegration vs appearance trade-off |
Risk assessment (FMEA) + response-surface design space |
Marketed-comparable (specific DT not reported in abstract) |
|
Quetiapine |
Extensively hepatically metabolized; low oral bioavailability |
Achieving porosity-driven rapid disintegration by direct compression |
3² full factorial design (sublimation technique) |
18.66 s |
|
Risperidone |
Established oral bioavailability profile |
Bench-to-clinic translation; taste masking |
DoE-based formulation optimization; Phase I clinical confirmation |
Clinically confirmed rapid disintegration (bench DT study-specific) |
5. Quality Evaluation Parameters for Antipsychotic ODTs
Across the reviewed studies, a consistent battery of pre- and post-compression quality evaluation parameters is applied, regardless of the specific antipsychotic or QbD tool used. Pre-compression evaluation typically includes angle of repose, bulk and tapped density, Carr's index, and Hausner ratio to confirm powder flow suitability for the selected manufacturing process (direct compression, wet granulation, or roll compaction). Post-compression evaluation consistently includes tablet hardness, friability, weight variation, drug content uniformity, wetting time, water absorption ratio, in vitro disintegration time, and in vitro dissolution/drug release, with FTIR and/or DSC used to rule out drug-excipient interaction and, for lyophilizate and solid-dispersion-based systems, XRD used to confirm the degree of amorphization achieved. Short-term or accelerated stability testing (commonly 40°C/75% relative humidity, over periods ranging from three to six months in the reviewed formulation-level studies) is used to confirm that optimized disintegration time and drug content remain within specification over the studied storage interval.
6. Future Perspectives
Several directions emerge from this review as priorities for advancing QbD-based ODT development for atypical antipsychotics. First, formal design-space publication (rather than single-point "optimized formulation" reporting) remains relatively uncommon in the reviewed literature outside the olanzapine lyophilizate study, representing an opportunity to more fully realize the regulatory-flexibility benefit that ICH Q8(R2) is intended to provide. Second, for aripiprazole specifically, integrating solubility-enhancement strategy (solid dispersion, co-crystallization, or liquisolid technology) directly into a unified DoE alongside disintegrant/binder/diluent screening — rather than treating solubility enhancement and disintegration optimization as sequential, separately optimized steps — would better reflect true multi-CQA QbD practice. Third, bench-to-clinic translation, well demonstrated for risperidone through Phase I disintegration/bioequivalence trials, is comparatively underdeveloped for aripiprazole, olanzapine, and quetiapine ODTs in the literature reviewed, and represents a clear direction for future clinical-translational work. Finally, given the taste-masking and mucosal-tolerability concerns specific to orally retained aripiprazole formulations (attributable to its pH-dependent solubility profile), continued application of QbD risk-assessment tools to taste-masking CMAs — not solely disintegration- and dissolution-related CQAs — is warranted.
7. CONCLUSION
The reviewed literature demonstrates that Quality by Design provides a scientifically rigorous and increasingly well-established framework for the development of orodispersible tablets of atypical antipsychotic drugs. Risk-assessment tools (Ishikawa diagrams, FMEA) combined with Design of Experiments methodologies (factorial, Box-Behnken, and central composite designs) have been successfully applied to identify and optimize the critical material attributes and critical process parameters governing disintegration time, mechanical strength, and dissolution performance across olanzapine, quetiapine, risperidone, and — with particular formulation complexity owing to its BCS Class IV solubility-permeability profile — aripiprazole. Aripiprazole in particular illustrates the value of integrating solubility-enhancement strategy within the QbD framework rather than treating it as a separate formulation problem, and the comparative results reviewed here (disintegration times of approximately 18.7-32 seconds across DoE-optimized formulations) confirm that systematic, risk-based formulation development can reliably meet the rapid-disintegration, patient-centric performance targets that make ODTs clinically valuable in this population, provided that design-space documentation and clinical translation continue to mature alongside the bench-level optimization work already well represented in the literature.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgment
The authors acknowledge [Institution/Department name] for providing the necessary literature access and support for this review.
REFERENCES

Dr. Rahul Solunke*, Ople Shivani, Quality by Design (QbD)-Based Development and Quality Evaluation of Orodispersible Tablets of Atypical Antipsychotic Drugs: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 2347-2356. https://doi.org/10.5281/zenodo.21318280
 10.5281/zenodo.21318280
10.5281/zenodo.21318280