
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy Practice, Shivlingeshwar College of Pharmacy, Almala, Latur, India
Helicobacter pylori (H. pylori) is a major cause of peptic ulcer disease (PUD) and gastric cancer. Since its identification, advancements in eradication therapies have significantly improved patient outcomes. This review discusses recent developments in the management of H. pylori infection, including improved diagnostic techniques, novel treatment regimens, and innovative therapeutic approaches such as nanotechnology-based drug delivery and probiotic applications. Traditional triple therapy is losing efficacy due to rising antibiotic resistance, leading to the adoption of quadruple therapy and emerging therapies such as vonoprazan-based regimens and nanoparticle-based antibiotics. Additionally, the role of non-pharmacological interventions, including lifestyle modifications and dietary changes, is explored. The review highlights the need for personalized treatment strategies, new antimicrobial agents, and innovative drug delivery systems to enhance eradication rates and reduce treatment-related complications.
A common cause of gastric cancer and peptic ulcers, Helicobacter pylori (H. pylori) gastritis is usually acquired in childhood through familial transmission[1]. This grouping within families raises the risk of gastric cancer and peptic ulcer disease[2]. About 17% of infected people will get a peptic ulcer in their lifetime[3]. Although it used to be the most common cancer worldwide, gastric cancer has become much less common in Western nations as a result of better food preservation, sanitation, and vitamin C fortification, which also slows the development of atrophic gastritis[4]. With the right eradication therapy, peptic ulcers can now be cured after it was discovered in the 1980s that H. pylori is the cause of the condition[3,5].
Similarly, attempts have been made to lower the prevalence of H. pylori, especially in high-risk groups, since it was identified as the main cause of gastric cancer and atrophic gastritis[6]. Although poor people and immigrants from high-prevalence areas are still at risk, improvements in sanitation, living conditions, and access to clean water have significantly reduced transmission rates, especially in wealthy countries[7-8].
Improved diagnostics, customized treatments, and the implementation of eradication programs in high-risk areas are currently the main focuses of H.[9] pylori management efforts, especially in nations like China, Korea, and Japan where population-wide eradication campaigns are being sought[10-13]. Targeted strategies are being tested to address persistent risk among particular subpopulations in low-prevalence nations like the US. [14,15].
Etiology :
Infection with H pylori :
The majority of peptic ulcer disease cases are caused by H pylori infection and the use of nonsteroidal anti-inflammatory drugs (NSAIDs). In the US, less than 75% of people who do not take NSAIDs have a H pylori infection that causes duodenal ulcers. In one study, 61% of duodenal ulcers and 63% of stomach ulcers were positive for H pylori, excluding patients who took NSAIDs. White people had lower rates than non-white people. Compared to uncomplicated ulcer disease, the prevalence of H pylori infection is much lower in complex ulcers (such as bleeding or perforation).
Drugs :
Peptic ulcer disease is frequently brought on by the use of NSAIDs. These medications make the mucosa more susceptible to damage by interfering with the mucosal permeability barrier. Up to 30% of persons who use NSAIDs experience gastrointestinal side effects. A history of prior peptic ulcer disease, advanced age, female sex, high dosages or combinations of NSAIDs, prolonged NSAID usage, concurrent use of anticoagulants, and severe comorbid conditions are all factors linked to an elevated risk of duodenal ulcers in the context of NSAID use.
According to a long-term prospective study, individuals with arthritis over 65 who frequently took low-dose aspirin were more likely to experience dyspepsia severe enough to need stopping NSAIDs. [7] This implies that in order to lower NSAID-associated upper gastrointestinal events, older patients should be consulted about better NSAID use management.
The majority of evidence currently supports the claim that H pylori and NSAIDs work in concert to prevent the development of peptic ulcer disease, despite the fact that this theory was once disputed. Eliminating H pylori in NSAID-naive users prior to starting NSAIDs was linked to a lower incidence of peptic ulcers, according to a meta-analysis.[10]
It is uncertain how often NSAID gastropathy is in children, although it appears to be on the rise, particularly in kids with NSAID-treated chronic arthritis. Low-dose ibuprofen has been shown in case reports to cause stomach ulcers in children, even after just one or two doses. [11]
While corticosteroids by themselves do not raise the risk of peptic ulcer disease, they can increase the risk of ulcers in people taking NSAIDs at the same time.
Users of serotonin reuptake inhibitors with moderate to high affinity for the serotonin transporter or the diuretic spironolactone [12] may be at higher risk of upper gastrointestinal tract hemorrhage. [13]
Factors related to lifestyle :
There is insufficient evidence to conclude that tobacco smoking increases the incidence of duodenal ulcers. The discovery that smoking may speed up stomach emptying and reduce pancreatic bicarbonate production lends credence to smoking's pathogenic involvement. Nevertheless, research has yielded conflicting results. In one prospective trial, smoking was not found to be a risk factor for duodenal ulcers in over 47,000 men. [14] Smoking, however, may raise the chance of a return of peptic ulcer disease when there is a H pylori infection. [15] Smokers' stomach antrums have higher levels of H pylori invasion, and smoking damages the gastroduodenal mucosa. [16]
It is well known that ethanol can lead to nonspecific gastritis and irritation of the stomach mucosa. There is conflicting evidence regarding alcohol use as a risk factor for duodenal ulcers. There was no correlation between alcohol consumption and duodenal ulcers in a prospective trial involving over 47,000 men. [14]
Caffeine use may not be linked to a higher incidence of duodenal ulcers, according to the available data.
High levels of physiological stress :
Burns, trauma to the central nervous system (CNS), surgery, and serious illness are stressful situations that can lead to peptic ulcer disease. Multiple traumatic injuries, hypotension, respiratory failure, sepsis, and serious systemic illness all raise the risk of secondary (stress) ulceration.
Cushing ulcers are usually deep, single ulcers that are prone to perforation and are linked to brain tumors or injuries. They are found in the stomach or duodenum and are linked to elevated gastric acid production. Curling ulcers are linked to severe burns. Complications such as upper-gastrointestinal (GI) bleeding and stress ulceration are becoming more common in severely ill children receiving intensive care. An higher risk of gastric ulcers and hemorrhage is associated with severe sickness and a lower pH in the stomach.
Physiological elements :
Both maximal acid output (MAO) and baseline acid output (BAO) are elevated in as many as one-third of patients with duodenal ulcers. For the development of duodenal ulcers, one study found that higher BAO was linked to an odds ratio [OR] of up to 3.5 and higher MAO to an OR of up to 7. People with a BAO higher than 15 mEq/h are particularly at risk. The fact that the parietal cell mass is elevated to almost double the reference range in a considerable percentage of individuals with duodenal ulcers may be the cause of the elevated BAO. [17]
Patients with duodenal ulcers frequently have rapid gastric emptying in addition to increased gastric and duodenal acidity. 95% of all duodenal ulcers occur in the first section of the duodenum, which receives a high acid load as a result of this acceleration. Duodenal villous cells are replaced by cells that resemble the gastric epithelium in both morphology and secretory properties when the duodenum becomes acidified, a condition known as gastric metaplasia. An environment that is conducive to H pylori colonization may be produced by gastric metaplasia.
Extreme weather conditions and seasonal variations can potentially harm the stomach mucosa and impair its barrier function. [18] Yuan et al. observed that individuals with peptic ulcer disease who were at high risk of bleeding had considerably reduced expression of heat shock protein 70 (HSP70) and decreased mucosal thickness in the stomach antrum as compared to those who were at low risk of bleeding in extremely cold climates.
Furthermore, occludin, HSP70, nitric oxide synthase (NOS), and epidermal growth factor receptor (EGFR) levels were significantly lower in extreme cold climates than in extreme hot climates; however, there were no statistically significant differences in these protein expression levels between patients at high and low risk of bleeding. [18] The pH levels of stomach juices and the frequencies of H pylori infection did not significantly differ between patients at high and low bleeding risk, according to the researchers. [18]
Epidemiology :
The complex changes in the risk factors for peptic ulcer disease, such as declining rates of H pylori infection, the widespread use of antisecretory agents and nonsteroidal anti-inflammatory drugs (NSAIDs), and an aging population, have contributed to a decline in the incidence and prevalence of peptic ulcer disease worldwide over the past few decades, as well as the corresponding rates of hospitalizations and mortality. [19]
Statistics from the United States :
An estimated 10% of Americans have signs of a duodenal ulcer at some point in their lives, and 4.6 million Americans suffer from peptic ulcer disease each year. [20] 70% to 90% of stomach ulcers and 90% of duodenal ulcers are caused by H pylori infection. [21] As people age, the percentage of those with peptic ulcer disease and H pylori infection rises steadily.
Over the previous three to four decades, duodenal ulcers have generally become less common. Due in part to the concurrent use of aspirin in an older population, the incidence of complicated gastric ulcers and hospitalization has remained consistent despite the drop in the rate of simple gastric ulcers.
The lifetime prevalence of peptic ulcer disease has changed from being more common in men to being more common in women. The lifetime prevalence is roughly 11%–14% in men and 8–11% in women. [20] According to age trends for ulcer occurrence, the annual incidence rates of peptic ulcer disease were found to be 0.10-0.19% for physician-diagnosed peptic ulcer disease and 0.03-0.17% when based on hospitalization data. [22] The 1-year prevalence based on physician diagnosis was 0.12-1.50%, and that based on hospitalization data was 0.10-0.19%. Most studies showed a decline in the incidence or prevalence of peptic ulcer disease over time.
Global data :
In various nations, the prevalence of peptic ulcer disease varies and is mostly based on correlation with the two main causes of the condition: H pylori and NSAIDs. [23] Spain had the greatest yearly incidence of total peptic ulcer illness (141.8/100,000 people), whereas the UK had the lowest (23.9/100,000 people), according to a 2018 systematic MEDLINE and PubMed review. [24] South Korea had the greatest yearly incidence of perforated peptic ulcer illness (4.4/100,000 people), while the UK had the lowest (2.2/100,000 people). [24]
The prognosis is quite good when the underlying cause of peptic ulcer disease is treated. The majority of patients receive successful treatment when the H pylori infection is eradicated, nonsteroidal anti-inflammatory drugs (NSAIDs) are avoided, and antisecretory medication is used appropriately. The natural course of the illness is altered when the H pylori infection is eradicated, as the ulcer recurrence rate drops from 60% to 90% to roughly 10% to 20%. This recurrence rate is larger than previously documented, though, and may indicate that there are more ulcers that are not brought on by a H pylori infection.
Classification :
One type of acid-peptic disease is peptic ulcers. Peptic ulcers can be categorized based on a number of variables,
On basis of location :
By place Duodenum (also known as duodenal ulcer)
Esophagus (also known as an esophageal ulcer)
Stomach (also known as a gastric ulcer)
Meckel's diverticulum (also known as Meckel's diverticulum ulcer, is extremely painful to the touch.) [25]
Modified Johnson :
Type I: Ulcer along the stomach's body, usually along the locus minoris resistantiae's smaller curve at incisura angularis. not connected to excessive acid secretion.
Type II: A body ulcer that coexists with duodenal ulcers. connected to excessive acid output.
Type III: Within 3 cm of the pylorus in the pyloric canal. connected to excessive acid output.
Proximal gastroesophageal ulcer, type IV.
Type V: May appear all over the stomach. connected to long-term NSAID use (e.g., ibuprofen). [25]
Pathophysiology :
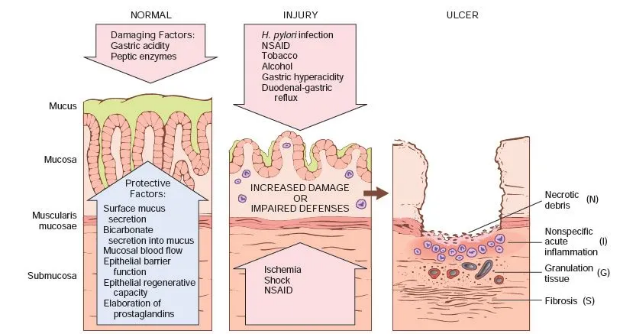
Fig: Pathophysiology of PUD [58]
Defects in the duodenal or stomach mucosa that penetrate the muscularis mucosa are known as peptic ulcers. Mucus is secreted by the stomach and duodenum's epithelial cells in reaction to cholinergic stimulation and irritation of the epithelial lining. Acid and pepsin cannot pass through the gel layer that makes up the surface part of the gastric and duodenal mucosa. Bicarbonate, which is secreted by other gastric and duodenal cells, helps buffer acid that is close to the mucosa. Prostaglandins of the E type (PGE) play a crucial protective role because they boost mucous layer and bicarbonate generation.
Additional safeguards are in place to lessen damage in the event that pepsin and acid penetrate the epithelial cells. By eliminating extra hydrogen ions, ion pumps in the basolateral cell membrane of the epithelial cells aid in controlling intracellular pH. Healthy cells go to the damaged location during the restoration process. Acid that permeates the damaged mucosa is eliminated by mucosal blood flow, which also supplies surface epithelial cells with bicarbonate.
Gastric acid secretion and gastroduodenal mucosal defense are physiologically balanced under normal circumstances. When the equilibrium between defensive mechanisms and aggressive elements is upset, mucosal damage and peptic ulcers result. By permitting the back passage of hydrogen ions and ensuing damage to epithelial cells, aggressive substances like alcohol, bile salts, pepsin, NSAIDs, H pylori infection, and acid might change the mucosal defense. Tight intercellular junctions, mucus, bicarbonate, mucosal blood flow, cellular restitution, and epithelial regeneration are some of the defense mechanisms.
In 1983, the gram-negative spirochete H pylori was initially connected to gastritis. Since then, additional research on H pylori has shown that it plays a significant role in the triad—which also contains pepsin and acid—that causes primary peptic ulcer disease. This organism's distinct microbiologic traits, like the production of urease, enable it to alkalinize its surroundings and endure for years in the stomach's hostile, acidic environment, where it inflames the mucosa and, in certain cases, exacerbates the severity of peptic ulcer disease.
Inflammation is typically the outcome of H pylori colonizing the stomach mucosa. In both the adult and pediatric literature, the link between H pylori gastritis and duodenal ulceration is now well established. It has been observed that patients with H pylori infection had lower levels of somatostatin and higher amounts of gastrin and pepsinogen. The duodenum is exposed to more acid in infected people. Urease, catalase, vacuolating cytotoxin, and lipopolysaccharide are among the well-known virulence agents that H pylori produces.
Because H pylori overcomes the abnormality, it has also been shown that the majority of individuals with duodenal ulcers had impaired duodenal bicarbonate secretion. [5] The development of gastric metaplasia, or the presence of gastric epithelium in the first part of the duodenum, is encouraged by the combination of decreased duodenal bicarbonate secretion and increased stomach acid secretion, which lowers the pH in the duodenum. In regions of stomach metaplasia, H pylori infection causes duodenitis and increases vulnerability to acid damage, which makes duodenal ulcers more likely. A study that tracked 181 patients with endoscopy-negative, nonulcer dyspepsia discovered that duodenal colonization by H pylori was a significantly significant predictor of the development of duodenal ulcers later on. [6]
Diagnosis :
Health and family background :
Your doctor will obtain a medical and family history in order to help diagnose peptic ulcers and look for ulcer-causing variables. Your physician might inquire about :
Your symptoms
your medical background, including any previous Helicobacter pylori (H. pylori) infections peptic ulcers
medications that you take particularly NSAIDs (nonsteroidal anti-inflammatory meds)
Your family's history of stomach cancer, H. pylori infection, or peptic ulcers
Physical examination :
A doctor can diagnose peptic ulcers or ulcer complications with the aid of a physical examination.When performing a physical examination, a physician typically
Checks for abdominal swelling :
uses a stethoscope to listen for sounds inside your abdomen and taps it. examining for discomfort or tenderness
Blood test :
Blood tests can be used by doctors to look for symptoms of peptic ulcer complications or an H. pylori infection. A medical practitioner will draw blood from you and send it to a laboratory for a blood test
Urea breath test :
To check for an H. pylori infection, doctors may do a urea breath test. You will swallow a pill, drink, or pudding that contains urea that has been "labeled" with a particular carbon atom for the test. The bacteria will turn the urea into carbon dioxide if H. pylori is present. You will exhale carbon dioxide into a container after a few minutes.
Your exhaled breath will be tested by a medical practitioner. The medical practitioner will certify that you have an H. pylori infection in your digestive tract if the test finds the tagged carbon atoms.
Stool examination :
To check for an H. pylori infection, doctors may use stool testing. A stool sample collection and keeping container will be provided by your physician. Instructions on where to mail or pick up the kit for testing will be sent to you.
Biopsy with upper gastrointestinal (GI) endoscopy:
To confirm the diagnosis of a peptic ulcer and investigate its cause, doctors may prescribe an upper gastrointestinal endoscopy.
During an upper GI endoscopy, a physician views the lining of your upper GI tract, including your stomach, duodenum, and esophagus, using an endoscope, which is a flexible tube equipped with a camera. A physician takes biopsies during an upper GI endoscopy by inserting a device through the endoscope to remove tiny fragments of tissue from the lining of your stomach. The tissue will be examined under a microscope by a pathologist.
The upper GI series :
An upper gastrointestinal series may occasionally be ordered by clinicians to aid in the diagnosis of peptic ulcers or ulcer complications. The Upper GI series views your upper GI system using x-rays and barium, a chalky liquid you consume. [25]
Prognosis :
The prognosis is quite good when the underlying cause of peptic ulcer disease is addressed. The majority of patients receive successful treatment when the H pylori infection is eradicated, nonsteroidal anti-inflammatory drugs (NSAIDs) are avoided, and antisecretory medication is used appropriately. The natural course of the illness is altered when the H pylori infection is eradicated, as the ulcer recurrence rate drops from 60% to 90% to roughly 10% to 20%. This recurrence rate is larger than previously documented, though, and may indicate that there are more ulcers that are not brought on by a H pylori infection.[29]
The incidence of blockage and perforation in ulcers caused by NSAIDs is roughly 0.1% and 0.3%, respectively, per patient year. When duodenal and stomach ulcers are combined, the annual rate of any consequence across all age categories is roughly 1% to 2% per ulcer.
About one person dies from peptic ulcer disease for every 100,000 instances, a mortality rate that has somewhat declined over the past few decades. The mortality rate from ulcer hemorrhage is about 5% when all patients with duodenal ulcers are taken into account. [20] Despite the introduction of proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs), the mortality rate in the context of ulcer hemorrhage has not altered significantly over the past 20 years. However, when intravenous PPIs are administered following effective endoscopic therapy, there is evidence from meta-analyses and other trials that the death risk from bleeding peptic ulcers is reduced. [25, 26, 27, 28]
Mortality was 15.2% at 30 days, 19.2% at 90 days, 22.6% at 1 year, and 24.8% at 2 years in a retrospective population-based study (2001-2014) that assessed long-term mortality in 234 patients who had surgery for a perforated peptic ulcer. [30] During a median follow-up of 57 months, 36% of patients passed away after excluding the 30-day mortality data. Age above 60 and the presence of comorbidities, such as active cancer, hypoalbuminemia, pulmonary illness, cardiovascular disease, and serious surgical complications during the initial stay, were independent factors linked to an elevated risk of long-term death. [31]
Treatment :
Antibiotics are usually used to treat H. pylori infections, and triple therapy and quadruple therapy are the most popular regimens [5]. A PPI plus two antibiotics (clarithromycin and amoxicillin or metronidazole) are commonly used in triple treatment. Usually, PPI, bismuth, metronidazole, and tetracycline make up quadruple therapy.
A network meta-analysis [8] assessing the efficacy of several treatment plans and current international guidelines propose vonoprazan-based triple therapy for seven days and non-bismuth quadruple therapies for ten to fourteen days. High eradication rates of >90% were attained for first-line H. pylori infections using vonoprazan triple therapy and reverse hybrid therapy, a hybrid (dual-quadruple) treatment that consists of a PPI and amoxicillin for 14 days with the addition of clarithromycin and metronidazole for the final seven days. In Western countries, levofloxacin triple therapy yielded the highest eradication rates. According to the network meta-analysis, the conventional triple therapy plan was the least successful. These regimens nevertheless have inherent problems that could lead to further increases in antibiotic resistance and dysbiosis of the gut microbiota because of the empirical use of several antibiotics.
International agreement currently highlights the significance of eradication treatment for H. pylori-infected individuals. Medications used to eradicate H. pylori include proton pump inhibitors (PPIs) and antibiotics. PPIs raise the pH of the stomach and prevent the production of gastric acid, which makes it easier for the antibiotics to have their bactericidal effect. Antibiotics kill H. pylori directly. H. pylori cannot be completely eradicated by a single medication; a multimodal treatment plan is required. Triple and quadruple therapy, as well as the ensuing sequential, concurrent, and mixed therapies, are the primary clinical regimens. The Toronto Consensus on the Treatment of Adult H. pylori Infection (Toronto Consensus) [31], the American College of Gastroenterology Consensus on the Treatment of H. pylori Infection (ACG Consensus) [32], the Maastricht V Consensus [33], and the Fifth Chinese National Consensus [34] are the leading international consensus opinions on H. pylori eradication treatment. Their main treatment plans are compiled and contrasted in Table.
The suggested primary treatment regimen for H. pylori infection is the subject of an international census.
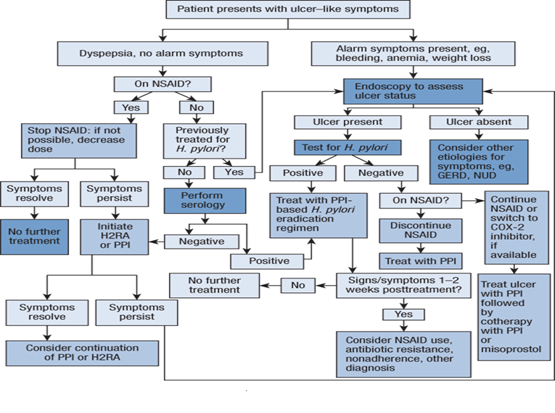
Fig: Treatment Algorithm [59]
Triple therapy :
Triple treatment is when two antibiotics and one PPI are taken together. In 1996, the clarithromycin-based conventional triple regimen was created [35] . Clarithromycin dosages of 500 mg and 250 mg, respectively, can be administered for seven days along with omeprazole, amoxicillin, or omeprazole with metronidazole. This regimen's minimal drug intake, short treatment duration, excellent efficacy, and low frequency of adverse effects made it the first-line regimen for H. pylori eradication at the time. High eradication rates were later attained by researchers who added metronidazole or levofloxacin to the triple treatment. However, as H. pylori's resistance to antibiotics has increased over time, Even when the regimen is prolonged to 10 or even 14 days, the eradication rate remains inadequate. The eradication rate of these drug-based triple regimens has been below or significantly below 80% [36]
Bismuth quadruple therapy :
Prior to the clarithromycin triple regimen, the traditional bismuth quadruple regimen was developed in 1995 and includes PPI, bismuth, tetracycline, and metronidazole [37]. Bismuth quadruplet was only utilized as a remedial treatment because clarithromycin triplet was the first-line regimen at the time. The effectiveness of the clarithromycin triplet regimen decreased as the rate of H. pylori resistance to the antibiotic rose, and bismuth quadruple therapy was relegated to first-line treatment. bismuth boosts the eradication rate of H. pylori-resistant strains by 30% to 40%. [38] The addition of bismuth to triple regimens combining clarithromycin, metronidazole, and levofloxacin has produced satisfactory efficacy despite the high rates of resistance to these medications [39]. Bismuth triple therapy is recommended as the first-line treatment option by the Maastricht V, Toronto, and ACG consensus because of its high eradication rate, low susceptibility to medication resistance, and good short-term safety.
Non Bismuth quadruple therapy :
A non-Bismuth Quadruple regimen includes concomitant therapy (four medications for 10 or 14 days), mixed therapy (same as sequential therapy for the first 5 or 7 days and concomitant therapy for the second 5 or 7 days), and sequential therapy (PPI + amoxicillin for the first 5 or 7 days and PPI + clarithromycin + metronidazole for the second 5 or 7 days), depending on the mode of administration. Concomitant therapy with three antibiotics offers the best relative efficacy of these regimens since it is the most successful at combating antibiotic resistance, but it also has a greater profile of side effects. The Maastricht V and Toronto consensus has excluded sequential medications for adult treatment due to their susceptibility to single resistance to metronidazole or clarithromycin. Non-bismuth quadruple treatment effectively turns into PPI plus amoxicillin two-component therapy when both clarithromycin and metronidazole develop resistance, and eradication rates for sequential, mixed, and concurrent medication are all decreased [40] The Fifth Chinese National Consensus states that non-bismuth quadruple therapy with clarithromycin and metronidazole is not advised for empirical treatment in regions where H. pylori dual resistance to clarithromycin and metronidazole is greater than 15% [41]
Combined Chinese and Western medicine therapy:
Herbal combination triple therapy and bismuth quadruple therapy are popular combined Chinese and Western medicine treatments; the former has the strongest clinical support. Studies have shown that while clinical symptom relief is better than bismuth quadruple therapy, some herbal combination triple therapy has equivalent eradication rates to bismuth quadruple therapy at 14 days [42]. Due to excessive drug use and a slight improvement in the eradication rate, Chinese herbal medicine in conjunction with bismuth quadruple therapy has been utilized comparatively infrequently. Due to excessive drug use and a slight improvement in the eradication rate, Chinese herbal medicine in conjunction with bismuth quadruple therapy has been utilized comparatively infrequently. The Chinese Expert Consensus on Collaborative Diagnosis and Treatment of Gastritis Caused by Helicobacter pylori in Adults states that in order to increase the eradication rate of bismuth quadruple remedy treatment, Chinese herbal medicine can be used in conjunction with various aspects of the treatment to identify symptoms [43]. Two weeks prior to starting bismuth triple therapy, patients with evident gastrointestinal problems can benefit from Traditional Chinese Medicine (TCM), which is backed by scientifically proven medical evidence. For two weeks following bismuth quadruple therapy, patients without overt gastrointestinal problems can receive evidence-based TCM treatment.
Other therapy :
Quinolones have a variety of uses. Levofloxacin resistance is common, with the exception of a few places, because they are often used in clinical settings and are cross-resistant to one another. Levofloxacin-containing therapy is not advised for initial treatment by the Fifth Chinese National Consensus, Maastricht V Consensus, or Toronto Consensus; nevertheless, it might be utilized as a corrective treatment option in the event that clarithromycin-based first-line therapy fails. second-line treatment (the traditional bismuth quadruple regimen); there is indications that a combination of high-dose PPI and amoxicillin can produce high eradication rates, but there is little clinical data and it is not part of the mainstream consensus guidelines. Although there isn't enough conclusive data to increase eradication rates, there is evidence that some adverse effects can be lessened by adding specific probiotics to traditional therapy.[44]
All things considered, triple therapy is no longer a viable first-line treatment option unless there are unambiguous drug sensitivity test results or proof of low resistance rates. Clarithromycin and metronidazole resistance, either single or dual, can compromise the effectiveness of non-bismuth quadruple regimens. Major mainstream consensus viewpoints advocate bismuth quadruple therapy as the best alternative for first treatment or in places where clarithromycin resistance is greater than 15% due to its high eradication rate and low resistance to bismuth.[44]
Novel antibiotic :
New antibiotics, such as rifabutin, rifaximin, sitafloxacin, and fidaxomicin, have shown promise in treating H. pylori infection, including MDRS [45]. These antibiotics offer new opportunities for effectively treating H. pylori infection and reducing the risk of antibiotic resistance [46].
Sequential therapy :
To treat an H. pylori infection, sequential therapy entails using two distinct antibiotics, then a PPI and another antibiotic. Sequential therapy may be useful in regions with high levels of clarithromycin resistance, according to recent investigations, and can yield high eradication rates [47].
Nanotechnology to combat Helicobacter pylori infection :
A promising area for the creation of novel therapies to treat H. pylori infection is nanotechnology [48]. The state of nanotechnology against Helicobacter pylori at the moment consists of:
Nanoparticle-based therapies :
The ability of nanoparticles to stop H. pylori from growing has been studied. In both in vitro and in vivo experiments, metal nanoparticles—such as those of silver, copper, gold, titanium dioxide, magnesium oxide, zinc oxide, and selenium—have demonstrated encouraging outcomes. The potential of polymer-based nanoparticles, including chitosan nanoparticles, as a medication delivery method for the management of H. pylori infection has also been studied. The targeting capabilities of the nanoparticles have been improved by functionalizing chitosan with the monosaccharide D-mannose.[49]
Nano emulsion :
One possible treatment for an H. pylori infection is the use of nanoemulsions. Antimicrobial drugs can be delivered directly to the site of infection using these emulsions, which are made up of oil droplets scattered in water [50].
Nanocarriers :
In order to treat H. pylori infection, nanocarriers have been created as a possible medication delivery mechanism [51]. By delivering medications straight to the illness site and shielding them from deterioration, these carriers can boost medication effectiveness and lessen adverse effects [52].
Nonstructured surface :
The application of nanostructured surfaces to prevent H. pylori from adhering to stomach epithelial cells has been investigated in recent research. In order to create a nanostructured surface, nanoparticles are coated onto a substrate. By decreasing the surface area accessible for bacterial adhesion, the nanostructured surface can stop biofilm formation [53].
Nanoparticle-based vaccines :
In order to prevent H. pylori infection, vaccinations based on nanoparticles have been created. In order to elicit an immunological response, these vaccines use nanoparticles coated with H. pylori antigens. According to recent research, vaccinations based on nanoparticles have the potential to prevent H. pylori infection and can elicit a robust immune response [54].
Nanoparticle-based drug conjugates :
Drug conjugates based on nanoparticles have been created as a possible remedy for H. pylori infection. These conjugates are made up of nanoparticles coated in probiotics or antibiotics, among other antimicrobial substances. By shielding the medications from deterioration and delivering them straight to the infection site, the nanoparticles improve their effectiveness and lessen their adverse effects [55].
Probiotics against H. pylori :
Probiotics are live bacteria that enhance the makeup and function of the gut microbiome, hence benefiting the host's health. Probiotics have the potential to lower the incidence of H. pylori infections and lessen symptoms linked to them, according to recent updates on their involvement in the prevention and treatment of H. pylori infections. Research has indicated that specific probiotic strains, including Lactobacillus and Bifidobacterium [56], can lessen the risk of H. pylori infection and ease symptoms related to H. pylori, including bloating and stomach pain. Probiotics can also enhance the function of the intestinal barrier and regulate the immune system, which can lower the risk of H. pylori infection and related illnesses [57].
The possibility of using probiotics in combination with other strategies, such antibiotics and lifestyle changes, is highlighted by recent updates on their involvement in the prevention and treatment of H. pylori infections. Probiotics can increase the efficiency of antibiotics in eliminating H. pylori bacteria and lowering the likelihood of adverse effects like diarrhea that are linked to drugs. Probiotic use in the treatment and prevention of H. pylori infections is not without its difficulties, though. The absence of standardization in probiotic products is a major obstacle that might make comparing their safety and effectiveness challenging. Furthermore, research is ongoing to determine the best probiotic strain, dosage, and duration for the treatment and prevention of H. pylori infections [57].
CONCLUSION
The management of H. pylori infection has evolved significantly with advancements in diagnostics and treatment strategies. The decline in the effectiveness of traditional triple therapy due to antibiotic resistance has necessitated the adoption of alternative regimens, including bismuth-based quadruple therapy and vonoprazan-based treatment. Novel approaches, such as nanotechnology and probiotics, offer promising alternatives by enhancing drug efficacy and reducing adverse effects. Future research should focus on personalized therapies, improved diagnostic tools, and the development of new antimicrobial agents to optimize eradication rates. A multidisciplinary approach incorporating pharmacological, technological, and lifestyle modifications will be essential for the effective management of H. pylori infections and associated complications.
REFERENCES




Azeem Bagwan, Bhosale Rohit, Vaishnavi Bansode, Divya Chordiya, Recent Advancement in Management of H. Pylori Induced PUD, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 462-476. https://doi.org/10.5281/zenodo.14992264
 10.5281/zenodo.14992264
10.5281/zenodo.14992264